
Efficacy of Sirolimus Treatment in PEComa–10 Years of Practice Perspective

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Analyzed Group
2.2. Treatment
2.3. Analyzed Data
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Treatment
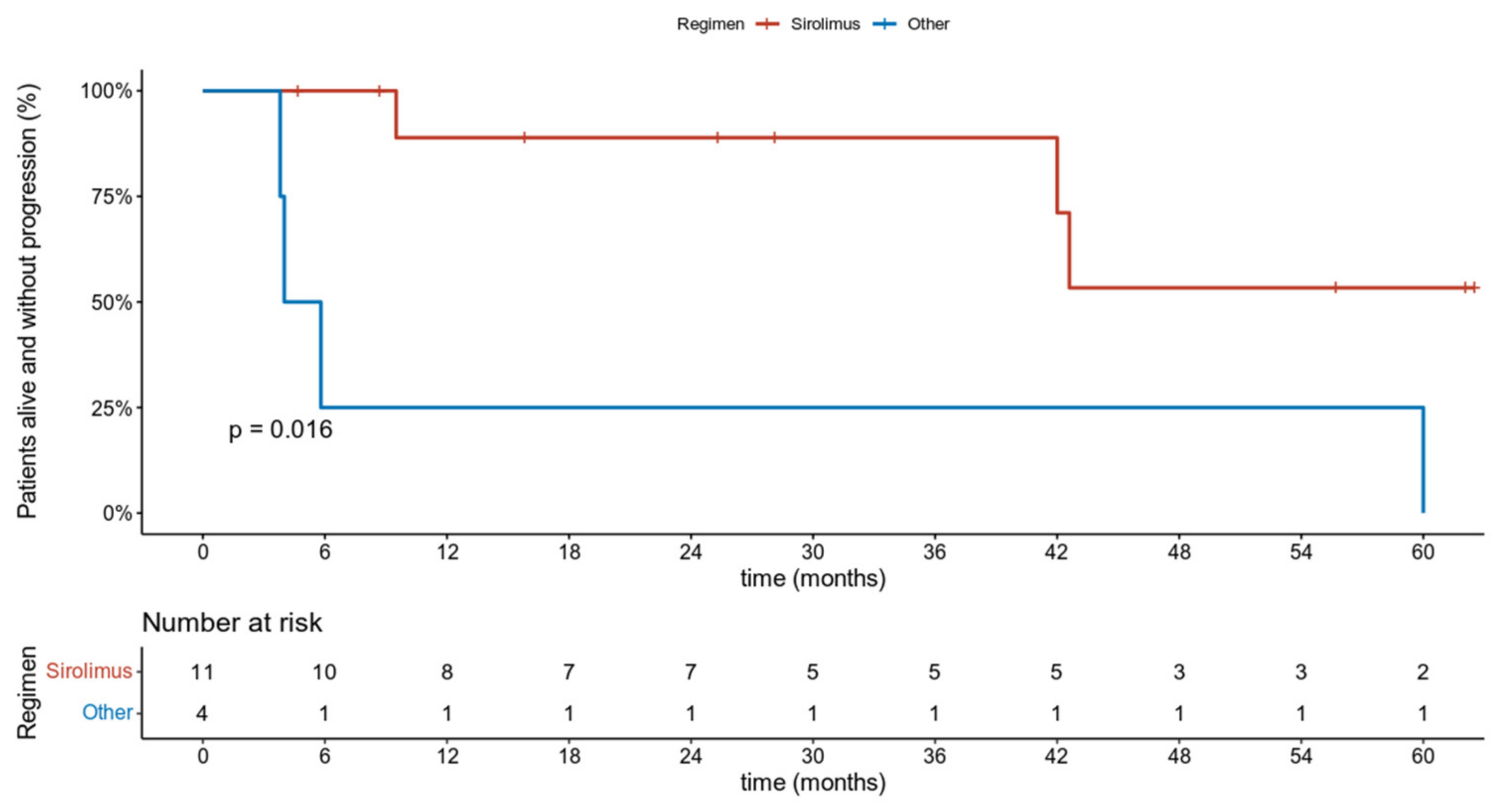
3.3. Efficacy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klimczak, A.; Pękul, M.; Wiater, K.; Rutkowski, P. PEComa—Grupa rzadkich nowotworów pochodzenia mezenchymalnego. Nowotw. J. Oncol. 2011, 61, 52–56. [Google Scholar]
- Bleeker, J.S.; Quevedo, J.F.; Folpe, A.L. “Malignant” perivascular epithelioid cell neoplasm: Risk stratification and treatment strategies. Sarcoma 2012, 2012, 541626. [Google Scholar] [CrossRef] [Green Version]
- Krawczyk, M.; Ziarkiewicz-Wróblewska, B.; Wróblewski, T.; Podgórska, J.; Grzybowski, J.; Gierej, B.; Krawczyk, P.; Nyckowski, P.; Kornasiewicz, O.; Patkowski, W.; et al. PEComa—A Rare Liver Tumor. J. Clin. Med. 2021, 10, 1756. [Google Scholar] [CrossRef] [PubMed]
- Sobiborowicz, A.; Czarnecka, A.M.; Szumera-Ciećkiewicz, A.; Rutkowski, P.; Świtaj, T. Diagnosis and treatment of malignant PEComa tumours. Oncol. Clin. Pract. 2020, 16, 22–33. [Google Scholar] [CrossRef]
- Rutkowski, P.L.; Mullen, J.T. Management of the “Other” retroperitoneal sarcomas. J. Surg. Oncol. 2018, 117, 79–86. [Google Scholar] [CrossRef]
- Sobiborowicz, A.; Czarnecka, A.M.; Szumera-Ciećkiewicz, A.; Rutkowski, P.; Świtaj, T. Diagnosis and treatment of angiomyolipoma (AML) tumours. Oncol. Clin. Pract. 2020, 16, 116–132. [Google Scholar] [CrossRef]
- Randle, S.C. Tuberous Sclerosis Complex: A Review. Pediatr. Ann. 2017, 46, e166–e171. [Google Scholar] [CrossRef] [PubMed]
- Muzykewicz, D.A.; Sharma, A.; Muse, V.; Numis, A.L.; Rajagopal, J.; Thiele, E.A. TSC1 and TSC2 mutations in patients with lymphangioleiomyomatosis and tuberous sclerosis complex. J. Med. Genet. 2009, 46, 465–468. [Google Scholar] [CrossRef]
- Smolarek, T.A.; Wessner, L.L.; McCormack, F.X.; Mylet, J.C.; Menon, A.G.; Henske, E.P. Evidence that lymphangiomyomatosis is caused by TSC2 mutations: Chromosome 16p13 loss of heterozygosity in angiomyolipomas and lymph nodes from women with lymphangiomyomatosis. Am. J. Hum. Genet. 1998, 62, 810–815. [Google Scholar] [CrossRef] [Green Version]
- Agaram, N.P.; Sung, Y.S.; Zhang, L.; Chen, C.L.; Chen, H.W.; Singer, S.; Dickson, M.A.; Berger, M.F.; Antonescu, C.R. Dichotomy of Genetic Abnormalities in PEComas With Therapeutic Implications. Am. J. Surg. Pathol. 2015, 39, 813–825. [Google Scholar] [CrossRef] [Green Version]
- Flechter, E.; Zohar, Y.; Guralnik, L.; Passhak, M.; Sela, G.B. Long-lasting stable disease with mTOR inhibitor treatment in a patient with a perivascular epithelioid cell tumor: A case report and literature review. Oncol. Lett. 2016, 12, 4739–4743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Manning, B.D. The TSC1-TSC2 complex: A molecular switchboard controlling cell growth. Biochem. J. 2008, 412, 179–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhaoighill, M.N.; Dunlop, E.A. Mechanistic target of rapamycin inhibitors: Successes and challenges as cancer therapeutics. Cancer Drug Resist. 2019, 2, 1069–1085. [Google Scholar] [CrossRef] [Green Version]
- Kenerson, H.; Folpe, A.L.; Takayama, T.K.; Yeung, R.S. Activation of the mTOR pathway in sporadic angiomyolipomas and other perivascular epithelioid cell neoplasms. Hum. Pathol. 2007, 38, 1361–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwiatkowski, D.J.; Wagle, N. mTOR Inhibitors in Cancer: What Can We Learn from Exceptional Responses? EBioMedicine 2015, 2, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Kwiatkowski, D.J.; Choueiri, T.K.; Fay, A.P.; Rini, B.I.; Thorner, A.R.; de Velasco, G.; Tyburczy, M.E.; Hamieh, L.; Albiges, L.; Agarwal, N.; et al. Mutations in TSC1, TSC2, and MTOR Are Associated with Response to Rapalogs in Patients with Metastatic Renal Cell Carcinoma. Clin. Cancer Res. 2016, 22, 2445–2452. [Google Scholar] [CrossRef] [Green Version]
- Badri, K.R.; Gao, L.; Hyjek, E.; Schuger, N.; Schuger, L.; Qin, W.; Chekaluk, Y.; Kwiatkowski, D.J.; Zhe, X. Exonic mutations of TSC2/TSC1 are common but not seen in all sporadic pulmonary lymphangioleiomyomatosis. Am. J. Respir. Crit. Care Med. 2013, 187, 663–665. [Google Scholar] [CrossRef]
- Pan, C.C.; Chung, M.Y.; Ng, K.F.; Liu, C.Y.; Wang, J.S.; Chai, C.Y.; Huang, S.H.; Chen, P.C.; Ho, D.M. Constant allelic alteration on chromosome 16p (TSC2 gene) in perivascular epithelioid cell tumour (PEComa): Genetic evidence for the relationship of PEComa with angiomyolipoma. J. Pathol. 2008, 214, 387–393. [Google Scholar] [CrossRef]
- Rutkowski, P.; Przybyl, J.; Switaj, T. Genetics of rare mesenchymal tumors: Implications for targeted treatment in DFSP, ASPS, CCS, GCTB and PEComa. Int. J. Biochem. Cell Biol. 2014, 53, 466–474. [Google Scholar] [CrossRef]
- Bissler, J.J.; McCormack, F.X.; Young, L.R.; Elwing, J.M.; Chuck, G.; Leonard, J.M.; Schmithorst, V.J.; Laor, T.; Brody, A.S.; Bean, J.; et al. Sirolimus for angiomyolipoma in tuberous sclerosis complex or lymphangioleiomyomatosis. N. Engl. J. Med. 2008, 358, 140–151. [Google Scholar] [CrossRef] [Green Version]
- Herry, I.; Neukirch, C.; Debray, M.P.; Mignon, F.; Crestani, B. Dramatic effect of sirolimus on renal angiomyolipomas in a patient with tuberous sclerosis complex. Eur. J. Intern. Med. 2007, 18, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Wienecke, R.; Fackler, I.; Linsenmaier, U.; Mayer, K.; Licht, T.; Kretzler, M. Antitumoral activity of rapamycin in renal angiomyolipoma associated with tuberous sclerosis complex. Am. J. Kidney Dis. 2006, 48, e27–e29. [Google Scholar] [CrossRef] [PubMed]
- Taille, C.; Debray, M.P.; Crestani, B. Sirolimus treatment for pulmonary lymphangioleiomyomatosis. Ann. Intern. Med. 2007, 146, 687–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, F.X.; Inoue, Y.; Moss, J.; Singer, L.G.; Strange, C.; Nakata, K.; Barker, A.F.; Chapman, J.T.; Brantly, M.L.; Stocks, J.M.; et al. Efficacy and safety of sirolimus in lymphangioleiomyomatosis. N. Engl. J. Med. 2011, 364, 1595–1606. [Google Scholar] [CrossRef]
- Bissler, J.J.; Budde, K.; Sauter, M.; Franz, D.N.; Zonnenberg, B.A.; Frost, M.D.; Belousova, E.; Berkowitz, N.; Ridolfi, A.; Christopher Kingswood, J. Effect of everolimus on renal function in patients with tuberous sclerosis complex: Evidence from EXIST-1 and EXIST-2. Nephrol. Dial. Transplant. 2019, 34, 1000–1008. [Google Scholar] [CrossRef]
- Bissler, J.J.; Kingswood, J.C.; Radzikowska, E.; Zonnenberg, B.A.; Belousova, E.; Frost, M.D.; Sauter, M.; Brakemeier, S.; de Vries, P.J.; Berkowitz, N.; et al. Everolimus long-term use in patients with tuberous sclerosis complex: Four-year update of the EXIST-2 study. PLoS ONE 2017, 12, e0180939. [Google Scholar] [CrossRef] [PubMed]
- Bissler, J.J.; Kingswood, J.C.; Radzikowska, E.; Zonnenberg, B.A.; Frost, M.; Belousova, E.; Sauter, M.; Nonomura, N.; Brakemeier, S.; de Vries, P.J.; et al. Everolimus for angiomyolipoma associated with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis (EXIST-2): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2013, 381, 817–824. [Google Scholar] [CrossRef]
- Giannella, L.; Delli Carpini, G.; Montik, N.; Verdecchia, V.; Puccio, F.; Di Giuseppe, J.; Tsiroglou, D.; Goteri, G.; Ciavattini, A. Ultrasound Features of a Uterine Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review. Diagnostics 2020, 10, 553. [Google Scholar] [CrossRef]
- Sobiborowicz, A.; Świtaj, T.; Teterycz, P.; Spałek, M.J.; Szumera-Ciećkiewicz, A.; Wągrodzki, M.; Zdzienicki, M.; Czarnecka, A.M.; Rutkowski, P. Feasibility and Long-Term Efficacy of PEComa Treatment—20 Years of Experience. J. Clin. Med. 2021, 10, 2200. [Google Scholar] [CrossRef]
- Benson, C.; Vitfell-Rasmussen, J.; Maruzzo, M.; Fisher, C.; Tunariu, N.; Mitchell, S.; Al-Muderis, O.; Thway, K.; Larkin, J.; Judson, I. A retrospective study of patients with malignant PEComa receiving treatment with sirolimus or temsirolimus: The Royal Marsden Hospital experience. Anticancer Res. 2014, 34, 3663–3668. [Google Scholar] [PubMed]
- Northrup, H.; Krueger, D.A.; International Tuberous Sclerosis Complex Consensus, G. Tuberous sclerosis complex diagnostic criteria update: Recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol 2013, 49, 243–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szumera-Cieækiewicz, A.; Kuczkiewicz-Siemion, O.; Seliga, K.; Grabowska-Kierył, M.; Tysarowski, A.; Wągrodzki, M.; Świtaj, T.; Prochorec-Sobieszek, M.; Rutkowski, P. Pigmented/melanocytic malignant perivascular epithelioid cell tumor with TFE3-SFPQ(PSF) rearrangement—A challenging diagnosis of PEComa family of tumors. Pol. J. Pat. hol. 2019, 70(4), 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruka, W.; Rutkowski, P.; Krzakowski, M.; Grzesiakowska, U.; Ptaszyński, K.; Jeziorski, A.; Polkowski, W.; Ryś, J.; Słuszniak, J.; Dziewirski, W.; et al. Soft tissue sarcoma—diagnosis and treatment. Onkol. Prak. Klin 2009, 5, 198–210. [Google Scholar]
- Ruka, W.; Rutkowski, P.; Krzakowski, M.; Grzesiakowska, U.; Ptaszyński, K.; Jeziorski, A.; Polkowski, W.; Ryś, J.; Słuszniak, J.; Dziewirski, W.; et al. Mięsaki tkanek miękkich u dorosłych—zasady postępowania diagnostyczno-terapeutycznego. Nowotw. J. Oncol. 2010, 60, 55. [Google Scholar]
- Rutkowski, P.; Ługowska, I.; Fijuth, J.; Jeziorski, A.; Ryś, J.; Wągrodzki, M.; Świtaj, T.; Koseła-Paterczyk, H.; Fonrobert, P.; Nowecki, Z.I.; et al. Soft tissue sarcomas in adults—guidelines for diagnostic and therapeutic management. Oncol. Clin. Pract. 2017, 13, 181–201. [Google Scholar] [CrossRef]
- MacDonald, A.; Scarola, J.; Burke, J.T.; Zimmerman, J.J. Clinical pharmacokinetics and therapeutic drug monitoring of sirolimus. Clin. Ther. 2000, 22 (Suppl. 2), B101–B121. [Google Scholar] [CrossRef]
- Raimondi, A.; Colombo, F.; Pintarelli, G.; Morosi, C.; Renne, S.L.; Frezza, A.M.; Saponara, M.; Dei Tos, A.P.; Mazzocchi, A.; Provenzano, S.; et al. Prolonged activity and toxicity of sirolimus in a patient with metastatic renal perivascular epithelioid cell tumor: A case report and literature review. Anticancer Drugs 2018, 29, 589–595. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Wickham, H. Easily Install and Load “Tidyverse” Packages; RStudio: Vienna, Austria, 2018. [Google Scholar]
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. Drawing Survival Curves Using “ggplot2.”; Survminer: Indianapolis, IN, USA, 2018. [Google Scholar]
- Sobiborowicz, A.; Czarnecka, A.M.; Szumera-Ciećkiewicz, A.; Rutkowski, P.; Świtaj, T. Diagnosis and treatment of lymphangioleiomyomatosis (LAM) from the PEComa group. Oncol. Clin. Pract. 2021, 17, 28–41. [Google Scholar] [CrossRef]
- Wagner, A.J.; Malinowska-Kolodziej, I.; Morgan, J.A.; Qin, W.; Fletcher, C.D.; Vena, N.; Ligon, A.H.; Antonescu, C.R.; Ramaiya, N.H.; Demetri, G.D.; et al. Clinical activity of mTOR inhibition with sirolimus in malignant perivascular epithelioid cell tumors: Targeting the pathogenic activation of mTORC1 in tumors. J. Clin. Oncol. 2010, 28, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Iwenofu, O.H.; Lackman, R.D.; Staddon, A.P.; Goodwin, D.G.; Haupt, H.M.; Brooks, J.S. Phospho-S6 ribosomal protein: A potential new predictive sarcoma marker for targeted mTOR therapy. Mod. Pathol. 2008, 21, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Z.F.; Yang, L.; Wang, T.T.; Han, P.; Liu, Z.H.; Wei, Q. Efficacy and safety of sirolimus for renal angiomyolipoma in patients with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis: A systematic review. J. Urol. 2014, 192, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.J.; Ravi, V.; Riedel, R.F.; Ganjoo, K.N.; Tine, B.A.V.; Chugh, R.; Cranmer, L.D.; Gordon, E.M.; Hornick, J.L.; Kwiatkowski, D.J.; et al. Long-term follow-up for duration of response (DoR) after weekly nab-sirolimus in patients with advanced malignant perivascular epithelioid cell tumors (PEComa): Results from a registrational open-label phase II trial, AMPECT. J. Clin. Oncol. 2020, 38, 11516. [Google Scholar] [CrossRef]
- Wagner, A.J.; Ravi, V.; Ganjoo, K.N.; Tine, B.A.V.; Riedel, R.F.; Chugh, R.; Cranmer, L.D.; Gordon, E.M.; Hornick, J.L.; Kwiatkowski, D.J.; et al. ABI-009 (nab-sirolimus) in advanced malignant perivascular epithelioid cell tumors (PEComa): Preliminary efficacy, safety, and mutational status from AMPECT, an open label phase II registration trial. J. Clin. Oncol. 2019, 37, 11005. [Google Scholar] [CrossRef]
- Hou, S.; Schmid, A.; Desai, N. Abstract 348: ABI-009 (nab-Sirolimus) improves tumor accumulation and antitumor activity over oral mTOR inhibitors. Exp. Mol. Ther. 2019, 79, 348. [Google Scholar] [CrossRef]
- Jimeno, A.; Rudek, M.A.; Kulesza, P.; Ma, W.W.; Wheelhouse, J.; Howard, A.; Khan, Y.; Zhao, M.; Jacene, H.; Messersmith, W.A.; et al. Pharmacodynamic-guided modified continuous reassessment method-based, dose-finding study of rapamycin in adult patients with solid tumors. J. Clin. Oncol. 2008, 26, 4172–4179. [Google Scholar] [CrossRef] [Green Version]
- Lurkin, A.; Ducimetiere, F.; Vince, D.R.; Decouvelaere, A.V.; Cellier, D.; Gilly, F.N.; Salameire, D.; Biron, P.; de Laroche, G.; Blay, J.Y.; et al. Epidemiological evaluation of concordance between initial diagnosis and central pathology review in a comprehensive and prospective series of sarcoma patients in the Rhone-Alpes region. BMC Cancer 2010, 10, 150. [Google Scholar] [CrossRef] [Green Version]
- Somcutian, O.; Buiga, R.; Galatir, M.; Tudor Eniu, D.; Rachieru, C.; Coza, D.; Terrier, P. Histopathological diagnostic concordance in bone and soft tissue sarcomas between two comprehensive cancer centers from eastern and western Europe: A collaborative experience. Ann. Pathol. 2015, 35, 32–40. [Google Scholar] [CrossRef]
- Folpe, A.L.; Mentzel, T.; Lehr, H.A.; Fisher, C.; Balzer, B.L.; Weiss, S.W. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: A clinicopathologic study of 26 cases and review of the literature. Am. J. Surg. Pathol. 2005, 29, 1558–1575. [Google Scholar] [CrossRef]
- Schoolmeester, J.K.; Howitt, B.E.; Hirsch, M.S.; Dal Cin, P.; Quade, B.J.; Nucci, M.R. Perivascular epithelioid cell neoplasm (PEComa) of the gynecologic tract: Clinicopathologic and immunohistochemical characterization of 16 cases. Am. J. Surg. Pathol. 2014, 38, 176–188. [Google Scholar] [CrossRef]
- Bao, L.; Shi, Y.; Zhong, J.; Zhao, M.; Wu, J.; Hai, L.; Xu, X.; Du, H.; Shi, Y. Histopathologic characteristics and immunotypes of perivascular epithelioid cell tumors (PEComa). Int. J. Clin. Exp. Pathol. 2019, 12, 4380–4389. [Google Scholar]
- Kwon, B.S.; Suh, D.S.; Lee, N.K.; Song, Y.J.; Choi, K.U.; Kim, K.H. Two cases of perivascular epithelioid cell tumor of the uterus: Clinical, radiological and pathological diagnostic challenge. Eur. J. Med. Res. 2017, 22, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirumani, S.H.; Shinagare, A.B.; Hargreaves, J.; Jagannathan, J.P.; Hornick, J.L.; Wagner, A.J.; Ramaiya, N.H. Imaging features of primary and metastatic malignant perivascular epithelioid cell tumors. AJR Am. J. Roentgenol. 2014, 202, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Stacchiotti, S.; Verderio, P.; Messina, A.; Morosi, C.; Collini, P.; Llombart-Bosch, A.; Martin, J.; Comandone, A.; Cruz, J.; Ferraro, A.; et al. Tumor response assessment by modified Choi criteria in localized high-risk soft tissue sarcoma treated with chemotherapy. Cancer 2012, 118, 5857–5866. [Google Scholar] [CrossRef]
- Bergamo, F.; Maruzzo, M.; Basso, U.; Montesco, M.C.; Zagonel, V.; Gringeri, E.; Cillo, U. Neoadjuvant sirolimus for a large hepatic perivascular epithelioid cell tumor (PEComa). World J. Surg. Oncol. 2014, 12, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No | Primary Site | PEComa Subtype | Previous Surgery | Line of Treatment | Previous Chemotherapy | Duration of Sirolimus Response | Best Response (RECIST) | Sirolimus Dose |
|---|---|---|---|---|---|---|---|---|
| 1 | Retroperitoneal | AML | Yes | 1 | NA | 55.7 | PR | 4 mg qd |
| 2 | Retroperitoneal | NOS | No | 2 | ADIC | 32 | PR | 3 mg qd |
| 3 | Abdomen | NOS | Yes | 1 | NA | 9.5 | SD | 6 mg qd |
| 4 | Genital | NOS | Yes | 1 | NA | 62.1 | CR | 4 mg qd |
| 5 | Genital | NOS | No | 2 | ADIC | 16 | PR | 5 mg qd |
| 6 | Genital | NOS | Yes | 2 | DDP + DOX | 9.2 | SD | 4 mg qd |
| 7 | Retroperitoneal | NOS | No | 1 | NA | 42 | PR | 4 mg qd |
| 8 | Visceral | AML | Yes | 1 | NA | 42.6 | CR | 4 mg qd |
| 9 | Trunk | LAM | No | 1 | NA | 25.3 | SD | 4 mg qd |
| 10 | Retroperitoneal | LAM | No | 1 | NA | 28.1 | PR | 4 mg qd |
| 11 | Abdomen | NOS | Yes | 4 | EP, ADIC, Gemcitabine | 21.9 | SD | 6 mg qd |
| 12 | Trunk | LAM | Yes | 1 | NA | 62.5 | CR | 4 mg qd |
| 13 | Trunk | NOS | Yes | 1 | NA | 15.8 | PR | 3 mg qd |
| 14 | Trunk | LAM | No | 1 | NA | 8.7 | PR | 3 mg qd |
| 15 | Retroperitoneal | NOS | No | 1 | NA | 4.7 | PR | 2 mg qd |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świtaj, T.; Sobiborowicz, A.; Teterycz, P.; Klimczak, A.; Makuła, D.; Wągrodzki, M.; Szumera-Ciećkiewicz, A.; Rutkowski, P.; Czarnecka, A.M. Efficacy of Sirolimus Treatment in PEComa–10 Years of Practice Perspective. J. Clin. Med. 2021, 10, 3705. https://doi.org/10.3390/jcm10163705
Świtaj T, Sobiborowicz A, Teterycz P, Klimczak A, Makuła D, Wągrodzki M, Szumera-Ciećkiewicz A, Rutkowski P, Czarnecka AM. Efficacy of Sirolimus Treatment in PEComa–10 Years of Practice Perspective. Journal of Clinical Medicine. 2021; 10(16):3705. https://doi.org/10.3390/jcm10163705
Chicago/Turabian StyleŚwitaj, Tomasz, Aleksandra Sobiborowicz, Paweł Teterycz, Anna Klimczak, Donata Makuła, Michał Wągrodzki, Anna Szumera-Ciećkiewicz, Piotr Rutkowski, and Anna M. Czarnecka. 2021. "Efficacy of Sirolimus Treatment in PEComa–10 Years of Practice Perspective" Journal of Clinical Medicine 10, no. 16: 3705. https://doi.org/10.3390/jcm10163705
APA StyleŚwitaj, T., Sobiborowicz, A., Teterycz, P., Klimczak, A., Makuła, D., Wągrodzki, M., Szumera-Ciećkiewicz, A., Rutkowski, P., & Czarnecka, A. M. (2021). Efficacy of Sirolimus Treatment in PEComa–10 Years of Practice Perspective. Journal of Clinical Medicine, 10(16), 3705. https://doi.org/10.3390/jcm10163705