
Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ)

 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scoring Materials and TMJ MRI Exams
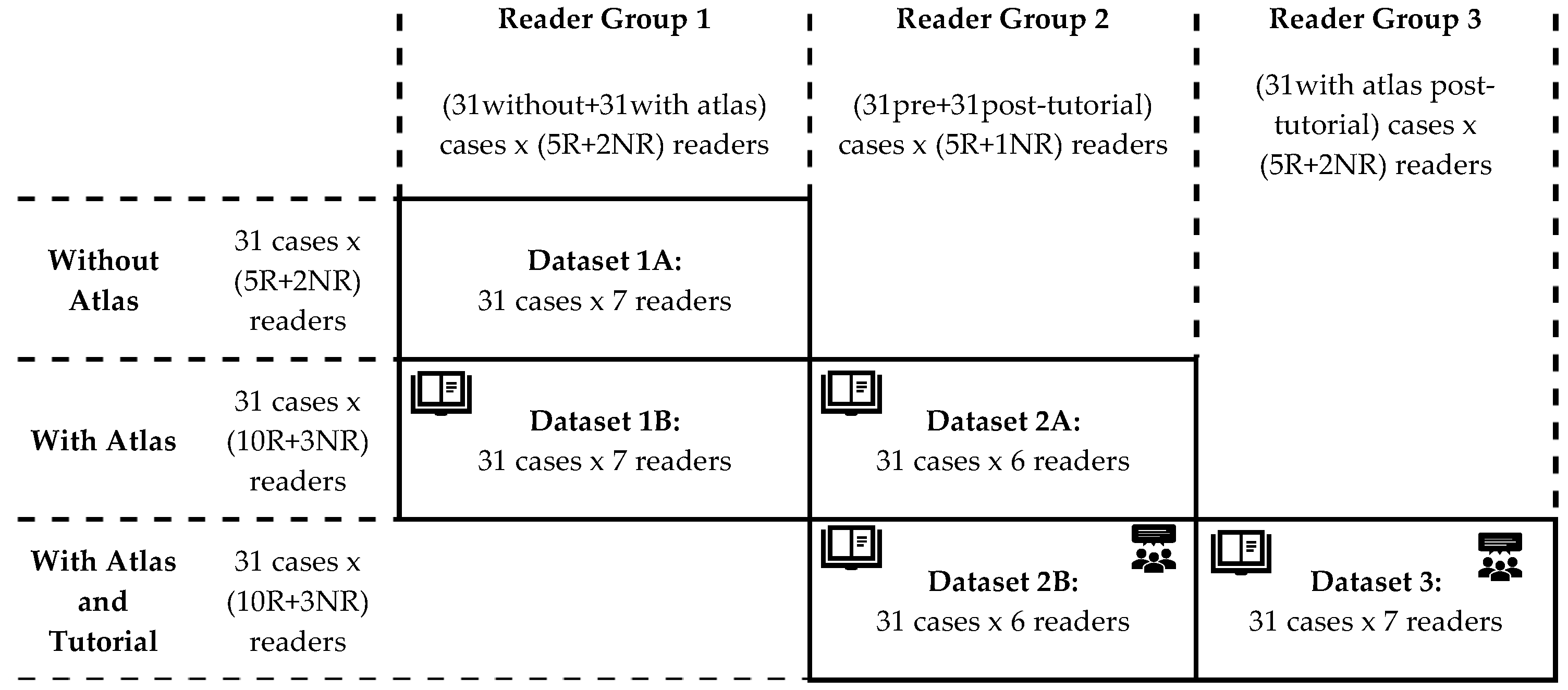
2.2. Reading Exercise and Data Structure
- Group 1 included five radiologists, one oral-maxillofacial surgeon, and one rheumatologist. These seven readers first scored the 31 cases with just the provided scoring system (dataset 1A), then scored the same cases again after 1–2 months, using the imaging atlas (dataset 1B).
- Group 2 included five radiologists and one oral-maxillofacial surgeon. These six readers first scored the same 31 cases using the scoring system and the atlas (dataset 2A), then scored the same cases again after 1–2 months, following a group calibration tutorial session (dataset 2B).
- Group 3 consisted of seven readers including 5 pediatric radiologists, 1 pediatric rheumatologist, and 1 orthodontist who also scored the same cases, but only once, after the group calibration session that was held together with the group 2 readers (dataset 3).
2.3. Data Analysis
- Combining the different calibration levels while keeping radiologist and non-radiologist groups separate, i.e., dataset 1A with 1B for +/−atlas, and 2A and 2B for +/−tutorial (vertical pooling on Figure 1).
- Combining the radiologist and non-radiologist data while keeping the calibration level separate, i.e., dataset 1B with 2A, and 2B with 3 (horizontal pooling on Figure 1).
2.4. Statistical Methods
3. Results
3.1. Two-Facet G Coefficients: Reliability by Subgroups of Measurement Aid and Reader Specialty
3.2. Multiway ANOVA: Contextual Impact of Calibration Level and Reader Specialty
3.3. Three-Facet G coefficients: Reliability When Variations in Calibration or Specialties Exist in the Dataset
3.4. Variation of Reliability by Study Design Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Background Information on Generalizability Theory as Applied to Imaging
Appendix B. JAMRIS-TMJ Scoring System

{kind=link}
{kind=link}
| INFLAMMATORY DOMAIN | |||||
| Definition | Bone Marrow Edema | Bone Marrow Enhancement | Effusion | Synovial Thickening | Joint Enhancement |
| Compared to the mandibular ramus, hyperintense marrow signaling within the condyle on T2w FS or STIR images, and/or hypointense signaling on pre-contrast T1w images without FS. | Compared to the mandibular ramus, hyperintense marrow signaling within the condyle on post-contrast T1w FS images. | Increased joint fluid with isointense signaling of joint space compared to that of cerebrospinal fluid on T2w FS or STIR images. | Thickened synovial lining of the TMJ with intermediate signal on T2w images. | Signal intensity of the synovium, capsule, and joint fluid higher than that of muscle on post-contrast T1w FS images. | |
| Grading | Absent | Absent | Normal: ≤1mm fluid in joint recess | Absent: No synovium visible (joint space ≤1 mm width) | Normal: High signal intensity confined to signal perimeter of normal amount of joint fluid on corresponding fluid-sensitive image |
| Present | Present | Small: >1 and ≤2mm fluid in recess or involving entire joint compartment | Mild: >1 and ≤2mm thickness at the point of maximum synovial thickening | Mild: High signal intensity focally exceeding signal perimeter of physiologic amount of joint fluid on corresponding fluid-sensitive image | |
| Large: >2mm fluid in recess or involving entire joint compartment | Moderate/Severe: >2mm thickness at the point of maximum synovial thickening | Moderate/Severe: High signal intensity diffusely involving one or both joint compartments | |||
| DAMAGE DOMAIN | |||||
| Definition | Condylar Flattening | Erosions | Disk Abnormalities | ||
| Loss of the round or slightly rectangular shape of the condylar head, viewed in the sagittal-oblique plane. | Any irregularity or breaks of the bony joint surfaces leading to the loss of the smooth continuous surface of the bone, seen in both sagittal and coronal planes | Any abnormality of the articular disk, including flattening, displacement, or destruction. | |||
| Grading | Normal round/slightly rectangular shape | No irregularities or deep breaks | Absent | ||
| Mild: Extent of flattening involves part of the surface of the condyle | Mild: Presence of irregularities involving only part of the articular surface of the condyle | Present | |||
| Moderate/Severe: Extent of flattening involves the entire surface of the condyle, or loss of height in the condyle. | Moderate/Severe: Presence of deep breaks in the subchondral bone seen in two planes, or irregularities involving the entire articular surface of the condyle | ||||
Appendix C. Imaging Protocol
| Imaging Sequence (in Order of Acquisition from Left to Right) | ||||||
|---|---|---|---|---|---|---|
| T1 FSPGR | PD FSE | T2 FSE FS | T1 FSE FS + Gd | T1 SE FS + Gd | 3D FSPGR + Gd | |
| Plane | Sagittal oblique | Sagittal oblique | Sagittal oblique | Sagittal oblique | Coronal | Sagittal oblique |
| Echo time (ms) | 4.2 | 25 | 86 | 11 | 19 | 10.4 |
| Repetition time (ms) | 325 | 2660 | 2840 | 600 | 600 | 4.2 |
| Flip angle | 80 | 90 | 90 | 90 | 90 | 20 |
| FOV (mm × mm) | 120 | 120 | 120 | 120 | 160 | 100 |
| Acquisition Matrix | 384 × 224 | 256 × 224 | 256 × 224 | 256 × 224 | 256 × 192 | 256 × 192 |
| Slice thickness (mm) | 2 | 2 | 2 | 2 | 2 | 2 |
| Slice spacing (mm) | 2 | 2 | 2 | 2 | 2 | 1 |
| Echo train length | - | 8 | 16 | 3 | - | - |
Appendix D. Generalizability Coefficient Formulae
| Coefficient Meaning | Formula |
|---|---|
| J:P × R × A Design—Pooling Across Use or Disuse of Aid, Separately for Radiologist and Non-Radiologist Readers | |
| Between readers of the same calibration (R random, P and A fixed) | |
| Same reader with vs. without aid (A random, P and R fixed) | |
| Between readers with different calibration (A and R random, P fixed) | |
| Between readers with different calibration, averaging 2 readings per reader (A and R random, P fixed, A/2) | |
| Between readers with different calibration, averaging 2 readers at a time (A and R random, P fixed, R/2) | |
| Between readers of the same calibration, averaging two readers at a time (R random, P and A fixed, R/2) | |
| Right-left joint agreement when scored by different readers with different calibration (J, A and R random) | |
| Right-left joint agreement when scored by the same reader with the same calibration (J random, A and R fixed) | |
| J:P × R:S Design—Pooling Across Radiologist and Non-Radiologist Readers, Separately for Each Aid | |
| Between radiologists and non-radiologists (R and S random, P fixed) | |
| Between readers of the same specialty (R random, S and P fixed) | |
| Right-left joint agreement when scored by radiologist and non-radiologist (J, S and R random) | |
| Right-left joint agreement when scored by the same reader (J random, R and S fixed) | |
Appendix E. Multiway ANOVA Results
| J:P × R × A Design | Inflammatory Domain | Damage Domain | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atlas Radiologists | Atlas Non-Radiologists | Tutorial Radiologists | Atlas Radiologists | Atlas Non-Radiologists | Tutorial Radiologists | |||||||
| Variance Component | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p |
| Joint (patient) | 44% | <0.0001 | 27% | 0.00 | 46% | <0.0001 | 40% | <0.0001 | 24% | 0.00 | 46% | <0.0001 |
| Patient | 20% | 0.05 | 14% | 0.11 | 27% | 0.02 | 38% | 0.00 | 23% | 0.01 | 34% | 0.01 |
| Reader | 8% | 0.03 | 0% | 0.30 | 3% | 0.06 | 0% | 0.91 | 19% | 0.00 | 4% | 0.05 |
| Aid | 0% | 0.41 | 2% | 0.40 | 3% | 0.04 | 1% | 0.19 | 1% | . | 0% | 0.44 |
| Reader*joint (patient) | 4% | <0.0001 | 16% | 0.00 | 1% | 0.16 | 0% | 0.66 | 4% | 0.14 | 0% | 0.32 |
| Aid*joint (patient) | 0% | 0.75 | 5% | 0.09 | 0% | 0.34 | 0% | 0.86 | 2% | 0.29 | 0% | 0.93 |
| Reader*Patient | 2% | 0.13 | 1% | 0.45 | 5% | 0.00 | 0% | 0.43 | 3% | 0.25 | 3% | 0.00 |
| Aid*patient | 0% | 0.63 | 0% | 0.91 | 0% | 0.34 | 1% | 0.19 | 0% | 0.74 | 0% | 0.33 |
| Aid*reader | 2% | 0.00 | 0% | 0.34 | 1% | 0.00 | 1% | 0.00 | 0% | 0.98 | 2% | <0.0001 |
| Aid*reader*patient | 13% | <0.0001 | 18% | 0.00 | 8% | <0.0001 | 6% | <0.0001 | 7% | 0.06 | 4% | <0.0001 |
| Residual | 8% | . | 17% | . | 7% | . | 12% | . | 18% | . | 7% | . |
| J:P × R:S Design | Baseline | Atlas | Atlas+Tutorial | Baseline | Atlas | Atlas+Tutorial | ||||||
| Variance Component | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p | Var Comp | p |
| Joint (patient) | 38% | <0.0001 | 35% | <0.0001 | 38% | <0.0001 | 34% | <0.0001 | 36% | <0.0001 | 43% | <0.0001 |
| Patient | 11% | 0.13 | 24% | 0.01 | 27% | 0.01 | 35% | 0.00 | 32% | 0.01 | 29% | 0.01 |
| Reader (specialty) | 5% | <0.0001 | 7% | <0.0001 | 6% | <0.0001 | 5% | <0.0001 | 5% | <0.0001 | 4% | <0.0001 |
| Specialty | 9% | 0.07 | 1% | 0.21 | 0% | 0.84 | 0% | 0.79 | 0% | 0.33 | 1% | 0.19 |
| Patient*specialty | 0% | 0.88 | 0% | 0.53 | 1% | 0.31 | 3% | 0.08 | 0% | 0.84 | 1% | 0.15 |
| Patient*reader (specialty) | 19% | <0.0001 | 15% | <0.0001 | 11% | <0.0001 | 9% | <0.0001 | 7% | <0.0001 | 8% | <0.0001 |
| Specialty*joint (patient) | 2% | 0.07 | 5% | <0.0001 | 3% | 0.01 | 2% | 0.05 | 7% | <0.0001 | 2% | 0.00 |
| Residual | 16% | . | 13% | . | 15% | . | 12% | . | 14% | . | 11% | . |
References
- Larheim, T.A.; Doria, A.S.; Kirkhus, E.; Parra, D.A.; Kellenberger, C.J.; Arvidsson, L.Z. TMJ Imaging in JIA Patients—An Overview. Semin. Orthod. 2015, 21, 102–110. [Google Scholar] [CrossRef]
- Billiau, A.D.; Hu, Y.; Verdonck, A.; Carels, C.; Wouters, C. Temporomandibular Joint Arthritis in Juvenile Idiopathic Arthritis: Prevalence, Clinical and Radiological Signs, and Relation to Dentofacial Morphology. J. Rheumatol. 2007, 34, 1925–1933. [Google Scholar]
- Weiss, P.F.; Arabshahi, B.; Johnson, A.; Bilaniuk, L.T.; Zarnow, D.; Cahill, A.M.; Feudtner, C.; Cron, R.Q. High Prevalence of Temporomandibular Joint Arthritis at Disease Onset in Children with Juvenile Idiopathic Arthritis, as Detected by Magnetic Resonance Imaging but Not by Ultrasound. Arthritis Rheum. 2008, 58, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, E.; Schroeder, S.; Müller, L.M.; Kellenberger, C.J.; Saurenmann, R.K. Temporomandibular Joint Involvement in Children with Juvenile Idiopathic Arthritis. J. Rheumatol. 2011, 38, 510–515. [Google Scholar] [CrossRef] [Green Version]
- Larheim, T.A.; Hoyeraal, H.M.; Stabrun, A.E.; Haanaes, H.R. The Temporomandibular Joint in Juvenile Rheumatoid Arthritis. Radiographic Changes Related to Clinical and Laboratory Parameters in 100 Children. Scand. J. Rheumatol. 1982, 11, 5–12. [Google Scholar] [CrossRef]
- Karhulahti, T.; Rönning, O.; Jämsä, T. Mandibular Condyle Lesions, Jaw Movements, and Occlusal Status in 15-Year-Old Children with Juvenile Rheumatoid Arthritis. Scand. J. Dent. Res. 1990, 98, 17–26. [Google Scholar] [CrossRef]
- Svensson, B.; Adell, R.; Kopp, S. Temporomandibular Disorders in Juvenile Chronic Arthritis Patients. A Clinical Study. Swed Dent. J. 2000, 24, 83–92. [Google Scholar] [PubMed]
- Twilt, M.; Mobers, S.M.L.M.; Arends, L.R.; ten Cate, R.; Suijlekom-Smit, L. van Temporomandibular Involvement in Juvenile Idiopathic Arthritis. J. Rheumatol. 2004, 31, 1418–1422. [Google Scholar] [PubMed]
- Schanberg, L.E.; Anthony, K.K.; Gil, K.M.; Maurin, E.C. Daily Pain and Symptoms in Children with Polyarticular Arthritis. Arthritis Rheum. 2003, 48, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Goldmuntz, E.A.; White, P.H. Juvenile Idiopathic Arthritis: A Review for the Pediatrician. Pediatr. Rev. 2006, 27, e24–e32. [Google Scholar] [CrossRef]
- Muller, L.; Kellenberger, C.J.; Cannizzaro, E.; Ettlin, D.; Schraner, T.; Bolt, I.B.; Peltomaki, T.; Saurenmann, R.K. Early Diagnosis of Temporomandibular Joint Involvement in Juvenile Idiopathic Arthritis: A Pilot Study Comparing Clinical Examination and Ultrasound to Magnetic Resonance Imaging. Rheumatology 2009, 48, 680–685. [Google Scholar] [CrossRef] [Green Version]
- Zwir, L.F.; Terreri, M.T.; do Amaral e Castro, A.; Rodrigues, W.D.R.; Fernandes, A.R.C. Is Power Doppler Ultrasound Useful to Evaluate Temporomandibular Joint Inflammatory Activity in Juvenile Idiopathic Arthritis? Clin. Rheumatol. 2020, 39, 1237–1240. [Google Scholar] [CrossRef]
- Rongo, R.; Alstergren, P.; Ammendola, L.; Bucci, R.; Alessio, M.; D’Antò, V.; Michelotti, A. Temporomandibular Joint Damage in Juvenile Idiopathic Arthritis: Diagnostic Validity of Diagnostic Criteria for Temporomandibular Disorders. J. Oral Rehabil. 2019, 46, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Bernini, J.M.; Kellenberger, C.J.; Eichenberger, M.; Eliades, T.; Papageorgiou, S.N.; Patcas, R. Quantitative Analysis of Facial Asymmetry Based on Three-Dimensional Photography: A Valuable Indicator for Asymmetrical Temporomandibular Joint Affection in Juvenile Idiopathic Arthritis Patients? Pediatr. Rheumatol. Online J. 2020, 18, 1–8. [Google Scholar] [CrossRef]
- Bollhalder, A.; Patcas, R.; Eichenberger, M.; Müller, L.; Schroeder-Kohler, S.; Saurenmann, R.K.; Kellenberger, C.J. Magnetic Resonance Imaging Followup of Temporomandibular Joint Inflammation, Deformation, and Mandibular Growth in Juvenile Idiopathic Arthritis Patients Receiving Systemic Treatment. J. Rheumatol. 2020, 47, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Tolend, M.A.; Twilt, M.; Cron, R.Q.; Tzaribachev, N.; Guleria, S.; von Kalle, T.; Koos, B.; Miller, E.; Stimec, J.; Vaid, Y.; et al. Toward Establishing a Standardized Magnetic Resonance Imaging Scoring System for Temporomandibular Joints in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2018, 70, 758–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolend, M.; Junhasavasdikul, T.; Cron, R.Q.; Clemente, E.J.I.; von Kalle, T.; Kellenberger, C.J.; Koos, B.; Miller, E.; van Rossum, M.A.; Saurenmann, R.K.; et al. Discrete Choice Experiment on a Magnetic Resonance Imaging Scoring System for Temporomandibular Joints in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Maxwell, L.J.; Shea, B.J.; Wells, G.A.; Boers, M.; Grosskleg, S.; Bingham, C.O.; Conaghan, P.G.; D’Agostino, M.A.; de Wit, M.P.; et al. Instrument Selection Using the OMERACT Filter 2.1: The OMERACT Methodology. J. Rheumatol. 2019, 46, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Kellenberger, C.J.; Junhasavasdikul, T.; Tolend, M.; Doria, A.S. Temporomandibular Joint Atlas for Detection and Grading of Juvenile Idiopathic Arthritis Involvement by Magnetic Resonance Imaging. Pediatr. Radiol. 2018, 48, 411–426. [Google Scholar] [CrossRef] [Green Version]
- Bloch, R.; Norman, G. Generalizability Theory for the Perplexed: A Practical Introduction and Guide: AMEE Guide No. 68. Med. Teach. 2012, 34, 960–992. [Google Scholar] [CrossRef]
- Brennan, R.L. Generalizability Theory; Statistics for Social and Behavioral Sciences; Springer: New York, NY, USA, 2001; ISBN 978-0-387-95282-6. [Google Scholar]
- Doros, G.; Lew, R. Design Based on Intra-Class Correlation Coefficients. Am. J. Biostat. 2010, 1, 1–8. [Google Scholar]
- Giraudeau, B.; Mary, J.Y. Planning a Reproducibility Study: How Many Subjects and How Many Replicates per Subject for an Expected Width of the 95 per Cent Confidence Interval of the Intraclass Correlation Coefficient. Stat. Med. 2001, 20, 3205–3214. [Google Scholar] [CrossRef]
- Vaid, Y.N.; Dunnavant, F.D.; Royal, S.A.; Beukelman, T.; Stoll, M.L.; Cron, R.Q. Imaging of the Temporomandibular Joint in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2014, 66, 47–54. [Google Scholar] [CrossRef]
- Koos, B.; Tzaribachev, N.; Bott, S.; Ciesielski, R.; Godt, A. Classification of Temporomandibular Joint Erosion, Arthritis, and Inflammation in Patients with Juvenile Idiopathic Arthritis. J. Orofac. Orthop. 2013, 74, 506–519. [Google Scholar] [CrossRef]
- Peacock, Z.S.; Vakilian, P.; Caruso, P.; Resnick, C.M.; Vangel, M.; Kaban, L.B. Quantifying Synovial Enhancement of the Pediatric Temporomandibular Joint. J. Oral Maxillofac. Surg. 2016, 74, 1937–1945. [Google Scholar] [CrossRef]
- Resnick, C.M.; Vakilian, P.M.; Kaban, L.B.; Peacock, Z.S. Quantifying the Effect of Temporomandibular Joint Intra-Articular Steroid Injection on Synovial Enhancement in Juvenile Idiopathic Arthritis. J. Oral Maxillofac. Surg. 2016, 74, 2363–2369. [Google Scholar] [CrossRef] [PubMed]
- Caruso, P.; Buch, K.; Rincon, S.; Hakimelahi, R.; Peacock, Z.S.; Resnick, C.M.; Foster, C.; Guidoboni, L.; Donahue, T.; Macdonald, R.; et al. Optimization of Quantitative Dynamic Postgadolinium MRI Technique Using Normalized Ratios for the Evaluation of Temporomandibular Joint Synovitis in Patients with Juvenile Idiopathic Arthritis. Am. J. Neuroradiol. 2017, 38, 2344–2350. [Google Scholar] [CrossRef] [Green Version]


| Clinical Characteristics of Patient Sample | |
|---|---|
| Age at diagnosis (years) | 8.0 (SD 4.5, range 0.5–15.3) |
| Age at MRI (years) | 11.6 (SD 3.0, range 6.2–16.9) |
| Disease duration (years) | 3.6 (SD 4.4, range 6.8–15.7) |
| Sex | 5 male, 26 female |
| JIA subtype | |
| Oligoarticular | 12 |
| Oligoarticular extended | 5 |
| Polyarticular | 9 (all RF−) |
| Enthesitis related | 1 |
| Psoriatic arthritis | 1 |
| Undifferentiated | 1 |
| No JIA diagnosis | 2 |
| HLA-B27+ (n tested, % of tested) | 1 (19, 5%) |
| ANA+ | 18 (58%) |
| RF+ (n tested, % of tested) | 1 (30, 3%) |
| Uveitis | 7 (23%) |
| Facial changes (including asymmetry, decreased condylar translation, retrognathia) | 19 (61%) |
| Crepitation | 4 (13%) |
| Decreased mouth opening (<10th percentile) | 10 (32%) |
| TMJ pain | 7 (23%) |
| Active treatment (including NSAIDs, DMARDs, anti-TNF, etc.) | 20 (65%) |
| History of DMARD use (past and/or current) | 15 (48%) |
| Inter-Reader Absolute Agreement Reliability | Generalizability Coefficient | 95% CI of Score (+/− Percentage Points) | ||||
|---|---|---|---|---|---|---|
| Baseline | Atlas | Atlas + Tutorial | Baseline | Atlas | Atlas + Tutorial | |
| Inflammatory domain | ||||||
| Radiologists (n = 5, 10, 10) | 0.71 | 0.73 | 0.73 | 27 | 26 | 25 |
| Non-radiologist clinicians (n = 2, 3, 3) | 0.49 | 0.53 | 0.45 | 35 | 30 | 37 |
| All readers (n = 7, 13, 13) | 0.61 | 0.66 | 0.67 | 32 | 28 | 28 |
| Damage domain | ||||||
| Radiologists (n = 5, 10, 10) | 0.76 | 0.77 | 0.77 | 24 | 25 | 25 |
| Non-radiologist clinicians (n = 2, 3, 3) | 0.44 | 0.46 | 0.70 | 42 | 42 | 28 |
| All readers (n = 7, 13, 13) | 0.68 | 0.66 | 0.74 | 29 | 31 | 27 |
| Pooling the Two Readings from the Same Readers | Generalizability Coefficient | 95% CI of Measurement (+/− Percentage Points) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inflammatory Domain | Damage Domain | Inflammatory Domain | Damage Domain | |||||||||
| Measurement Scenario (Main Effects Definitions) | +/− Atlas | Atlas +/− Tutorial Rad | +/− Atlas | Atlas +/− Tutorial Rad | +/− Atlas | Atlas +/− Tutorial Rad | +/− Atlas | Atlas +/− Tutorial Rad | ||||
| Non-Rad | Rad | Non-Rad | Rad | Non-Rad | Rad | Non-Rad | Rad | |||||
| Between readers of the same calibration (R random, P and A fixed) | 0.49 | 0.69 | 0.81 | 0.39 | 0.78 | 0.80 | 35 | 28 | 21 | 47 | 24 | 23 |
| Same reader with vs. without aid (A random, P and R fixed) | 0.65 | 0.86 | 0.83 | 0.59 | 0.77 | 0.88 | 29 | 17 | 20 | 33 | 24 | 18 |
| Between readers with different calibration (A and R random, P fixed) | 0.41 | 0.67 | 0.75 | 0.37 | 0.76 | 0.78 | 37 | 29 | 25 | 48 | 25 | 25 |
| Between readers with different calibration, averaging two readings per reader (A and R random, P fixed, A/2) | 0.50 | 0.73 | 0.83 | 0.43 | 0.86 | 0.84 | 31 | 26 | 20 | 42 | 18 | 20 |
| Between readers with different calibration, averaging two readers at a time (A and R random, P fixed, R/2) | 0.56 | 0.81 | 0.84 | 0.53 | 0.86 | 0.88 | 28 | 21 | 19 | 35 | 18 | 17 |
| Between readers of the same calibration, averaging two readers at a time (R random, P and A fixed, R/2) | 0.65 | 0.82 | 0.90 | 0.56 | 0.87 | 0.89 | 25 | 20 | 15 | 34 | 17 | 16 |
| Between right and left joints when scored by different readers with different calibration (J, A and R random) | 0.12 | 0.20 | 0.27 | 0.23 | 0.39 | 0.34 | 54 | 56 | 55 | 65 | 54 | 56 |
| Between right and left joints when scored by the same reader with the same calibration (J random, A and R fixed) | 0.30 | 0.39 | 0.43 | 0.39 | 0.47 | 0.44 | 48 | 47 | 47 | 51 | 50 | 50 |
| Pooling the Readings from Same Calibration | Generalizability Coefficient | 95% CI of Measurement | ||||||||||
| Measurement Scenario (Main Effects Definitions) | Inflammatory Domain | Damage Domain | Inflammatory Domain | Damage Domain | ||||||||
| Baseline | Atlas | Tutorial | Baseline | Baseline | Atlas | Tutorial | Baseline | Baseline | Atlas | Tutorial | Baseline | |
| Between radiologists and non-radiologists (R and S random, P fixed) | 0.56 | 0.59 | 0.63 | 0.64 | 0.61 | 0.70 | 36 | 31 | 29 | 30 | 33 | 28 |
| Between readers of the same specialty (R random, S and P fixed) | 0.67 | 0.69 | 0.67 | 0.68 | 0.70 | 0.76 | 29 | 27 | 28 | 29 | 29 | 26 |
| Between right and left joints when scored by a radiologist and a clinician (J, R and S random) | 0.12 | 0.25 | 0.26 | 0.35 | 0.32 | 0.30 | 60 | 53 | 53 | 56 | 55 | 56 |
| Between right and left joints when scored by the same reader (J random, R and S fixed) | 0.34 | 0.43 | 0.40 | 0.49 | 0.41 | 0.42 | 48 | 45 | 46 | 49 | 50 | 50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tolend, M.; Doria, A.S.; Meyers, A.B.; Larheim, T.A.; Abramowicz, S.; Aguet, J.; Appenzeller, S.; Arvidsson, L.Z.; Averill, L.W.; Feldman, B.M.; et al. Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ). J. Clin. Med. 2021, 10, 4047. https://doi.org/10.3390/jcm10184047
Tolend M, Doria AS, Meyers AB, Larheim TA, Abramowicz S, Aguet J, Appenzeller S, Arvidsson LZ, Averill LW, Feldman BM, et al. Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ). Journal of Clinical Medicine. 2021; 10(18):4047. https://doi.org/10.3390/jcm10184047
Chicago/Turabian StyleTolend, Mirkamal, Andrea S. Doria, Arthur B. Meyers, Tore A. Larheim, Shelly Abramowicz, Julien Aguet, Simone Appenzeller, Linda Z. Arvidsson, Lauren W. Averill, Brian M. Feldman, and et al. 2021. "Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ)" Journal of Clinical Medicine 10, no. 18: 4047. https://doi.org/10.3390/jcm10184047
APA StyleTolend, M., Doria, A. S., Meyers, A. B., Larheim, T. A., Abramowicz, S., Aguet, J., Appenzeller, S., Arvidsson, L. Z., Averill, L. W., Feldman, B. M., Guleria, S., Inarejos Clemente, E. J., Jaremko, J. L., Junhasavasdikul, T., von Kalle, T., Kirkhus, E., Koos, B., Miller, E., Moineddin, R., ... Kellenberger, C. J. (2021). Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ). Journal of Clinical Medicine, 10(18), 4047. https://doi.org/10.3390/jcm10184047