Aorto-Iliac Artery Calcification and Graft Outcomes in Kidney Transplant Recipients

 ,
, 
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Computed Tomography (CT) Assessment of Aorto-Iliac Calcification
2.3. Clinical Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics and Short-Term Graft Outcomes
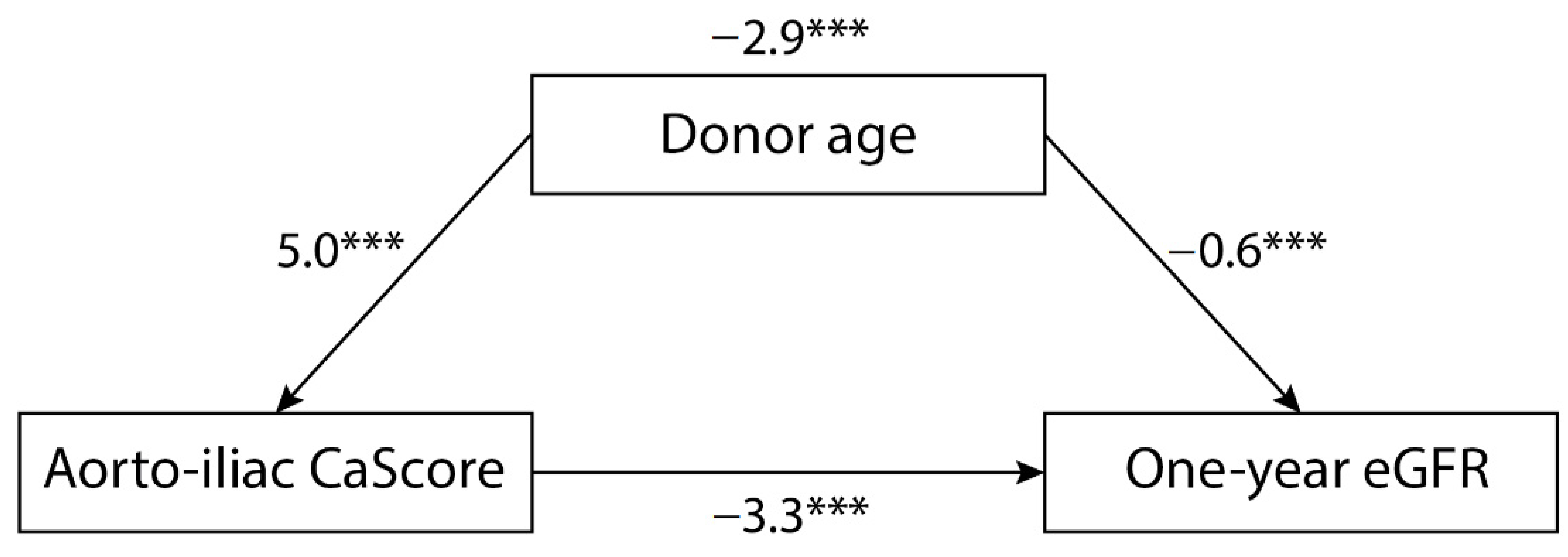
3.2. Aorto-Iliac Calcification Score (CaScore) and One-Year Kidney Transplant Function
3.3. Aorto-Iliac CaScore and Death-Censored Graft Failure
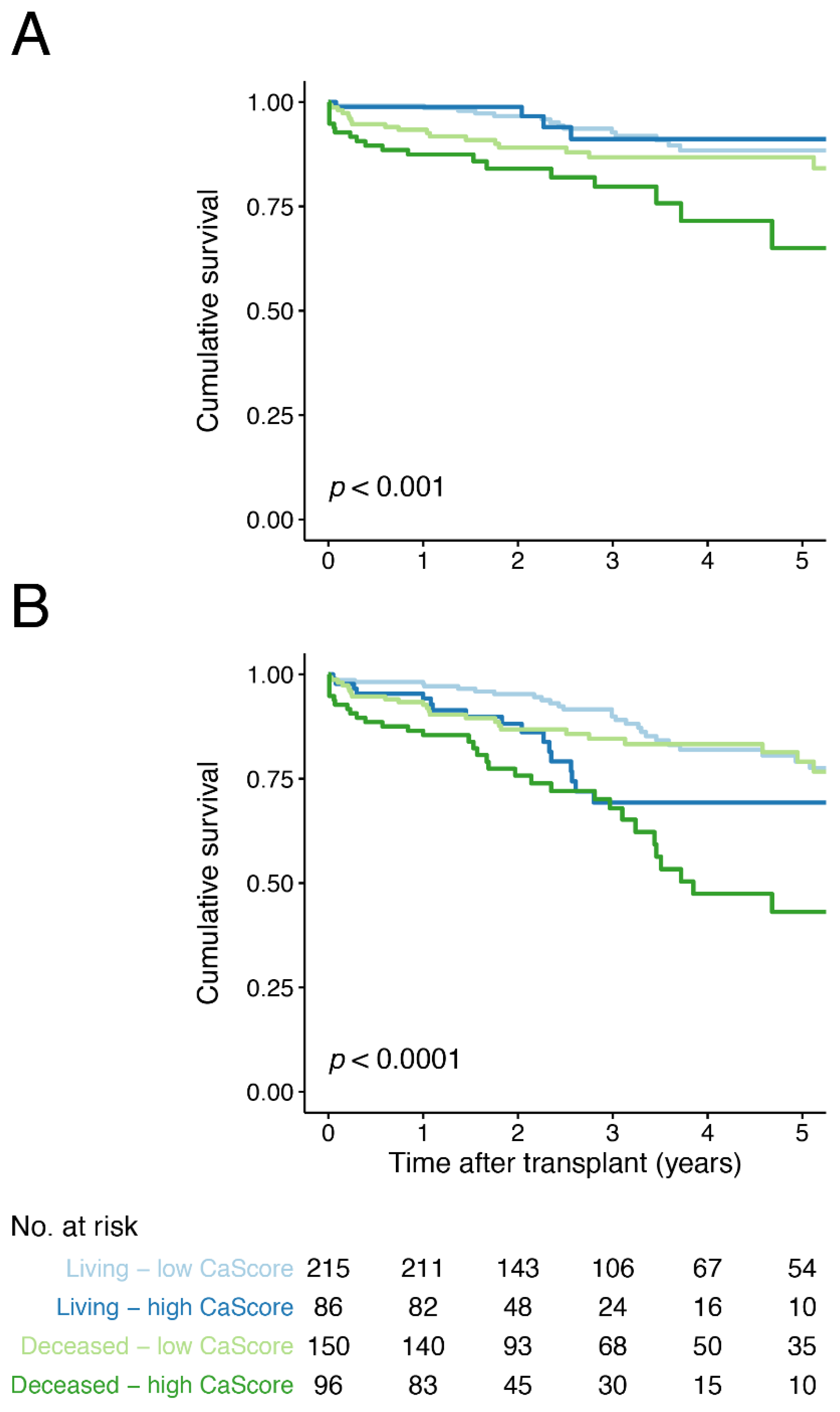
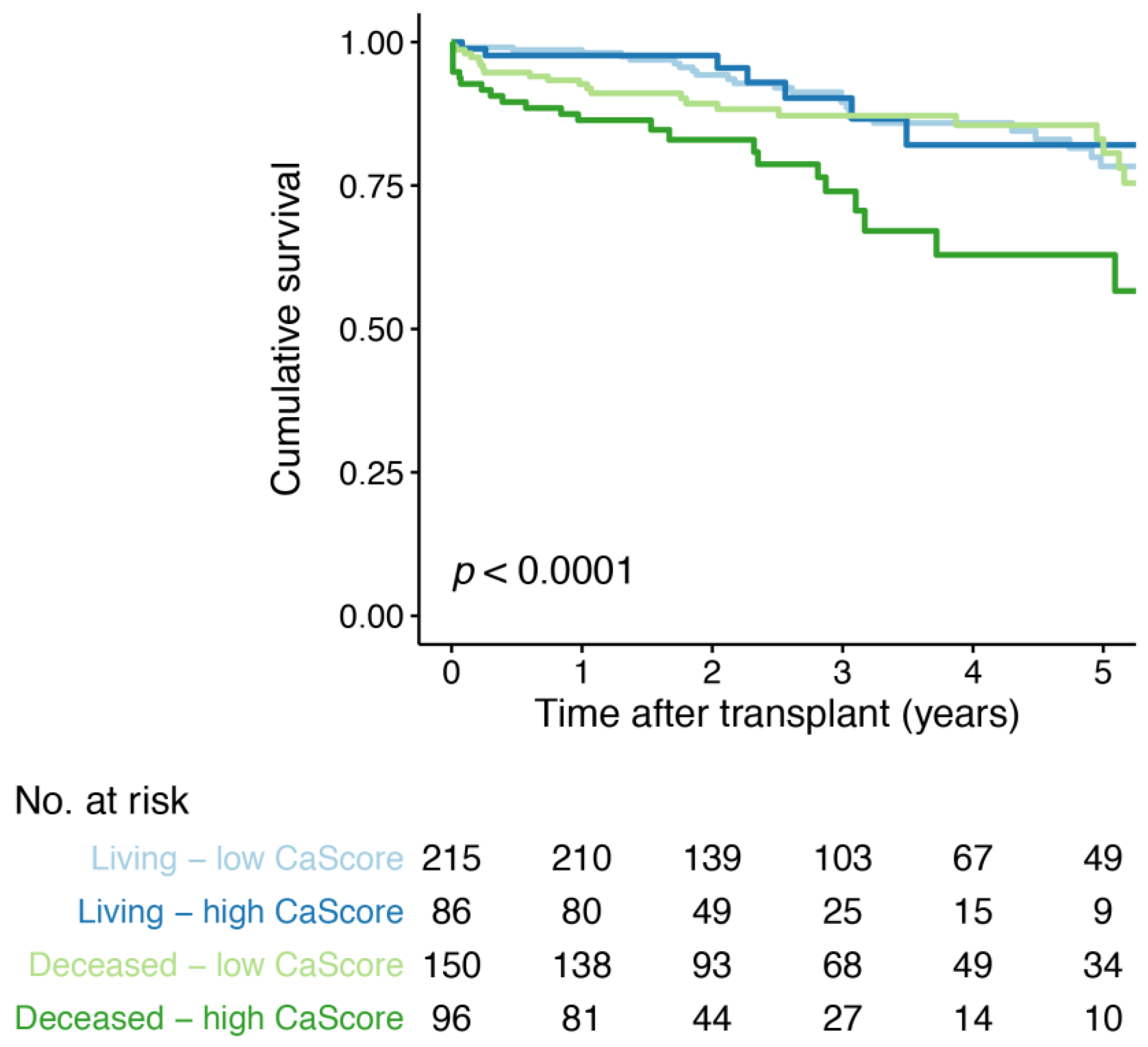
3.4. Aorto-Iliac CaScore and Overall Graft Failure
3.5. Aorto-Iliac CaScore and Death with a Functioning Graft
3.6. Aorto-Iliac CaScore and Graft Function Decline
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamens, S.; Rijkse, E.; te Velde-Keyzer, C.A.; Berger, S.P.; Moers, C.; de Borst, M.H.; Yakar, D.; Slart, R.H.J.A.; Dor, F.J.M.F.; Minnee, R.C.; et al. Aorto-iliac artery calcification prior to kidney transplantation. J. Clin. Med. 2020, 9, 2893. [Google Scholar] [CrossRef] [PubMed]
- Rangaswami, J.; Mathew, R.O.; Parasuraman, R.; Tantisattamo, E.; Lubetzky, M.; Rao, S.; Yaqub, M.S.; Birdwell, K.A.; Bennett, W.; Dalal, P.; et al. Cardiovascular disease in the kidney transplant recipient: Epidemiology, diagnosis and management strategies. Nephrol. Dial. Transpl. 2019, 34, 760–773. [Google Scholar] [CrossRef] [PubMed]
- Cianciolo, G.; Capelli, I.; Angelini, M.L.; Valentini, C.; Baraldi, O.; Scolari, M.P.; Stefoni, S. Importance of vascular calcification in kidney transplant recipients. Am. J. Nephrol. 2014, 39, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Hamed, M.O.; Chen, Y.; Pasea, L.; Watson, C.J.; Torpey, N.; Bradley, J.A.; Pettigrew, G.; Saeb-Parsy, K. Early graft loss after kidney transplantation: Risk factors and consequences. Am. J. Transpl. 2015, 15, 1632–1643. [Google Scholar] [CrossRef] [PubMed]
- De Vusser, K.; Lerut, E.; Kuypers, D.; Vanrenterghem, Y.; Jochmans, I.; Monbaliu, D.; Pirenne, J.; Naesens, M. The predictive value of kidney allograft baseline biopsies for long-term graft survival. J. Am. Soc. Nephrol. 2013, 24, 1913–1923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issa, N.; Lopez, C.L.; Denic, A.; Taler, S.J.; Larson, J.J.; Kremers, W.K.; Ricaurte, L.; Merzkani, M.A.; Alexander, M.P.; Chakkera, H.A.; et al. Kidney structural features from living donors predict graft failure in the recipient. J. Am. Soc. Nephrol. 2020, 31, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Burton, H.; Iyamu Perisanidou, L.; Steenkamp, R.; Evans, R.; Mumford, L.; Evans, K.M.; Caskey, F.J.; Hilton, R. Causes of renal allograft failure in the UK: Trends in uk renal registry and national health service blood and transplant data from 2000 to 2013. Nephrol. Dial. Transpl. 2019, 34, 355–364. [Google Scholar] [CrossRef]
- Naesens, M.; Kuypers, D.R.J.; de Vusser, K.; Evenepoel, P.; Claes, K.; Bammens, B.; Meijers, B.; Sprangers, B.; Pirenne, J.; Monbaliu, D.; et al. The histology of kidney transplant failure: A long-term follow-up study. Transplantation 2014, 98, 427–435. [Google Scholar] [CrossRef]
- Van Loon, E.; Senev, A.; Lerut, E.; Coemans, M.; Callemeyn, J.; Van Keer, J.M.; Daniëls, L.; Kuypers, D.; Sprangers, B.; Emonds, M.-P.; et al. Assessing the complex causes of kidney allograft loss. Transplantation 2020, 104. [Google Scholar] [CrossRef]
- Van Loon, E.; Bernards, J.; van Craenenbroeck, A.H.; Naesens, M. The causes of kidney allograft failure: More than alloimmunity. Transplantation 2020, 104, e46–e56. [Google Scholar] [CrossRef]
- Lamb, K.E.; Lodhi, S.; Meier-Kriesche, H.-U. Long-term renal allograft survival in the United States: A critical reappraisal. Am. J. Transpl. 2011, 11, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Gomes-Neto, A.W.; Eisenga, M.F.; Nolte, I.M.; Anderson, J.L.; de Borst, M.H.; Osté, M.C.; Rodrigo, R.; Gans, R.O.; Berger, S.P.; et al. Consumption of fruits and vegetables and cardiovascular mortality in renal transplant recipients: A prospective cohort study. Nephrol. Dial. Transpl. 2020, 35, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnitzler, M.A.; Lentine, K.L.; Gheorghian, A.; Axelrod, D.; Trivedi, D.; L’Italien, G. Renal function following living, standard criteria deceased and expanded criteria deceased donor kidney transplantation: Impact on graft failure and death. Transpl. Int. 2012, 25, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Opelz, G.; Döhler, B. Influence of time of rejection on long-term graft survival in renal transplantation. Transplantation 2008, 85, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Gaston, R.S.; Fieberg, A.; Hunsicker, L.; Kasiske, B.L.; Leduc, R.; Cosio, F.G.; Gourishankar, S.; Grande, J.; Mannon, R.B.; Rush, D.; et al. Late graft failure after kidney transplantation as the consequence of late versus early events. Am. J. Transpl. 2018, 18, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Skeans, M.A. Patient outcomes in renal transplantation (port) investigators the relationship between kidney function and long-term graft survival after kidney transplant. Am. J. Kidney Dis. 2011, 57, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Rijkse, E.; Dam, J.L.; Roodnat, J.I.; Kimenai, H.J.A.N.; IJzermans, J.N.M.; Minnee, R.C. The prognosis of kidney transplant recipients with aorto-iliac calcification: A systematic review and meta-analysis. Transpl. Int. 2020, 33, 483–496. [Google Scholar] [CrossRef] [Green Version]
- Schachtner, T.; Otto, N.M.; Reinke, P. Two decades of the Eurotransplant Senior Program: The gender gap in mortality impacts patient survival after kidney transplantation. Clin. Kidney J. 2020, 13, 1091–1100. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Loupy, A.; Haas, M.; Solez, K.; Racusen, L.; Glotz, D.; Seron, D.; Nankivell, B.J.; Colvin, R.B.; Afrouzian, M.; Akalin, E.; et al. The banff 2015 kidney meeting report: Current challenges in rejection classification and prospects for adopting molecular pathology. Am. J. Transpl. 2017, 17, 28–41. [Google Scholar] [CrossRef]
- Clark, T.G.; Bradburn, M.J.; Love, S.B.; Altman, D.G. Survival analysis Part I: Basic concepts and first analyses. Br. J. Cancer 2003, 89, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Janes, H.; Dominici, F.; Zeger, S. On quantifying the magnitude of confounding. Biostatistics 2010, 11, 572–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijkse, E.; Kimenai, H.J.A.N.; Roodnat, J.I.; Ten Raa, S.; Bijdevaate, D.C.; van Dam, J.L.; Muller, K.; IJzermans, J.N.M.; van der Zijden, M.A.; Minnee, R.C. Impact of aortoiliac stenosis on graft and patient survival in kidney transplant recipients using the tasc ii classification. Transplantation 2019, 103, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Munguia, P.; Caramelo, R.; Rubio, M.V.; Sahdalá, L.; Arnaudas, L.; Paul, J.; Blasco, Á.; Lou, L.M.; Aladren, M.J.; Sanjuan, A.; et al. Pre-transplant assessment of vascular calcification as a risk factor of mortality, graft loss, and cardiovascular events in renal transplant recipients. Transpl. Proc. 2015, 47, 2368–2370. [Google Scholar] [CrossRef] [PubMed]
- Chavent, B.; Maillard, N.; Boutet, C.; Albertini, J.-N.; Duprey, A.; Favre, J.-P. Prognostic value of aortoiliac calcification score in kidney transplantation recipients. Ann. Vasc. Surg. 2017, 44, 245–252. [Google Scholar] [CrossRef]
- Aitken, E.; Ramjug, S.; Buist, L.; Kingsmore, D. The Prognostic Significance of Iliac Vessel Calcification in Renal Transplantation. In Transplantation Proceedings; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Hwang, H.S.; Lim, S.W.; Sun, I.O.; Yang, K.S.; Yoon, H.E.; Chung, B.H.; Choi, B.S.; Choi, Y.J.; Kim, J., II; Sung Moon, I.; et al. Clinical significance of preexisting microcalcification in the iliac artery in renal transplant recipients. Transplantation 2015, 99, 811–817. [Google Scholar] [CrossRef]
- Keyzer, C.A.; de Borst, M.H.; van den Berg, E.; Jahnen-Dechent, W.; Arampatzis, S.; Farese, S.; Bergmann, I.P.; Floege, J.; Navis, G.; Bakker, S.J.L.; et al. Calcification propensity and survival among renal transplant recipients. J. Am. Soc. Nephrol. 2016, 27, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Veroux, M.; Grosso, G.; Corona, D.; Mistretta, A.; Giaquinta, A.; Giuffrida, G.; Sinagra, N.; Veroux, P. Age is an important predictor of kidney transplantation outcome. Nephrol. Dial. Transpl. 2012, 27, 1663–1671. [Google Scholar] [CrossRef] [Green Version]
- Benjamens, S.; van den Berg, T.A.J.; Kuipers, T.G.J.; Moers, C.; Berger, S.P.; Leuvenink, H.G.D.; Pol, R.A. Kidney temperature during living donor kidney transplantation is associated with short-term measured glomerular filtration rate—A prospective study. Transpl. Int. 2020, 33, 174–180. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, S.; Srinivasa, S.; Callaghan, C.J.; Watson, C.J.; Dark, J.H.; Fisher, A.J.; Wilson, C.H.; Friend, P.J.; Johnson, R.; Forsythe, J.L.; et al. Novel organ perfusion and preservation strategies in transplantation—where are we going in the UK? Transplantation 2020, 104. [Google Scholar] [CrossRef]
- Gill, J.; Dong, J.; Eng, M.; Landsberg, D.; Gill, J.S. Pulsatile perfusion reduces the risk of delayed graft function in deceased donor kidney transplants, irrespective of donor type and cold ischemic time. Transplantation 2014, 97, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Peters-Sengers, H.; Houtzager, J.H.E.; Idu, M.M.; Heemskerk, M.B.A.; van Heurn, E.L.W.; van der Heide, J.J.H.; Kers, J.; Berger, S.P.; van Gulik, T.M.; Bemelman, F.J. Impact of cold ischemia time on outcomes of deceased donor kidney transplantation: An Analysis of a national registry. Transpl. Direct 2019, 5, e448. [Google Scholar] [CrossRef] [PubMed]
- Jardine, A.G.; Gaston, R.S.; Fellstrom, B.C.; Holdaas, H. Prevention of cardiovascular disease in adult recipients of kidney transplants. Lancet 2011, 378, 1419–1427. [Google Scholar] [CrossRef]
- Krenzien, F.; ElKhal, A.; Quante, M.; Cetina Biefer, H.R.; Hirofumi, U.; Gabardi, S.; Tullius, S.G. A rationale for age-adapted immunosuppression in organ transplantation. Transplantation 2015, 99, 2258–2268. [Google Scholar] [CrossRef] [Green Version]
- Sotomayor, C.G.; te Velde-Keyzer, C.A.; de Borst, M.H.; Navis, G.J.; Bakker, S.J.L. Lifestyle, inflammation, and vascular calcification in kidney transplant recipients: Perspectives on long-term outcomes. J. Clin. Med. 2020, 9, 1911. [Google Scholar] [CrossRef] [PubMed]
- Sotomayor, C.G.; Benjamens, S.; Gomes-Neto, A.W.; Pol, R.A.; Groothof, D.; te Velde-Keyzer, C.A.; Chong, G.; Glaudemans, A.W.J.M.; Berger, S.P.; Bakker, S.J.L.; et al. Bone Mineral Density and Aortic Calcification. Transplantation 2020, 105. [Google Scholar] [CrossRef]
- Peters-Sengers, H.; Berger, S.P.; Heemskerk, M.B.A.; Al Arashi, D.; van der Heide, J.J.H.; Hemke, A.C.; Ten Berge, I.J.M.; Idu, M.M.; Betjes, M.G.H.; van Zuilen, A.D.; et al. Stretching the limits of renal transplantation in elderly recipients of grafts from elderly deceased donors. J. Am. Soc. Nephrol. 2017, 28, 621–631. [Google Scholar] [CrossRef]
- Benjamens, S.; Glaudemans, A.W.J.M.; Berger, S.P.; Slart, R.H.J.A.; Pol, R.A. Have we forgotten imaging prior to and after kidney transplantation? Eur. Radiol. 2018, 28, 3263–3267. [Google Scholar] [CrossRef] [Green Version]
- Chadban, S.J.; Ahn, C.; Axelrod, D.A.; Foster, B.J.; Kasiske, B.L.; Kher, V.; Kumar, D.; Oberbauer, R.; Pascual, J.; Pilmore, H.L.; et al. Summary of the kidney disease: Improving global outcomes (KDIGO) clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation 2020, 104, 708–714. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 547) | Low CaScore (n = 365) | High CaScore (n = 182) | p-Value |
|---|---|---|---|---|
| Patient | ||||
| Male gender, n (%) a | 336 (61.4) | 205 (56.2) | 131 (72.0) | <0.001 b |
| Age, years c | 60 (51, 68) | 55 (47, 64) | 66 (60, 71) | <0.001 d |
| Diabetes mellitus, n (%) a | 173 (31.6) | 117 (32.1) | 56 (30.8) | 0.836 b |
| Body Mass Index, kg/m2 b | 26.8 (4.7) | 26.9 (4.9) | 26.7 (4.1) | 0.670 c |
| Smoker, n (%) a | 0.004 b | |||
| Non | 154 (28.2) | 119 (32.6) | 35 (19.2) | |
| Former | 332 (60.7) | 206 (56.4) | 126 (69.2) | |
| Current | 61 (11.2) | 40 (11.0) | 21 (11.5) | |
| Hypercholesterolemia, n (%) a | 153 (28.0) | 96 (26.3) | 57 (31.3) | 0.258 b |
| Total cholesterol, mmol/L | 4.7 (1.3) | 4.8 (1.5) | 4.5 (1.2) | 0.031 c |
| Systolic blood pressure, mmHg | 145 (22) | 143 (21) | 148 (24) | 0.014 c |
| Use of antihypertensive medication, n (%) | 439 (80.3) | 282 (77.3) | 157 (86.3) | 0.017 b |
| Type of dialysis, n (%) a | 0.109 b | |||
| Pre-emptive | 197 (36.0) | 142 (38.9) | 55 (30.2) | |
| Haemodialysis | 250 (45.7) | 162 (44.4) | 88 (48.4) | |
| Peritoneal dialysis | 100 (18.3) | 61 (16.7) | 39 (21.4) | |
| Dialysis vintage, months c | 12 (0, 28) | 11 (0, 25) | 16 (0, 33) | 0.012 d |
| Previous transplants, n (%) a | 0.872 b | |||
| Non | 514 (94.0) | 343 (94.0) | 171 (94.0) | |
| One | 22 (4.0) | 14 (3.8) | 8 (4.4) | |
| Two | 11 (2.0) | 8 (2.2) | 3 (1.6) | |
| Aorto-iliac CaScore, HU | 2994 (294, 7888) | 856 (46, 2994) | 9732 (7918, 14315) | <0.001 d |
| Transplantation | ||||
| Type of donation, n (%) a | 0.025 b | |||
| Living-donation | 301 (55.0) | 215 (58.9) | 86 (47.3) | |
| Donation after circulatory death | 128 (23.4) | 75 (20.5) | 53 (29.1) | |
| Donation after brain death | 118 (21.6) | 75 (20.5) | 43 (23.6) | |
| Male gender donor, n (%) | 253 (46.3) | 160 (43.8) | 93 (51.1) | 0.130 b |
| Donor age, years | 54 (14) | 52 (14) | 59 (12) | <0.001 c |
| No. of HLA-mismatches, n | 3.5 (1.5) | 3.4 (1.5) | 3.6 (1.4) | 0.127 c |
| Warm ischemia time, minutes | 42 (36) | 42 (44) | 41 (13) | 0.676 c |
| Cold ischemia time, minutes | 433 (340) | 415(343) | 470 (331) | 0.076 c |
| Follow-up e | ||||
| eGFR at six-months a | 50 (18) | 51 (19) | 46 (17) | 0.004 c |
| eGFR at one-year a | 51 (21) | 53 (20) | 48 (21) | 0.007 c |
| Haemoglobin at one-year, mmol/L | 8.3 (3.8) | 8.3 (4.6) | 8.2 (1.1) | 0.811 c |
| Calcium at one-year, mmol/L | 2.43 (0.14) | 2.43 (0.14) | 2.45 (0.14) | 0.034 c |
| Phosphate at one year, mmol/L | 0.93 (0.21) | 0.95 (0.21) | 0.89 (0.19) | 0.004 c |
| Albumin at one-year, g/L | 43 (3) | 43 (3) | 43 (3) | 0.234 c |
| Glucose at one-year, mmol/L | 5.9 (5.1, 7.3) | 5.7 (5.1, 7.2) | 6.2 (5.4, 7.6) | 0.005 d |
| PTH at one-year, pmol/L | 10 (7, 16) | 10 (7, 15) | 12 (8, 16) | 0.064 d |
| Protein excretion at one-year, g/24 h | 0.2 (0.1, 0.3) | 0.1 (0.1, 0.2) | 0.2 (0.1, 0.3) | 0.002 d |
| Cytomegalovirus infection, n (%) | 29 (5.3) | 17 (4.7) | 12 (6.6) | 0.453 b |
| Outcome Measures | Total (n = 547) | Low CaScore (n = 365) | High CaScore (n = 182) | p-Value |
|---|---|---|---|---|
| Median follow-up, years | 3.1 (1.4, 5.2) | 3.2 (1.5, 5.6) | 2.7 (1.2, 4.2) | |
| Short-term graft outcomes | ||||
| Early graft failure (death-censored) | 14 (2.6) | 5 (1.4) | 9 (4.9) | 0.027 |
| Delayed graft function | 155 (28.3) | 100 (27.4) | 55 (30.2) | 0.555 |
| Acute rejection (first-year) | 70 (12.8) | 47 (12.9) | 23 (12.6) | 1.000 |
| Long-term graft outcomes | ||||
| Death-censored graft failure | 64 (11.7) | 41 (11.2) | 23 (12.6) | 0.734 |
| Overall graft failure | 118 (21.6) | 64 (17.5) | 54 (29.7) | 0.002 |
| Death with a functioning graft | 54 (9.9) | 23 (6.3) | 31 (17.0) | <0.001 |
| Graft function decline | 81 (14.8) | 51 (14.0) | 30 (16.5) | 0.515 |
| One-Year eGFR | Standard β | 95% CI | p-Value |
|---|---|---|---|
| Univariate | −3.3 | −5.1 to −1.5 | <0.0001 |
| Model 1 | −3.5 | −5.3 to −1.7 | <0.0001 |
| Model 2 | −4.1 | −5.9 to −2.4 | <0.0001 |
| Model 3 | −2.7 | −4.6 to −0.7 | 0.008 |
| Model 4 | −1.7 | −3.6 to 0.2 | 0.077 |
| Outcomes Measures | Low CaScore | High CaScore | ||
|---|---|---|---|---|
| Hazard Ratio | Hazard Ratio | 95% CI | p-Value | |
| Death censored graft failure | ||||
| Univariate | 1.0 (Ref) | 1.5 | 0.9 to 2.5 | 0.125 |
| Model 1 | 1.0 (Ref) | 1.6 | 0.9 to 2.7 | 0.082 |
| Model 2 | 1.0 (Ref) | 1.4 | 0.8 to 2.4 | 0.211 |
| Model 3 | 1.0 (Ref) | 1.1 | 0.6 to 2.0 | 0.697 |
| Model 4 | 1.0 (Ref) | 1.1 | 0.6 to 2.0 | 0.711 |
| Overall graft failure | ||||
| Univariate | 1.0 (Ref) | 2.4 | 1.7 to 3.5 | <0.0001 |
| Model 1 | 1.0 (Ref) | 2.5 | 1.7 to 3.7 | <0.0001 |
| Model 2 | 1.0 (Ref) | 2.4 | 1.6 to 3.5 | <0.0001 |
| Model 3 | 1.0 (Ref) | 1.8 | 1.2 to 2.7 | 0.008 |
| Model 4 | 1.0 (Ref) | 1.9 | 1.2 to 2.9 | 0.006 |
| Death with a functioning graft | ||||
| Univariate | 1.0 (Ref) | 3.8 | 2.2 to 6.5 | <0.0001 |
| Model 1 | 1.0 (Ref) | 3.9 | 2.3 to 6.9 | <0.0001 |
| Model 2 | 1.0 (Ref) | 4.0 | 2.3 to 7.1 | <0.0001 |
| Model 3 | 1.0 (Ref) | 2.8 | 1.5 to 5.2 | 0.002 |
| Model 4 | 1.0 (Ref) | 2.7 | 1.4 to 5.0 | 0.004 |
| Graft function decline | ||||
| Univariate | 1.0 (Ref) | 1.6 | 1.0 to 2.6 | 0.038 |
| Model 1 | 1.0 (Ref) | 1.8 | 1.1 to 2.8 | 0.018 |
| Model 2 | 1.0 (Ref) | 1.6 | 1.0 to 2.6 | 0.043 |
| Model 3 | 1.0 (Ref) | 1.3 | 0.8 to 2.1 | 0.368 |
| Model 4 | 1.0 (Ref) | 1.4 | 0.8 to 2.4 | 0.223 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benjamens, S.; Alghamdi, S.Z.; Rijkse, E.; te Velde-Keyzer, C.A.; Berger, S.P.; Moers, C.; de Borst, M.H.; Slart, R.H.J.A.; Dor, F.J.M.F.; Minnee, R.C.; et al. Aorto-Iliac Artery Calcification and Graft Outcomes in Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 325. https://doi.org/10.3390/jcm10020325
Benjamens S, Alghamdi SZ, Rijkse E, te Velde-Keyzer CA, Berger SP, Moers C, de Borst MH, Slart RHJA, Dor FJMF, Minnee RC, et al. Aorto-Iliac Artery Calcification and Graft Outcomes in Kidney Transplant Recipients. Journal of Clinical Medicine. 2021; 10(2):325. https://doi.org/10.3390/jcm10020325
Chicago/Turabian StyleBenjamens, Stan, Saleh Z. Alghamdi, Elsaline Rijkse, Charlotte A. te Velde-Keyzer, Stefan P. Berger, Cyril Moers, Martin H. de Borst, Riemer H. J. A. Slart, Frank J. M. F. Dor, Robert C. Minnee, and et al. 2021. "Aorto-Iliac Artery Calcification and Graft Outcomes in Kidney Transplant Recipients" Journal of Clinical Medicine 10, no. 2: 325. https://doi.org/10.3390/jcm10020325
APA StyleBenjamens, S., Alghamdi, S. Z., Rijkse, E., te Velde-Keyzer, C. A., Berger, S. P., Moers, C., de Borst, M. H., Slart, R. H. J. A., Dor, F. J. M. F., Minnee, R. C., & Pol, R. A. (2021). Aorto-Iliac Artery Calcification and Graft Outcomes in Kidney Transplant Recipients. Journal of Clinical Medicine, 10(2), 325. https://doi.org/10.3390/jcm10020325