
Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
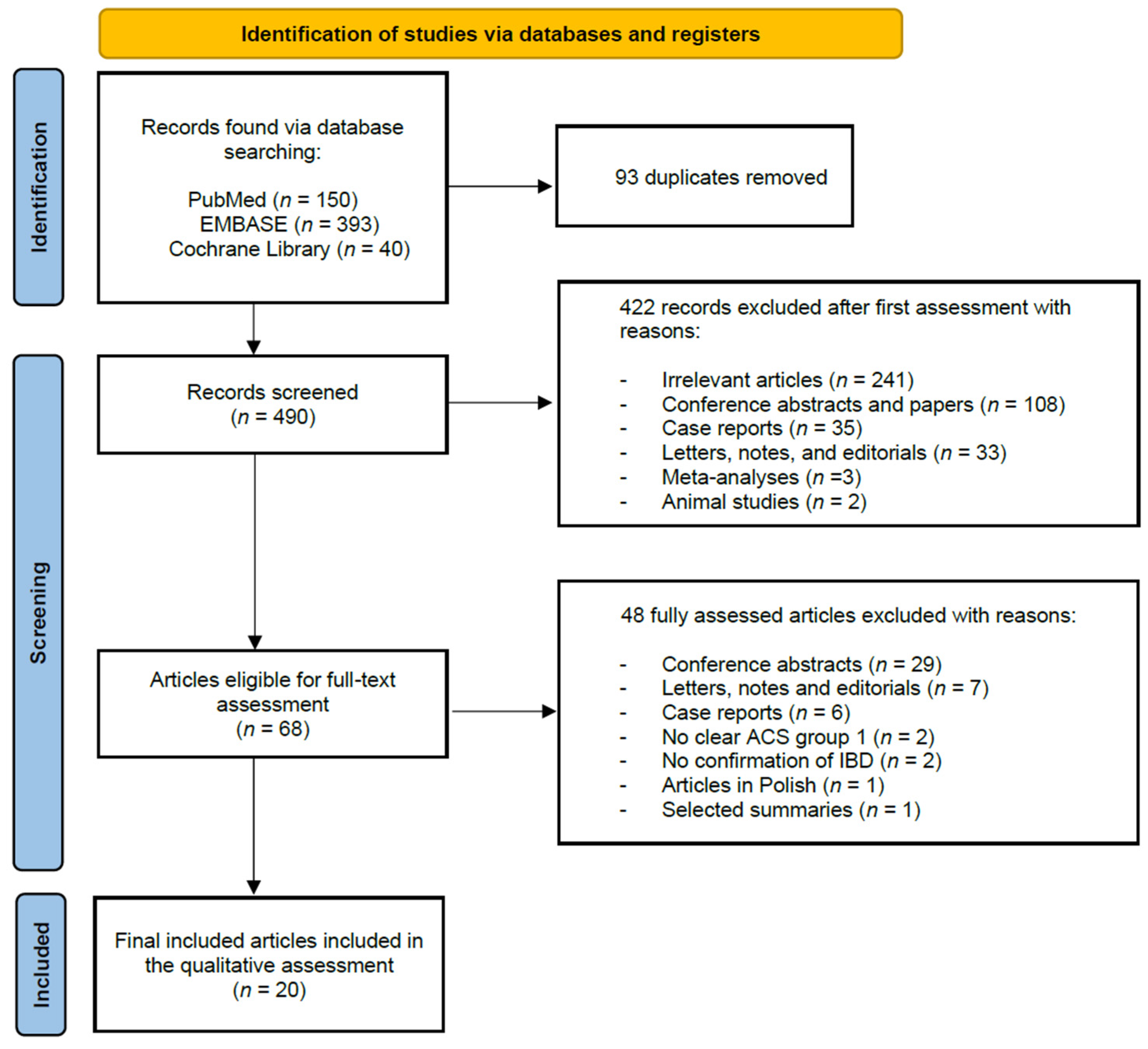
3.1. Literature Search
3.2. Study Characteristics

{kind=link}
| First Author/Year/ Country | Study Design | Study Characteristics | Main Findings |
|---|---|---|---|
| Mendelsohn et al./1995/USA [59] | Cross-sectional | • Total Subjects: 80 • Population: Crohn’s disease patients (deaths) • ACS patients: MI: 3 (12%) • ACS mortality: • IBD: Crohn’s disease: 25 (100%) • Mean age (years): - • Gender (males): 15 (60%) • IBD severity: • Treatment: operated (22 (88%) • Follow up: - | MI was associated with the death of three out of twenty-five patients with CD. Two patients who died from MI had hypertension possibly aggravated by multiple courses of steroid therapy. |
| Archimandritis et al./2002/Greece [60] | Cross-sectional | • Total Subjects: 172 • Population: IBD patients on follow-up • ACS patients: 4 (2.32%); UC: 2 (1.5%), CD: 2 (5%) • ACS mortality: 4 (100%) • IBD: 172 (100%); UC: 130 (67%); CD: 42 (42%) • Mean age (years): UC (men: 46.00 ± 16.24, women: 40.00 ± 16.76)/CD (men: 36.85 ± 13.0, women: 33.79 ± 16.9)) • Gender (males): 95 (55.8%); UC: 73 (56.1%); CD: 22 (52.3%) • IBD severity: - • Treatment: UC (conservative: 108 responded well vs. 22 did not respond well; surgical: 6); CD (known drug regimen and individualized: 42, required surgery: 12) • Follow up: UC: 25% of patients experienced a severe attack and 17% had their bowel involvement worsen | The mortality rate for UC was 5%, but only 1.5% could be directly connected with the disease; the rate was 5% in CD, unrelated to the disease. The only two men who died while having CD had an MI. |
| Ha et al./2009/USA [61] | Retrospective cohort analysis | • Total Subjects: 17,487 • Population: IBD patients (code: ICD-9CM) aged between 18–59 years, from the MarketScan Commercial claims and Encounters database • ACS patients: IBD: 148 (0.9%); UC: 83 (0.8%); CD: 65 (0.9%) • ACS mortality: - • IBD: 17,487 (100%); UC: 9968 (57%), CD: 7480 (42,77%) • Mean age (years): UC: 43.6, CD: 42.9; Control: 43.2 (18–59)44 • Gender (males): UC: 4455 (44.7%); CD: 3254 (43.5) • IBD severity: - • Treatment: - • Follow up: UC: 3.2 (0.5–5.7) years; CD: 3.3 (0.5–5.7) years | Only IBD women between 40–59 showed an elevated risk for MI, while for men over 40 there was no increase and a significant lower risk of atherosclerosis. A higher percentage of women used contraceptives vs. age-adjusted control group. |
| Pemmasani et al./2020/USA [73] | Retrospective cohort analysis | • Total Subjects: • Population: ACS patients • ACS patients: ACS: 6,896,635 (100%) • ACS mortality: IBD related comorbidities and complications associated with increased mortality • IBD: 24,200 (0.35%); CD: 12,846 (53%); UC: 11,374 (47%) • Mean age (years): No IBD: 67.2 ± 14.4; IBD: 66.9 ± 13.4 • Gender (males): 4,130,321 (60.1%) • IBD severity: - • Treatment: - • Follow up: - | ACS-related risk profiles and mortality were more favorable with IBD-ACS than with non-IBD ACS. Comorbidities and complications more frequently associated with IBD were strongly associated with mortality from ACS. Among IBD patients with ACS, comorbidities and complications that were potentially related to IBD were strong independent predictors of increased mortality. |
| Osterman et al./2011/USA [62] | Retrospective cohort analysis | • Total Subjects: 25,327 • Population: Patients with CD or UC older than 18 years old, no history of RA, SLE, psoriasis, MI, CAD, CHF, ventricular arrhythmia, cardiac defibrillator implantation before the start of the follow-up, pulled from the General Practice Research Database • ACS patients: IBD: 390 ; UC: 280 (1.8%) ; CD: 110 (1.1%) • ACS mortality: - • IBD: 100%, UC: 61.2% (15,498); CD: 38.8% (9829) • Mean age (years): UC: 50 vs. 49.1 from general population; CD: 44.2 vs. 43.3 from general population • Gender (males): UC: 48.4% (7501); CD: 41% (4030) • IBD severity: - • Treatment: - • Follow up: UC f/u: mean of 4.6 years; CD f/u: mean of 4.4 years | Patients with UC or CD do not appear to be at increased risk of MI. These results are contrary to those seen in other chronic inflammatory diseases, such as RA, SLE, and psoriasis. |
| Merril et al./2012/USA [63] | Retrospective cohort study | • Total Subjects: 271,368 • Population: Patients with inflammatory bowel disease (IBD) undergoing surgery • ACS patients: 9 (0.4%) PS: MI and CVA, study does not provide separate numbers • ACS mortality: - • IBD: 2249 (0.8%) • Mean age (years): IBD: 43; Non-IBD: 55.5 • Gender (males): 1122 (49.9%) • IBD severity: - • Treatment: - • Follow up: - | This analysis revealed no association between IBD and perioperative MI and stroke. |
| Kristensen et al./2013/Denmark [64] | Retrospective cohort study | • Total Subjects: 20,795 • Population: IBD cases ≥ 15 years old who received first diagnosis of IBD during 1996–2009 with dispensed IBD treatment prescription with no prior IBD or MI or stroke before that period • ACS patients: 365; UC: 272 (74.5%); CD: 61 (16.7%) unspecified IBD = 32 (8%) • ACS mortality: IBD: 778 (3.74%); UC: 540 (69.4%); CD: 148 (19%) 11% is unspecified IBD. Mentions cardiovascular death in IBD patients not ACS or MI explicitly • IBD: 100% UC: 13,622 (65.5%); CD: 4732 (22.8%) • Mean age (years): IBD: 43.8 years (SD: 18.7); Control: 43.1 (18.7SD) • Gender (males): 45.5% (9462) • IBD severity: - • Treatment: Anti-TNF and corticosteroids • Follow up: Mean f/u time is 6.04 years | IBD patients were found to have a significantly increased (two-fold) risk of MI, stroke, and cardiovascular mortality. This risk was predominantly present in periods of IBD flares and persistent activity, whereas the risk was insignificantly raised for MI and stroke and not increased for cardiovascular death during remission disease stages. |
| Aggarwal et al.//2014/USA [65] | Retrospective cohort study | • Total Subjects: 131 • Population: Patients with IBD who were diagnosed with CAD by cardiac catheterization between January 2004 and June 2010 • ACS patients: 31 (23.66%) • ACS mortality has a death parameter but associated with CAD not ACS specifically. • IBD: 131 (100%); UC: 77 (58.77%); CD: 54 (41.22%) • Mean age (years): 65.3 years (10.0SD); UC: 64.8 (10.8SD); CD: 66.1 (8.7 SD); non-IBD: 67.8 (11.0SD) years • Gender (males): 97 (74.04%); UC: 34 (63%); CD: 63 (81.8%) • IBD severity: - • Treatment: Amino-salicylates, immunomodulators (any use of 6-mercaptopurine, azathioprine, or methotrexate), corticosteroids (oral or intravenous steroidal agents), topical therapies (enemas or suppositories), or biologics (any use of infliximab, adalimumab, or certolizumab) • Follow up: Median follow-up was 12 months (post-PCI) | Patients with IBD are diagnosed with CAD at a younger age as compared with non-IBD patients, are less likely to be active smokers and have lower body mass index. There was no difference in post-PCI major adverse cardiovascular outcomes. |
| Kristensen et al./2014/Denmark [1] | Retrospective cohort study | • Total Subjects: 73,451 • Population: Patients aged ≥ 30 years old hospitalized for the first-time MI between 2002–2011 alive 30 days post-discharge • ACS patients: 100%. • ACS mortality: 270 all-cause death • IBD: 863 (1,17%); UC: 655 (75.9%); CD: 208 (24.1%) • Mean age (years): IBD: 68.5 (13.5SD); No-IBD: 68.4 (13.7) • Gender (males): 498 (57.7%) • IBD severity: - • Treatment: Corticosteroid, anti-TNF • Follow up: Mean follow-up for patients with IBD alive 30 days after their first-time MI is: 3.9 years | Patients with IBD have increased long-term risk of all-cause mortality and major adverse cardiovascular events after MI, and this risk is exclusively observed during active IBD, in particular in relation with flare-ups. |
| Tsai et al./2014/Taiwan [66] | Retrospective cohort study | • Total Subjects: 11,822 • Population: Patients with IBD symptoms • ACS patients: 434; UC: 162 (37.32%); CD: 272 (62.68%) • ACS mortality: - • IBD: 100% does not specify numbers by UC and CD • Mean age (years): control: 52.3 (19.2SD); IBD:52.8 (19.3SD) • Gender (males): 6428 (54.4%) • IBD severity: - • Treatment: - • Follow up: Mean follow-up periods = 6.37 (3.76SD) years | The patients with IBD in this study were more likely to exhibit traditional risk factors for ACS. Patients with IBD are at elevated risks of deaths from myocardial infarction, stroke, and cardiovascular disorders. Patients with IBD who, on average, required two or more hospitalization per year were nearly 20-fold more likely to have ACS than those who required one hospitalization per year. |
| Kuy et al./2014/USA [67] | Retrospective cross-sectional analysis | • Total Subjects: 461,415 • Population: Patients with IBD from 2000 to 2009 • ACS patients: 9197 (1.99%) • ACS mortality: - • IBD: 100% • Mean age (years): - • Gender (males): • IBD severity: - • Treatment: - • Follow up: | ATEs represent most clinically relevant thromboembolic complications associated with inpatient admissions of IBD patients. |
| Zakroysky et al./2015/USA [68] | Case-control study | • Total Subjects: 177 • Population: IBD patients with a first presentation of ACS • ACS patients: 59 (33.33%); STEMI (ST-ACS) = 25 (42%); NSTEMI (NST-ACS) = 25 (42%); Unstable-angina = 9 (15%) • ACS mortality: Two deaths from cardiac causes; Patients with inflammatory bowel disease with acute coronary syndrome had a significantly higher all-cause mortality than those without acute coronary syndrome (17% vs. 5%, OR 3.7; 95% CI, 1.3–11.0; P = 0.02) • IBD: 100%; UC: 99 (55.9%); CD: 78 (44.06%) • Mean age (years): ACS: 67 ± 10; No-ACS: 67 ± 10 • Gender (males): 132 (74.5%); ACS: 44 (75%); No-ACS: 88 (75%) • IBD severity: - • Treatment: Anti-inflammatory (Steroids); biological agent (Infliximab); immunomodifiers (azathioprine, 6-mercaptopurines, methotrexate) • Follow up: - | There is an association between steroid exposure and significantly reduced odds of acute coronary syndrome. However, the use of amino salicylates, immune modifiers, and biologic therapies did not affect acute coronary syndrome events. |
| Barnes et al./2016/USA [69] | Retrospective cross-sectional study | • Total Subjects: - • Population: Patients ≥ 18 years diagnosed with IBD between 2000–2011 • ACS patients: - • ACS mortality: - • IBD: 563,687 (0.71%); UC: 204,589 (36.3%); CD: 359,098 (63.7%) • Gender (males): IBD: 237,111 (42.1%); Without-IBD: 30,623,519 (39.2%) • IBD severity: - • Treatment: - • Follow up: - | Patients with IBD had 0.51-fold odds of diagnosis of acute MI compared with patients without IBD. Patients with UC were more likely to have a diagnosis of acute MI than patients with CD. Lower rates of acute MI were demonstrated in the IBD population when compared with the general population (nationwide database). |
| Ehrenpreis et al./2016/USA [70] | Case-control | • Total Subjects: 5349 • Population: patients with ICD-9 cm codes for primary diagnosis of acute myocardial infarction, pneumonia or congestive heart failure with a co-diagnosis of IBD, Crohn’s disease (CD) or ulcerative colitis (UC). 2005–2011 NIS Database • ACS patients: 2280 (42.62%); CD: 1164 (51.05%); UC: 1123 (48.95%) • ACS mortality: 94; CD: 47 (50%); UC: 47 (50%) • IBD: UC: 1985 (37.10%); CD: 3364 (62.89%) • Mean age (years): UC: 65.79 ± 17.96; CD: 61.32 ± 17.88 • Gender (males): IBD: 2328 (43.5%) UC: 997 (50.23% out of UC patients); CD: 1331 (39.57% out of CD patients) • IBD severity: - • Treatment: - • Follow up: - | IBD confers a survival benefit for patients hospitalized with AMI. |
| Aniwan et al./2018/USA [71] | Population-based cohort study | • Total Subjects: 736 • Population: Patients with IBD in Olmsted County, Minnesota from 1980 through 2010 • ACS patients: 75 (10.19%) • ACS mortality: - • IBD: 100%; CD: 339 (46.05%); UC: 397 (53.94%) • Mean age (years): - • Gender (males): IBD: 405 (55%); CD: 177 (52%); UC: 228 (57%) • IBD severity: Systemic corticosteroids and IBD-related intraabdominal surgery as markers of disease severity and not scores • Treatment: Systemic corticosteroids, biologics, intraabdominal surgery • Follow up: - | The relative risk of AMI was significantly increased in patients with Crohn’s disease and ulcerative colitis. The relative risk of AMI was increased among users of systemic corticosteroids. Patients with IBD are at increased risk of AMI and heart failure. |
| Le Gall et al./2018/France [22] | Case-control study | • Total Subjects: 3539 • Population: All patients, aged 18 or older with an occurrence of acute arterial event between 1996 and 2015 the MICISTA database. Only patients with a follow-up greater than one year and at least one visit per year in our IBD unit. • ACS patients: 22 (0.63%) • ACS mortality: - • IBD: 100% • Mean age (years): [nested case–control] median Cases: 41.9 (25.3–58.7) vs. Control: 43.3 (31.7–54.6) • Gender (males): [nested case–control] 18 (60% of 30 cases) • IBD severity: - • Treatment: Corticosteroids, 5 amino-salicylates, thiopurines, methotrexate, and anti–tumor necrosis factor agents [anti-TNFs] • Follow up: Follow-up greater than one year and at least one visit per year in our IBD unit | The median interval between IBD diagnosis and occurrence of acute arterial event was 15.4 years. Disease activity may have an independent impact on the risk of acute arterial events in patients with IBD. |
| Choi et al./2019/South Korea [7] | Cohort study | • Total Subjects: 37,477 • Population: Patients diagnosed with Crohn’s disease (CD) or ulcerative colitis (UC) between 2006 and 2009 • ACS patients: Total: 604 (1.6%); CD: 146 (1.36); UC: 440 (1.64) • ACS mortality: the table mentions death but not specifically mentions if the death was due to ACS • IBD: 100%; CD: 10,708 (28.57%); UC: 26,769 (71.43%) • Mean age (years): IBD: 40.4 ± 16.6; Control: 40.4 ± 16.6; CD: 32.5 ± 15.7; UC: 43.5 ± 15.9 • Gender (males): 21,293 (56.8%); CD: 6881 (64.3%); UC: 14,412 (53.8%) • IBD severity: - • Treatment: Surgery (related to IBD: bowel resection) • Follow up: Median follow-up durations of control and IBD groups were 8.4 ± 1.6 years | The risk of MI is higher in patients with CD than in the general population, and this trend is stronger in female patients and those aged <40 years. |
| Panhwar et al./2019/USA [2] | Retrospective cohort analysis | • Total Subjects: 29,090,220 • Population: adult patients (20 to 65 years) with a diagnosis of IBD—ulcerative colitis (UC) or Crohn’s disease (CD)—who had active records between August 2013 and August 2018 • ACS patients: IBD: 20,040 (6.9%) UC: 9086 (45.33%) vs. CD 10,954 (54.66%) • ACS mortality: - • IBD: 290,430 (0.99%); UC: 131,680 (0.45%); CD: 158,750 (0.55%) • Mean age (years): (UC or CD were less likely to be younger (20–65 years old) • Gender (males): IBD: 11,6967 (40.27%); UC: 53,549 (40.7%); CD: 63,373 (39.92%) • IBD severity: - • Treatment: - • Follow up: - | IBD is associated with significantly increased MI risk compared with non-IBD patients. The relative risk of MI was highest in younger patients and decreased with age. The prevalence of MI was higher in patients with UC and CD vs. non-IBD patients. Patients with CD had greater odds of MI compared with patients with UC (across all age groups). Male gender conferred higher risk of MI. |
| Card et al./2020/UK [72] | Retrospective cohort study | • Total Subjects: 31,175 • Population: IBD patients with no restriction on age, no history of CAD, TEE or malignancy before diagnosis and no other steroids indication from the CPRD database, between 1997 and 2017 • ACS patients: 532 (1.7%) • ACS mortality: mentions 469 cardiovascular deaths, not exactly as a result from MIs/ACS • IBD: 31,175 (100%); UC: 16,779 (53.82%); CD: 10,721 (34.38%); Indeterminate-IBD: 3538 (11.34%) • Mean age (years): IBD: 45.2 vs. 45.4 Controls; UC: 47.8; CD: 41.5 • Gender (males): IBD: 14,883 (47.8%) vs. Control: 73,863 (47.8%); UC: 8359 (50%); CD: 4887 (44.8%); • IBD severity: - • Treatment: - • Follow up: Follow-up time according to disease activity; 220,000 person years vs. 1,000,000 person years in controls. MIs had 1.85 per 1000 person years when hospitalized | Hospitalized IBD patients had a lower risk of vascular events than controls, being significant only for MIs. An increased hazard of MI in ambulatory patients when disease was active. The incidence ratios for MIs were significantly increased in acute and chronic activity of IBD within ambulatory but not hospitalized patients. |
| Gauravpal S. Gill et al./2020/USA [75] | Retrospective Cohort study | • Total Subjects: 3,917,894 • Population: Patients with IBD from MedStar Health electronic record system pool of patients • ACS patients: No-IBD: 1.8% (277); IBD: 2.0% (302) • ACS mortality: Non-IBD: 2.1% (324) ; IBD: 2.3% (352) ; UC: 2.6% (171) ; CD: 2.2% (207) • IBD: 0.39% (15,292), UC: 43% (6658), CD: 61% (9406) • Mean age (years): IBD: 50; Non-IBD: 51; UC: 53; CD: 49 • Gender (males): Non-IBD: 41% (6337) ; IBD: 42% (6377) ; UC: 43% (2868); CD: 41% (3835) • IBD severity: - • Treatment: - • Follow up: Median follow-up of 4.4 years | Among patients with IBD, incidence of acute coronary events did not show a statistically significant difference when compared to the matched cohort. |
3.3. Quality Assessment
3.4. Definition of IBD
3.5. IBD Potentially Increasing the Odds of ACS Occurrence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kristensen, S.L.; Ahlehoff, O.; Lindhardsen, J.; Erichsen, R.; Lamberts, M.; Khalid, U.; Nielsen, O.H.; Torp-Pedersen, C.; Gislason, G.H.; Hansen, P.R. Prognosis after first-time myocardial infarction in patients with inflammatory bowel disease according to disease activity: Nationwide cohort study. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 857–862. [Google Scholar] [CrossRef] [Green Version]
- Panhwar, M.S.; Mansoor, E.; Al-Kindi, S.G.; Sinh, P.; Katz, J.; Oliveira, G.H.; Cooper, G.S.; Ginwalla, M. Risk of Myocardial Infarction in Inflammatory Bowel Disease: A Population-based National Study. Inflamm. Bowel Dis. 2019, 25, 1080–1087. [Google Scholar] [CrossRef]
- Ng, S.C.; Tang, W.; Ching, J.Y.; Wong, M.; Chow, C.M.; Hui, A.J.; Wong, T.C.; Leung, V.K.; Tsang, S.W.; Yu, H.H.; et al. Incidence and Phenotype of Inflammatory Bowel Disease Based on Results from the Asia-Pacific Crohn’s and Colitis Epidemiology Study. Gastroenterology 2013, 145, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N. Environmental Risk Factors for Inflammatory Bowel Diseases: A Review. Dig. Dis. Sci. 2015, 60, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G. The global burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Cosnes, J.; Gower-Rousseau, C.; Seksik, P.; Cortot, A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011, 140, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Lee, D.H.; Shin, D.W.; Han, K.D.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, N. Patients with inflammatory bowel disease have an increased risk of myocardial infarction: A nationwide study. Aliment. Pharmacol. Ther. 2019, 50, 769–779. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 21 February 2021).
- Olén, O.; Askling, J.; Sachs, M.C.; Neovius, M.; Smedby, K.E.; Ekbom, A.; Ludvigsson, J.F. Mortality in adult-onset and elderly-onset IBD: A nationwide register-based cohort study 1964–2014. Gut 2020, 69, 453–461. [Google Scholar] [CrossRef]
- Fernández-Gutiérrez, B.; Perrotti, P.P.; Gisbert, J.P.; Domènech, E.; Fernández-Nebro, A.; Cañete, J.D.; Ferrándiz, C.; Tornero, J.; García-Sánchez, V.; Panés, J.; et al. Cardiovascular disease in immune-mediated inflammatory diseases: A cross-sectional analysis of 6 cohorts. Medicine 2017, 96, e7308. [Google Scholar] [CrossRef]
- Fedorov, G.I.; Tsvineva, E.V. Extensive ulcerous-necrotic lesions of the digestive tract in myocardial infarct. Klin. Med. 1967, 45, 117–119. [Google Scholar]
- Baty, V.; Blain, H.; Saadi, L.; Jeandel, C.; Canton, P. Fatal myocardial infarction in an elderly woman with severe ulcerative colitis: What is the role of steroids? Am. J. Gastroenterol. 1998, 93, 2000–2001. [Google Scholar] [CrossRef] [PubMed]
- Efremidis, M.; Prappa, E.; Kardaras, F. Acute myocardial infarction in a young patient during an exacerbation of ulcerative colitis. Int. J. Cardiol. 1999, 70, 211–212. [Google Scholar] [CrossRef]
- Petitpain, N.; Bornert-Keller, N.; Peyrin-Biroulet, L. Acute coronary syndrome in a Crohn’s disease patient treated with adalimumab. J. Crohn’s Colitis 2013, 7, e396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şenol, A.; Işler, M.; Özaydin, M.; Türker, Y.; Songür, Y.; Koçkar, C. Acute myocardial infarction complicated by sudden cardiac arrest in a patient with ulcerative colitis. Turk. J. Gastroenterol. 2010, 21, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Theocharidou, E.; Gossios, T.D.; Karagiannis, A. Acute Coronary Syndrome in Patients with Inflammatory Bowel Diseases: The Plaque and the Thrombus. Angiology 2017, 68, 843–844. [Google Scholar] [CrossRef]
- Wei, B.; Wang, J.; Zhang, Y.; Zhao, J. Letter: Inflammatory bowel disease and risk of myocardial infarction. Aliment. Pharmacol. Ther. 2020, 51, 671–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazici, H.U.; Birdane, A.; Nadiradze, A.; Ünalir, A. Late bare-metal stent thrombosis in a patient with Crohn’s disease. Anatol. J. Cardiol. 2011, 11, 461–464. [Google Scholar] [CrossRef] [Green Version]
- Christou, A.; Patsilinakos, S.; Chinofoti, I.; Marinakos, A.; Nikolaou, N.; Spanodimos, S. Acute myocardial infarction in a patient with coronary artery aneurysm and Crohn’s Disease. Hell. J. Cardiol. 2012, 53, 400–402. [Google Scholar]
- Le Gall, G.; Kirchgesner, J.; Bejaoui, M.; Landman, C.; Nion-Larmurier, I.; Bourrier, A.; Sokol, H.; Seksik, P.; Beaugerie, L. Clinical activity is an independent risk factor of ischemic heart and cerebrovascular arterial disease in patients with inflammatory bowel disease. PLoS ONE 2018, 13, e0201991. [Google Scholar] [CrossRef] [Green Version]
- Mutlu, B.; Ermeydan, C.M.H.; Enç, F.; Fotbolcu, H.; Demirkol, O.; Bayrak, F.; Basaran, Y. Acute myocardial infarction in a young woman with severe ulcerative colitis. Int. J. Cardiol. 2002, 83, 183–185. [Google Scholar] [CrossRef]
- Navarro, B.; Blázquez, T.; Herreras, J.; Iborra, M. Acute myocardial infarction in a patient with a recent diagnosis of Crohn’s disease. Gastroenterol. Hepatol. 2019, 42, 183–184. [Google Scholar] [CrossRef] [PubMed]
- Tsigkas, G.; Davlouros, P.; Despotopoulos, S.; Assimakopoulos, S.F.; Theocharis, G.; Hahalis, G. Inflammatory Bowel Disease: A Potential Risk Factor for Coronary Artery Disease. Angiology 2017, 68, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hao, X.; Zheng, X.; Zhao, H.; Zhang, W.; Zhang, L. Acute myocardial infarction in a young woman with ulcerative colitis: A case report and literature review. Medicine 2017, 96, e8885. [Google Scholar] [CrossRef]
- Cinemre, H.; Bilir, C.; Gokosmanoglu, F.; Kadakal, F. Anti-Saccharomyces cerevisiae antibodies in acute myocardial infarction. J. Investig. Med. 2007, 55, 444–449. [Google Scholar] [CrossRef]
- El Mokhtari, N.E.; Ott, S.J.; Nebel, A.; Schäfer, A.; Rosenstiel, P.; Förster, M.; Nothnagel, M.; Simon, R.; Schreiber, S. Role of NOD2/CARD15 in coronary heart disease. BMC Genet. 2007, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Ajose, T.; Atem, N.N.; Effoe, V.S. Cardiovascular outcomes in patients with coexisting coronary artery disease and inflammatory bowel disease. Circulation 2019, 140, A11770. [Google Scholar] [CrossRef]
- Aggarwal, A.; Atreja, A.; Kapadia, S.; Achkar, J.P. Coronary artery disease in inflammatory bowel disease: A look at the percutaneous coronary intervention outcomes. Gastroenterology 2012, 142, S267. [Google Scholar] [CrossRef]
- Al-Abboodi, Y.; Kubaissy, A.; Ali, A.M. Do people with history of inflammatory disease have a higher risk for acute coronary syndrome. Am. J. Gastroenterol. 2019, 114, S12. [Google Scholar] [CrossRef]
- Al-Salameh, N.; DeCoskey, D.; Fernandez, A.G.; Green, S. A rare case of acute coronary syndrome in a young female. Chest 2020, 158, A202. [Google Scholar] [CrossRef]
- Barnes, E.L.; Marchioni Beery, R.M.; Schulman, A.; McCarthy, E.P.; Korzenik, J.R.; Winter, R.W. Myocardial infarction among patients with inflammatory bowel disease: A nationwide analysis. Gastroenterology 2016, 150, S388–S389. [Google Scholar] [CrossRef]
- Chadha, S.; Lodha, A.; Shetty, V.; Sadiq, A.; Hollander, G.; Shani, J. A rare complication of ulcerative colitis: ST elevation myocardial infarction. Am. J. Gastroenterol. 2012, 107, S498. [Google Scholar] [CrossRef]
- Dave, M.; Mehta, K.; Badheka, A.; Loftus, E. Inflammatory bowel disease does not impact mortality, but increases length of hospitalization in patients with acute myocardial infarction. Am. J. Gastroenterol. 2013, 108, S523–S524. [Google Scholar] [CrossRef]
- Garcia Gordo, P.O.; Martinez Toro, J.; Martinez Ojeda, J.; Figueroa Navarro, R. Acute myocardial infarction in a young female bodybuilder with ulcerative colitis and chronic anabolic steroid use. J. Investig. Med. 2013, 61, 381. [Google Scholar] [CrossRef]
- Garza, H.H.; Truong, T.; Patel, R.; Thai, H. Arterial embolism causing myocardial infarction in a patient with ulcerative colitis. J. Am. Coll. Cardiol. 2015, 65, A686. [Google Scholar] [CrossRef] [Green Version]
- Gill, G.; Fernandez, S.; Soud, M.; Mete, M.; Malhotra, N.; Garcia-Garcia, H.M. Major acute cardiovascular events in patients with inflammatory bowel disease. Eur. Heart J. 2019, 40, ehz746.0987. [Google Scholar] [CrossRef]
- Gorgis, S.; Dhillon, D.; Mishra, K.; Saleh, A.; Basir, M.; Fuller, B. Aggressive acute coronary thrombosis in ulcerative colitis flare. J. Am. Coll. Cardiol. 2020, 75, 3302. [Google Scholar] [CrossRef]
- Ha, C.; Choi, J.; Katz, S.; Kosutic, G.; Spearman, M.; Coarse, J.; Hasan, I.; Loftus, E.V., Jr. Comparison of cardiovascular events in elderly and younger Crohn’s disease patients treated with certolizumab pegol: Results from a pooled safety analysis. Am. J. Gastroenterol. 2015, 110, S778–S779. [Google Scholar] [CrossRef]
- Inamdar, S.; Altafi, S.; Sultan, K. Increased risk of coronary artery disease among patients with inflammatory bowel disease. Gastroenterology 2012, 142, S792–S793. [Google Scholar] [CrossRef]
- Jemilat, B.; Elie, A.K.; Berkeley, L.; Wendy, P.; Susan, H. Cardiovascular morbidity in hospitalized patients with inflammatory bowel disease compared to patients without inflammatory bowel disease and other autoimmune diseases. Inflamm. Bowel Dis. 2014, 20, S41. [Google Scholar] [CrossRef] [Green Version]
- Kasarala, G.; Sheri, G.; Harvin, G. Coronary artery disease and inflammatory bowel disease. Am. J. Gastroenterol. 2017, 112, S352. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Hansen, P.R.; Ahlehoff, O.; Lindhardsen, J.; Horvath-Puho, E.; Erichsen, R.; Torp-Pedersen, C.; Nielsen, O.H.; Gislason, G.H.; Sorensen, H.T. Increased risk of myocardial infarction and stroke in patients with inflammatory bowel disease—A nationwide cohort study. Eur. Heart J. 2012, 33, 239. [Google Scholar] [CrossRef]
- Levy, A.N.; Anderson, J.M.; Horton, H.; Sun, E.; Vasiliauskas, E.A.; Dubinsky, M.; Fleshner, P.; Shih, D.Q.; Kaur, M.; Ippoliti, A.; et al. Thromboembolic risk in hospitalized IBD patients is compounded by traditional risk factors and hypercoagulable states. Gastroenterology 2013, 144, S615. [Google Scholar] [CrossRef]
- Moradi, D.; John, E.S.; Das, K.; Seril, D. A case of non-ST elevation myocardial infarction in a young ulcerative colitis patient on adalimumab therapy. Am. J. Gastroenterol. 2017, 112, S1092. [Google Scholar] [CrossRef]
- Naymagon, S.; Ullman, T.; Cohen, B. Management of severe ulcerative colitis in the setting of acute myocardial infarction. Am. J. Gastroenterol. 2013, 108, S422. [Google Scholar] [CrossRef]
- Osterman, M.T.; Yang, Y.X.; Brensinger, C.M.; Lichtenstein, G.; Lewis, J.D. Risk of myocardial infarction in ulcerative colitis and Crohn’s disease. Gastroenterology 2010, 138, S198. [Google Scholar] [CrossRef]
- Panhwar, M.S.; Mansoor, E.; Al-Kindi, S.; Cooper, G.; Ginwalla, M. Risk of myocardial infarction in patients with inflammatory bowel disease. J. Am. Coll. Cardiol. 2018, 71, A183. [Google Scholar] [CrossRef]
- Ruisi, P.; Makaryus, J.N.; Ruisi, M.; Hakimian, J.; Makaryus, A.N. Inflammatory bowel disease as a precursor to premature cardiac events. J. Am. Coll. Cardiol. 2011, 57, E917. [Google Scholar] [CrossRef]
- Shah, P.; Shamah, S.; Chadha, S.; Rhamdaney, S.; Mayer, I.; Rahmani, R. Ulcerative colitis exacerbation in a young patient causing acute myocardial infarction: A case report. Am. J. Gastroenterol. 2013, 108, S421–S422. [Google Scholar] [CrossRef]
- Shaheen, A.; Ma, C.; Panaccione, R.; Seow, C.; Novak, K.; Ghosh, S.; Stapleton, M.; Kaplan, G. Inflammatory bowel diseases patients are at lower risk of acute coronary syndrome. Can. J. Gastroenterol. Hepatol. 2016, 2016, 4792898. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.W.; Kim, H.S.; Oh, D.J.; Lee, D.H. Crohn’s Disease is Associated with Increased Risk of Myocardial Infarction and Cardiovascular Death: A Nationwide Population-Based Cohort Study in Korea. Gastroenterology 2018, 154, S408–S409. [Google Scholar] [CrossRef]
- Singh, S.; Singh, H.; Loftus, E.; Pardi, D. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: A systematic review and meta-analysis. Am. J. Gastroenterol. 2013, 108, S513–S514. [Google Scholar] [CrossRef]
- Verdon, C.; Reinglas, J.; Filliter, C.; Gonczi, L.; Afif, W.; Wild, G.; Seidman, E.G.; Bitton, A.; Bessissow, T.; Brassard, P.; et al. Increased Prevalence but Not Incidence of Myocardial Infarction and Stroke in Patients with Inflammatory Bowel Diseases in Quebec in 1996–2015: Disease Severity Defined as Exposure to Biologicals Was Identified as Risk Factor for Myocardial Infarction. Gastroenterology 2020, 158, S940. [Google Scholar] [CrossRef]
- Weber, A.; Sauk, J.; Limketkai, B. Leading Causes of Mortality in Inflammatory Bowel Disease: A Nationwide Analysis. Gastroenterology 2020, 158, S41–S42. [Google Scholar] [CrossRef]
- Zakroysky, P.; Basnet, S.; Thai, W.E.; Onandia, Z.G.; Gandhi, S.; Truong, Q. Dramatic reduction in acute coronary syndrome with steroid exposure in patients with inflammatory bowel disease. J. Am. Coll. Cardiol. 2013, 61, E180. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.; Singal, A.G.; Sussman, J.; Waljee, A.K. At the “heart” of inflammatory bowel diseases. Gastroenterology 2013, 145, 1486–1488. [Google Scholar] [CrossRef]
- Mendelsohn, R.R.; Korelitz, B.I.; Gleim, G.W. Death from Crohn’s disease: Lessons from a personal experience. J. Clin. Gastroenterol. 1995, 20, 22–26. [Google Scholar] [CrossRef]
- Archimandritis, A.J.; Kourtesas, D.; Sougioultziz, S.; Giontzis, A.; Grigoriadis, P.; Davaris, P.; Tzivras, M. Inflammatory bowel disease in Greece—A hospital-based clinical study of 172 consecutive patients. Med. Sci. Monit. 2002, 8, Cr158–Cr164. [Google Scholar] [PubMed]
- Ha, C.; Magowan, S.; Accortt, N.A.; Chen, J.; Stone, C.D. Risk of arterial thrombotic events in inflammatory bowel disease. Am. J. Gastroenterol. 2009, 104, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Osterman, M.T.; Yang, Y.X.; Brensinger, C.; Forde, K.A.; Lichtenstein, G.R.; Lewis, J.D. No increased risk of myocardial infarction among patients with ulcerative colitis or Crohn’s disease. Clin. Gastroenterol. Hepatol. 2011, 9, 875–880. [Google Scholar] [CrossRef] [Green Version]
- Merrill, A.; Millham, F. Increased risk of postoperative deep vein thrombosis and pulmonary embolism in patients with inflammatory bowel disease: A study of National Surgical Quality Improvement Program patients. Arch. Surg. 2012, 147, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristensen, S.L.; Ahlehoff, O.; Lindhardsen, J.; Erichsen, R.; Jensen, G.V.; Torp-Pedersen, C.; Nielsen, O.H.; Gislason, G.H.; Hansen, P.R. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death—A Danish nationwide cohort study. PLoS ONE 2013, 8, e56944. [Google Scholar] [CrossRef]
- Aggarwal, A.; Atreja, A.; Kapadia, S.; Lopez, R.; Achkar, J.P. Conventional risk factors and cardiovascular outcomes of patients with inflammatory bowel disease with confirmed coronary artery disease. Inflamm. Bowel Dis. 2014, 20, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.S.; Lin, C.L.; Chen, H.P.; Lee, P.H.; Sung, F.C.; Kao, C.H. Long-term risk of acute coronary syndrome in patients with inflammatory bowel disease: A 13-year nationwide cohort study in an Asian population. Inflamm. Bowel Dis. 2014, 20, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Kuy, S.; Dua, A.; Chappidi, R.; Seabrook, G.; Brown, K.R.; Lewis, B.; Rossi, P.J.; Lee, C.J. The increasing incidence of thromboembolic events among hospitalized patients with inflammatory bowel disease. Vascular 2015, 23, 260–264. [Google Scholar] [CrossRef]
- Zakroysky, P.; Thai, W.E.; Deaño, R.C.; Basnet, S.; Onandia, Z.G.; Gandhi, S.; Tawakol, A.; Min, J.K.; Truong, Q.A. Steroid exposure, acute coronary syndrome, and inflammatory bowel disease: Insights into the inflammatory milieu. Am. J. Med. 2015, 128, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Barnes, E.L.; Beery, R.M.; Schulman, A.R.; McCarthy, E.P.; Korzenik, J.R.; Winter, R.W. Hospitalizations for Acute Myocardial Infarction Are Decreased among Patients with Inflammatory Bowel Disease Using a Nationwide Inpatient Database. Inflamm. Bowel Dis. 2016, 22, 2229–2237. [Google Scholar] [CrossRef] [Green Version]
- Ehrenpreis, E.D.; Zhou, Y.; Alexoff, A.; Melitas, C. Effect of the diagnosis of inflammatory bowel disease on risk-adjusted mortality in hospitalized patients with acute myocardial infarction, congestive heart failure and pneumonia. PLoS ONE 2016, 11, e0158926. [Google Scholar] [CrossRef]
- Aniwan, S.; Pardi, D.S.; Tremaine, W.J.; Loftus, E.V. Increased Risk of Acute Myocardial Infarction and Heart Failure in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1607–1615.e1. [Google Scholar] [CrossRef] [Green Version]
- Card, T.R.; Zittan, E.; Nguyen, G.C.; Grainge, M.J. Disease Activity in Inflammatory Bowel Disease Is Associated with Arterial Vascular Disease. Inflamm. Bowel Dis. 2021, 27, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Pemmasani, G.; Elgendy, I.; Mamas, M.A.; Leighton, J.A.; Aronow, W.S.; Tremaine, W.J. Epidemiology and Clinical Outcomes of Patients with Inflammatory Bowel Disease Presenting with Acute Coronary Syndrome. Inflamm. Bowel Dis. 2021, 27, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Roe, A.; Bartz, D.A.; Douglas, P.S. Combined Estrogen-Progestin Contraception: Side Effects and Health Concerns. Available online: https://www.uptodate.com/contents/combined-estrogen-progestin-contraception-side-effects-and-health-concerns#H360636587 (accessed on 21 February 2021).
- Gill, G.S.; Fernandez, S.J.; Malhotra, N.; Mete, M.; Garcia-Garcia, H.M. Major acute cardiovascular events in patients with inflammatory bowel disease. Coron. Artery Dis. 2021, 32, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Zanoli, L.; Briet, M.; Empana, J.P.; Cunha, P.G.; Maki-Petaja, K.M.; Protogerou, A.D.; Tedgui, A.; Touyz, R.M.; Schiffrin, E.L.; Spronck, B.; et al. Vascular consequences of inflammation: A position statement from the ESH Working Group on Vascular Structure and Function and the ARTERY Society. J. Hypertens. 2020, 38, 1682–1698. [Google Scholar] [CrossRef]
- Hernandez-Camba, A.; Carrillo-Palau, M.; Ramos, L.; Hernandez Alvarez-Buylla, N.; Alonso-Abreu, I.; Hernandez-Perez, A.; Vela, M.; Arranz, L.; Hernandez-Guerra, M.; Gonzalez-Gay, M.A.; et al. Carotid Plaque Assessment Reclassifies Patients with Inflammatory Bowel Disease into Very-High Cardiovascular Risk. J. Clin. Med. 2021, 10, 1671. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaaouani, A.; Ismaiel, A.; Popa, S.-L.; Dumitrascu, D.L. Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection. J. Clin. Med. 2021, 10, 4710. https://doi.org/10.3390/jcm10204710
Jaaouani A, Ismaiel A, Popa S-L, Dumitrascu DL. Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection. Journal of Clinical Medicine. 2021; 10(20):4710. https://doi.org/10.3390/jcm10204710
Chicago/Turabian StyleJaaouani, Ayman, Abdulrahman Ismaiel, Stefan-Lucian Popa, and Dan L. Dumitrascu. 2021. "Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection" Journal of Clinical Medicine 10, no. 20: 4710. https://doi.org/10.3390/jcm10204710
APA StyleJaaouani, A., Ismaiel, A., Popa, S. -L., & Dumitrascu, D. L. (2021). Acute Coronary Syndromes and Inflammatory Bowel Disease: The Gut–Heart Connection. Journal of Clinical Medicine, 10(20), 4710. https://doi.org/10.3390/jcm10204710