
COVID-19 Pandemic and Patients with Rare Inherited Metabolic Disorders and Rare Autoinflammatory Diseases—Organizational Challenges from the Point of View of Healthcare Providers

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
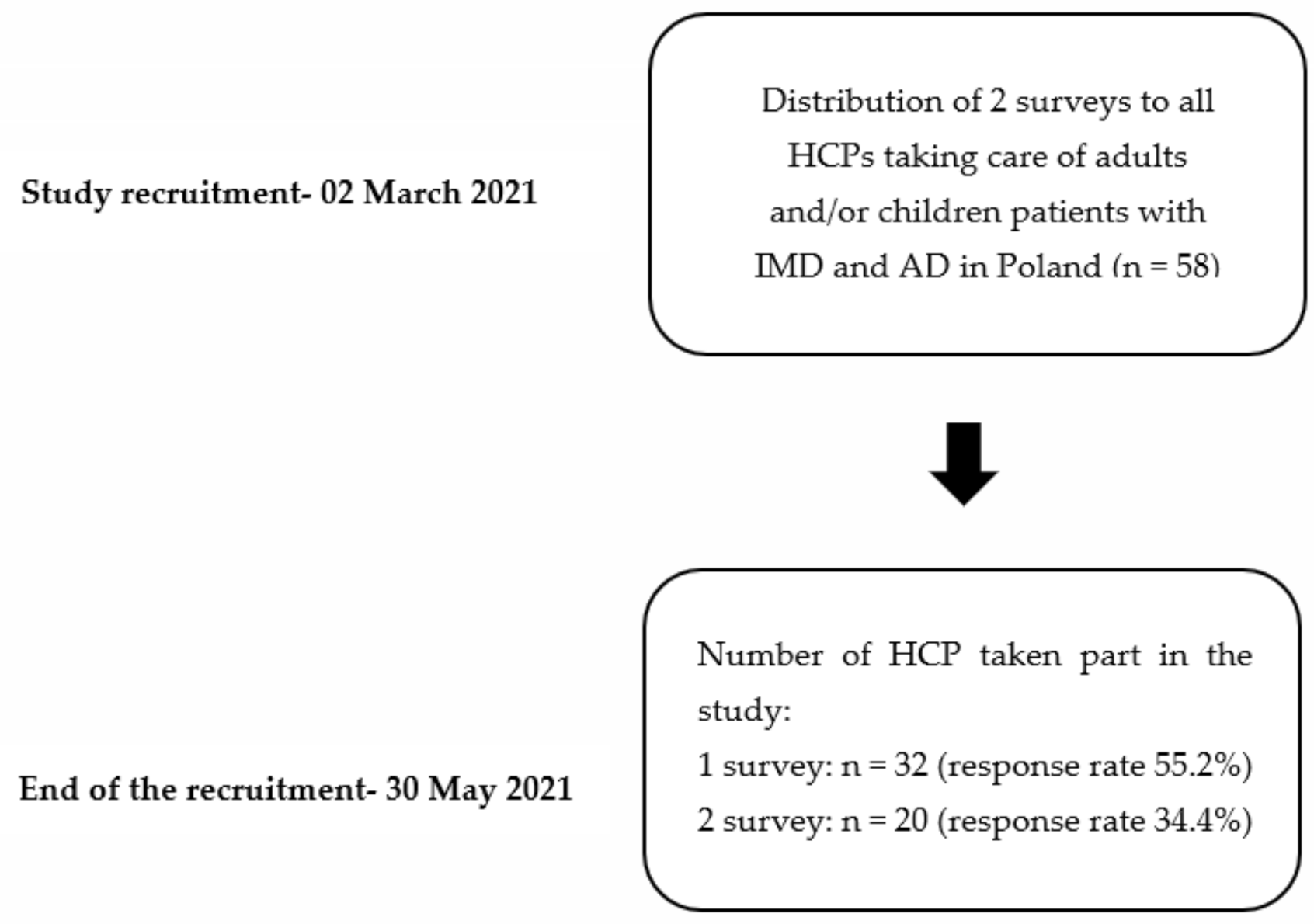
2. Materials and Methods
3. Results
3.1. General Information
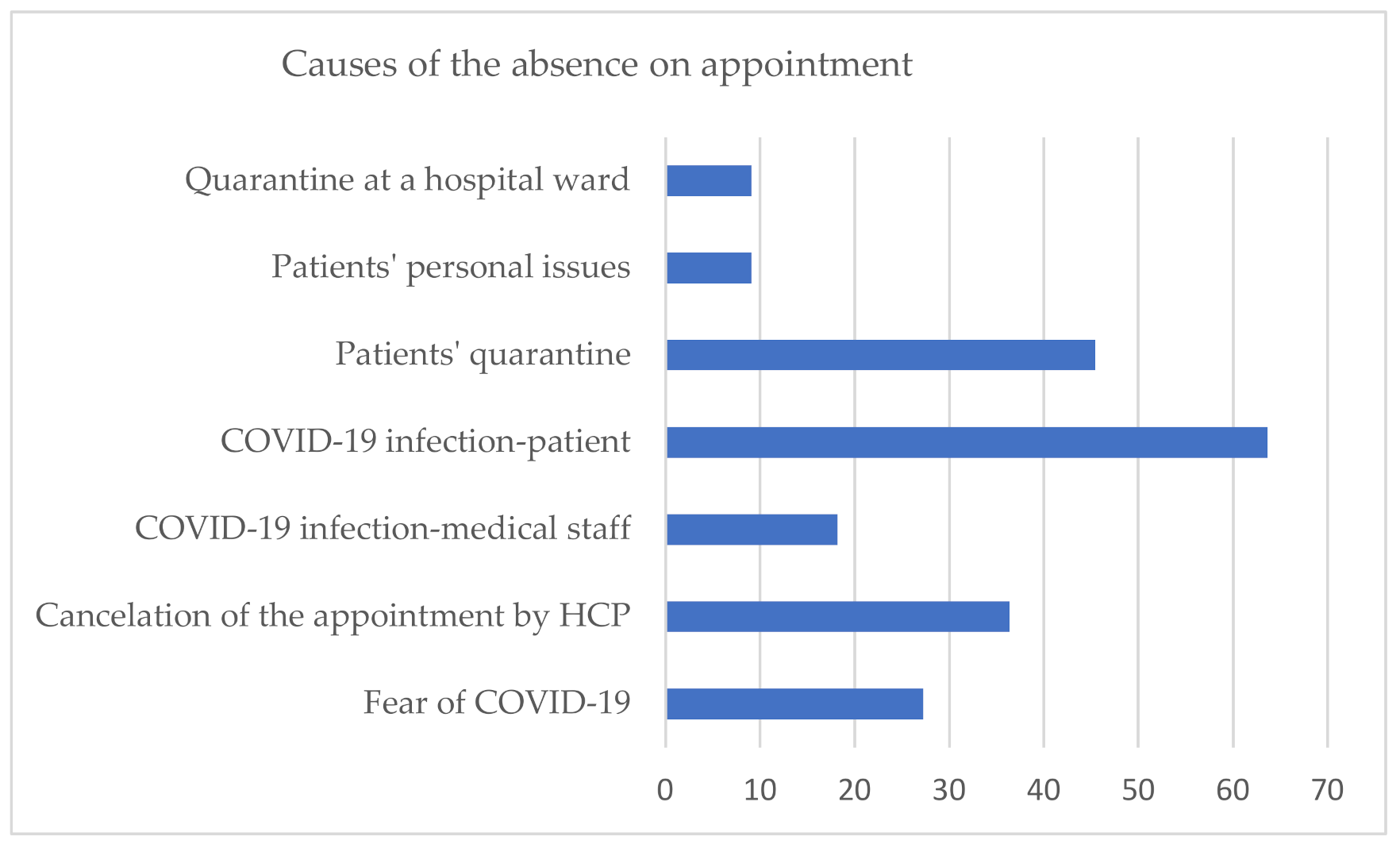
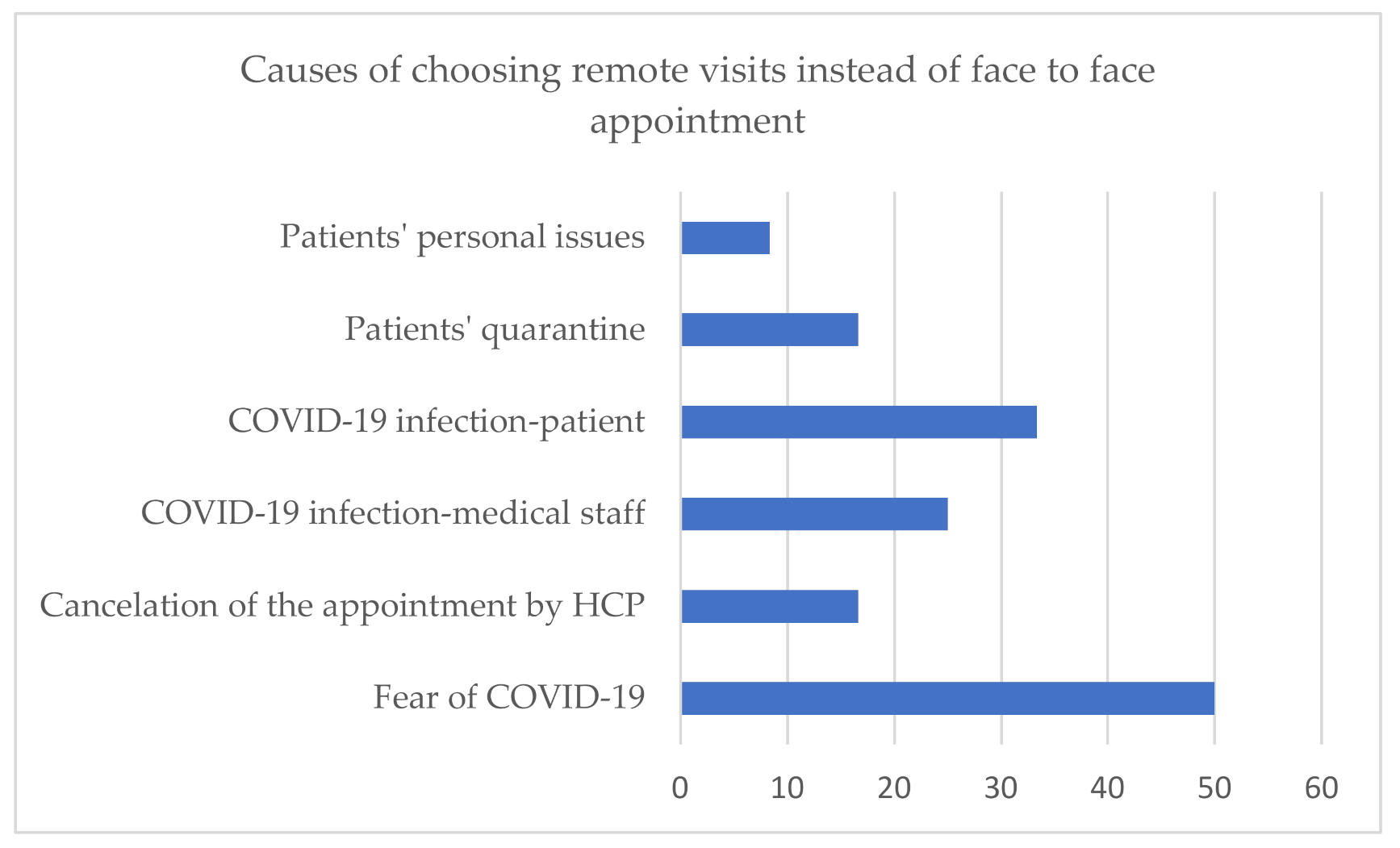
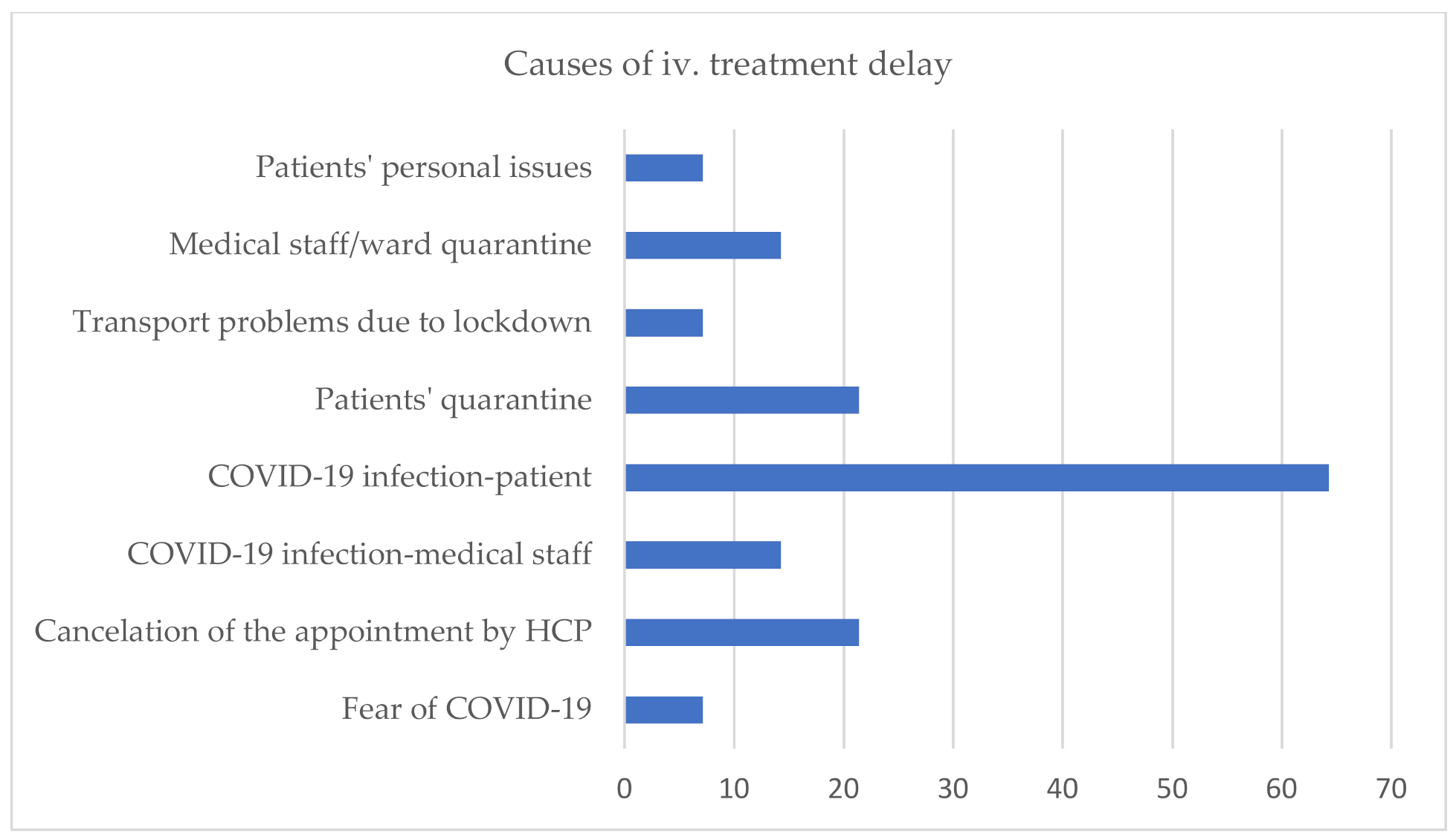
3.2. Health Care Units’ Functioning during the Pandemic
3.3. Pandemic Impact on the Diagnosis of New Cases/Routine Admissions to Hospital
3.4. Patients and SARS-COV-2 Infection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IMD | rare inherited metabolic disorders |
| AD | rare autoinflammatory diseases |
| HCP | health care providers |
| GD | Gaucher disease |
| MPS | mucopolysaccharidosis |
| ERT | enzyme replacement therapy |
| NPC | Niemann Pick disease type C |
| NPB | Niemann Pick disease type B |
| VLCADD | Very long-chain acyl-CoA dehydrogenase deficiency |
| FCAS | Familial cold urticaria |
| CAPS | Cryopyrin associated periodic syndrome |
References
- EURORDIS. 2017 Juggling Care and Daily Life: The Balancing Act of the Rare Disease Community; EURORDIS: Paris, France, 2017. [Google Scholar]
- Archived: WHO Timeline—COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 21 June 2021).
- Siegler, J.E.; Heslin, M.E.; Thau, L.; Smith, A.; Jovin, T.G. Falling Stroke Rates during COVID-19 Pandemic at a Comprehensive Stroke Center. J. Stroke Cerebrovasc. Dis. 2020, 29, 104953. [Google Scholar] [CrossRef]
- Tam, C.-C.F.; Cheung, K.-S.; Lam, S.; Wong, A.; Yung, A.; Sze, M.; Lam, Y.-M.; Chan, C.; Tsang, T.-C.; Tsui, M.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on ST-Segment–Elevation Myocardial Infarction Care in Hong Kong, China. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006631. [Google Scholar] [CrossRef] [PubMed]
- MetabERN Collaboration Group; Lampe, C.; Dionisi-Vici, C.; Bellettato, C.M.; Paneghetti, L.; van Lingen, C.; Bond, S.; Brown, C.; Finglas, A.; Francisco, R.; et al. The Impact of COVID-19 on Rare Metabolic Patients and Healthcare Providers: Results from Two MetabERN Surveys. Orphanet J. Rare Dis. 2020, 15, 341. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.C.Y.; Ng, Y.N.C.; Jain, R.; Chung, B.H.Y. A Thematic Study: Impact of COVID-19 Pandemic on Rare Disease Organisations and Patients across Ten Jurisdictions in the Asia Pacific Region. Orphanet J. Rare Dis. 2021, 16, 119. [Google Scholar] [CrossRef]
- Castro, R.; Berjonneau, E.; Courbier, S. Learning from the Pandemic to Improve Care for Vulnerable Communities: The Perspectives and Recommendations from the Rare Disease Community. Int. J. Integr. Care 2021, 21, 12. [Google Scholar] [CrossRef]
- Sechi, A.; Macor, D.; Valent, S.; Da Riol, R.M.; Zanatta, M.; Spinelli, A.; Bianchi, K.; Bertossi, N.; Dardis, A.; Valent, F.; et al. Impact of COVID-19 Related Healthcare Crisis on Treatments for Patients with Lysosomal Storage Disorders, the First Italian Experience. Mol. Genet. Metab. 2020, 130, 170–171. [Google Scholar] [CrossRef]
- Schwartz, I.V.D.; Randon, D.N.; Monsores, N.; Moura de Souza, C.F.; Horovitz, D.D.G.; Wilke, M.V.M.B.; Brunoni, D. SARS-CoV-2 Pandemic in the Brazilian Community of Rare Diseases: A Patient Reported Survey. Am. J. Med. Genet. 2021, 187, 301–311. [Google Scholar] [CrossRef]
- Canadian Organization for Rare Disorders. Applying Lessons from COVID-19 to Better Healthcare for Rare Diseases; Canadian Organization for Rare Disorders: Toronto, ON, Canada, 2020. [Google Scholar]
- Rare Diseases Ireland. Living with a Rare Disease in Ireland during the COVID-19 Pandemic; Rare Diseases Ireland: Dublin, Ireland, 2020. [Google Scholar]
- National Organisation for Rare Disorders. COVID-19 Community Followup Survey Report: 92% of Rare Disease Patients Still Affected; National Organisation for Rare Disorders: Danbury, CT, USA, 2020. [Google Scholar]
- EURORDIS. Rare Disease Patients’ Experience of COVID-19; EURORDIS: Paris, France, 2020. [Google Scholar]
- EURORDIS. How Has COVID-19 Impacted People with Rare Diseases? EURORDIS: Paris, France, 2020. [Google Scholar]
- Limongelli, G.; Iucolano, S.; Monda, E.; Elefante, P.; De Stasio, C.; Lubrano, I.; Caiazza, M.; Mazzella, M.; Fimiani, F.; Galdo, M.; et al. Diagnostic Issues Faced by a Rare Disease Healthcare Network during COVID-19 Outbreak: Data from the Campania Rare Disease Registry. J. Public Health 2021, fdab137. [Google Scholar] [CrossRef]
- Kusztal, M.; Kłopotowski, M.; Bazan-Socha, S.; Błażejewska-Hyżorek, B.; Pawlaczyk, K.; Oko, A.; Krajewska, M.; Nowicki, M. Is Home-Based Therapy in Fabry Disease the Answer to Compelling Patients’ Needs during the COVID-19 Pandemic? Survey Results from the Polish FD Collaborative Group. Adv. Clin. Exp. Med. 2021, 30, 449–454. [Google Scholar] [CrossRef]
- Elmonem, M.A.; Belanger-Quintana, A.; Bordugo, A.; Boruah, R.; Cortès-Saladelafont, E.; Endrakanti, M.; Giraldo, P.; Grünert, S.C.; Gupta, N.; Kabra, M.; et al. The Impact of COVID-19 Pandemic on the Diagnosis and Management of T Inborn Errors of Metabolism: A Global Perspective. Mol. Genet. Metab. 2020, 131, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Andrade-Campos, M.; Escuder-Azuara, B.; de Frutos, L.L.; Serrano-Gonzalo, I.; Giraldo, P. Direct and Indirect Effects of the SARS-CoV-2 Pandemic on Gaucher Disease Patients in Spain: Time to Reconsider Home-Based Therapies? Blood Cells Mol. Dis. 2020, 85, 102478. [Google Scholar] [CrossRef]
- Chung, C.C.Y.; Wong, W.H.S.; Fung, J.L.F.; Hong Kong, R.D.; Chung, B.H.Y. Impact of COVID-19 Pandemic on Patients with Rare Disease in Hong Kong. Eur. J. Med Genet. 2020, 63, 104062. [Google Scholar] [CrossRef]
- Koronawirus w Niedzielę 30 Maja. Niespełna 600 Zakażeń i 56 Zgonów. Available online: https://biqdata.wyborcza.pl/biqdata/7,159116,27143472,koronawirus-w-niedziele-30-maja-niespelna-600-zakazen-i-56.html (accessed on 22 June 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Fierro, L.; Nesheiwat, N.; Naik, H.; Narayanan, P.; Mistry, P.K.; Balwani, M. Gaucher Disease and SARS-CoV-2 Infection: Experience from 181 Patients in New York. Mol. Genet. Metab. 2021, 132, 44–48. [Google Scholar] [CrossRef]
- Pierzynowska, K.; Gaffke, L.; Węgrzyn, G. Transcriptomic Analyses Suggest That Mucopolysaccharidosis Patients May Be Less Susceptible to COVID-19. FEBS Lett. 2020, 594, 3363–3370. [Google Scholar] [CrossRef]
- Gómez-Luján, M.; Cruzalegui, C.; Aguilar, C.; Alvarez-Vargas, M.; Segura-Saldaña, P. When Frequent (Pandemic) Occurs in a Non-Frequent Disease: COVID-19 and Fabry Disease: Report of Two Cases. Jpn. J. Infect. Dis. 2021, 74, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Zimran, A.; Szer, J.; Revel-Vilk, S. Impact of Gaucher Disease on COVID-19. Intern. Med. J. 2020, 50, 894–895. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and Coagulation: Bleeding and Thrombotic Manifestations of SARS-CoV-2 Infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Lazzaroni, M.G.; Piantoni, S.; Masneri, S.; Garrafa, E.; Martini, G.; Tincani, A.; Andreoli, L.; Franceschini, F. Coagulation Dysfunction in COVID-19: The Interplay between Inflammation, Viral Infection and the Coagulation System. Blood Rev. 2021, 46, 100745. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Ginsberg, L. Natural History of the Cerebrovascular Complications of Fabry Disease: Cerebrovascular Complications of Fabry Disease. Acta Paediatr. 2007, 94, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Reisin, R.C.; Rozenfeld, P.; Bonardo, P. Fabry Disease Patients Have an Increased Risk of Stroke in the COVID-19 ERA. A Hypothesis. Med. Hypotheses 2020, 144, 110282. [Google Scholar] [CrossRef]
- Sturley, S.L.; Rajakumar, T.; Hammond, N.; Higaki, K.; Márka, Z.; Márka, S.; Munkacsi, A.B. Potential COVID-19 Therapeutics from a Rare Disease: Weaponizing Lipid Dysregulation to Combat Viral Infectivity. J. Lipid Res. 2020, 61, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Ballout, R.A.; Sviridov, D.; Bukrinsky, M.I.; Remaley, A.T. The Lysosome: A Potential Juncture between SARS-CoV-2 Infectivity and Niemann-Pick Disease Type C, with Therapeutic Implications. FASEB J. 2020, 34, 7253–7264. [Google Scholar] [CrossRef] [PubMed]
- Moutsopoulos, H.M. Anti-Inflammatory Therapy May Ameliorate the Clinical Picture of COVID-19. Ann. Rheum. Dis. 2020, 79, 1253–1254. [Google Scholar] [CrossRef] [PubMed]
- Haslak, F.; Yildiz, M.; Adrovic, A.; Sahin, S.; Koker, O.; Aliyeva, A.; Barut, K.; Kasapcopur, O. Management of Childhood-Onset Autoinflammatory Diseases during the COVID-19 Pandemic. Rheumatol. Int. 2020, 40, 1423–1431. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No of Patients | |||
|---|---|---|---|
| Total | On Treatment | SARS-COV-2 (+) | |
| Pediatric | 1101 | 137 | 19 |
| Adult | 625 | 109 | 25 |
| Group of IMD patients followed at the centre | |||
| No of healthcare units | |||
| Only pediatric | 6 | ||
| Only adult | 21 | ||
| Both | 5 | ||
| Number of treated patients in the centre | |||
| No of healthcare units | |||
| 1 | 12 | ||
| 2 to 4 | 11 | ||
| 5 to 50 | 5 | ||
| 50 and more | 4 | ||
| Diagnosis | No of Adults | No of Children | Severity of COVID-19 Symptoms | No of Hospitalised Patients | Cause of Hospitalisation |
|---|---|---|---|---|---|
| MPS II | 0 | 6 | mild-6/6 | 0 | n/a |
| MPS IV | 1 | 0 | moderate (dyspnea) 1/1 | 0 | n/a |
| Gaucher disease t. I | 4 | 0 | mild-3/4, moderate 1/4 (dyspnea) | 1 | massive deep vein thrombosis (after SARS-COV-2 infection) |
| Gaucher disease t. III | 0 | 1 | mild 1/1 | 0 | n/a |
| Fabry disease | 3 | 2 | mild 5/5 | 1 (adult) | ischemic stroke during SARS-COV-2 infection |
| Pompe disease | 2 | 0 | mild 2/2 | 0 | n/a |
| NPC | 4 | 0 | mild 3/4death 1/4 | 1 | respiratory failure caused by massive bilateral pneumonia in the course of COVID-19 |
| NPB | 1 | 0 | mild 1/1 | 0 | n/a |
| Cystinosis | 1 | 0 | mild 1/1 | 0 | n/a |
| VLCADD | 0 | 1 | moderate 1/1 | 1 | dehydration and metabolic decompensation |
| Methylmalonic acidemia | 1 | 0 | moderate 1/1 (dyspnea, saturation decrease) | 0 | n/a |
| FCAS | 3 | 0 | mild 3/3 | 0 | n/a |
| CAPS | 3 | 0 | mild 3/3 | 0 | n/a |
| Schnitzler syndrome | 2 | 0 | mild 2/2 | 0 | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tobór-Świętek, E.; Sykut-Cegielska, J.; Bik-Multanowski, M.; Walczak, M.; Rokicki, D.; Kałużny, Ł.; Wierzba, J.; Pac, M.; Jahnz-Różyk, K.; Więsik-Szewczyk, E.; et al. COVID-19 Pandemic and Patients with Rare Inherited Metabolic Disorders and Rare Autoinflammatory Diseases—Organizational Challenges from the Point of View of Healthcare Providers. J. Clin. Med. 2021, 10, 4862. https://doi.org/10.3390/jcm10214862
Tobór-Świętek E, Sykut-Cegielska J, Bik-Multanowski M, Walczak M, Rokicki D, Kałużny Ł, Wierzba J, Pac M, Jahnz-Różyk K, Więsik-Szewczyk E, et al. COVID-19 Pandemic and Patients with Rare Inherited Metabolic Disorders and Rare Autoinflammatory Diseases—Organizational Challenges from the Point of View of Healthcare Providers. Journal of Clinical Medicine. 2021; 10(21):4862. https://doi.org/10.3390/jcm10214862
Chicago/Turabian StyleTobór-Świętek, Ewa, Jolanta Sykut-Cegielska, Mirosław Bik-Multanowski, Mieczysław Walczak, Dariusz Rokicki, Łukasz Kałużny, Joanna Wierzba, Małgorzata Pac, Karina Jahnz-Różyk, Ewa Więsik-Szewczyk, and et al. 2021. "COVID-19 Pandemic and Patients with Rare Inherited Metabolic Disorders and Rare Autoinflammatory Diseases—Organizational Challenges from the Point of View of Healthcare Providers" Journal of Clinical Medicine 10, no. 21: 4862. https://doi.org/10.3390/jcm10214862
APA StyleTobór-Świętek, E., Sykut-Cegielska, J., Bik-Multanowski, M., Walczak, M., Rokicki, D., Kałużny, Ł., Wierzba, J., Pac, M., Jahnz-Różyk, K., Więsik-Szewczyk, E., & Kieć-Wilk, B. (2021). COVID-19 Pandemic and Patients with Rare Inherited Metabolic Disorders and Rare Autoinflammatory Diseases—Organizational Challenges from the Point of View of Healthcare Providers. Journal of Clinical Medicine, 10(21), 4862. https://doi.org/10.3390/jcm10214862