
Association between Pulpal-Periapical Pathology and Autoimmune Diseases: A Systematic Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Study Data
2.5. Quality Assessment
3. Results
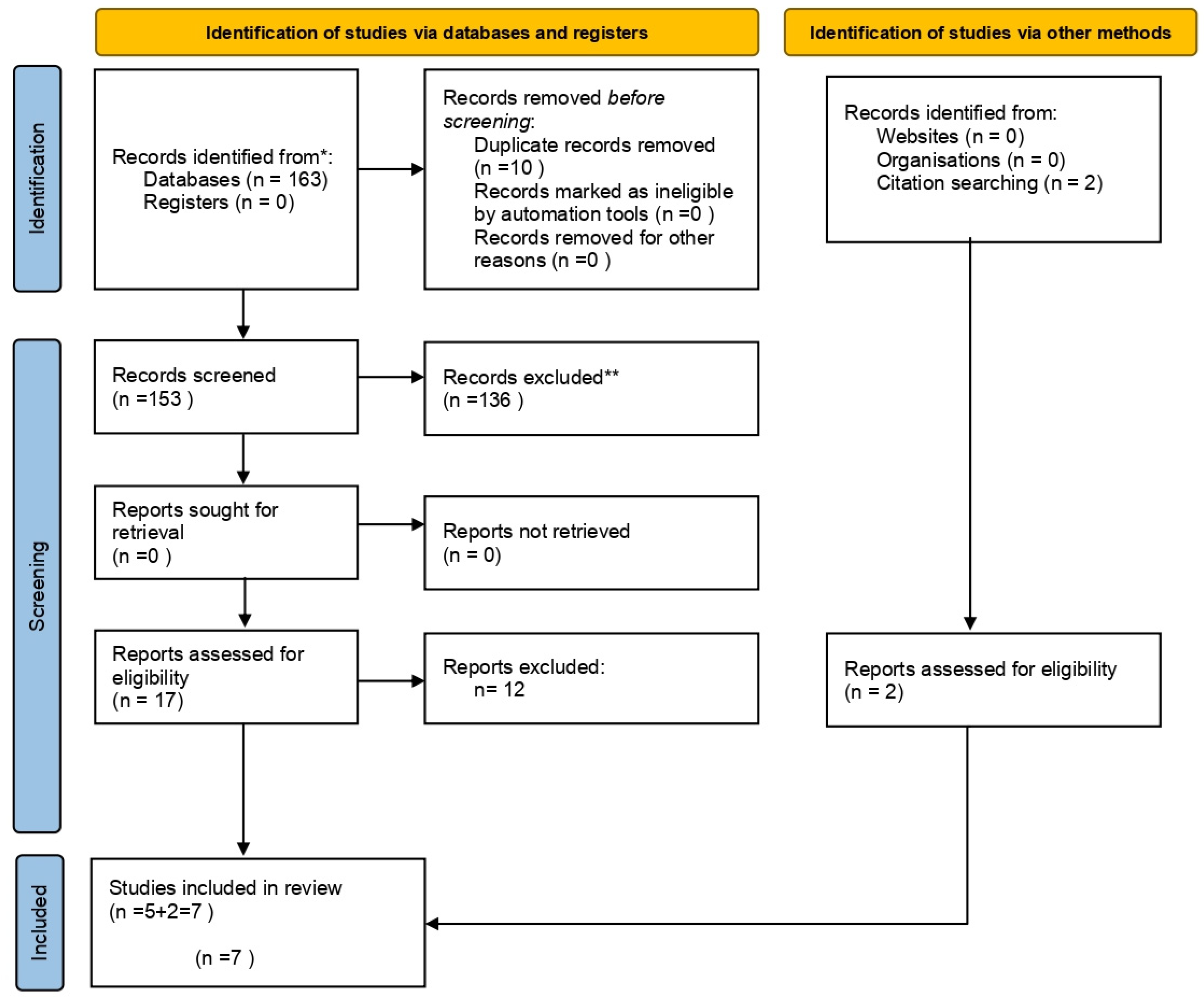
3.1. Study Selection and Flow Diagram
3.2. Study Characteristics
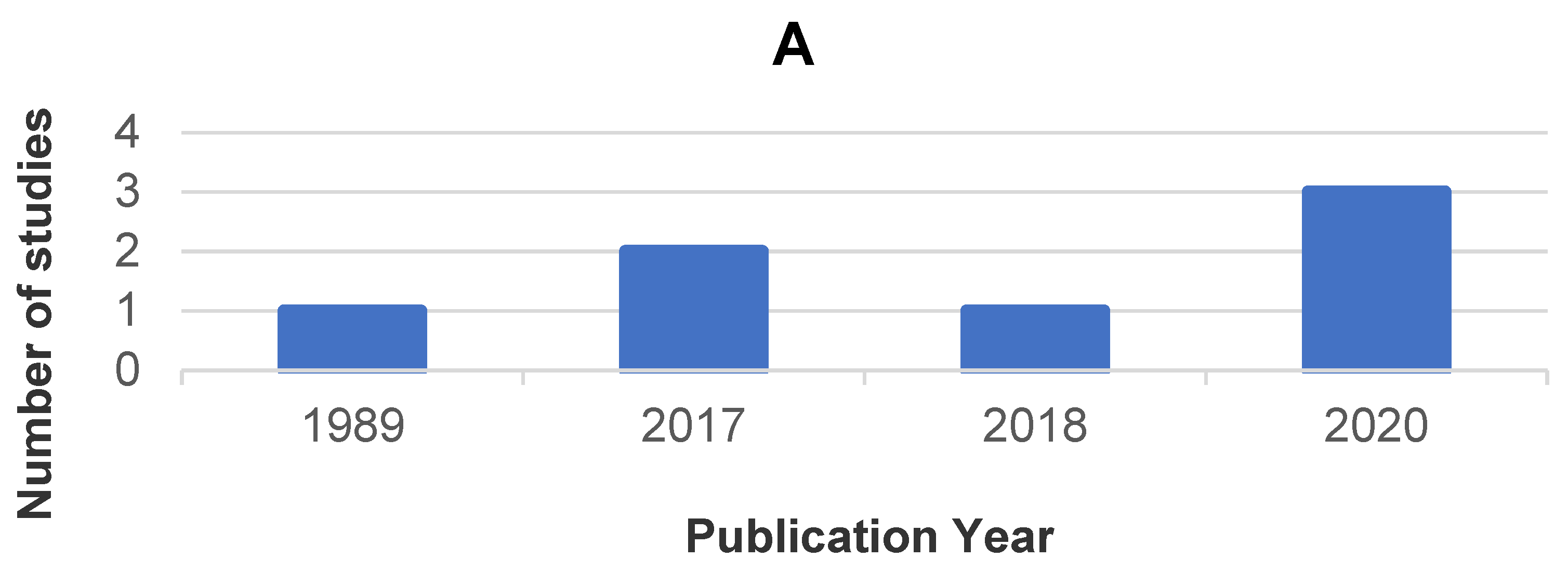
3.2.1. Bibliometric Analysis
3.2.2. Type of Autoimmune Disease
3.2.3. Study Type
3.2.4. Sample and Groups
3.2.5. Diagnostic Criteria for Apical Periodontitis
3.2.6. Association between Autoimmune Disease and Apical Periodontitis
3.2.7. Analyzed Variables
3.3. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zero, D.T.; Zandona, A.F.; Vail, M.M.; Spolnik, K.J. Dental caries and pulpal disease. Dent. Clin. N. Am. 2011, 55, 29–46. [Google Scholar] [CrossRef]
- American Association of Endodontists. Endodontic Diagnosis. 2013. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/endodonticdiagnosisfall2013.pdf (accessed on 19 October 2021).
- Gomes, B.; Herrera, D.R. Etiologic role of root canal infection in apical periodontitis and its relationship with clinical symptomatology. Braz. Oral. Res. 2018, 32, e69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngo, S.T.; Steyn, F.J.; McCombe, P.A. Gender differences in autoimmune disease. Front. Neuroendocr. 2014, 35, 347–369. [Google Scholar] [CrossRef] [Green Version]
- Gravina, G.; Wasén, C.; Garcia-Bonete, M.J.; Turkkila, M.; Erlandsson, M.C.; Töyrä Silfverswärd, S.; Brisslert, M.; Pullerits, R.; Andersson, K.M.; Katona, G.; et al. Survivin in autoimmune diseases. Autoimmun. Rev. 2017, 16, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulou, C.; Nikoleri, D.; Bertsias, G. Immunometabolism: An overview and therapeutic prospects in autoimmune diseases. Immunotherapy 2019, 11, 813–829. [Google Scholar] [CrossRef] [PubMed]
- Surace, A.E.A.; Hedrich, C.M. The Role of Epigenetics in Autoimmune/Inflammatory Disease. Front. Immunol. 2019, 10, 1525. [Google Scholar] [CrossRef] [Green Version]
- Cooper, G.S.; Stroehla, B.C. The epidemiology of autoimmune diseases. Autoimmun. Rev. 2003, 2, 119–125. [Google Scholar] [CrossRef]
- Wolf, V.L.; Ryan, M.J. Autoimmune Disease-Associated Hypertension. Curr. Hypertens. Rep. 2019, 21, 10. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, F.S.; Gershwin, M.E. Human autoimmune diseases: A comprehensive update. J. Intern. Med. 2015, 278, 369–395. [Google Scholar] [CrossRef]
- Shu, S.A.; Wang, J.; Tao, M.H.; Leung, P.S. Gene Therapy for Autoimmune Disease. Clin. Rev. Allergy Immunol. 2015, 49, 163–176. [Google Scholar] [CrossRef]
- Chandrashekara, S. The treatment strategies of autoimmune disease may need a different approach from conventional protocol: A review. Indian J. Pharm. 2012, 44, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Stojanovich, L.; Marisavljevich, D. Stress as a trigger of autoimmune disease. Autoimmun. Rev. 2008, 7, 209–213. [Google Scholar] [CrossRef]
- John, V.; Alqallaf, H.; De Bedout, T. Periodontal Disease and Systemic Diseases: An Update for the Clinician. J. Indiana Dent. Assoc. 2016, 95, 16–23. [Google Scholar]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Cavalla, F.; Letra, A.; Silva, R.M.; Garlet, G.P. Determinants of Periodontal/Periapical Lesion Stability and Progression. J. Dent. Res. 2021, 100, 29–36. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Martin-Gonzalez, J.; Castellanos-Cosano, L. Endodontic medicine: Connections between apical periodontitis and systemic diseases. Int. Endod. J. 2015, 48, 933–951. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef]
- Cintra, L.T.A.; Estrela, C.; Azuma, M.M.; Queiroz, Í.O.A.; Kawai, T.; Gomes-Filho, J.E. Endodontic medicine: Interrelationships among apical periodontitis, systemic disorders, and tissue responses of dental materials. Braz. Oral Res. 2018, 32, e68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiou, A.C.; Crielaard, W.; Armenis, I.; de Vries, R.; van der Waal, S.V. Apical Periodontitis Is Associated with Elevated Concentrations of Inflammatory Mediators in Peripheral Blood: A Systematic Review and Meta-analysis. J. Endod. 2019, 45, 1279–1295. [Google Scholar] [CrossRef]
- An, G.K.; Morse, D.E.; Kunin, M.; Goldberger, R.S.; Psoter, W.J. Association of Radiographically Diagnosed Apical Periodontitis and Cardiovascular Disease: A Hospital Records-based Study. J. Endod. 2016, 42, 916–920. [Google Scholar] [CrossRef]
- Sisli, S.N. Evaluation of the Relationship between Type II Diabetes Mellitus and the Prevalence of Apical Periodontitis in Root-Filled Teeth Using Cone Beam Computed Tomography: An Observational Cross-Sectional Study. Med. Princ. Pract. 2019, 28, 533–538. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Karataş, E.; Kul, A.; Tepecik, E. Association between Rheumatoid Arthritis and Apical Periodontitis: A Cross-sectional Study. Eur. Endod. J. 2020, 5, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Jalali, P.; Glickman, G.N.; Schneiderman, E.D.; Schweitzer, J.L. Prevalence of Periapical Rarefying Osteitis in Patients with Rheumatoid Arthritis. J. Endod. 2017, 43, 1093–1096. [Google Scholar] [CrossRef]
- Limeira, F.I.R.; Arantes, D.C.; de Souza Oliveira, C.; de Melo, D.P.; Magalhães, C.S.; Bento, P.M. Root Canal Treatment and Apical Periodontitis in a Brazilian Population with Type 1 Diabetes Mellitus: A Cross-sectional Paired Study. J. Endod. 2020, 46, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Falk, H.; Hugoson, A.; Thorstensson, H. Number of teeth, prevalence of caries and periapical lesions in insulin-dependent diabetics. Scand. J. Dent. Res. 1989, 97, 198–206. [Google Scholar] [CrossRef]
- Poyato-Borrego, M.; Segura-Sampedro, J.J.; Martin-Gonzalez, J.; Torres-Dominguez, Y.; Velasco-Ortega, E.; Segura-Egea, J.J. High Prevalence of Apical Periodontitis in Patients With Inflammatory Bowel Disease: An Age- and Gender-matched Case-control Study. Inflamm. Bowel Dis. 2020, 26, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Cotti, E.; Mezzena, S.; Schirru, E.; Ottonello, O.; Mura, M.; Ideo, F.; Susnik, M.; Usai, P. Healing of Apical Periodontitis in Patients with Inflammatory Bowel Diseases and under Anti-tumor Necrosis Factor Alpha Therapy. J. Endod. 2018, 44, 1777–1782. [Google Scholar] [CrossRef]
- Piras, V.; Usai, P.; Mezzena, S.; Susnik, M.; Ideo, F.; Schirru, E.; Cotti, E. Prevalence of Apical Periodontitis in Patients with Inflammatory Bowel Diseases: A Retrospective Clinical Study. J. Endod. 2017, 43, 389–394. [Google Scholar] [CrossRef]
- Martinho, F.C.; Nascimento, G.G.; Leite, F.R.; Gomes, A.P.; Freitas, L.F.; Camões, I.C. Clinical influence of different intracanal medications on Th1-type and Th2-type cytokine responses in apical periodontitis. J. Endod. 2015, 41, 169–175. [Google Scholar] [CrossRef]
- Martinho, F.C.; Chiesa, W.M.; Leite, F.R.; Cirelli, J.A.; Gomes, B.P. Correlation between clinical/radiographic features and inflammatory cytokine networks produced by macrophages stimulated with endodontic content. J. Endod. 2012, 38, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Marending, M.; Peters, O.A.; Zehnder, M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 119–124. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Martín-González, J.; Cabanillas-Balsera, D.; Fouad, A.F.; Velasco-Ortega, E.; López-López, J. Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: Systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Aggarwal, V.; Mehta, N.; Abraham, D.; Singh, A. Diabetes mellitus and the healing of periapical lesions in root filled teeth: A systematic review and meta-analysis. Int. Endod. J. 2020, 53, 1472–1484. [Google Scholar] [CrossRef]
- Gutmann, J.L.; Baumgartner, J.C.; Gluskin, A.H.; Hartwell, G.R.; Walton, R.E. Identify and define all diagnostic terms for periapical/periradicular health and disease states. J. Endod. 2009, 35, 1658–1674. [Google Scholar] [CrossRef]
- Jakovljevic, A.; Nikolic, N.; Jacimovic, J.; Pavlovic, O.; Milicic, B.; Beljic-Ivanovic, K.; Miletic, M.; Andric, M.; Milasin, J. Prevalence of Apical Periodontitis and Conventional Nonsurgical Root Canal Treatment in General Adult Population: An Updated Systematic Review and Meta-analysis of Cross-sectional Studies Published between 2012 and 2020. J. Endod. 2020, 46, 1371–1386. [Google Scholar] [CrossRef]
- Tiburcio-Machado, C.S.; Michelon, C.; Zanatta, F.B.; Gomes, M.S.; Marin, J.A.; Bier, C.A. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 2021, 54, 712–735. [Google Scholar] [CrossRef]
- Giardino, L.; Grande, N.M.; Savadori, P.; Fabbro, M.D.; Plotino, G. Clinical and Histological Findings of Post-Treatment Infection in the Presence of Vertical Root Fracture and Apical Periodontitis: Case Reports. Eur. Endod. J. 2019, 4, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Leonardi Dutra, K.; Haas, L.; Porporatti, A.L.; Flores-Mir, C.; Nascimento Santos, J.; Mezzomo, L.A.; Correa, M.; De Luca Canto, G. Diagnostic Accuracy of Cone-beam Computed Tomography and Conventional Radiography on Apical Periodontitis: A Systematic Review and Meta-analysis. J. Endod. 2016, 42, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Teh, L.A.; Abdullah, D.; Liew, A.K.C.; Soo, E. Evaluation of Pulpal Involvement, Ulceration, Fistula, and Abscess Index and Periapical Index in Screening for Endodontic Disease: Reliability and Accuracy. J. Endod. 2020, 46, 748–755. [Google Scholar] [CrossRef]
- Shivashankar, V.Y.; Johns, D.A.; Maroli, R.K.; Sekar, M.; Chandrasekaran, R.; Karthikeyan, S.; Renganathan, S.K. Comparison of the Effect of PRP, PRF and Induced Bleeding in the Revascularization of Teeth with Necrotic Pulp and Open Apex: A Triple Blind Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, zc34–zc39. [Google Scholar] [CrossRef]
- Olcay, K.; Eyüboglu, T.F.; Özcan, M. Clinical outcomes of non-surgical multiple-visit root canal retreatment: A retrospective cohort study. Odontology 2019, 107, 536–545. [Google Scholar] [CrossRef]
- Lamkanfi, M.; Dixit, V.M. Mechanisms and functions of inflammasomes. Cell 2014, 157, 1013–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalighinejad, N.; Aminoshariae, M.R.; Aminoshariae, A.; Kulild, J.C.; Mickel, A.; Fouad, A.F. Association between Systemic Diseases and Apical Periodontitis. J. Endod. 2016, 42, 1427–1434. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.C. Association of Functional Gene Polymorphism with Apical Periodontitis. J. Endod. 2015, 41, 999–1007. [Google Scholar] [CrossRef]
- Peddis, N.; Musu, D.; Ideo, F.; Rossi-Fedele, G.; Cotti, E. Interaction of biologic therapy with apical periodontitis and periodontitis: A systematic review. Aust. Dent. J. 2019, 64, 122–134. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Field 1 | “autoimmune disease” OR “autoimmunity” |
| AND | |
| Field 2 | “periapical lesion” OR “apical periodontitis” OR “irreversible pulpitis” OR “endodontic” OR “root canal treatment” |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies including patients with pulpal-periapical pathology and autoimmune disease. | Studies that include any pathology other than pulpal-periapical in patients with autoimmune disease. |
| Case-control studies, cohort studies, cross-sectional descriptive studies, systematic reviews, and meta-analyses | Clinical cases |
| Human studies | Animal studies |
| Studies in English and Spanish | Studies in any language other than English or Spanish |
| Search Strategy | #1 | “autoimmune disease“ OR “autoimmunity” |
| #2 | “periapical lesion” OR “apical periodontitis” OR “irreversible pulpitis“ OR “endodontic” OR “root canal treatment” | |
| #1 AND #2 | (“autoimmune disease” OR “autoimmunity”) AND (“periapical lesion” OR “apical periodontitis” OR “irreversible pulpitis” OR endodontic OR “root canal treatment”) | |
| Database | Search Strategy | Findings |
| MEDLINE | #1 | 494.844 |
| #2 | 47.639 | |
| #1 AND #2 | 113 | |
| SciELO | #1 | 2.093 |
| #2 | 91 | |
| #1 AND #2 | 0 | |
| Cochrane Library | #1 | 82 |
| #2 | 18 | |
| #1 AND #2 | 1 | |
| Web of Science | #1 | 302.106 |
| #2 | 34.210 | |
| #1 AND #2 | 33 | |
| Scopus | #1 | 215.584 |
| #2 | 1.185 | |
| #1 AND #2 | 16 |
| Author and Year | Autoimmune Disease | Study Type | Sample and Groups | Diagnostic Criteria for AP | Results of Interest | Association AD and AP |
|---|---|---|---|---|---|---|
| Karatas et al., 2020 [26] | Rheumatoid Arthritis | Cross-sectional | n = 96 patients, 2051 teeth SG = 48 patients, 1026 teeth CG = 48 patients, 1025 teeth | Periapical XR Clinical examination Periapical Index (PAI) | ≤1 teeth with AP in SG: 4.3%, in CG: 2% (OR = 2.193; p = 0.003) | Yes |
| RCT+AP in patients in SG: 10.4%, in CG: 12.5% (OR = 0.473; p = 0.375) | No | |||||
| Patients with AP in SG: 47.9%, in CG: 29,7% (OR = 3,087; p = 0.027) | Yes | |||||
| Jalali et al., 2017 [27] | Rheumatoid Arthritis | Case-control | n = 162 patients, 6855 teeth SG = 131 patients, 3260 teeth CG = 131 patients, 3395 teeth | Panoramic XR Periapical XR Periapical Index (PAI) | ≤1 teeth with AP in SG: 3.96%, in CG: 3.53% (p = 0.364) | No |
| ≤1 teeth with RCT+AP in SG: 24.1%, in CG: 30,7% (p = 0.142) | No | |||||
| Patients with AP in SG: 49.6%, in CG: 54.2% (p = 0.458) | No | |||||
| Poyato-Borrego et al., 2020 [30] | Inflammatory Bowel Disease | Case-control | n = 108 patients SG = 54 patients CG = 54 patients | Panoramic XR Periapical Index (PAI) | ≤1 teeth with AP in SG: 35.2%, in CG: 16.7% (OR = 2.75; p = 0.03) | Yes |
| ≤1 teeth with RCT+AP in SG: 48.3%, in CG: 36.4% (OR = 1.63; p = 0.39) | No | |||||
| Cotti et al., 2018 [31] | Inflammatory Bowel Disease | Case-control | n = 33 patients, n = 44 teeth with AP SG = 19 patients, 22 teeth with AP CG = 14 patients, 22 teeth with AP | Periapical XR Clinical examination Periapical Index (PAI) | Cure rate at 3 months in SG: 100%, in CG: 95.5% (p = 1.00). Cure rate at 2 years in SG: 100%, in CG: 81.8% (p = 0.108) | Yes, there is a higher cure rate in SG with biological therapy |
| Piras et al., 2017 [32] | Inflammatory Bowel Disease | Case-control | n = 220 patients SG = 110 patients CG = 110 patients | Panoramic XR Clinical examination: Periapical XR Periapical Index (PAI) | Patients with AP in SG: 64%, in CG: 59% (p > 0.05) | No |
| Number of teeth with AP higher in SG than CG (p > 0.05) | No | |||||
| Higher risk of AP in women of SG than CG (p > 0.05) | No | |||||
| The number of teeth with AP was higher in SG woman than CG (p < 0.05) | Yes | |||||
| Limeira et al., 2020 [28] | Diabetes mellitus type 1 | Cross-sectional | n= 150 patients SG = 50 patients CG = 100 patients | Panoramic XR Periapical Index (PAI) | Patients with PA in SG: 58%, in CG: 15% (OR = 3.508; p = 0.011) | Yes |
| Patients with RCT+AP in SG: 52%, in CG: 8% (OR = 7.220; p = 0.00) | Yes | |||||
| Falk et al., 1989 [29] | Diabetes mellitus type 1 | Case-control | n = 231 SG = 154 patients CG = 77 patients | Periapical XR Bitewing XR | Higher frequency of RCT+AP in LTD than CG | No |
| Women: LTD higher % of RCT+AP than STD and non-diabetics (p < 0.01) | Yes, only in women | |||||
| LTD 40%, SDD 15% and non-diabetics 23% have ≥2 teeth with AP (p < 0.001) | Yes |
| Gender | Age | Smoking Habit | Teeth with AP | Teeth with RCT | Teeth with RCT+AP | Patients with AP | Patients with RCT | Patients with RCT+AP | Quality of RCT | |
|---|---|---|---|---|---|---|---|---|---|---|
| Karatas et al. [26] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | No |
| Jalali et al. [27] | No | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Yes |
| Poyato-Borrego et al. [30] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | No | No |
| Cotti et al. [31] | Yes | Yes | No | No | No | No | No | No | No | Yes |
| Piras et al. [32] | Yes | No | No | Yes | No | No | Yes | No | No | No |
| Limeira et al. [28] | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Falk et al. [29] | Yes | No | No | Yes | Yes | Yes | No | No | No | No |
| Total of studies | 6 | 5 | 3 | 5 | 3 | 3 | 4 | 3 | 2 | 3 |
| Methods | ||
| Setting | 1 | Describes the setting, participating locations, relevant dates (period of recruitment, exposure, follow-up, data collection) |
| Participants | 2 | Gives the inclusion and exclusion criteria (including paired or control groups) |
| 3 | Describes autoimmune disease history | |
| Variables | 4 | Clearly defines apical periodontitis and its diagnostic criteria |
| Data sources/measurement | 5 | Describes methods of evaluation of apical periodontitis |
| Study size | 6 | Explains how the study sample size was arrived at |
| Statistical methods | 7 | Describes statistical methods, including those used to control for confounders |
| 8 | Describes any methods used to examine subgroups and interactions | |
| Results | ||
| Descriptive data | 9 | Provides characteristics of study participants (e.g., demographic, clinical, social) and reports on exposures and potential confounders |
| 10 | Indicates the number of participants with missing data and explains how this was addressed | |
| Outcome data | 11 | Measures and presents exposure data |
| Falk et al. [29] | Limeira et al. [28] | Poyato-Borrego et al. [30] | Cotti et al. [31] | Piras et al. [32] | Karatas et al. [26] | Jalali et al. [27] | |
|---|---|---|---|---|---|---|---|
| 1 | ✓ | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ |
| 2 | ✕ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ |
| 3 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ |
| 4 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 5 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 6 | ✕ | ✓ | ✓ | ✕ | ✕ | ✓ | ✕ |
| 7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| 9 | ✕ | ✓ | ✓ | ✕ | ✓ | ✓ | ✕ |
| 10 | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✕ |
| 11 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Total Score Risk of Bias | 7 Moderate | 9 Low | 10 Low | 6 Moderate | 9 Low | 11 Low | 7 Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero-Gironés, J.; Ros-Valverde, A.; Pecci-Lloret, M.P.; Rodríguez-Lozano, F.J.; Pecci-Lloret, M.R. Association between Pulpal-Periapical Pathology and Autoimmune Diseases: A Systematic Review. J. Clin. Med. 2021, 10, 4886. https://doi.org/10.3390/jcm10214886
Guerrero-Gironés J, Ros-Valverde A, Pecci-Lloret MP, Rodríguez-Lozano FJ, Pecci-Lloret MR. Association between Pulpal-Periapical Pathology and Autoimmune Diseases: A Systematic Review. Journal of Clinical Medicine. 2021; 10(21):4886. https://doi.org/10.3390/jcm10214886
Chicago/Turabian StyleGuerrero-Gironés, Julia, Antonio Ros-Valverde, María Pilar Pecci-Lloret, Francisco Javier Rodríguez-Lozano, and Miguel Ramón Pecci-Lloret. 2021. "Association between Pulpal-Periapical Pathology and Autoimmune Diseases: A Systematic Review" Journal of Clinical Medicine 10, no. 21: 4886. https://doi.org/10.3390/jcm10214886
APA StyleGuerrero-Gironés, J., Ros-Valverde, A., Pecci-Lloret, M. P., Rodríguez-Lozano, F. J., & Pecci-Lloret, M. R. (2021). Association between Pulpal-Periapical Pathology and Autoimmune Diseases: A Systematic Review. Journal of Clinical Medicine, 10(21), 4886. https://doi.org/10.3390/jcm10214886