
The Electrical Activity of the Orbicularis Oris Muscle in Children with Down Syndrome—A Preliminary Study

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Population
2.3. Experimental Procedures
2.3.1. Clinical Examination
2.3.2. Electromyographical Assessment of the Orbicularis Oris Muscle Activity
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Da Silva Alves Pinheiro, D.L.; dos Santos Alves, G.A.; Montenegro Fausto, F.M.; de Figueiredo Pessoa, L.S.; da Silva, L.A.; de Freitas Pereira, S.A.; Alves de Almeida, L.N. Effects of electrostimulation associated with masticatory training in individuals with down syndrome. CoDAS 2018, 30, e20170074. [Google Scholar]
- Giannasi, L.C.; Dutra, M.T.S.; Tenguan, V.L.S.; Mancilha, G.P.; Silva, G.L.C.; Fillietaz-Bacigalupo, E.; da Silva, D.B.; Politti, F.; Nacif, S.R.; de Oliveira, E.F.; et al. Evaluation of the masticatory muscle function, physiological sleep variables, and salivary parameters after electromechanical therapeutic approaches in adult patients with Down syndrome: A randomized controlled clinical trial. Trials 2019, 20, 215. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Sena, L.; Palma, L.F.; Marques, S.R.; Sanches, M.L.; Carvalho de Moraes, L.O. A home-based multidisciplinary programme for Down syndrome adults with muscular temporomandibular disorder. J. Oral Rehabil. 2020, 47, 939–943. [Google Scholar] [CrossRef]
- Mubayrik, A.B. The dental needs and treatment of patients with Down syndrome. Dent. Clin. N. Am. 2016, 60, 613–626. [Google Scholar] [CrossRef]
- Salgueiro, M.C.C.; Silva, T.; Motta, L.J.; Horliana, A.C.R.T.; Gonçalves, M.L.L.; Gomes, A.O.; Pinto, M.M.; Bortoletto, C.C.; Altavista, O.M.; Deana, A.M.; et al. Effects of Photobiomodulation in Children with Down Syndrome and Possible Sleep Bruxism: Protocol For A Randomized, Controlled, Blind, Clinical Trial: Study protocol clinical trial (SPIRIT compliant). Medicine 2020, 99, e19904. [Google Scholar] [CrossRef] [PubMed]
- Ruy Carneiro, N.C.; de Castro Souza, I.; Duda Deps Almeida, T.; Serra-Negra, J.M.C.; Almeida Pordeus, I.; Borges-Oliveira, A.C. Risk factors associated with reported bruxism among children and adolescents with Down Syndrome. Cranio 2018, 38, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Gallo, C.; Pastore, I.; Beghetto, M.; Mucignat-Caretta, C. Symmetry of dental agenesis in down syndrome children. J. Dent. Sci. 2019, 14, 61–65. [Google Scholar] [CrossRef]
- Kaczorowska, N.; Kaczorowski, K.; Laskowska, J.; Mikulewicz, M. Down syndrome as a cause of abnormalities in the craniofacial region: A systematic literature review. Adv. Clin. Exp. Med. 2019, 28, 1587–1592. [Google Scholar] [CrossRef] [Green Version]
- Nęcka, A.; Kawala, B.; Matthews-Brzozowska, T. Evaluation of facial muscle tone using surface electromyography in children with Down’s syndrome. Ann. Acad. Med. Stetin. 2007, 53, 98–101. [Google Scholar]
- Szyszka-Sommerfeld, L.; Machoy, M.; Lipski, M.; Woźniak, K. The diagnostic value of electromyography in identifying patients with pain-related temporomandibular disorders. Front. Neurol. 2019, 10, 180. [Google Scholar] [CrossRef]
- Szyszka-Sommerfeld, L.; Budzyńska, A.; Lipski, M.; Kulesza, S.; Woźniak, K. Assessment of masticatory muscle function in patients with bilateral complete cleft lip and palate and posterior crossbite by means of electromyography. J. Healthc. Eng. 2020, 2020, 8828006. [Google Scholar] [CrossRef]
- Szyszka-Sommerfeld, L.; Lipski, M.; Woźniak, K. Surface electromyography as a method for diagnosing muscle function in patients with congenital maxillofacial abnormalities. J. Healthc. Eng. 2020, 2020, 8846920. [Google Scholar] [CrossRef]
- Woźniak, K.; Piątkowska, D.; Lipski, M.; Mehr, K. Surface electromyography in orthodontics-a literature review. Med. Sci. Monit. 2013, 19, 416–423. [Google Scholar]
- Woźniak, K.; Piątkowska, D.; Lipski, M. The influence of natural head position on the assessment of facial morphology. Adv. Clin. Exp. Med. 2012, 21, 743–749. [Google Scholar]
- Szyszka-Sommerfeld, L.; Machoy, M.; Wilczyński, S.; Lipski, M.; Woźniak, K. Superior orbicularis oris muscle activity in children surgically treated for bilateral complete cleft lip and palate. J. Clin. Med. 2021, 10, 1720. [Google Scholar] [CrossRef]
- Szyszka-Sommerfeld, L.; Woźniak, K.; Matthews-Brzozowska, T.; Kawala, B.; Mikulewicz, M. Electromyographic analysis of superior orbicularis oris muscle function in children surgically treated for unilateral complete cleft lip and palate. J. Craniomaxillofac. Surg. 2017, 45, 1547–1551. [Google Scholar] [CrossRef]
- Donaldson, S.; Donaldson, M. Multi-Channel EMG Assessment and Treatment Techniques. In Clinical EMG for Surface Recordings; Cram, J.R., Ed.; Clinical Resources: Nevada City, CA, USA, 1990; pp. 143–174. [Google Scholar]
- Christensen, L.V.; Hutching, M.O. Methodological observations on positive and negative work (teeth grinding) by human jaw muscles. J. Oral Rehabil. 1992, 19, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, M.; Ahlgren, J. Mentalis and orbicularis oris activity in children with incompetent lips: An electromyographic and cephalometric study. Acta Odontol. Scand. 1975, 33, 355–363. [Google Scholar] [CrossRef]
- Gamboa, N.A.; Miralles, R.; Valenzuela, S.; Santander, H.; Cordova, R.; Bull, R.; Espinoza, D.A.; Martínez, C.A. Comparison of muscle activity between subjects with or without lip competence: Electromyographic activity of lips, supra- and infrahyoid muscles. Cranio 2017, 35, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, N.; Ichida, T.; Yamaguchi, K. Electromyographic activity of lower lip muscles when chewing with the lips in contact and apart. Angle Orthod. 2004, 74, 31–36. [Google Scholar] [PubMed]
- Lipari, M.A.; Pimentel, G.; Gamboa, N.A.; Bayas, I.; Guerrero, N.; Miralles, R. Electromyographic Comparison of Lips and Jaw Muscles between Children With Competent and Incompetent Lips: A Cross Sectional Study. J. Clin. Pediatr. Dent. 2020, 44, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Tosello, D.O.; Vitti, M.; Berzin, F. EMG activity of the orbicularis oris and mentalis muscles in children with malocclusion, incompetent lips and atypical swallowing part I. J. Oral Rehabil. 1998, 25, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Störmer, K.; Pancherz, H. Electromyography of the perioral and masticatory muscles in orthodontic patients with atypical swallowing. J. Orofac. Orthop. 1999, 60, 13–23. [Google Scholar] [CrossRef]
- López-Soto, L.M.; López-Soto, O.P.; Osorio-Forero, A.; Restrepo, F.; Tamayo-Orrego, L. Muscle Activity and Muscle Strength in Atypical Swallowing. Salud Uninorte 2017, 33, 273–284. [Google Scholar] [CrossRef]
- Szyszka-Sommerfeld, L.; Woźniak, K.; Matthews-Brzozowska, T.; Kawala, B.; Mikulewicz, M.; Machoy, M. The electrical activity of the masticatory muscles in children with cleft lip and palate. Int. J. Paediatr. Dent. 2018, 28, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Lin, J.; Fu, M. Electromyographic investigation of masticatory muscles in unilateral cleft lip and palate patients with anterior crossbite. Cleft Palate Craniofac. J. 1998, 35, 415–418. [Google Scholar] [CrossRef]
- Ciccone de Faria Tdos, S.; Hallak Regalo, S.C.; Thomazinho, A.; Vitti, M.; de Felicĩo, C.M. Masticatory muscle activity in children with a skeletal or dentoalveolar open bite. Eur. J. Orthod. 2010, 32, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Nuño-Licona, A.; Cavazos, E., Jr.; Angeles-Medina, F. Electromyographic changes resulting from orthodontic correction of class III malocclusion. Int. J. Paediatr. Dent. 1993, 3, 71–76. [Google Scholar] [CrossRef]
- Merkel-Walsh, R. Orofacial myofunctional therapy with children ages 0-4 and individuals with special needs. Int. J. Orofac. Myol. 2020, 46, 22–36. [Google Scholar] [CrossRef]
- Saccucci, M.; Tecco, S.; Ierardoa, G.; Luzzi, V.; Festa, F.; Polimeni, A. Effects of interceptive orthodontics on orbicular muscle activity: A surface electromyographic study in children. J. Electromyogr. Kinesiol. 2011, 21, 665–671. [Google Scholar] [CrossRef]
- Castroflorio, T.; Farina, D.; Bottin, A.; Piancino, M.G.; Bracco, P.; Merletti, R. Surface EMG of jaw elevator muscles: Effect of electrode location and inter-electrode distance. J. Oral Rehabil. 2005, 32, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castroflorio, T.; Icardi, K.; Torsello, F.; Deregibus, A.; Debernardi, C.; Bracco, P. Reproducibility of surface EMG in the human masseter and anterior temporalis muscle areas. Cranio 2005, 23, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Hugger, S.; Schindler, H.J.; Kordass, B.; Hugger, A. Clinical relevance of surface EMG of the masticatory muscles. (Part 1): Resting activity, maximal and submaximal voluntary contraction, symmetry of EMG activity. Int. J. Comput. Dent. 2012, 15, 297–314. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | DS Group Mean Age 10.1 ± 1.1 | Control Group Mean Age 9.8 ± 1.0 | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Gender | Females | 6 | 40 | 7 | 46.7 |
| Males | 9 | 60 | 8 | 53.3 | |
| Total | 15 | 100 | 15 | 100 | |
| Lip seal | Competent | 0 | 0 | 15 | 100 |
| Incompetent | 15 | 100 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Atypical swallowing | No | 5 | 33.3 | 15 | 100 |
| Yes | 10 | 66.7 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Mode of breathing | Nasal | 7 | 46.7 | 15 | 100 |
| Mouth | 8 | 53.3 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Facial profile | Straight | 7 | 46.7 | 11 | 73.3 |
| Concave | 3 | 20 | 4 | 26.7 | |
| Convex | 5 | 33.3 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Vertical overlap | ≥0 <3 mm | 6 | 40 | 15 | 100 |
| ≥3 mm | 4 | 26.7 | 0 | 0 | |
| Reverse (anterior open bite) | 5 | 33.3 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Overjet | ≥0 <3 mm | 5 | 33.3 | 15 | 100 |
| ≥3 mm | 5 | 33.3 | 0 | 0 | |
| Negative (anterior crossbite) | 5 | 33.4 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Angle Class | I | 15 | 100 | 15 | 100 |
| II | 0 | 0 | 0 | 0 | |
| III | 0 | 0 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Posterior crossbite | No | 5 | 33.3 | 15 | 100 |
| Yes | 10 | 66.7 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Lateral open bite | No | 11 | 73.3 | 15 | 100 |
| Yes | 4 | 26.7 | 0 | 0 | |
| Total | 15 | 100 | 15 | 100 | |
| Activity | DS Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Min | Q1 | Mdn | Q3 | Max | n | Min | Q1 | Mdn | Q3 | Max | |
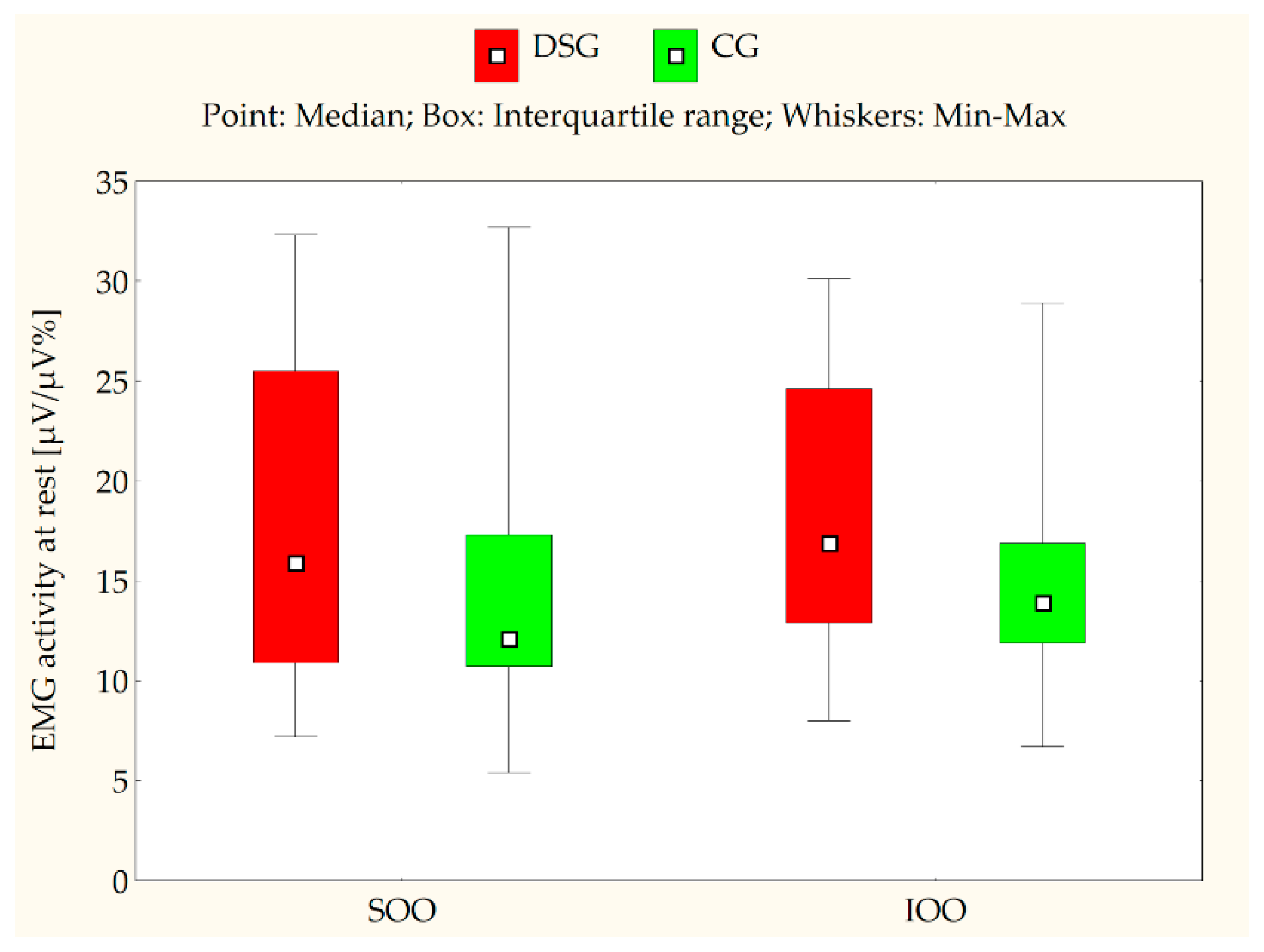
| Rest | 15 | 7.2 | 10.9 | 15.9 | 25.5 | 32.7 | 15 | 5.4 | 10.7 | 12.1 | 17.3 | 32.3 |
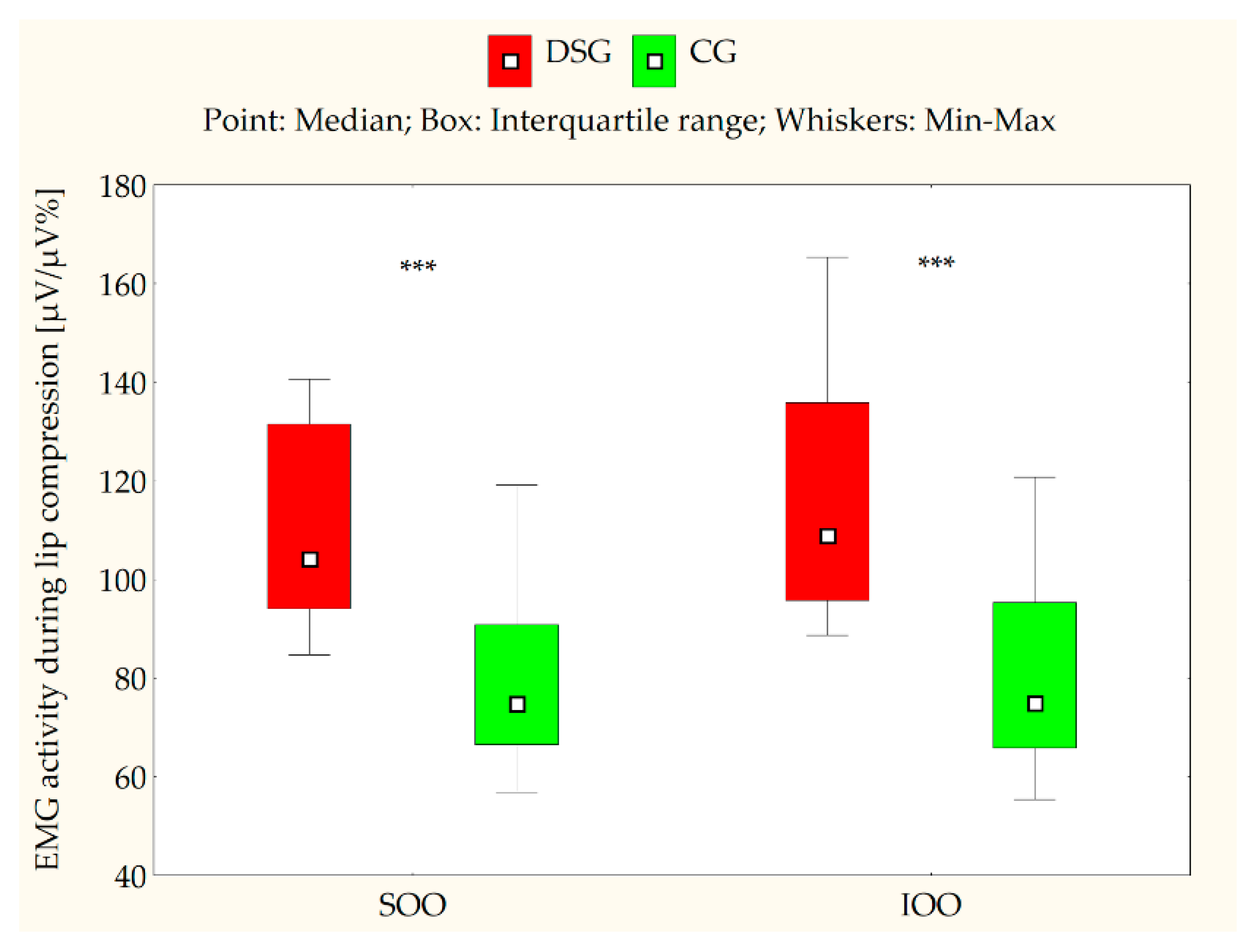
| Lip compression | 15 | 84.8 | 94.1 | 104.1 | 131.5 | 140.6 | 15 | 56.9 | 66.5 | 74.8 | 90.8 | 119.1 |
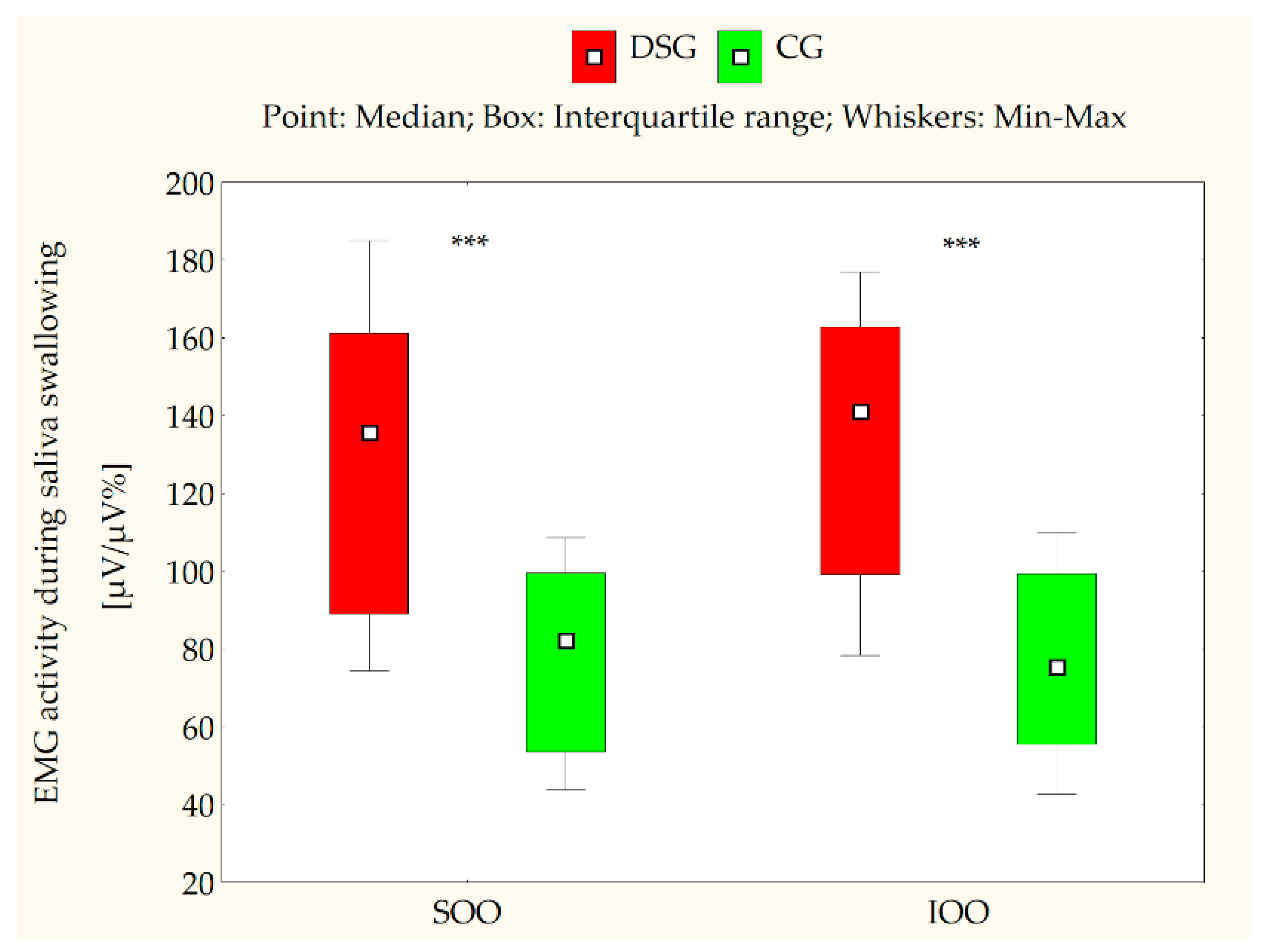
| Saliva swallowing | 15 | 74.3 | 89.1 | 135.7 | 161.2 | 185.0 | 15 | 43.8 | 53.6 | 82.3 | 99.5 | 108.6 |
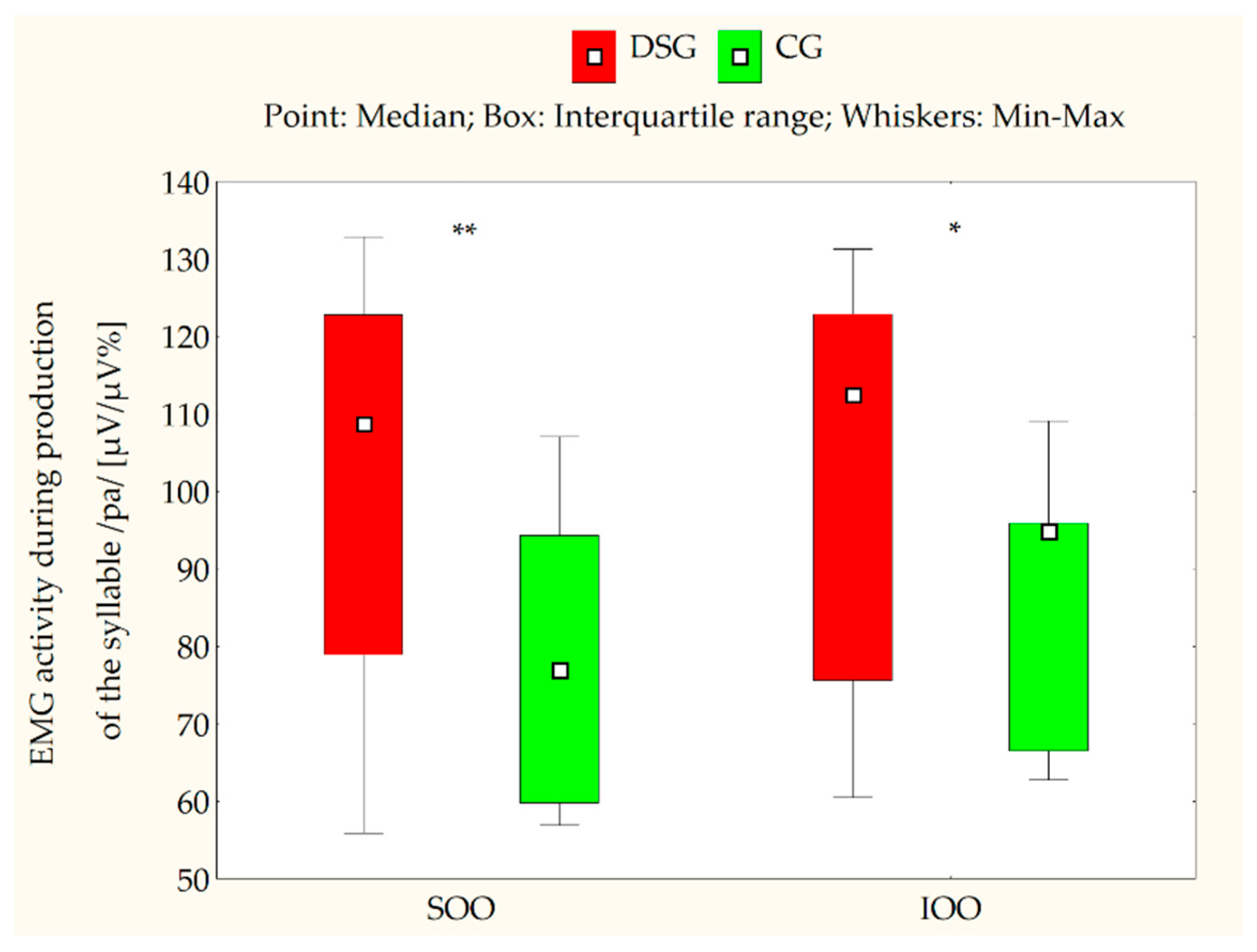
| Production of the syllable/pa/ | 15 | 56.9 | 78.9 | 108.7 | 122.8 | 132.8 | 15 | 55.9 | 59.8 | 76.9 | 94.3 | 107.1 |
| Activity | DS Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Min | Q1 | Mdn | Q3 | Max | n | Min | Q1 | Mdn | Q3 | Max | |
| Rest | 15 | 8.0 | 12.9 | 16.9 | 24.6 | 30.1 | 15 | 6.7 | 11.9 | 13.9 | 16.9 | 28.9 |
| Lip compression | 15 | 88.7 | 95.8 | 108.9 | 135.8 | 165.3 | 15 | 55.4 | 65.8 | 74.9 | 95.4 | 120.7 |
| Saliva swallowing | 15 | 78.4 | 99.1 | 141.2 | 162.8 | 176.9 | 15 | 42.8 | 55.5 | 75.5 | 99.4 | 109.8 |
| Production of the syllable/pa/ | 15 | 62.8 | 75.6 | 112.5 | 122.9 | 131.3 | 15 | 60.5 | 66.5 | 94.8 | 95.9 | 109.1 |
| Variable | n | Min | Q1 | Mdn | Q3 | Max | |
|---|---|---|---|---|---|---|---|
| Atypical swallowing | No | 5 | 74.3 | 78.4 | 79.1 | 89.1 | 98.8 |
| Present | 10 | 127.9 | 135.7 | 145.0 | 169.7 | 185.0 | |
| Mode of breathing | Nasal | 7 | 74.3 | 79.1 | 98.8 | 135.7 | 161.2 |
| Mouth | 8 | 78.4 | 132.2 | 145.0 | 171.3 | 185.0 | |
| Vertical overlap | ≥0 mm | 10 | 74.3 | 79.1 | 89.1 | 98.8 | 135.7 |
| Reverse (anterior open bite) | 5 | 78.4 | 128.4 | 145.0 | 169.7 | 185.0 | |
| Overjet | ≥0 mm | 10 | 98.8 | 98.8 | 99.1 | 100.1 | 100.1 |
| Negative (anterior crossbite) | 5 | 145.3 | 161.2 | 162.8 | 164.8 | 176.9 | |
| Posterior crossbite | No | 5 | 74.3 | 79.1 | 89.1 | 135.7 | 141.2 |
| Present | 10 | 78.4 | 127.9 | 142.3 | 169.7 | 185.0 | |
| Lateral open bite | No | 11 | 74.3 | 79.1 | 128.4 | 141.2 | 172.8 |
| Present | 4 | 127.9 | 138.3 | 159.2 | 177.4 | 185.0 | |
| Variable | n | Min | Q1 | Mdn | Q3 | Max | |
|---|---|---|---|---|---|---|---|
| Atypical swallowing | No | 5 | 78.4 | 89.1 | 98.8 | 99.1 | 100.1 |
| Present | 10 | 132.8 | 141.2 | 153.3 | 164.8 | 176.9 | |
| Mode of breathing | Nasal | 7 | 78.4 | 89.1 | 99.1 | 161.2 | 164.8 |
| Mouth | 8 | 100.1 | 135.4 | 143.3 | 167.8 | 176.9 | |
| Vertical overlap | ≥0 mm | 10 | 78.4 | 89.1 | 98.8 | 99.1 | 164.8 |
| Reverse (anterior open bite) | 5 | 100.1 | 137.9 | 144.5 | 162.8 | 176.9 | |
| Overjet | ≥0 mm | 10 | 74.3 | 74.3 | 79.1 | 98.8 | 98.8 |
| Negative (anterior crossbite) | 5 | 135.7 | 135.9 | 148.7 | 161.2 | 185.0 | |
| Posterior crossbite | No | 5 | 78.4 | 89.1 | 99.1 | 135.7 | 164.8 |
| Present | 10 | 98.8 | 132.8 | 144.5 | 162.8 | 176.9 | |
| Lateral open bite | No | 11 | 78.4 | 98.8 | 132.8 | 161.1 | 172.8 |
| Present | 4 | 137.9 | 140.8 | 144.5 | 162.8 | 176.9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szyszka-Sommerfeld, L.; Sycińska-Dziarnowska, M.; Woźniak, K.; Machoy, M.; Wilczyński, S.; Turkina, A.; Spagnuolo, G. The Electrical Activity of the Orbicularis Oris Muscle in Children with Down Syndrome—A Preliminary Study. J. Clin. Med. 2021, 10, 5611. https://doi.org/10.3390/jcm10235611
Szyszka-Sommerfeld L, Sycińska-Dziarnowska M, Woźniak K, Machoy M, Wilczyński S, Turkina A, Spagnuolo G. The Electrical Activity of the Orbicularis Oris Muscle in Children with Down Syndrome—A Preliminary Study. Journal of Clinical Medicine. 2021; 10(23):5611. https://doi.org/10.3390/jcm10235611
Chicago/Turabian StyleSzyszka-Sommerfeld, Liliana, Magdalena Sycińska-Dziarnowska, Krzysztof Woźniak, Monika Machoy, Sławomir Wilczyński, Anna Turkina, and Gianrico Spagnuolo. 2021. "The Electrical Activity of the Orbicularis Oris Muscle in Children with Down Syndrome—A Preliminary Study" Journal of Clinical Medicine 10, no. 23: 5611. https://doi.org/10.3390/jcm10235611
APA StyleSzyszka-Sommerfeld, L., Sycińska-Dziarnowska, M., Woźniak, K., Machoy, M., Wilczyński, S., Turkina, A., & Spagnuolo, G. (2021). The Electrical Activity of the Orbicularis Oris Muscle in Children with Down Syndrome—A Preliminary Study. Journal of Clinical Medicine, 10(23), 5611. https://doi.org/10.3390/jcm10235611