
Pulmonary Vein Isolation Outcome Degree Is a New Score for Efficacy of Atrial Fibrillation Catheter Ablation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ablation Protocol
2.2. Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Study Population
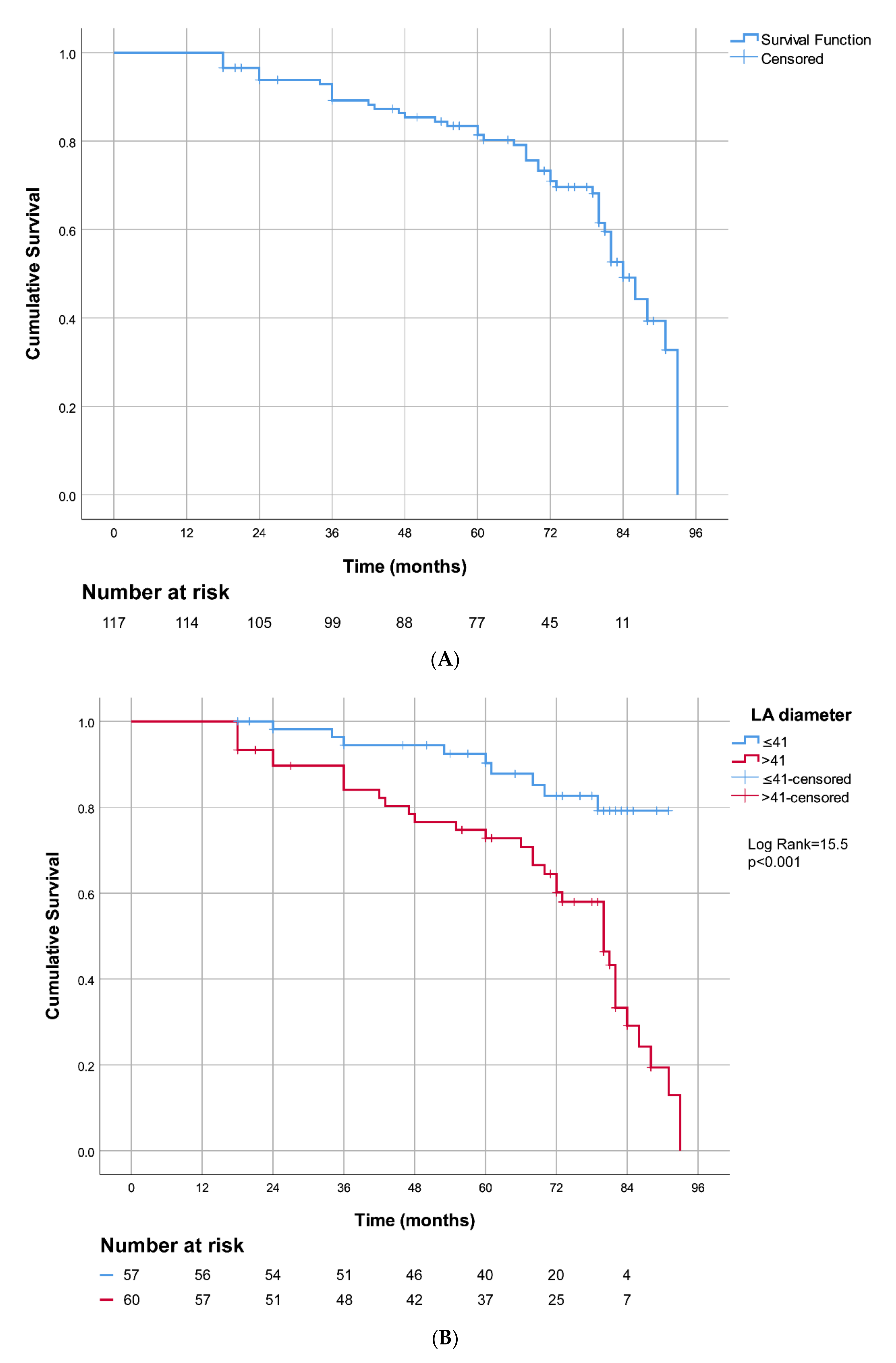
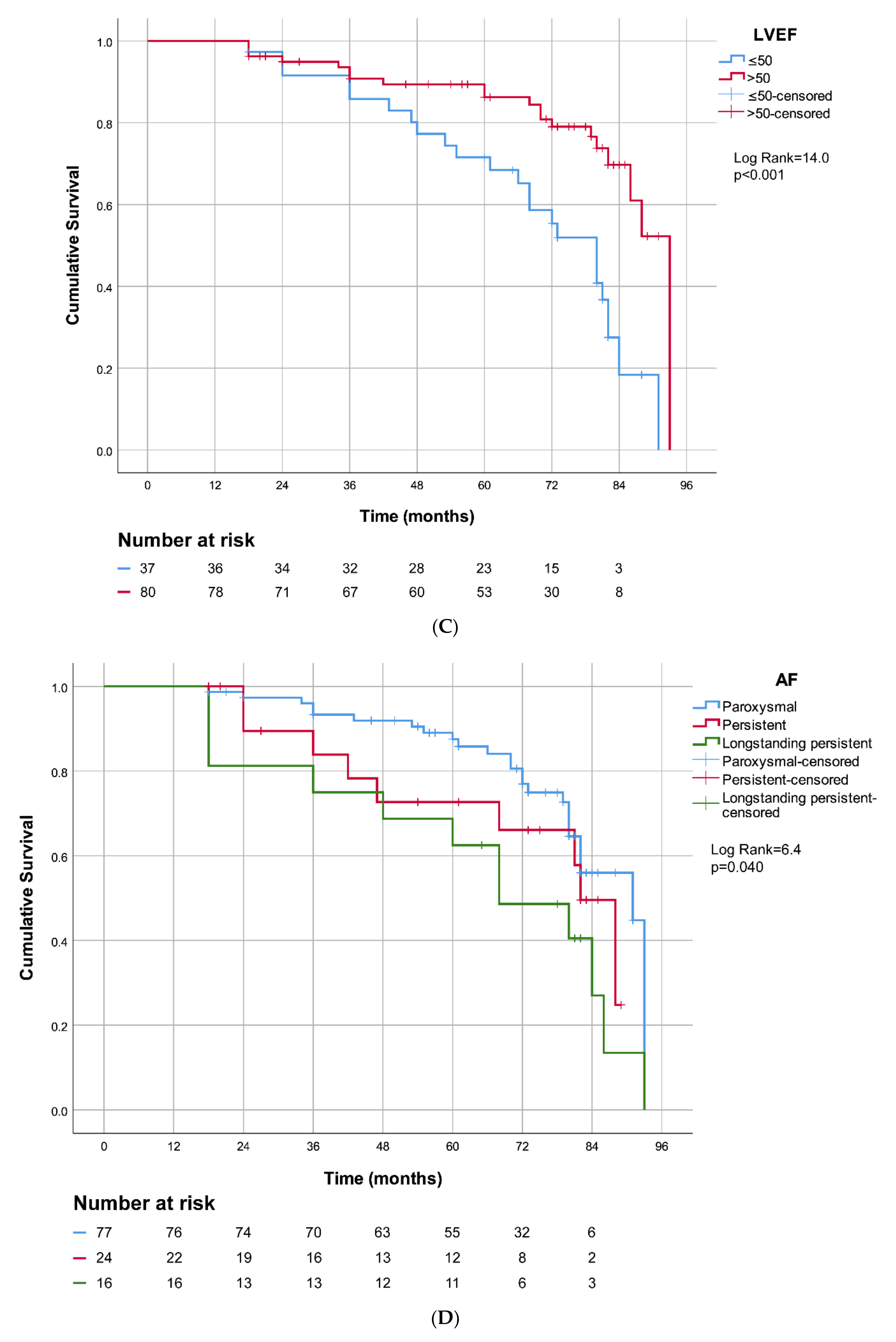
3.2. Catheter Ablation Success after 7-Year Follow-Up
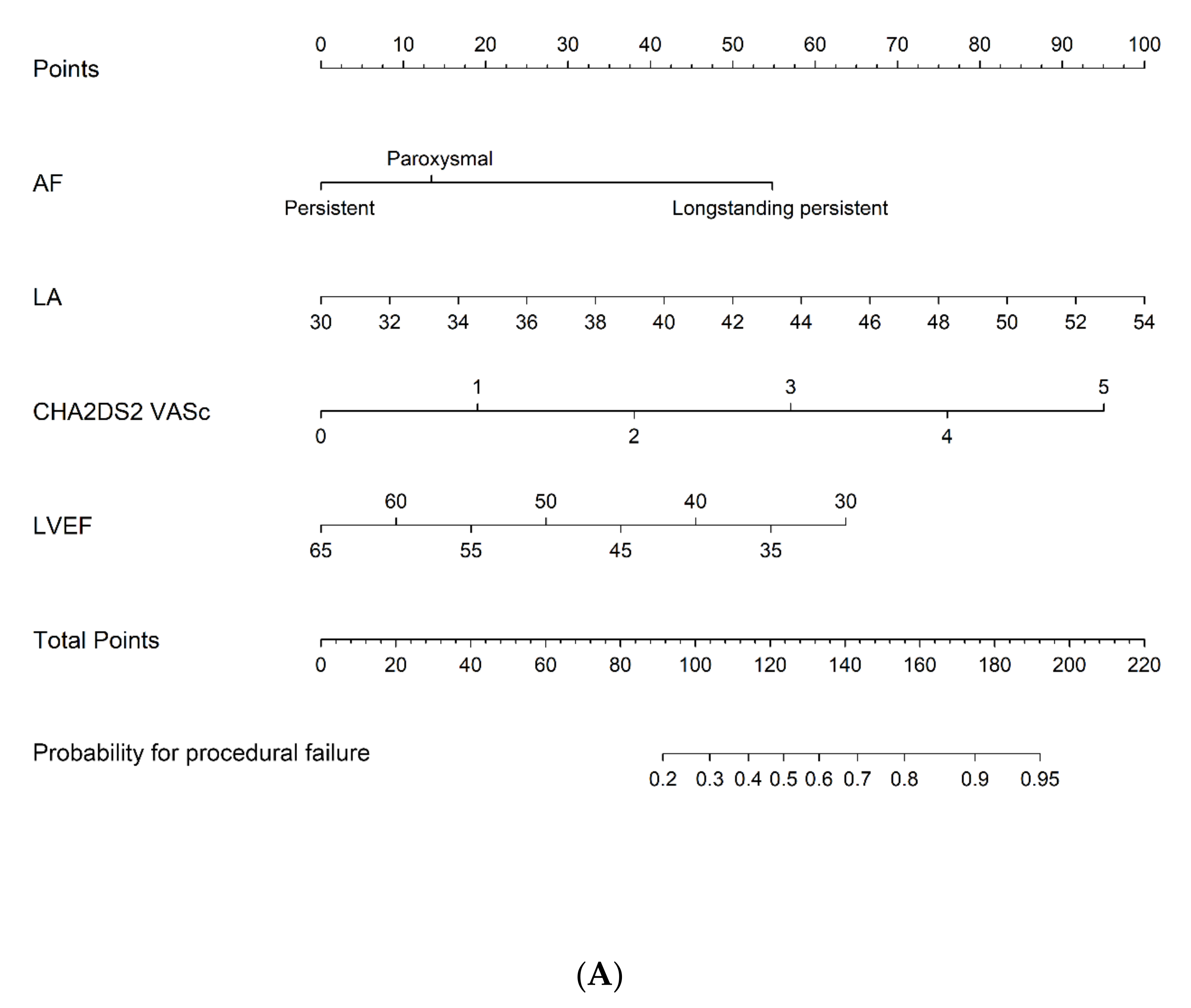
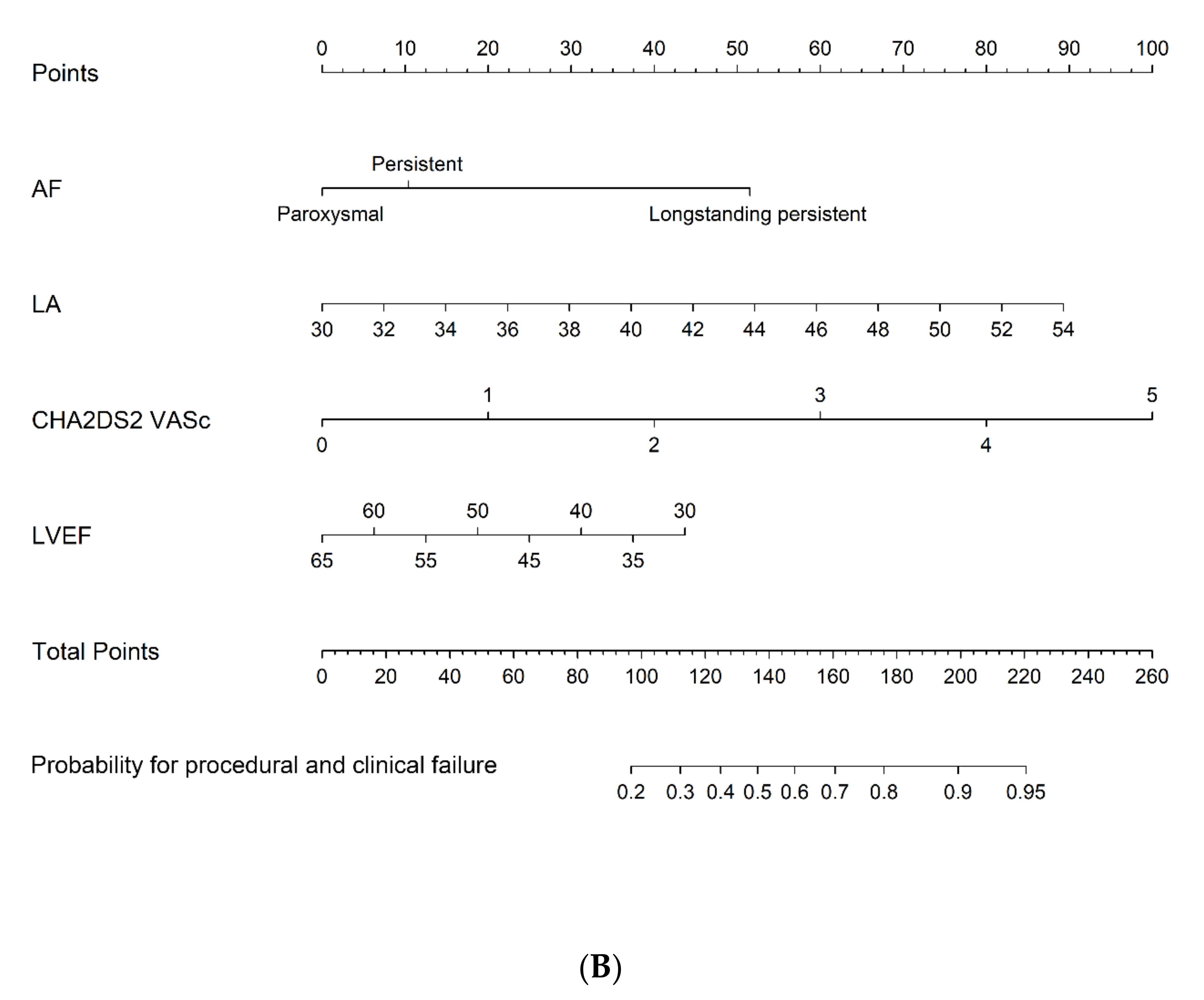
3.3. Predictors for Unsuccessful Catheter Ablation of Pulmonary Vein
3.4. Catheter Ablation Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teunissen, C.; Kassenberg, W.; van der Heijden, J.F.; Hassink, R.J.; van Driel, V.J.; Zuithoff, N.P.; Doevendans, P.A.; Loh, P. Five-year efficacy of pulmonary venous antrum isolation as a primary ablation strategy for atrial fibrillation: A single-centre cohort study. Europace 2016, 18, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Haissaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, F.; Tilz, R.; Chun, J.; Schmidt, B.; Wissner, E.; Zerm, T.; Neven, K.; Köktürk, B.; Konstantinidou, M.; Metzner, A.; et al. Long-Term Results of Catheter Ablation in Paroxysmal Atrial Fibrillation: Lessons from a 5-year follow-up. Circulation 2010, 122, 2368–2377. [Google Scholar] [CrossRef]
- Gaita, F.; Caponi, D.; Scaglione, M.; Montefusco, A.; Corleto, A.; Di Monte, F.; Coin, D.; Di Donna, P.; Giustetto, C. Long-term clinical results of 2 different ablation strategies in patients with paroxysmal and persistent atrial fibrillation. Circ. Arrhythmia Electrophysiol. 2008, 1, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Kagawa, Y.; Fujii, E.; Fujita, S.; Ito, M. Association between left atrial reverse remodeling and maintenance of sinus rhythm after catheter ablation of persistent atrial fibrillation. Heart Vessel. 2020, 35, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Fiala, M.; Chovančík, J.; Nevřalová, R.; Neuwirth, R.; Jiravský, O.; Nykl, I.; Škňouřil, L.; Dorda, M.; Januška, J.; Branny, M. Pulmonary vein isolation using segmental versus electroanatomical circumferential ablation for paroxysmal atrial fibrillation: Over 3-year results of a prospective randomized study. J. Interv. Card. Electrophysiol. 2008, 22, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Kornej, J.; Hindricks, G.; Kosiuk, J.; Arya, A.; Sommer, P.; Husser, D.; Rolf, S.; Richter, S.; Huo, Y.; Piorkowski, C.; et al. Comparison of CHADS2, R2CHADS2 and CHA2DS2-VASc Scores for the Prediction of Rhythm Outcomes After Catheter Ablation of Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2014, 7, 281–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garvanski, I.; Simova, I.; Angelkov, L.; Matveev, M. Predictors of recurrence of AF in patients after radiofrequency ablation. Eur. Cardiol. Rev. 2019, 14, 165–168. [Google Scholar] [CrossRef] [Green Version]
- Kornej, J.; Schumacher, K.; Dinov, B.; Kosich, F.; Sommer, P.; Arya, A.; Husser, D.; Bollmann, A.; Lip, G.Y.; Hindricks, G. Prediction of electro-anatomical substrate and arrhythmia recurrences using APPLE, DR-FLASH and MB-LATER scores in patients with atrial fibrillation undergoing catheter ablation. Nature 2018, 8, 12686. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Kuck, K.H.; Cappato, R.; Brugada, J.; Camm, A.J.; Chen, S.A.; Crijns, H.J.; Damiano, R.J., Jr.; Davies, D.W.; DiMarco, J.; et al. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Patient Selection, Procedural Techniques, Patient Management and Follow-up, Definitions, Endpoints, and Research Trial Design. Europace 2012, 14, 528–606. [Google Scholar] [CrossRef]
- Williams, S.E.; O’Neill, L.; Roney, C.H.; Julia, J.; Metzner, A.; Reißmann, B.; Mukherjee, R.K.; Sim, I.; Whitaker, J.; Wright, M.; et al. Left atrial effective conducting size predicts atrial fibrillation vulnerability in persistent but not paroxysmal atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 1416–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindrinks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, E.P.; Fauchier, L.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Miyazaki, S.; Kajiyama, T.; Watanabe, T.; Nakamura, H.; Hachiya, H.; Tada, H.; Iesaka, Y. Can the Durability of Pulmonary Vein Isolation Be Predicted by the Time-to-Isolation in Second–Generation Cryoballoon Ablation? Circ. Arrhythmia Electrophysiol. 2020, 13, e008076. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Corleto, A.; Biondi-Zoccai, G.; Anselmino, M.; Ferraris, F.; Di Biase, L.; Natale, A.; Hunter, R.J.; Schilling, R.J.; Miyazaki, S.; et al. Which are the most reliable predictors of recurrence of atrial fibrillation after transcatheter ablation? A meta-analysis. Int. J. Cardiol. 2013, 167, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, S.M.; Larson, M.G.; Benjamin, E.J.; Levy, D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart study. Circulation 1994, 89, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, J.; Wang, Y.; Tang, K.; Li, X.; Peng, W.; Liang, C.; Xu, Y. Association between left atrial size and atrial fibrillation recurrence after single circumferential pulmonary vein isolation: A systemic review and meta-analysis of observational studies. Europace 2012, 14, 638–645. [Google Scholar] [CrossRef]
- Beukema, W.P.; Elvan, A.; Sie, H.T.; Misier, A.R.R.; Wellens, H.J.J. Successful radiofrequency ablation in patients with previous atrial fibrillation results in a significant decrease in left atrial size. Circulation 2005, 112, 2089–2095. [Google Scholar] [CrossRef] [Green Version]
- Kohari, M.; Zado, E.; Marchlinski, E.F.; Callans, J.D.; Han, Y. Left atrial volume best predicts recurrence after catheter ablation in patients with persistent and longstanding persistent atrial fibrillation. Pacing Clin. Electrophysiol. 2014, 37, 422–429. [Google Scholar] [CrossRef]
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left attrial volume predicts atrial fibrillation recurrence after radiofrequency ablation:a meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Hauser, T.; Essebag, V.; Baldessin, F.; McClennen, S.; Yeon, B.S.; Manning, J.W.; Josephson, E.M. Prognostic value of pulmonary vein size in prediction of atrial fibrillation recurrence after pulmonary vein isolation: A cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2015, 17, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letsas, K.P.; Efremidis, M.; Giannopoulos, G.; Deftereos, S.; Lioni, L.; Korantzopoulos, P.; Vlachos, K.; Xydonas, S.; Kossyvakis, C.; Sideris, A. CHADS2 and CHA2DS2-VASc scores as predictors of left atrial ablation outcomes for paroxysmal atrial fibrillation. Europace 2014, 16, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Jiang, S.L.; Lui, X.; Yang, Y.Q. Repeat Catheter Ablation of Long-standing Persistent Atrial Fibrillation in Patients with a Total Atrial Fibrillation Duration of More Than 2 Years: Effect of the CHA2DS2-VASc Score and Estimated Glomerular Filtration Rate on the Outcomes. Intern. Med. 2016, 55, 2537–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodani, E.; Akao, M. Atrial fibrillation and stroke prevention: State of the art-epidemiology and pathophysiology: New risk factors, concepts and controversies. Eur. Heart. J. 2020, 22, 1–13. [Google Scholar] [CrossRef]
- Kloosterman, M.; Chua, W.; Fabritz, L.; Al-Khalidi, H.R.; Schotten, U.; Nielsen, J.C.; Piccini, J.P.; Di Biase, L.; Häusler, K.G.; Todd, D.; et al. Sex differences in catheter ablation of atrial fibrillation: Results from AXAFA-AFNET 5. Europece 2020, 22, 1026–1035. [Google Scholar] [CrossRef]
- Berkowitsch, A.; Greiss, H.; Vukajlovic, D.; Kuniss, M.; Neumann, T.; Zaltsberg, S.; Kurzidim, K.; Hamm, C.; Pitschner, H.F. Usefulness of atrial fibrillation burden as a predictor for success of pulmonary vein isolation. Pacing Clin. Electrophysiol. 2005, 28, 1292–1301. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Purerfellner, H.; Meyer, C.; Acou, W.; Schatter, A.; Ling, Z.; Liu, S.; Yin, Y.; Martineu, M.; Kiuchi, G.M. Rhythm control for patients with atrial fibrillation complicated with heart failure in the contemporary era of catheter ablation: A stratified pooled analysis of randomized data. Eur. Heart J. 2019, 41, 2863–2873. [Google Scholar] [CrossRef]
- Wyse, D.G.; Van Gelder, I.C.; Ellinor, P.T.; Go, A.S.; Kalman, J.M.; Narayan, S.M.; Nattel, S.; Schotten, U.; Rienstra, M. Lone Atrial Fibrillation: Does it Exist? A “White Paper” of the Journal of the American College of Cardiology. J. Am. Coll. Cardiol. 2014, 63, 1715–1723. [Google Scholar] [CrossRef] [Green Version]
- Chun, K.J.; Perrotta, L.; Bordignon, S.; Khalil, J.; Dugo, D.; Konstantinou, A.; Fürnkranz, A.; Schmidt, B. Complications in Catheter Ablation of Atrial Fibrillation in 3000 Consecutive Procedures. Ballon versus Radiofrequency Current Ablation. J. Am. Coll. Cardiol. 2017, 3, 154–161. [Google Scholar]
- Magnani, W.J.; Benjamin, J.E. “Where Do We Come from? Where Are We Going” Adverse Outcomes in Catheter Ablation for Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2014, 7, 195–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All | PVIOD 1 | PVIOD 2 | PVIOD 3 | PVIOD 4 | p-Value |
|---|---|---|---|---|---|---|
| n = 117 | n = 38 | n = 34 | n = 17 | n = 28 | ||
| Age (years) | 56.2 ± 8.5 | 56.0 ± 7.8 | 54.3 ± 9.4 | 59.8 ± 8.3 | 56.8 ± 8.3 | 0.189 |
| Sex (male) | 93 (79.5%) | 30 (78.9%) | 30 (88.2%) | 14 (82.4%) | 19 (67.9%) | 0.26 |
| Duration of AF (years) | 5 (1–18) | 5 (1–16) | 4 (1–16) | 8 (1–18) | 5.5 (2–15) | 0.125 |
| Paroxysmal AF | 77 (65.8%) | 31 (81.6%) | 22 (64.7%) | 12 (70.6%) | 12 (42.9%) | |
| Persistent AF | 24 (20.5%) | 5 (13.2%) | 10 (29.4%) | 2 (11.8%) | 7 (25%) | 0.009 |
| Longstanding persistent AF | 16 (13.7%) | 2 (5.3%) | 2 (5.9%) | 3 (17.6%) | 9 (32.1%) | |
| BMI (kg/m2) * | 27.7 ± 4.0 | 26.9 ± 4.3 | 27.8 ± 4.1 | 27.5 ± 3.4 | 28.6 ± 3.8 | 0.553 |
| CHA2DS2-VASc score | 1 (0-5) | 1 (0-3) | 0 (0–3) | 1 (0–5) | 2 (0–4) | <0.001 |
| Hypertension | 75 (64.1%) | 24 (63.2%) | 16 (47.1%) | 12 (70.6%) | 23 (82.1%) | 0.035 |
| Diabetes mellitus | 9 (7.7%) | 2 (5.3%) | 1 (2.9%) | 1 (5.9%) | 5 (17.9%) | 0.183 |
| Hypercholesterolemia | 53 (45.3%) | 18 (47.4%) | 12 (35.3%) | 11 (64.7%) | 12 (42.9%) | 0.252 |
| Structural heart disease | 21 (17.9%) | 5 (13.2%) | 3 (8.8%) | 3 (17.6%) | 10 (35.7%) | 0.046 |
| Left atrial diameter (mm) | 41.9 ± 4.7 | 39.3 ± 3.8 | 41.9 ± 4.6 | 43.1 ± 5.1 | 44.7 ± 3.9 | <0.001 |
| LVEF | 54.8 ± 6.9 | 56.8 ± 4.7 | 57.1 ± 5.7 | 52.7 ± 6.2 | 50.7 ± 6.2 | <0.001 |
| Propafenone | 33 (28.2%) | 15 (39.5%) | 8 (23.5%) | 4 (23.5%) | 6 (21.4%) | 0.312 |
| Betablocker | 70 (59.8%) | 23 (60.5%) | 19 (55.9%) | 9 (52.9%) | 19 (67.9%) | 0.726 |
| Antiarrhythmic group III | 68 (58.1%) | 17 (44.7%) | 22 (64.7%) | 12 (70.6%) | 17 (60.7%) | 0.207 |
| Verapamil | 5 (4.3%) | 3 (7.9%) | 0 (0.0%) | 0 (0.0%) | 2 (7.1%) | 0.276 |
| Paroxysmal AF n = 77 | Persistent AF n = 24 | Longstanding p. AF n = 16 | All n = 117 | |
|---|---|---|---|---|
| PVIOD 1 | 40.2 | 20.8 | 12.5 | 32.5 |
| PVIOD 2 | 28.6 (68.8) | 41.7 (62.5) | 12.5 (25) | 29.1 (61.6) |
| PVIOD 3 | 15.6 (84.4) | 8.3 (70.8) | 18.7 (43.7) | 14.5 (76.1) |
| PVIOD 4 | 15.6 (100) | 29.2 (100) | 56.3 (100) | 23.9 (100) |
| Predictor | UV | MV | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (years) | 1 | 1.0–1.1 | 0.43 | |||
| Sex (male) | 1.5 | 0.7–3.5 | 0.289 | |||
| Duration of AF (years) | 1.1 | 1.0–1.2 | 0.127 | |||
| Paroxysmal AF | Referent | Referent | ||||
| Persistent AF | 1.9 | 0.8–4.4 | 0.124 | 1.1 | 0.4–2.8 | 0.9 |
| Longstanding persistent AF | 6.5 | 2.3–18.6 | 0.001 | 3.5 | 1.1–10.7 | 0.031 |
| BMI (kg/m2) * | 1.1 | 1.0–1.2 | 0.173 | |||
| CHA2DS2-VASc score | 1.5 | 1.1–2.1 | 0.008 | 1.4 | 0.95–2.0 | 0.086 |
| Hypertension | 1.8 | 0.3–3.5 | 0.105 | |||
| Diabetes mellitus | 3.6 | 1.0–13 | 0.049 | 2.7 | 0.6–12.1 | 0.205 |
| Hypercholesterolemia | 1 | 0.5–2.0 | 0.895 | |||
| Structural heart disease | 3 | 1.2–7.2 | 0.014 | 0.4 | 0.1–1.6 | 0.21 |
| Left atrial diameter (mm) | 1.2 | 1.1–1.3 | <0.001 | 1.2 | 1.1–1.3 | 0.001 |
| LVEF | 0.9 | 0.85–0.95 | <0.001 | 0.9 | 0.86–1.0 | 0.038 |
| Propafenone | 0.5 | 0.2–1.1 | 0.086 | |||
| Betablocker | 1.1 | 0.6–2.2 | 0.695 | |||
| Antiarrhythmic group III | 1.7 | 0.9–3.4 | 0.109 | |||
| Verapamil | 0.6 | 0.1–3.1 | 0.545 |
| Complications | Number (%) n = 18 (8.6%) |
|---|---|
| Major: | 7 (3.3%) |
| Cardiac tamponade | 2 |
| Rupture of mitral valve chordae | 1 |
| Pneumothorax | 1 |
| Stroke | 1 |
| Retroperitoneal hematoma | 1 |
| Jugular vein subcutaneous hematoma | 1 |
| Minor: | 11 (5.3%) |
| Pericardial effusion | 5 |
| Inguinal subcutaneous hematoma | 5 |
| Superficial thrombophlebitis | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurcevic, R.; Angelkov, L.; Tasic, N.; Tomovic, M.; Kojic, D.; Otasevic, P.; Bojic, M. Pulmonary Vein Isolation Outcome Degree Is a New Score for Efficacy of Atrial Fibrillation Catheter Ablation. J. Clin. Med. 2021, 10, 5827. https://doi.org/10.3390/jcm10245827
Jurcevic R, Angelkov L, Tasic N, Tomovic M, Kojic D, Otasevic P, Bojic M. Pulmonary Vein Isolation Outcome Degree Is a New Score for Efficacy of Atrial Fibrillation Catheter Ablation. Journal of Clinical Medicine. 2021; 10(24):5827. https://doi.org/10.3390/jcm10245827
Chicago/Turabian StyleJurcevic, Ruzica, Lazar Angelkov, Nebojsa Tasic, Milosav Tomovic, Dejan Kojic, Petar Otasevic, and Milovan Bojic. 2021. "Pulmonary Vein Isolation Outcome Degree Is a New Score for Efficacy of Atrial Fibrillation Catheter Ablation" Journal of Clinical Medicine 10, no. 24: 5827. https://doi.org/10.3390/jcm10245827
APA StyleJurcevic, R., Angelkov, L., Tasic, N., Tomovic, M., Kojic, D., Otasevic, P., & Bojic, M. (2021). Pulmonary Vein Isolation Outcome Degree Is a New Score for Efficacy of Atrial Fibrillation Catheter Ablation. Journal of Clinical Medicine, 10(24), 5827. https://doi.org/10.3390/jcm10245827