
Epidemiology of Antepartum Stillbirths in Austria—A Population-Based Study between 2008 and 2020


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analyses
2.3. Ethical Approval and Consent
3. Results
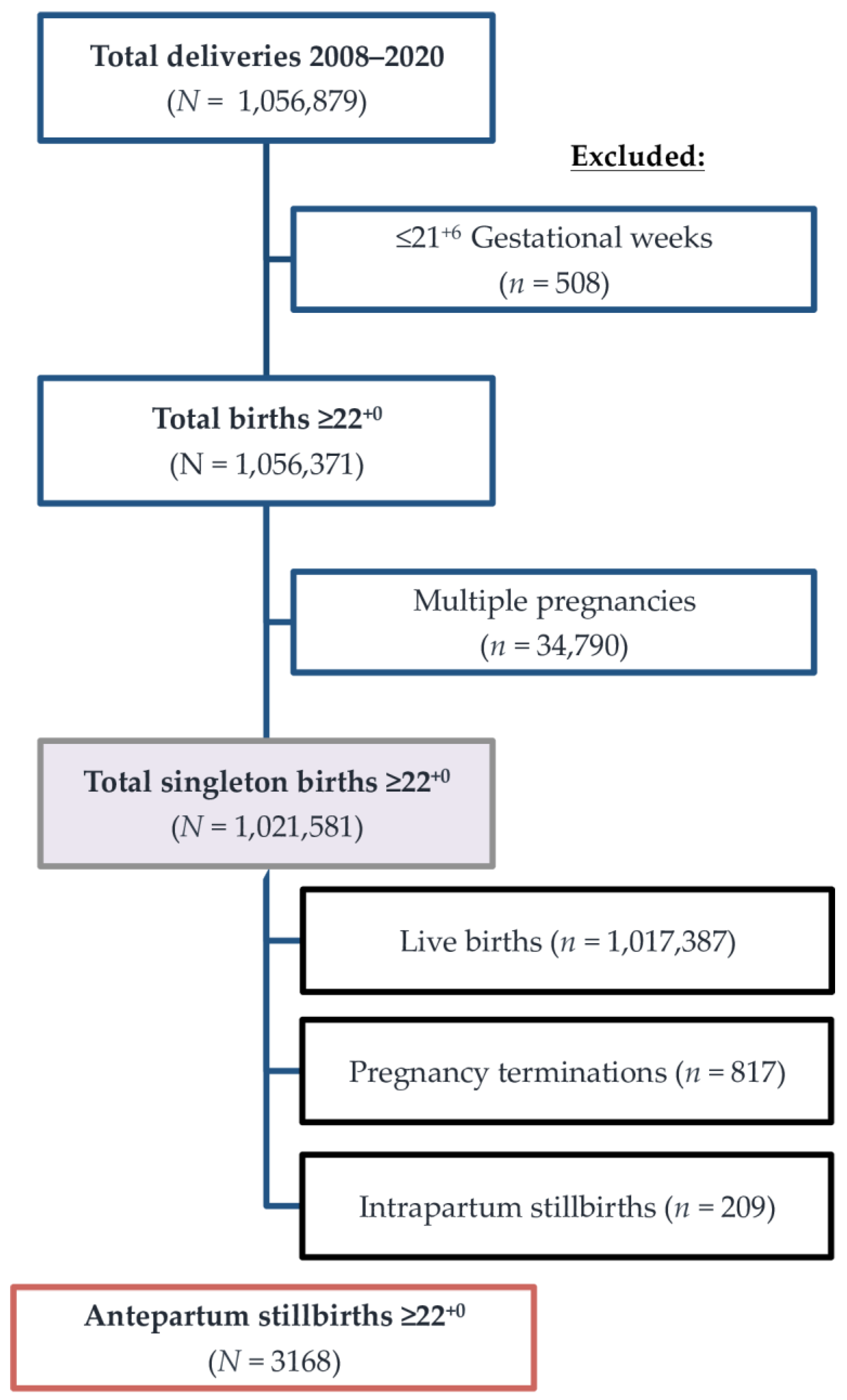
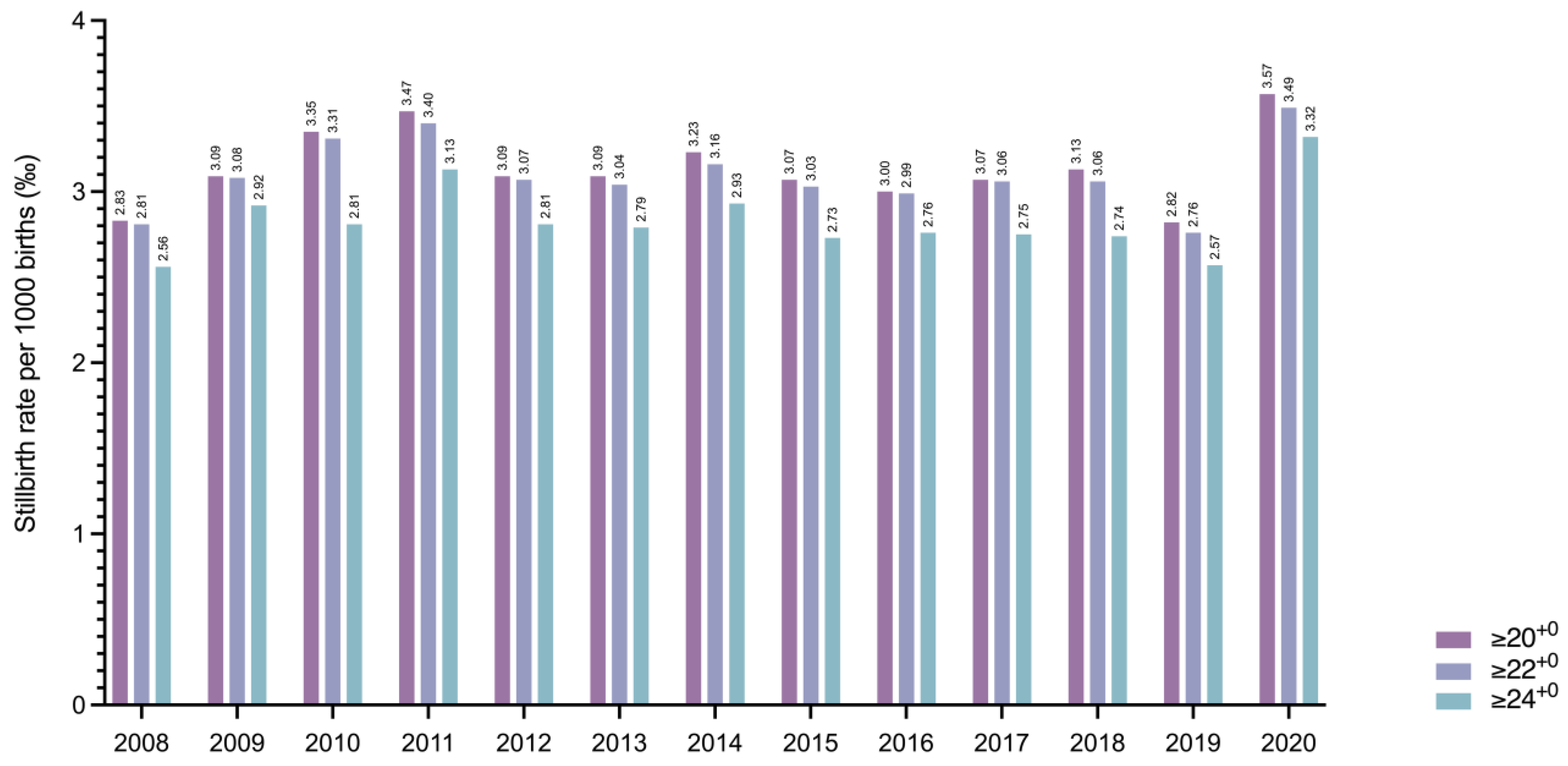
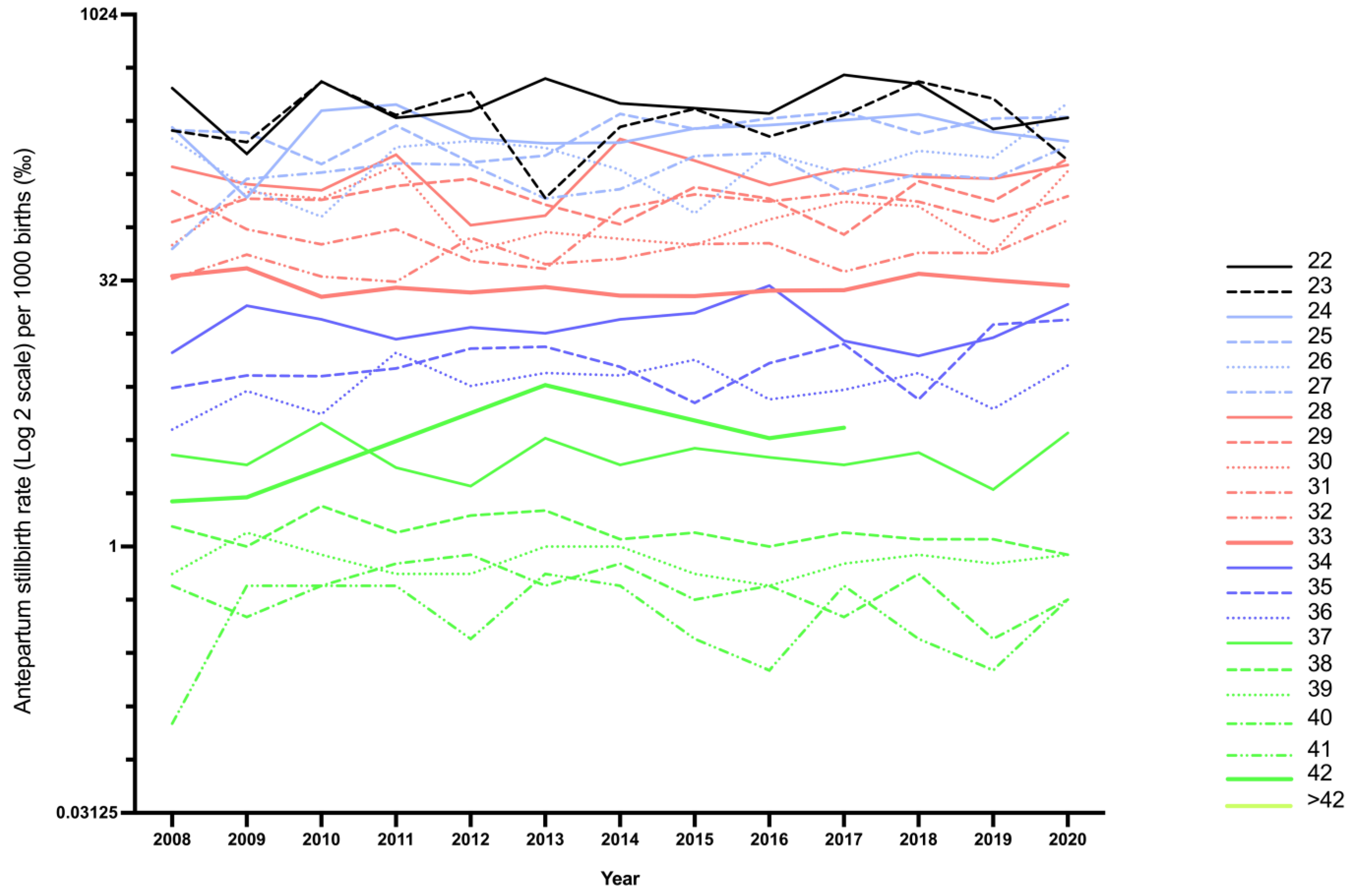
3.1. Incidence of Antepartum Stillbirths in Austria
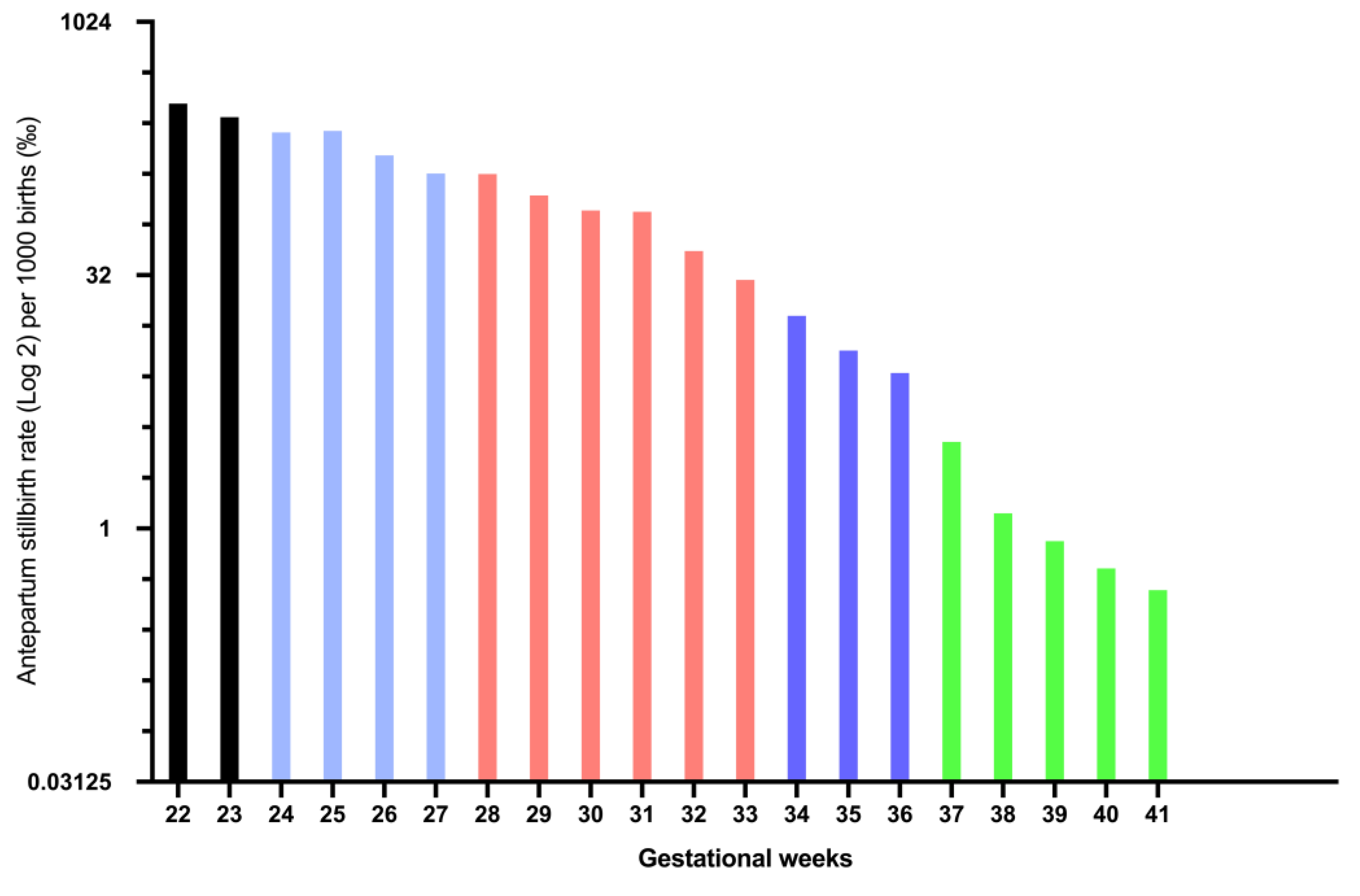
3.2. Timing of Antepartum Stillbirths
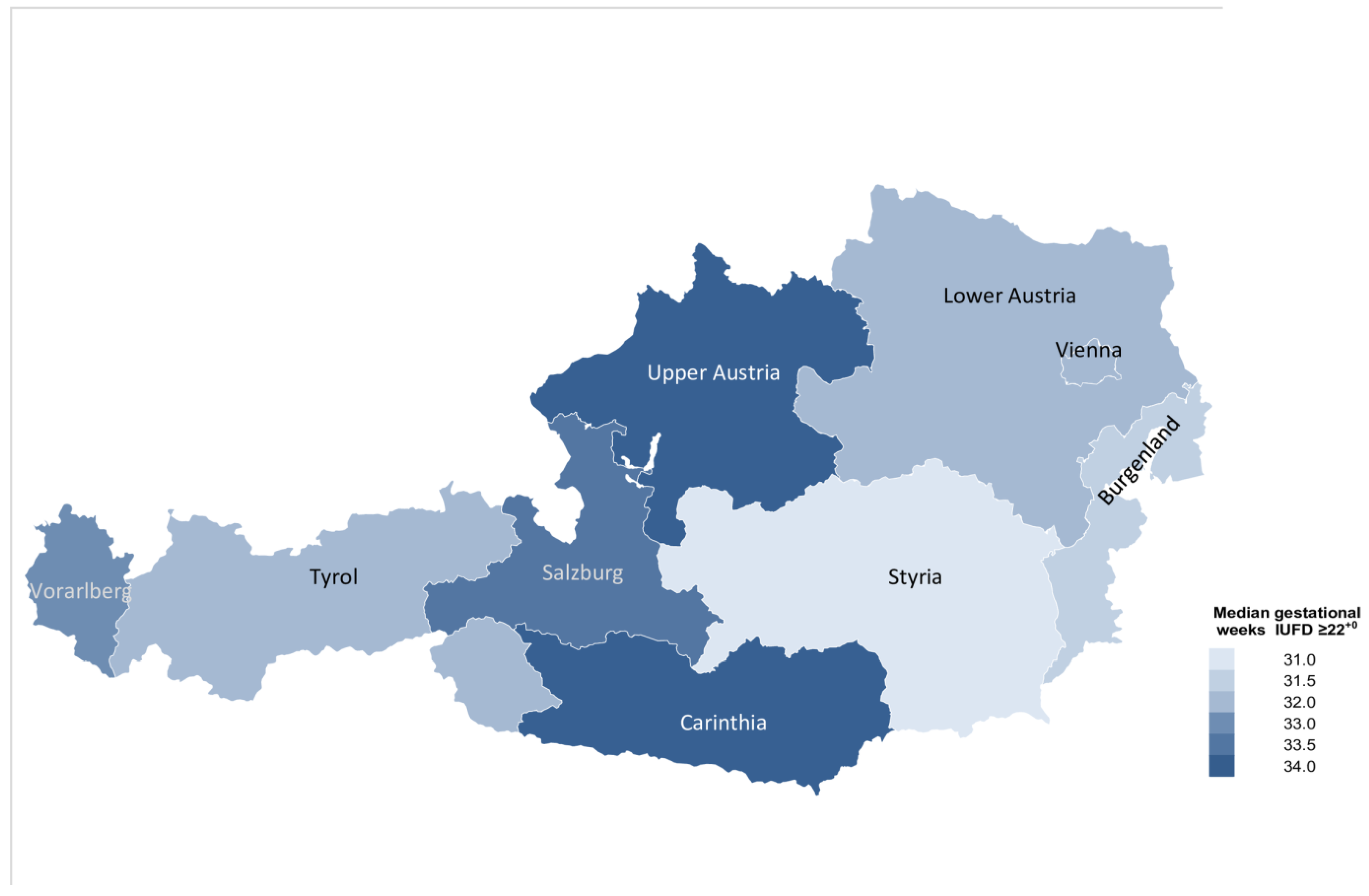
3.3. Risk Factors for Suffering Antepartum Stillbirth in Austria
4. Discussion
4.1. Main Findings and Interpretation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hug, L.; You, D.; Blencowe, H.; Mishra, A.; Wang, Z.; Fix, M.J.; Wakefield, J.; Moran, A.C.; Gaigbe-Togbe, V.; Suzuki, E.; et al. Global, regional, and national estimates and trends in stillbirths from 2000 to 2019: A systematic assessment. Lancet 2021, 398, 772–785. [Google Scholar] [CrossRef]
- Smith, L.K.; Blondel, B.; Zeitlin, J. Producing valid statistics when legislation, culture and medical practices differ for births at or before the threshold of survival: Report of a European workshop. BJOG 2020, 127, 314–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohangoo, A.D.; Buitendijk, S.E.; Szamotulska, K.; Chalmers, J.; Irgens, L.M.; Bolumar, F.; Nijhuis, J.G.; Zeitlin, J.; Euro-Peristat Scientific Committee. Gestational age patterns of fetal and neonatal mortality in Europe: Results from the Euro-Peristat project. PLoS ONE 2011, 6, e24727. [Google Scholar] [CrossRef] [Green Version]
- Blondel, B.; Cuttini, M.; Hindori-Mohangoo, A.D.; Gissler, M.; Loghi, M.; Prunet, C.; Heino, A.; Smith, L.; van der Pal-de Bruin, K.; Macfarlane, A.; et al. How do late terminations of pregnancy affect comparisons of stillbirth rates in Europe? Analyses of aggregated routine data from the Euro-Peristat Project. BJOG 2018, 125, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Spong, C.Y.; Reddy, U.M.; Willinger, M. Addressing the complexity of disparities in stillbirths. Lancet 2011, 377, 1635–1636. [Google Scholar] [CrossRef]
- Klebermass-Schrehof, K.; Wald, M.; Schwindt, J.; Grill, A.; Prusa, A.R.; Haiden, N.; Hayde, M.; Waldhoer, T.; Fuiko, R.; Berger, A. Less invasive surfactant administration in extremely preterm infants: Impact on mortality and morbidity. Neonatology 2013, 103, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Gulland, A. Fall in rate of stillbirth drives down perinatal mortality. BMJ 2017, 357, j3050. [Google Scholar] [CrossRef] [PubMed]
- Muin, D.A.; Neururer, S.; Falcone, V.; Windsperger, K.; Helmer, H.; Leitner, H.; Kiss, H.; Farr, A. Antepartum stillbirth rates during the COVID-19 pandemic in Austria: A population-based study. Int. J. Gynaecol. Obstet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ashish, K.C.; Gurung, R.; Kinney, M.V.; Sunny, A.K.; Moinuddin, M.; Basnet, O.; Paudel, P.; Bhattarai, P.; Subedi, K.; Shrestha, M.P.; et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Glob. Health 2020, 8, e1273–e1281. [Google Scholar]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef]
- De Curtis, M.; Villani, L.; Polo, A. Increase of stillbirth and decrease of late preterm infants during the COVID-19 pandemic lockdown. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 106, 456. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; Khalil, A.; von Dadelszen, P. Covid-19: UK Obstetric Surveillance System (UKOSS) study in context. BMJ 2020, 370, m2915. [Google Scholar] [CrossRef]
- Khalil, A.; von Dadelszen, P.; Ugwumadu, A.; Draycott, T.; Magee, L.A. Effect of COVID-19 on maternal and neonatal services. Lancet Glob. Health 2021, 9, e112. [Google Scholar] [CrossRef]
- Khalil, A.; von Dadelszen, P.; Draycott, T.; Ugwumadu, A.; O’Brien, P.; Magee, L. Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. JAMA 2020, 324, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Hedermann, G.; Hedley, P.L.; Bækvad-Hansen, M.; Hjalgrim, H.; Rostgaard, K.; Poorisrisak, P.; Breindahl, M.; Melbye, M.; Hougaard, D.M.; Christiansen, M.; et al. Danish premature birth rates during the COVID-19 lockdown. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 93–95. [Google Scholar] [CrossRef]
- Philip, R.K.; Purtill, H.; Reidy, E.; Daly, M.; Imcha, M.; McGrath, D.; O’Connell, N.H.; Dunne, C.P. Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID-19 lockdown in Ireland: A ‘natural experiment’ allowing analysis of data from the prior two decades. BMJ Glob. Health 2020, 5, e003075. [Google Scholar] [CrossRef]
- Windsperger, K.; Kiss, H.; Oberaigner, W.; Leitner, H.; Binder, F.; Muin, D.A.; Foessleitner, P.; Husslein, P.W.; Farr, A. Exposure to night-time light pollution and risk of prolonged duration of labor: A nationwide cohort study. Birth 2021. [CrossRef]
- Jiang, T.B.; Deng, Z.W.; Zhi, Y.P.; Cheng, H.; Gao, Q. The Effect of Urbanization on Population Health: Evidence From China. Front. Public Health 2021, 9, 706982. [Google Scholar] [CrossRef]
- Zhu, J.; Liang, J.; Mu, Y.; Li, X.; Guo, S.; Scherpbier, R.; Wang, Y.; Dai, L.; Liu, Z.; Li, M.; et al. Sociodemographic and obstetric characteristics of stillbirths in China: A census of nearly 4 million health facility births between 2012 and 2014. Lancet Glob. Health 2016, 4, e109–e118. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.K.; Hindori-Mohangoo, A.D.; Delnord, M.; Durox, M.; Szamotulska, K.; Macfarlane, A.; Alexander, S.; Barros, H.; Gissler, M.; Blondel, B.; et al. Quantifying the burden of stillbirths before 28 weeks of completed gestational age in high-income countries: A population-based study of 19 European countries. Lancet 2018, 392, 1639–1646. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antepartum Stillbirth | Total | Non-Specified | Vienna | Styria | Lower Austria | Upper Austria | Tyrol | Salzburg | Carinthia | Vorarlberg | Burgenland | p-Value 4 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total deliveries (n) | 1,021,581 | 32,165 | 231,674 | 130,211 | 163,290 | 175,254 | 88,325 | 66,727 | 57,734 | 48,785 | 27,416 | . | |
| Total antepartum stillbirths (n; ≥22+0) | 3163 | 146 | 884 | 402 | 499 | 489 | 236 | 170 | 145 | 135 | 57 | <0.001 | |
| Antepartum stillbirth rate (‰; ≥22+0) | 3.10 | . | 3.82 | 3.09 | 3.06 | 2.79 | 2.67 | 2.55 | 2.51 | 2.77 | 2.08 | <0.001 | |
| Median gestational age of stillbirth (IQR) | 33+0 (27+2–37+4) | 32+3 (27+6–37+6) | 32+6 (26+5–37+2) | 31+6 (26+1–36+6) | 32+0 (26+5–37+0) | 34+2 (29+1–38+1) | 32+5 (27+6–37+2) | 33+5 (28+5–38+0) | 34+3 (27+3–38+3) | 33+0 (28+0–37+5) | 32+1 (27+5–36+6) | <0.001 | |
| Median maternal age at stillbirth (IQR) | 31 (26–35) | 32 (29–36) | 30 (26–35) | 31 (26–35) | 31 (27–35) | 30 (26–34) | 31 (27–35) | 31 (27–36) | 30 (26–34) | 31 (27–36) | 33 (29–37) | 0.188 | |
| Median BMI (IQR; kg/m 2) | 23.4 (20.7–27.0) | 22.9 (20.7–26.9) | 23.4 (20.7–27.3) | 23.4 (20.4–26.6) | 23.8 (21.4–27.1) | 23.5 (20.8–27.6) | 22.8 (20.7–25.7) | 22.8 (20.2–26.9) | 23.1 (20.9–26.0) | 22.4 (20.3–27.7) | 23.5 (21.8–28.0) | 0.244 | |
| BMI category 1 | Underweight | 122 (6.0%) | 3 (5.3%) | 38 (6.6%) | 16 (6.9%) | 6 (2.1%) | 24 (7.2%) | 17 (7.7%) | 9 (6.9%) | 3 (2.7%) | 4 (6.0%) | 2 (5.9%) | 0.241 |
| Normal weight | 1205 (59.0%) | 36 (63.2%) | 330 (57.1%) | 138 (59.5%) | 166 (59.1%) | 182 (54.7%) | 140 (63.6%) | 76 (58.5%) | 76 (67.9%) | 41 (61.2%) | 20 (58.8%) | ||
| Overweight | 443 (21.7%) | 12 (21.1%) | 126 (21.8%) | 49 (21.1%) | 70 (24.9%) | 73 (21.9%) | 45 (20.5%) | 28 (21.5%) | 23 (20.5%) | 10 (14.9%) | 7 (20.6%) | ||
| Obese | 274 (13.4%) | 6 (10.5%) | 84 (14.5%) | 29 (12.5%) | 39 (13.9%) | 54 (16.2%) | 18 (8.2%) | 17 (13.1%) | 10 (8.9%) | 12 (17.9%) | 5 (14.7%) | ||
| Parity | 0 | 1605 (50.7%) | 90 (61.6%) | 447 (50.6%) | 191 (47.5%) | 251 (50.3%) | 244 (49.9%) | 119 (50.4%) | 94 (55.3%) | 80 (55.2%) | 62 (45.9%) | 27 (47.4%) | 0.201 |
| 1–3 | 1416 (44.8%) | 48 (32.9%) | 387 (43.8%) | 193 (48.0%) | 226 (45.3%) | 222 (45.4%) | 114 (48.3%) | 71 (41.8%) | 64 (44.1%) | 65 (48.1%) | 26 (45.6%) | ||
| ≥4 | 142 (4.5%) | 8 (5.5%) | 50 (5.7%) | 18 (4.5%) | 22 (4.4%) | 23 (4.7%) | 3 (1.3%) | 5 (2.9%) | 1 (0.7%) | 8 (5.9%) | 4 (7.0%) | ||
| Nicotine consumption | 327 (10.3%) | 13 (8.9%) | 131 (14.8%) | 38 (9.5%) | 39 (7.8%) | 35 (7.2%) | 22 (9.3%) | 20 (11.8%) | 15 (10.3%) | 9 (6.7%) | 5 (8.8%) | <0.001 | |
| Obstetric risk factors 2 | 200 (6.3%) | 2 (1.4%) | 58 (6.6%) | 59 (14.7%) | 30 (6.0%) | 16 (3.3%) | 18 (7.6%) | 0 (0 %) | 8 (5.5%) | 5 (3.7%) | 4 (7.0%) | <0.001 | |
| Fetal sex 3 | Male | 1639 (52.0%) | 71 (49.0%) | 479 (54.3%) | 196 (48.9%) | 251 (50.8%) | 265 (54.4%) | 129 (54.7%) | 89 (53.0%) | 63 (43.4%) | 62 (45.9%) | 34 (60.7%) | 0.096 |
| Female | 1510 (48.0%) | 74 (51.0%) | 403 (45.7%) | 205 (51.1%) | 243 (49.2%) | 222 (45.6%) | 107 (45.3%) | 79 (47.0%) | 82 (56.6%) | 73 (54.1%) | 22 (39.3%) | ||
| Median birth weight (g) [IQR] | 1700 (860–2700) | 1570 (850–2810) | 1634.5 (781–2685) | 1575 (770–2580) | 1590 (817–2643) | 1988 (1050–2850) | 1565 (868–2625) | 1815 (990–2776) | 1912 (890–2810) | 1634 (930–2740) | 1380 (870–2555) | <0.001 | |
| Median birth height (cm) [IQR] | 43 (35–49) | 42 (35–50) | 43 (34–49) | 42 (34–49) | 42 (34–49) | 45 (36–50) | 42 (35–49) | 44 (38–50) | 46 (36–51) | 43 (36–50) | 41.5 (34–48) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muin, D.A.; Helmer, H.; Leitner, H.; Neururer, S. Epidemiology of Antepartum Stillbirths in Austria—A Population-Based Study between 2008 and 2020. J. Clin. Med. 2021, 10, 5828. https://doi.org/10.3390/jcm10245828
Muin DA, Helmer H, Leitner H, Neururer S. Epidemiology of Antepartum Stillbirths in Austria—A Population-Based Study between 2008 and 2020. Journal of Clinical Medicine. 2021; 10(24):5828. https://doi.org/10.3390/jcm10245828
Chicago/Turabian StyleMuin, Dana Anaïs, Hanns Helmer, Hermann Leitner, and Sabrina Neururer. 2021. "Epidemiology of Antepartum Stillbirths in Austria—A Population-Based Study between 2008 and 2020" Journal of Clinical Medicine 10, no. 24: 5828. https://doi.org/10.3390/jcm10245828
APA StyleMuin, D. A., Helmer, H., Leitner, H., & Neururer, S. (2021). Epidemiology of Antepartum Stillbirths in Austria—A Population-Based Study between 2008 and 2020. Journal of Clinical Medicine, 10(24), 5828. https://doi.org/10.3390/jcm10245828