
Cytotoxicity and Epidermal Barrier Function Evaluation of Common Antiseptics for Clinical Use in an Artificial Autologous Skin Model

 ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Isolation and Culture
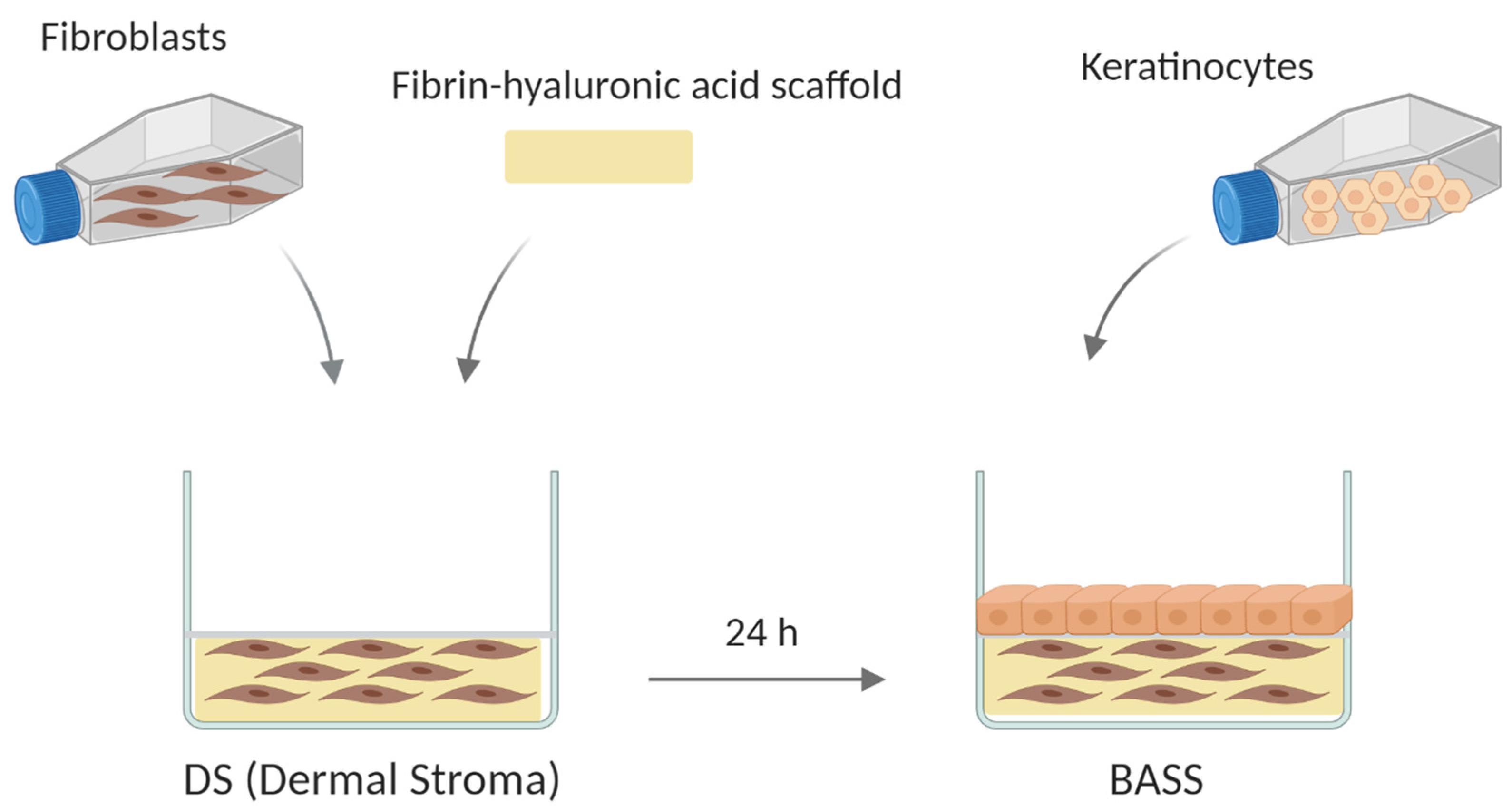
2.2. Bioengineered Artificial Skin Substitute (BASS) Manufacturing
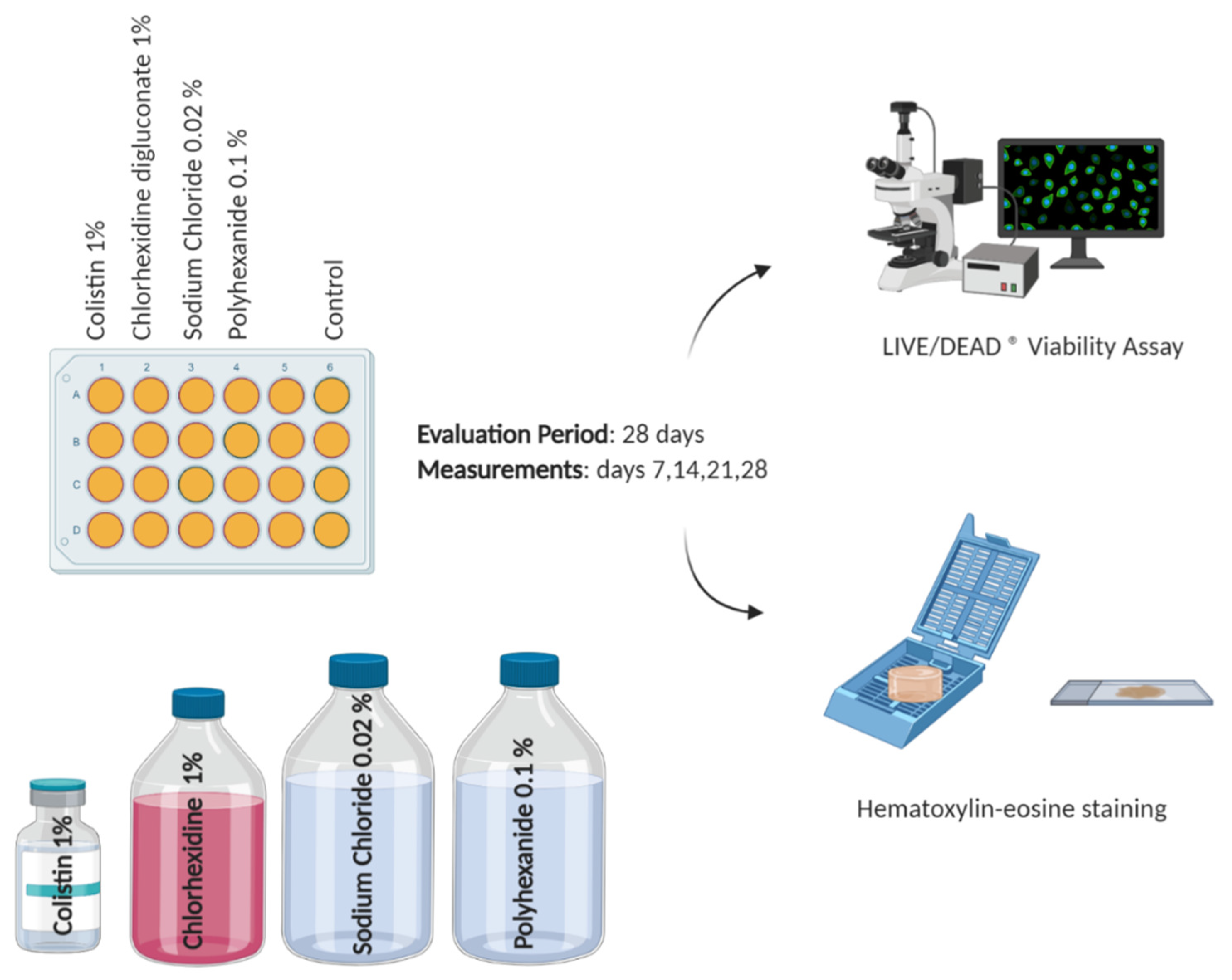
2.3. Antiseptic/Antibiotic Test
2.4. Viability Assay
2.5. Histological Analysis
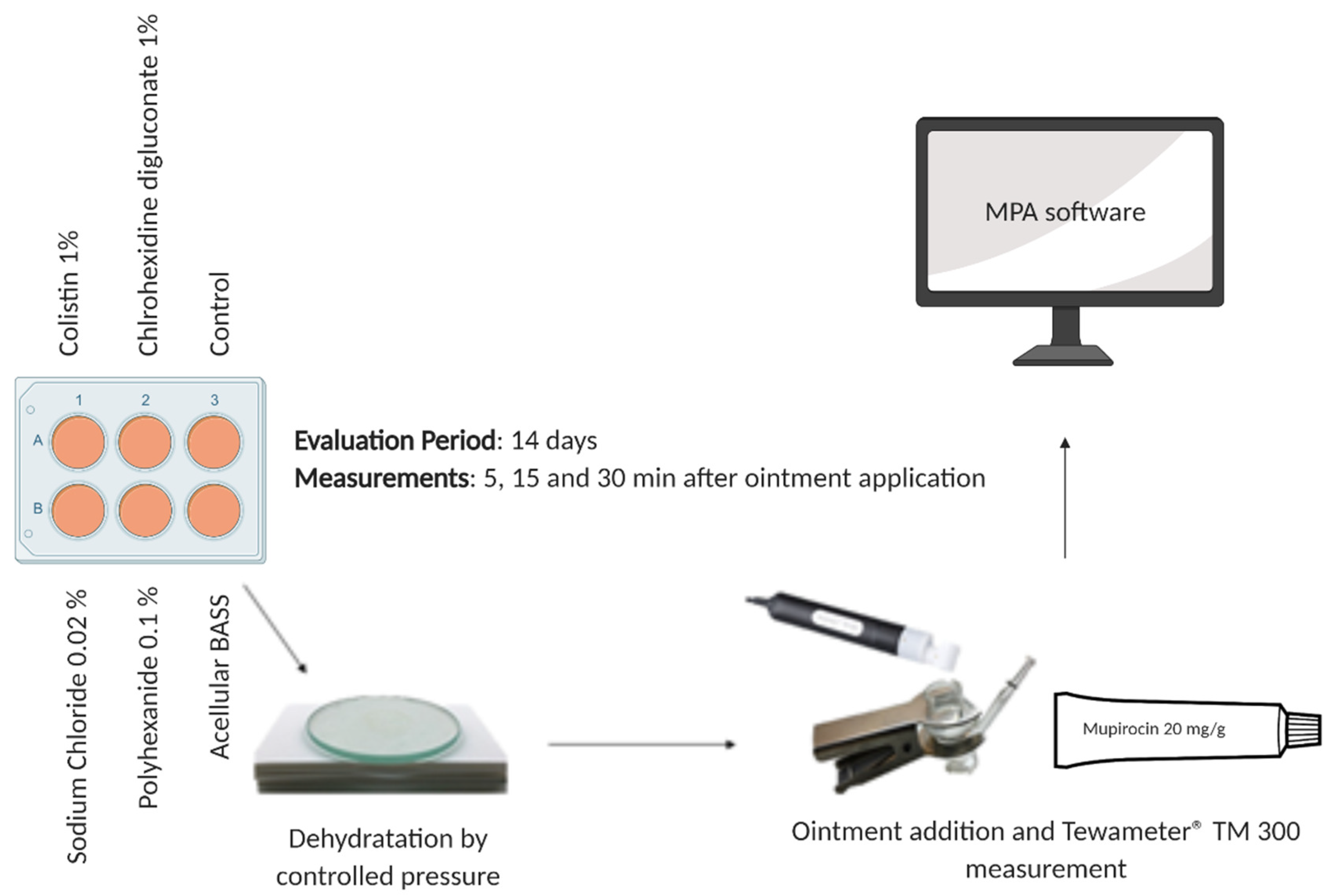
2.6. Epidermal Barrier Function Evaluation
2.7. Statistical Analysis
3. Results
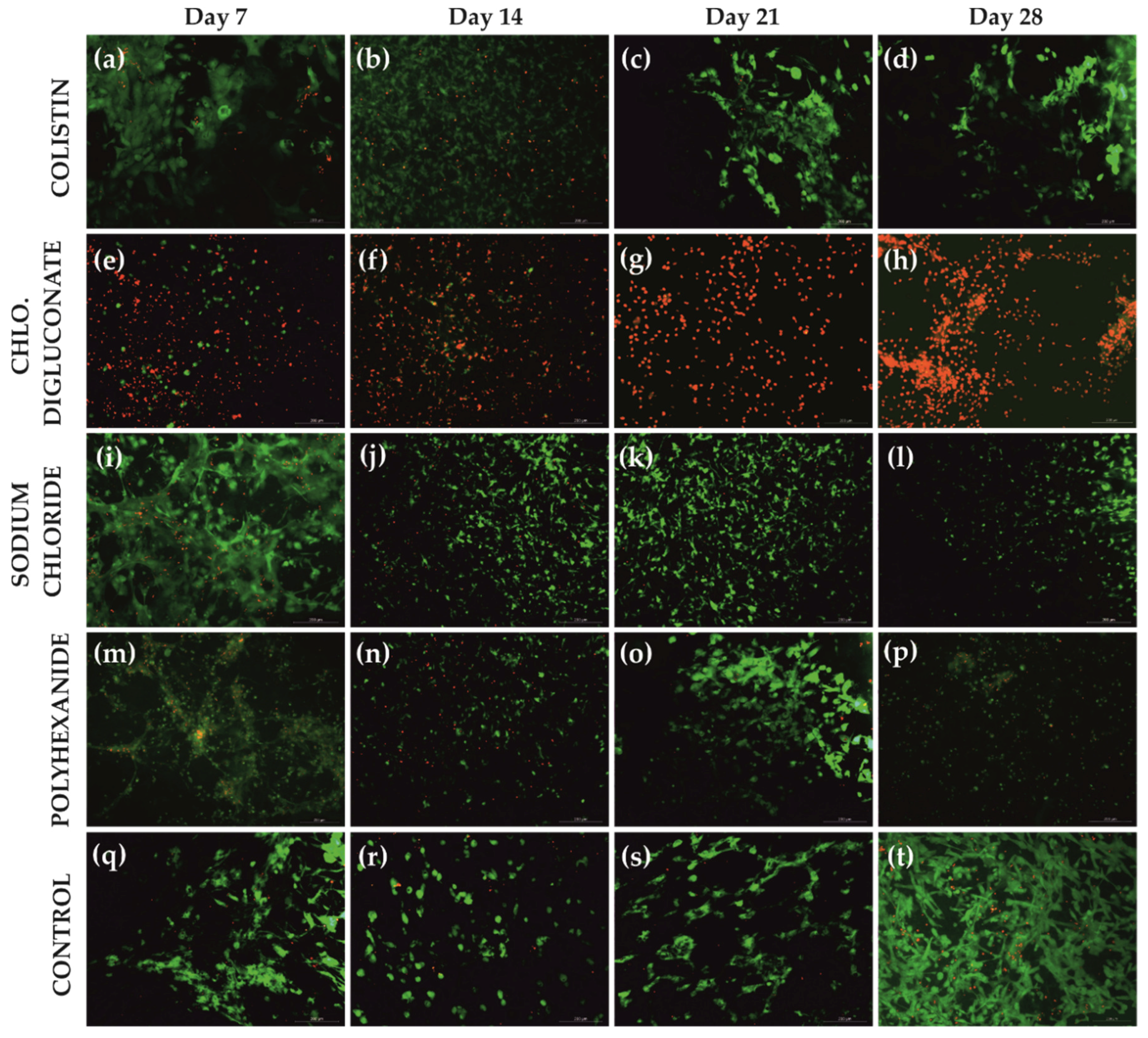
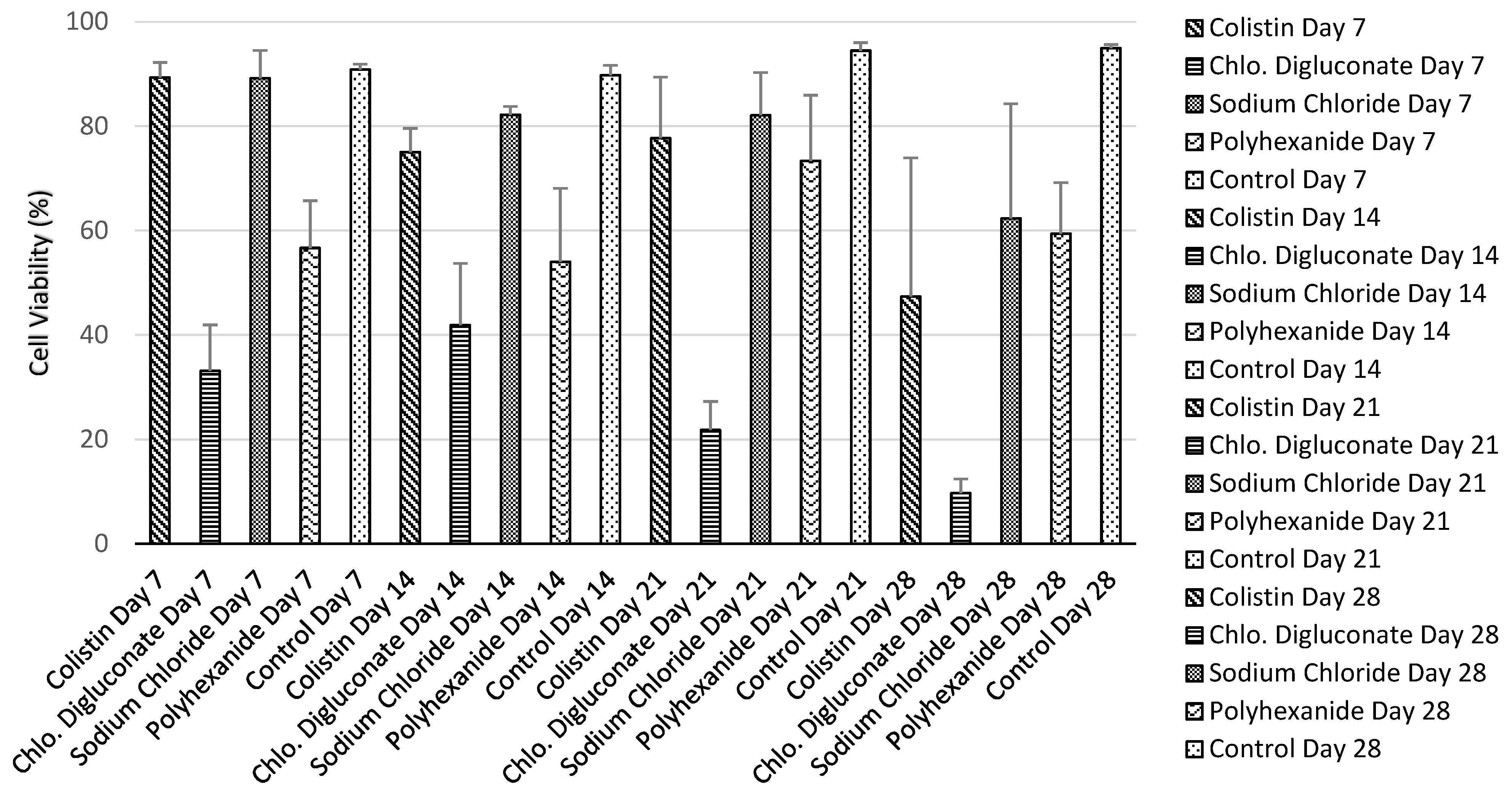
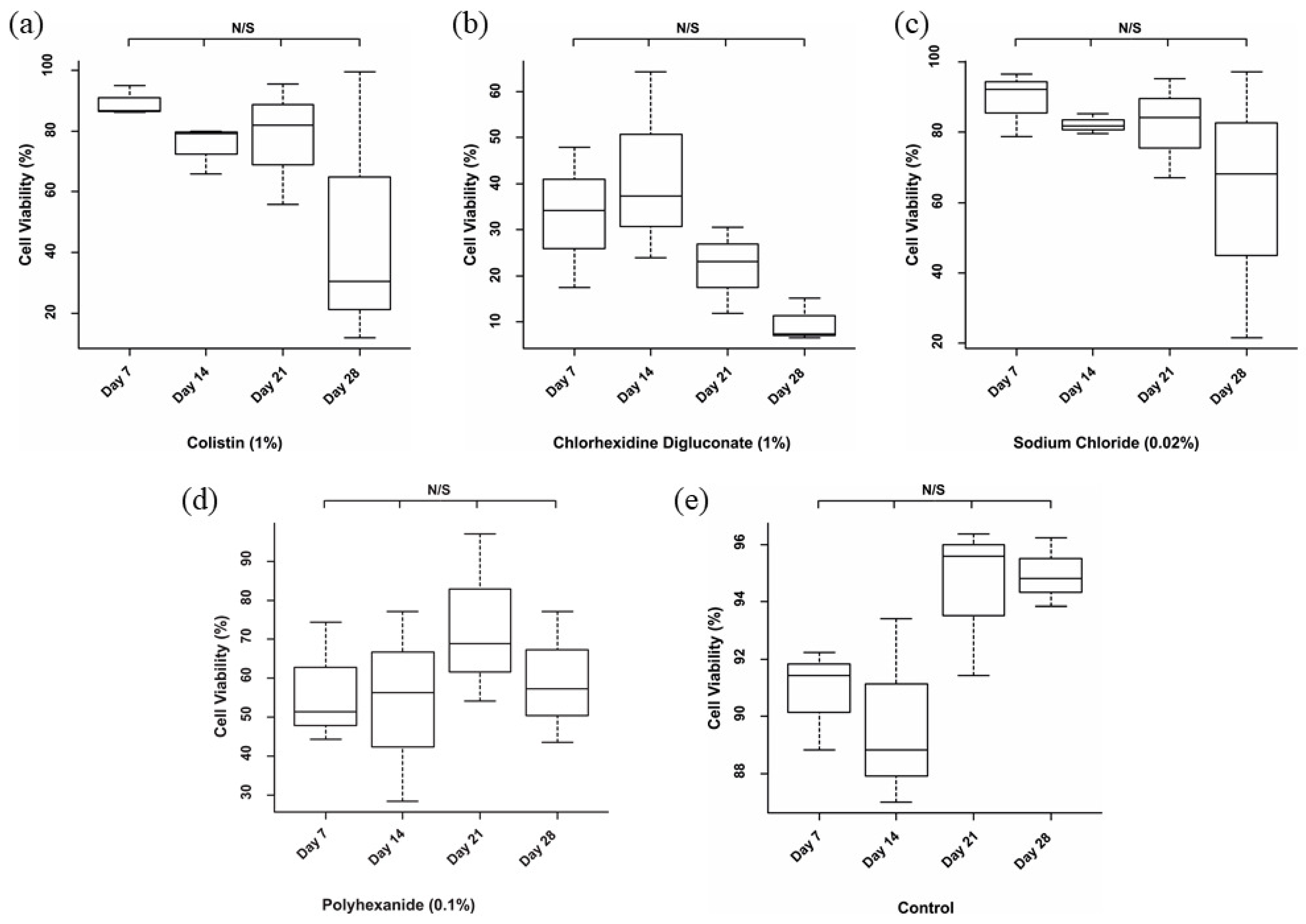
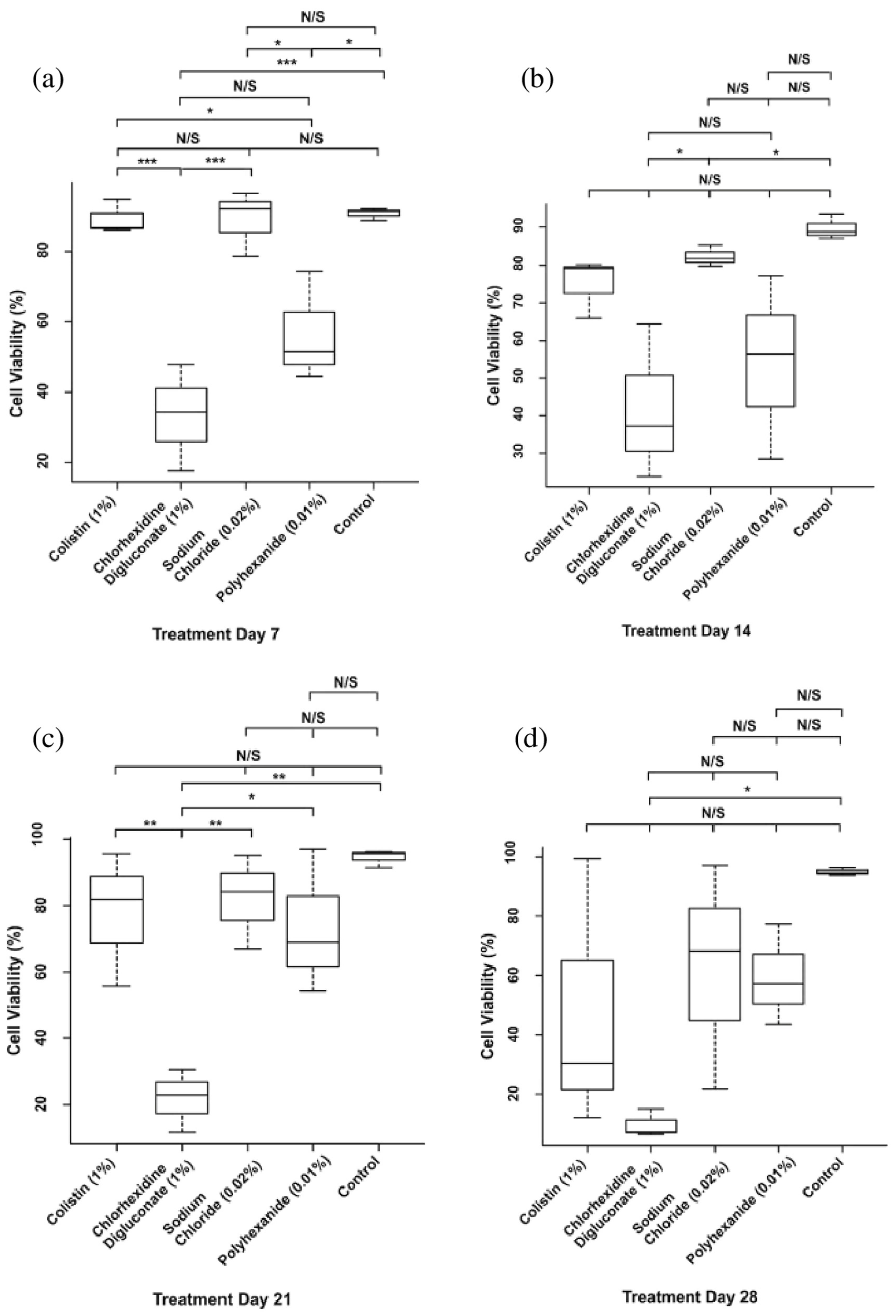
3.1. Chlorhexidine Digluconate Affects Cell Viability to a Greater Extent Compared to the Other Treatments
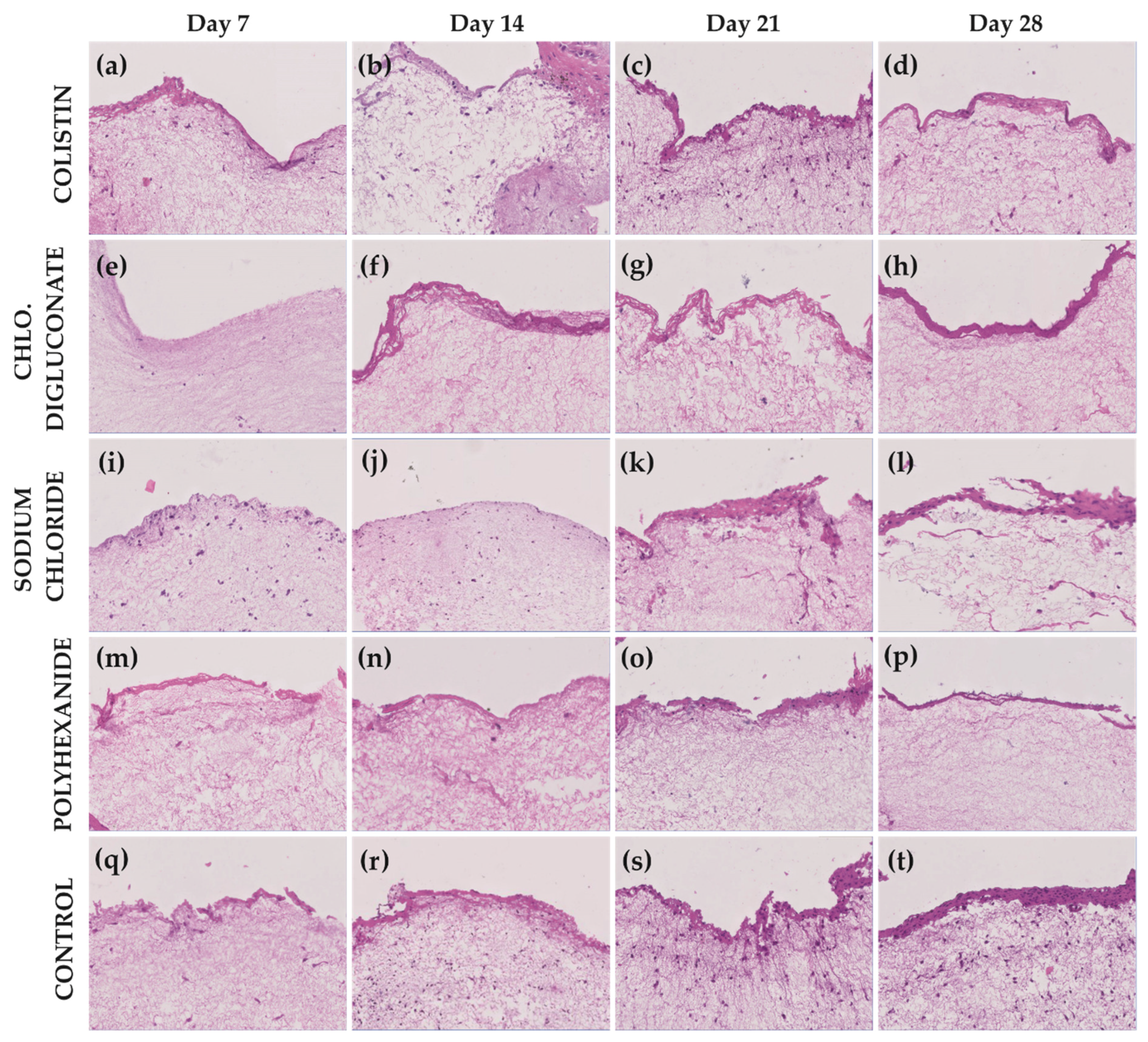
3.2. Chlorhexidine Digluconate and Polyhexanide Affect the Epithelium Integrity to a Greater Extent Compared to the Other Treatments
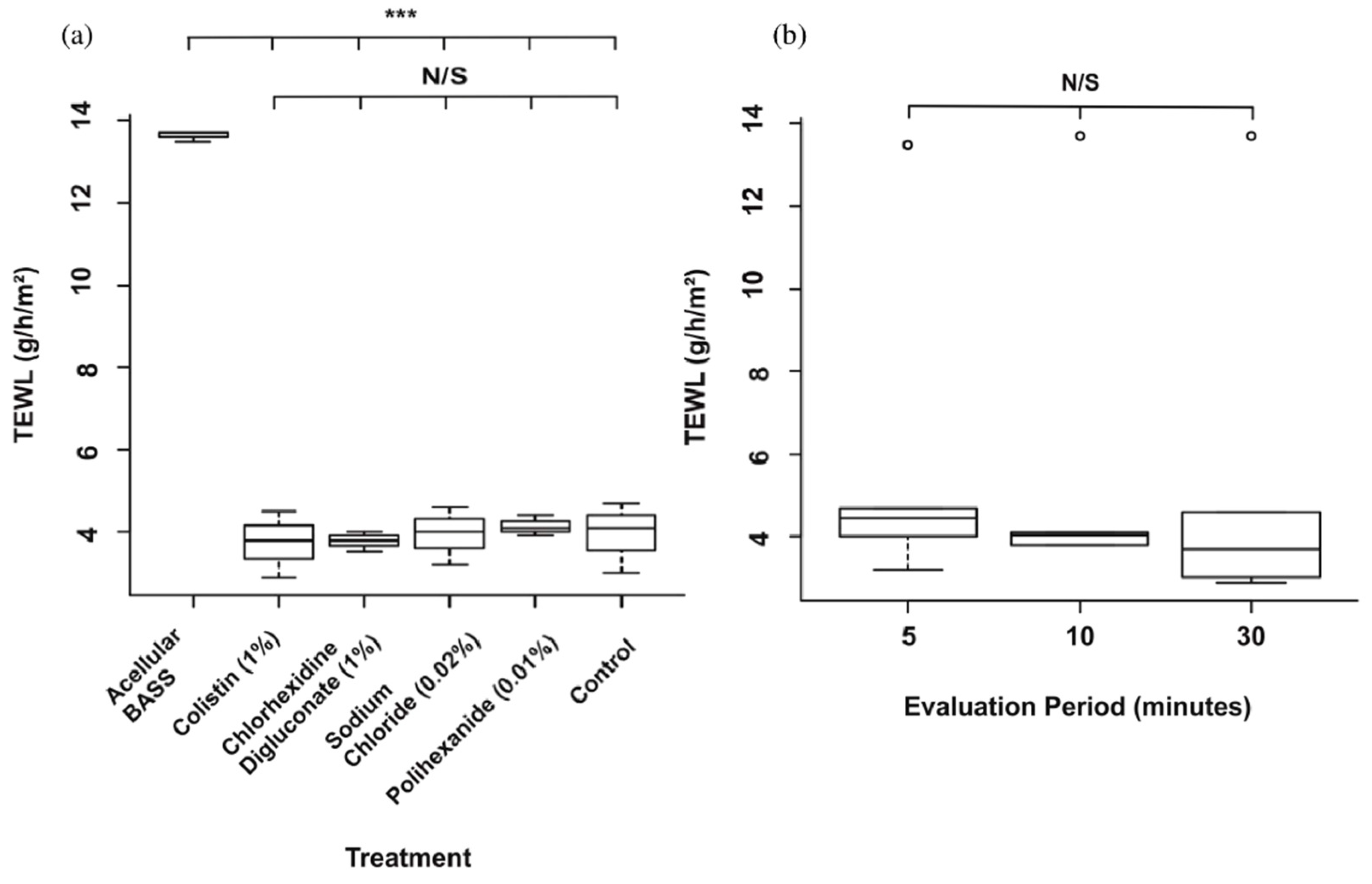
3.3. Skin Barrier Function Was Not Significantly Affected after the Antibiotic/Antiseptic Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vig, K.; Chaughari, A.; Tripathi, S.; Dixit, S.; Sahu, R.; Pillai, S.; Dennis, V.A.; Singh, S.R. Advances in skin regenation using tissue engineering. Int. J. Mol. Sci. 2017, 18, 789. [Google Scholar] [CrossRef]
- Nicholas, M.N.; Jeschke, M.G.; Amini-Nik, S. Methodologies in creating skin substitutes. Cell. Mol. Life Sci. 2016, 73, 3453–3472. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.; Walsh, C.; Yue, D.; Dardik, A.; Cheema, U. Current advancements and strategies in tissue engineering for wound healing: A comprehensive review. Adv. Wound Care 2017, 6, 191–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Sayed, P.; Hirt-Burri, N.; Roessingh, A.D.B.; Raffoul, W.; Applegate, L.A. Evolution of biological bandages as first cover for burn patients. Adv. Wound Care 2019, 8, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Oualla-Bachiri, W.; Fernández-González, A.; Quiñones-Vico, M.I.; Arias-Santiago, S. From grafts to human bioengineered vascularized skin substitutes. Int. J. Mol. Sci. 2020, 21, 8197. [Google Scholar] [CrossRef]
- Egea-Guerrero, J.J.; Carmona, G.; Correa, E.; Mata, R.; Arias-Santiago, S.; Alaminos, M.; Gacto, P.; Cuende, N. Transplant of tissue-engineered artificial autologous human skin in andalusia: An example of coordination and institutional collaboration. Transplant. Proc. 2019, 51, 3047–3050. [Google Scholar] [CrossRef] [PubMed]
- Haddad, A.G.; Giatsidis, G.; Orgill, D.P.; Halvorson, E.G. Skin substitutes and bioscaffolds: Temporary and permanent coverage. Clin. Plast. Surg. 2017, 44, 627–634. [Google Scholar] [CrossRef]
- González, A.F.; Moreno, A.M.L.; Ramos, M.D.M.D.P.; García, A.R.; Ibáñez, O.E.; Porcel, N.F.; Calvo, J.G.; Arrabal, M.; López-Carmona, F.; Arias-Santiago, S. Optimization of human keratinocyte culture to develop an artificial human skin model: Cell alternatives as feeder layer of advanced therapies. Actual. MEDICA 2016, 101, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Ścieżyńska, A.; Nogowska, A.; Sikorska, M.; Konys, J.; Karpińska, A.; Komorowski, M.; Ołdak, M.; Malejczyk, J. Isolation and culture of human primary keratinocytes—a methods review. Exp. Dermatol. 2019, 28, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Tracy, L.E.; Minasian, R.A.; Caterson, E. Extracellular matrix and dermal fibroblast function in the healing wound. Adv. Wound Care 2016, 5, 119–136. [Google Scholar] [CrossRef]
- Turner, N.J.; Badylak, S.F. The use of biologic scaffolds in the treatment of chronic nonhealing wounds. Adv. Wound Care 2015, 4, 490–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.M.; Melrose, J. Proteoglycans in normal and healing skin. Adv. Wound Care 2015, 4, 152–173. [Google Scholar] [CrossRef] [Green Version]
- Sierra-Sánchez, A.; Fernández-González, A.; Lizana-Moreno, O.E.-I.; Martinez-Lopez, A.J.; Guerrero-Calvo, N.; Fernández-Porcel, A.; Ruiz-García, A.; Ordoñez-Luque, V.; Carriel, S.A.-S. Hyaluronic acid biomaterial for human tissue-engineered skin substitutes: Preclinical comparative in vivo study of wound healing. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2414–2427. [Google Scholar]
- Ali, M.; Jahromi, M.; Sahandi, P.; Masoud, S.; Basri, M.; Sahandi, K.; Ghamarypour, A.; Aref, A.R.; Karimi, M.; Hamblin, M.R. Nanomedicine and advanced technologies for burns: Preventing infection and facilitating wound healing. Adv. Drug Deliv. Rev. 2018, 123, 33–64. [Google Scholar]
- Zieger, M.A.J.; Campana, G.; Tholpady, S.; Ziaie, B.; Sood, R.; Ochoa, M.; Rahimi, R. Skin regeneration using dermal substrates that contain autologous cells and silver nanoparticles to promote antibacterial activity: In vitro studies. Mil. Med. 2017, 182, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Norman, G.; Christie, J.; Liu, Z.; Mj, W.; Jm, J.; Hudson, T.; Edwards, J.; Dp, M.; Ia, H.; Jc, D. Antiseptics for burns (Review). Cochrane Database Syst. Rev. 2017, 7, 1–236. [Google Scholar]
- Barajas-Nava, L.A.; Lopez-Alcalde, J.; Roque i Figuls, M.; Solà, I.; Bonfill Cosp, X. Antibiotic prophylaxis for preventing burn wound infection. Cochrane Database Syst. Rev. 2013, 6. [Google Scholar]
- Hidalgo, E.; Dominguez, C. Mechanisms underlying chlorhexidine-induced cytotoxicity. Toxicol. Vitr. 2001, 15, 271–276. [Google Scholar] [CrossRef]
- Liu, J.X.; Werner, J.; Kirsch, T.; Zuckerman, J.D.; Virk, M. Cytotoxicity evaluation of chlorhexidine gluconate on human fibroblasts, myoblasts, and osteoblasts. J. Bone Jt. Infect. 2018, 3, 165–172. [Google Scholar] [CrossRef]
- Dabrowska, A.; Spano, F.; Derler, S.; Adlhart, C.; Spencer, N.; Rossi, R. The relationship between skin function, barrier properties, and body-dependent factors. Ski. Res. Technol. 2017, 24, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Sayed, P.; Tornay, D.; Hirt-Burri, N.; Roessingh, A.D.B.; Raffoul, W.; Applegate, L.A. Implications of chlorhexidine use in burn units for wound healing. Burn. 2020, 46, 1150–1156. [Google Scholar] [CrossRef]
- Sivathasan, N.; Goodfellow, P.B. Skin cleansers: The risks of chlorhexidine. J. Clin. Pharmacol. 2011, 51, 785–786. [Google Scholar] [CrossRef]
- Paulson, D.S.; Topp, R.; Boykin, R.E.; Schultz, G.; Yang, Q. Efficacy and safety of a novel skin cleansing formulation versus chlorhexidine gluconate. Am. J. Infect. Control. 2018, 46, 1262–1265. [Google Scholar] [CrossRef]
- Donskey, C.J.; Deshpande, A. Effect of chlorhexidine bathing in preventing infections and reducing skin burden and environmental contamination: A review of the literature. Am. J. Infect. Control. 2016, 44, e17–e21. [Google Scholar] [CrossRef] [Green Version]
- Sivathasan, N.; Sivathasan, N.; Vijayarajan, L. Chlorhexidine’s complications. J. Perioper. Pract. 2010, 20, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Bever, G.J.; Brodie, F.L.; Hwang, D.G. Corneal Injury from Presurgical Chlorhexidine Skin Preparation. World Neurosurg. 2016, 96, 610.e1–610.e4. [Google Scholar] [CrossRef]
- Niedner, R.; Schopf, E. Inhibition of wound healing by antiseptics. Br. J. Dermatol. 1986, 115, 41–44. [Google Scholar] [CrossRef]
- Popp, J.A.; Layon, A.J.; Nappo, R.; Richards, W.T.; Mozingo, D.W. Hospital-acquired infections and thermally injured patients: Chlorhexidine gluconate baths work. Am. J. Infect. Control. 2014, 42, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Guth, K.; Schäfer-Korting, M.; Fabian, E.; Landsiedel, R.; Van Ravenzwaay, B. Suitability of skin integrity tests for dermal absorption studies in vitro. Toxicol. Vitr. 2015, 29, 113–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, R.S.-D.; Fernández-González, A.; Quiñones-Vico, M.I.; Montero-Vilchez, T.; Arias-Santiago, S. Bioengineered skin intended as in vitro model for pharmacosmetics, skin disease study and environmental skin impact analysis. Biomedicines 2020, 8, 464. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Segura-Fernández-Nogueras, M.-V.; Pérez-Rodríguez, I.; Soler-Gongora, M.; Martinez-Lopez, A.; Fernández-González, A.; Molina-Leyva, A.; Arias-Santiago, S. Skin barrier function in psoriasis and atopic dermatitis: Transepidermal water loss and temperature as useful tools to assess disease severity. J. Clin. Med. 2021, 10, 359. [Google Scholar] [CrossRef] [PubMed]
- Netzlaff, F.; Kostka, K.-H.; Lehr, C.-M.; Schaefer, U.F. TEWL measurements as a routine method for evaluating the integrity of epidermis sheets in static Franz type diffusion cells in vitro. Limitations shown by transport data testing. Eur. J. Pharm. Biopharm. 2006, 63, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Alexander, H.; Brown, S.; Danby, S.; Flohr, C. Research techniques made simple: Transepidermal water loss measurement as a research tool. J. Investig. Dermatol. 2018, 138, 2295–2300.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trebilcock, K.; Heylings, J.; Wilks, M. In vitro tape stripping as a model for in vivo skin stripping. Toxicol. Vitr. 1994, 8, 665–667. [Google Scholar] [CrossRef]
- Dong, P.; Nikolaev, V.; Kröger, M.; Zoschke, C.; Darvin, M.E.; Witzel, C.; Lademann, J.; Patzelt, A.; Schäfer-Korting, M.; Meinke, M.C. Barrier-disrupted skin: Quantitative analysis of tape and cyanoacrylate stripping efficiency by multiphoton tomography. Int. J. Pharm. 2020, 574, 118843. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Day 7 | Day 14 | Day 21 | Day 28 |
|---|---|---|---|---|
| Colistin | 89.35% | 75.03% | 77.7% | 47.34% |
| Chlorhexidine digluconate | 33.16% | 41.86% | 21.81% | 9.69% |
| Sodium chloride | 89.15% | 82.18% | 82.08% | 62.34% |
| Polyhexanide | 56.66% | 53.99% | 73.37% | 59.41% |
| Control | 90.83% | 89.76% | 94.47% | 94.96% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quiñones-Vico, M.I.; Fernández-González, A.; Pérez-Castejón, E.; Montero-Vílchez, T.; Arias-Santiago, S. Cytotoxicity and Epidermal Barrier Function Evaluation of Common Antiseptics for Clinical Use in an Artificial Autologous Skin Model. J. Clin. Med. 2021, 10, 642. https://doi.org/10.3390/jcm10040642
Quiñones-Vico MI, Fernández-González A, Pérez-Castejón E, Montero-Vílchez T, Arias-Santiago S. Cytotoxicity and Epidermal Barrier Function Evaluation of Common Antiseptics for Clinical Use in an Artificial Autologous Skin Model. Journal of Clinical Medicine. 2021; 10(4):642. https://doi.org/10.3390/jcm10040642
Chicago/Turabian StyleQuiñones-Vico, María I., Ana Fernández-González, Elena Pérez-Castejón, Trinidad Montero-Vílchez, and Salvador Arias-Santiago. 2021. "Cytotoxicity and Epidermal Barrier Function Evaluation of Common Antiseptics for Clinical Use in an Artificial Autologous Skin Model" Journal of Clinical Medicine 10, no. 4: 642. https://doi.org/10.3390/jcm10040642
APA StyleQuiñones-Vico, M. I., Fernández-González, A., Pérez-Castejón, E., Montero-Vílchez, T., & Arias-Santiago, S. (2021). Cytotoxicity and Epidermal Barrier Function Evaluation of Common Antiseptics for Clinical Use in an Artificial Autologous Skin Model. Journal of Clinical Medicine, 10(4), 642. https://doi.org/10.3390/jcm10040642