
Perinatal Outcomes of Small for Gestational Age in Twin Pregnancies: Twin vs. Singleton Charts

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Variables and Outcomes
- Perinatal death, which includes stillbirth (IUD after 24 completed weeks of pregnancy) and early neonatal death (death of a newborn within seven days after birth),
- PTB before 34 weeks’ gestation,
- HDP,
- Admission to NNU.
2.3. Statistical Analysis
3. Results
3.1. Study Population
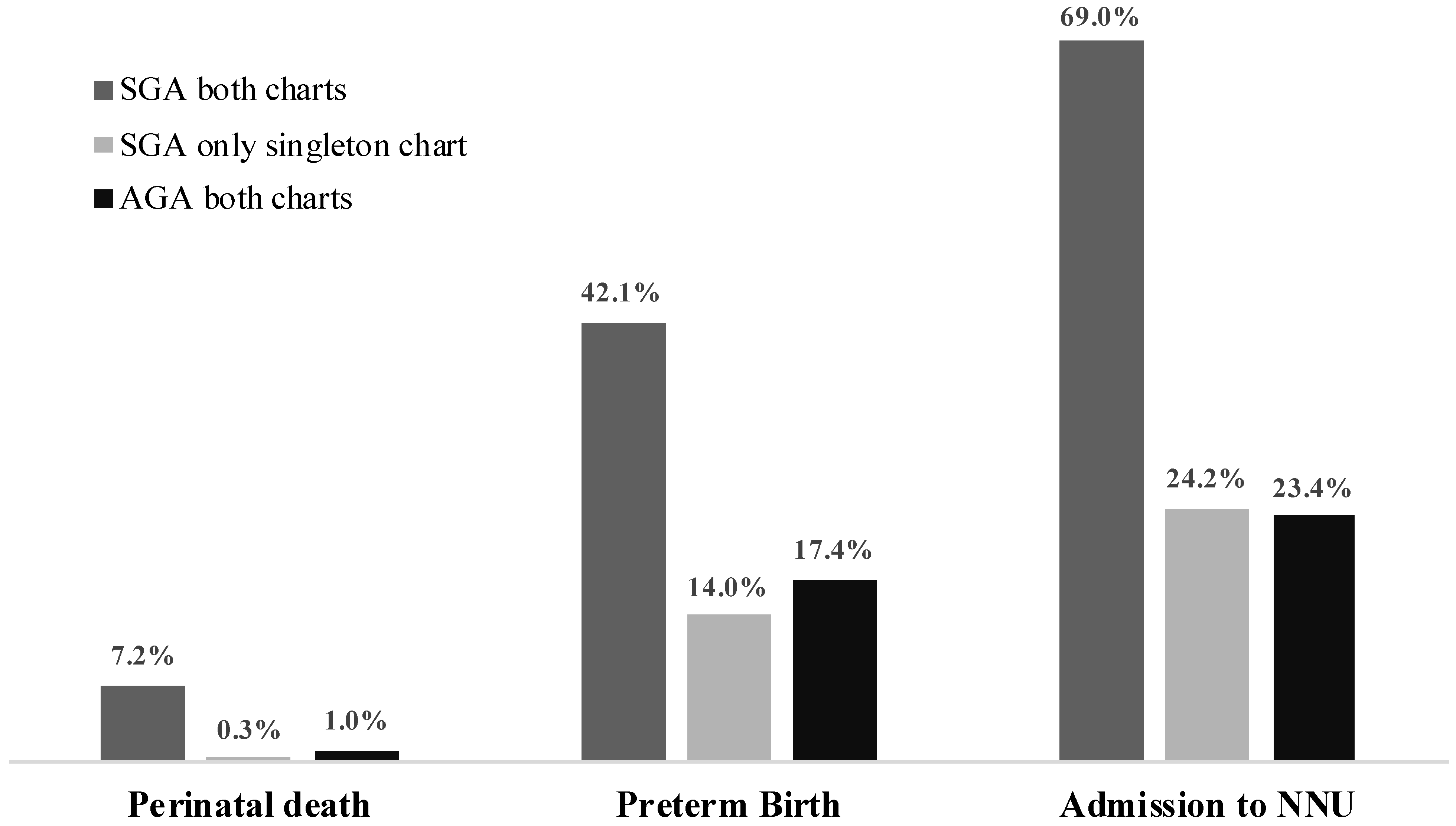
3.2. EFW Centile According to Twin References versus Singleton References
3.3. The Comparison of Doppler Assessment in Fetuses with EFW Less than 10th Centile According to Twin vs. Singleton Chart
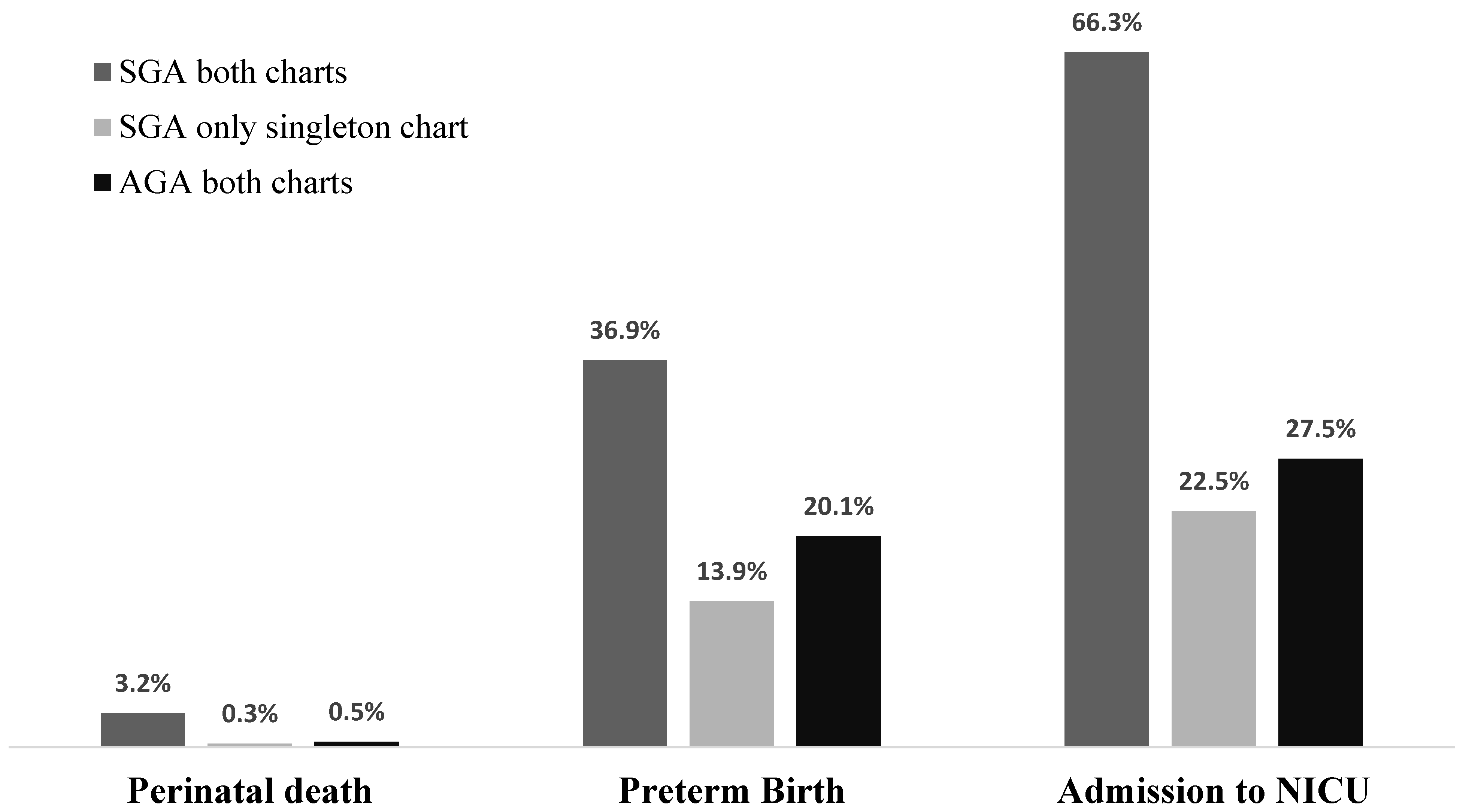
3.4. BW Centile According to Twin vs. Singleton Chart
4. Discussion
4.1. Summary of Main Findings
4.2. Interpretation of Study Findings and Comparison with Published Literature
4.3. Clinical and Research Implications
4.4. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Danon, D.; Sekar, R.; Hack, K.E.A.; Fisk, N.M. Increased Stillbirth in Uncomplicated Monochorionic Twin Pregnancies: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2013, 121, 1318–1326. [Google Scholar] [CrossRef]
- Lee, Y.M.; Wylie, B.J.; Simpson, L.L.; D’Alton, M.E. Twin chorionicity and the risk of stillbirth. Obstet. Gynecol. 2008, 111, 301–308. [Google Scholar] [CrossRef]
- Burgess, J.L.; Unal, E.R.; Nietert, P.J.; Newman, R.B. Risk of late-preterm stillbirth and neonatal morbidity for monochorionic and dichorionic twins. Am. J. Obstet. Gynecol. 2014, 210, 578.e1–578.e9. [Google Scholar] [CrossRef] [Green Version]
- D’Antonio, F.; Khalil, A.; Dias, T.; Thilaganathan, B. Weight discordance and perinatal mortality in twins: Analysis of the Southwest Thames Obstetric Research Collaborative (STORK) multiple pregnancy cohort. Ultrasound Obstet. Gynecol. 2013, 41, 643–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grantz, K.L.; Grewal, J.; Albert, P.S.; Wapner, R.; D’Alton, M.E.; Sciscione, A.; Grobman, W.A.; Wing, D.A.; Owen, J.; Newman, R.B.; et al. Dichorionic twin trajectories: The NICHD Fetal Growth Studies. Am. J. Obstet. Gynecol. 2016, 215, 221.e1–221.e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herruzo, A.J.; Martínez, L.; Biel, E.; Robles, R.; Rosales, M.A.; Miranda, J.A. Perinatal morbidity and mortality in twin pregnancies. Int. J. Gynecol. Obstet. 1991, 36, 17–22. [Google Scholar] [CrossRef]
- Kalafat, E.; Sebghati, M.; Thilaganathan, B.; Khalil, A.; Bahamie, A.; Bhide, A.; Deans, A.; Egbor, M.; Ellis, C.; Gandhi, H.; et al. Predictive accuracy of Southwest Thames Obstetric Research Collaborative (STORK) chorionicity-specific twin growth charts for stillbirth: A validation study. Ultrasound Obstet. Gynecol. 2019, 53, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Shivkumar, S.; Himes, K.P.; Hutcheon, J.A.; Platt, R.W. An ultrasound-based fetal weight reference for twins. Am. J. Obstet. Gynecol. 2015, 213, 224.e1–224.e9. [Google Scholar] [CrossRef]
- Stirrup, O.T.; Khalil, A.; D’Antonio, F.; Thilaganathan, B. Fetal growth reference ranges in twin pregnancy: Analysis of the Southwest Thames Obstetric Research Collaborative (STORK) multiple pregnancy cohort. Ultrasound Obstet. Gynecol. 2015, 45, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.R.; Kogan, M.; Martin, J.; Papiernik, E. What are the fetal growth patterns of singletons, twins, and triplets in the United States? Clin. Obstet. Gynecol. 1998, 41, 115–125. [Google Scholar] [CrossRef]
- Stirrup, O.T.; Khalil, A.; D’Antonio, F.; Thilaganathan, B. Patterns of Second- and Third-Trimester Growth and Discordance in Twin Pregnancy: Analysis of the Southwest Thames Obstetric Research Collaborative (STORK) Multiple Pregnancy Cohort. Fetal Diagn. Ther. 2017, 41, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Ghi, T.; Prefumo, F.; Fichera, A.; Lanna, M.; Periti, E.; Persico, N.; Viora, E.; Rizzo, G.; Arduini, D.; Arduino, S.; et al. Development of customized fetal growth charts in twins. Am. J. Obstet. Gynecol. 2017, 216, 514.e1–514.e17. [Google Scholar] [CrossRef]
- Ananth, C.V.; Vintzileos, A.M.; Shen-Schwarz, S.; Smulian, J.C.; Lai, Y.L. Standards of birth weight in twin gestations stratified by placental chorionicity. Obstet. Gynecol. 1998, 91, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Gabbay-Benziv, R.; Crimmins, S.; Contag, S.A. Reference values for sonographically estimated fetal weight in twin gestations stratified by chorionicity: A single center study. J. Ultrasound Med. 2017, 36, 793–798. [Google Scholar] [CrossRef]
- Gandhi, M.; Gandhi, R.; Mack, L.M.; Shypailo, R.; Adolph, A.L.; Puyau, M.R.; Wong, W.W.; Deter, R.L.; Sangi-Haghpeykar, H.; Lee, W.; et al. Estimated energy requirements increase across pregnancy in healthy women with dichorionic twins. Am. J. Clin. Nutr. 2018, 108, 775–783. [Google Scholar] [CrossRef]
- Gardosi, J. Toward safe standards for assessment of fetal growth in twin pregnancy. Am. J. Obstet. Gynecol. 2017, 216, 431–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolaides, K.H.; Wright, D.; Syngelaki, A.; Wright, A.; Akolekar, R. Fetal Medicine Foundation fetal and neonatal population weight charts. Ultrasound Obstet. Gynecol. 2018, 52, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Rodgers, M.; Baschat, A.; Bhide, A.; Gratacos, E.; Hecher, K.; Kilby, M.D.; Lewi, L.; Nicolaides, K.H.; Oepkes, D.; et al. ISUOG Practice Guidelines: Role of ultrasound in twin pregnancy. Ultrasound Obstet. Gynecol. 2016, 47, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Sepulveda, W.; Sebire, N.J.; Odibo, A.; Psarra, A.; Nicolaides, K.H. Prenatal determination of chorionicity in triplet pregnancy by ultrasonographic examination of the ipsilon zone. Obstet. Gynecol. 1996, 88, 855–858. [Google Scholar] [CrossRef]
- Poon, L.C.Y.; Tan, M.Y.; Yerlikaya, G.; Syngelaki, A.; Nicolaides, K.H. Birth weight in live births and stillbirths. Ultrasound Obstet. Gynecol. 2016, 48, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.P.; Fleming, J.E.E. A Critical Evaluation of Sonar “Crown-Rump Length” Measurements. BJOG Int. J. Obstet. Gynaecol. 1975, 82, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Dias, T.; Ladd, S.; Mahsud-Dornan, S.; Bhide, A.; Papageorghiou, A.T.; Thilaganathan, B. Systematic labeling of twin pregnancies on ultrasound. Ultrasound Obstet. Gynecol. 2011, 38, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Briffa, C.; Stirrup, O.; Huddy, C.; Richards, J.; Shetty, S.; Reed, K.; Khalil, A. Twin chorionicity-specific population birth-weight charts developed with adjustment for estimated fetal weight. Ultrasound Obstet. Gynecol. 2021, uog.23606. [Google Scholar] [CrossRef]
- Khalil, A.A.; Khan, N.; Bowe, S.; Familiari, A.; Papageorghiou, A.; Bhide, A.; Thilaganathan, B. Discordance in fetal biometry and Doppler are independent predictors of the risk of perinatal loss in twin pregnancies. Am. J. Obstet. Gynecol. 2015, 213, 222.e1–222.e10. [Google Scholar] [CrossRef]
- Gardosi, J.; Mongelli, M.; Wilcox, M.; Chang, A. An adjustable fetal weight standard. Ultrasound Obstet. Gynecol. 1995, 6, 168–174. [Google Scholar] [CrossRef]
- Giorgione, V.; Bhide, A.; Bhate, R.; Reed, K.; Khalil, A. Are Twin Pregnancies Complicated by Weight Discordance or Fetal Growth Restriction at Higher Risk of Preeclampsia? J. Clin. Med. 2020, 9, 3276. [Google Scholar] [CrossRef]
- Kalafat, E.; Abiola, A.; Thilaganathan, B.; Bhide, A.; Khalil, A. The association between hypertension in pregnancy and preterm birth with fetal growth restriction in singleton and Twin pregnancy: Use of Twin versus Singleton Charts. J. Clin. Med. 2020, 9, 2518. [Google Scholar] [CrossRef] [PubMed]
- Proctor, L.K.; Kfouri, J.; Hiersch, L.; Aviram, A.; Zaltz, A.; Kingdom, J.; Barrett, J.; Melamed, N. Association between hypertensive disorders and fetal growth restriction in twin compared with singleton gestations. Am. J. Obstet. Gynecol. 2019, 221, 251.e1–251.e8. [Google Scholar] [CrossRef]
- NICE Twin and Triplet Pregnancy. Available online: https://www.nice.org.uk/guidance/ng137 (accessed on 31 December 2020).
- ACOG. Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal Pregnancies. Acog 2016, 123, 1118–1132. [Google Scholar]



{kind=link}
{kind=link}
| Twin Pregnancies (n = 1740) | |
|---|---|
| Maternal age in years, median (IQR) | 34 (30–37) |
| Maternal body mass index in kg/m2, median (IQR) | 24.4 (21.8–27.9) |
| Nulliparous, n (%) | 975 (56) |
| Racial origin, n (%) | |
| 1122 (64.8) 279 (16.1) 205 (11.8) 29 (1.7) 97 (5.6) |
| Smokers, n (%) | 89 (5.2) |
| Assisted conception, n (%) | 477 (27.6) |
| Pre-existing hypertension, n (%) | 59 (3.4) |
| Gestational age at delivery in weeks, median (IQR) | 36.7 (34.6–37.4) |
| Hypertensive disorders of pregnancy, n (%) | 243 (14) |
| Preterm birth before 34 weeks, n (%) | 354 (20.3) |
| Twin-to-twin transfusion syndrome, n (%) | 54 (3.1) |
| Twins (n = 3480) | |
| Pregnancy outcome | |
| 31 (0.9) 22 (0.6) |
| Birthweight in grams, median (IQR) | 2301 (1902–2595) |
| Admission to the neonatal unit, n (%) | 1003 (29.1) |
| Adverse Outcomes | EFW-Twin Chart | EFW-Singleton Chart | BW-Twin Chart | BW-Singleton Chart | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SGA | AGA | p Value * | SGA | AGA | p Value * | SGA | AGA | p Value * | SGA | AGA | p Value * | |
| Perinatal death, n (%) | 20 (7.2) | 26 (0.8) | <0.0001 | 23 (2) | 23 (1) | 0.029 | 8 (3.2) | 13 (0.4) | <0.0001 | 11 (0.8) | 11 (0.5) | 0.263 |
| Preterm birth <34 weeks, n (%) | 117 (42.1) | 507 (16.4) | <0.0001 | 242 (20.6) | 282 (17.4) | 0.020 | 92 (36.9) | 567 (18.1) | <0.0001 | 242 (18.3) | 442 (20.8) | 0.067 |
| NNU admission, n (%) | 185 (69) | 736 (24) | <0.0001 | 401 (34.5) | 520 (23.9) | <0.0001 | 165 (66.3) | 811 (25.8) | <0.0001 | 406 (30.7) | 593 (28) | 0.095 |
| HDP, n (%) | 28 (21.2) | 210 (13.5) | 0.015 | 152 (13.9) | 86 (14.6) | 0.696 | 24 (23.5) | 215 (13.5) | 0.005 | 97 (15.1) | 143 (13.2) | 0.273 |
| Adverse Outcomes | Estimated Fetal Weight < 10th Centile | |||||
|---|---|---|---|---|---|---|
| Twin Chart | Singleton Chart | |||||
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Perinatal death | 9.14 | 5.0–16.6 | <0.0001 | 1.9 | 1.1–3.4 | 0.032 |
| Preterm birth prior to 34 weeks | 3.7 | 2.9–4.8 | <0.0001 | 1.2 | 1.0–1.5 | 0.020 |
| Neonatal unit admission | 7.1 | 5.4–9.3 | <0.0001 | 1.7 | 1.4–2.0 | <0.0001 |
| Hypertensive disorders of pregnancy | 1.7 | 1.1–2.7 | 0.016 | 1.1 | 0.8–1.4 | 0.696 |
| Birth Weight < 10th Centile | ||||||
| Twin Chart | Singleton Chart | |||||
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Perinatal death | 8.0 | 3.3–19.5 | <0.0001 | 1.6 | 0.7–3.7 | 0.268 |
| Preterm birth prior to 34 weeks | 2.7 | 2.0–3.5 | <0.0001 | 0.9 | 0.7–1.0 | 0.067 |
| Neonatal unit admission | 5.6 | 4.3–7.4 | <0.0001 | 1.1 | 1.0–1.3 | 0.095 |
| Hypertensive disorders of pregnancy | 2.0 | 1.2–3.2 | 0.006 | 1.2 | 0.9–1.5 | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giorgione, V.; Briffa, C.; Di Fabrizio, C.; Bhate, R.; Khalil, A. Perinatal Outcomes of Small for Gestational Age in Twin Pregnancies: Twin vs. Singleton Charts. J. Clin. Med. 2021, 10, 643. https://doi.org/10.3390/jcm10040643
Giorgione V, Briffa C, Di Fabrizio C, Bhate R, Khalil A. Perinatal Outcomes of Small for Gestational Age in Twin Pregnancies: Twin vs. Singleton Charts. Journal of Clinical Medicine. 2021; 10(4):643. https://doi.org/10.3390/jcm10040643
Chicago/Turabian StyleGiorgione, Veronica, Corey Briffa, Carolina Di Fabrizio, Rohan Bhate, and Asma Khalil. 2021. "Perinatal Outcomes of Small for Gestational Age in Twin Pregnancies: Twin vs. Singleton Charts" Journal of Clinical Medicine 10, no. 4: 643. https://doi.org/10.3390/jcm10040643
APA StyleGiorgione, V., Briffa, C., Di Fabrizio, C., Bhate, R., & Khalil, A. (2021). Perinatal Outcomes of Small for Gestational Age in Twin Pregnancies: Twin vs. Singleton Charts. Journal of Clinical Medicine, 10(4), 643. https://doi.org/10.3390/jcm10040643