
Cardiovascular and Renal Disease in Chronic Critical Illness

 ,
, 
Abstract
:1. Introduction
2. Definitions and Epidemiology of Chronic Critical Illness
3. Definitions, Epidemiology, and Risk for Cardiovascular and Renal Disease in Chronic Critical Illness
3.1. Cardiovascular Disease
3.2. Renal Disease
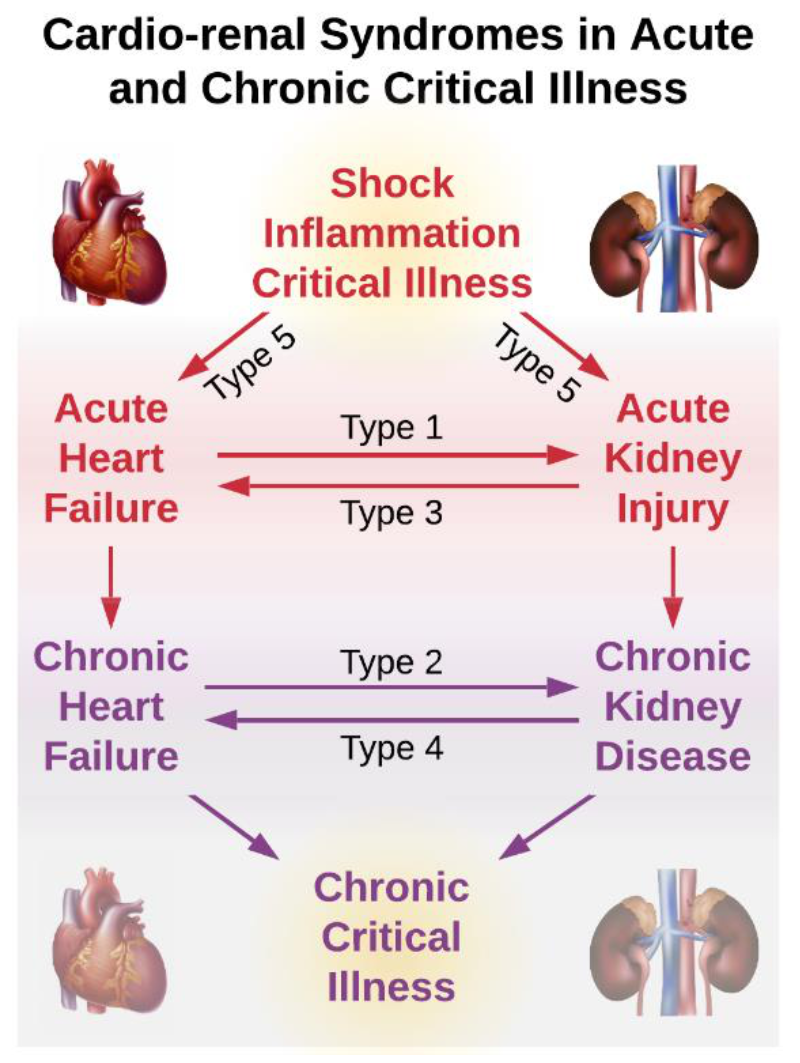
3.3. Associations between Renal and Cardiovascular Disease
4. Pathophysiology of Cardiovascular and Renal Disease in Chronic Critical Illness
5. Predicting Cardiovascular and Renal Disease in Chronic Critical Illness
6. Therapeutic Interventions for Cardiovascular and Renal Disease in Chronic Critical Illness
6.1. Behavioral and Lifestyle Interventions
6.2. Pharmacologic Interventions
6.3. Procedural Interventions
6.4. Treatment Paradigms
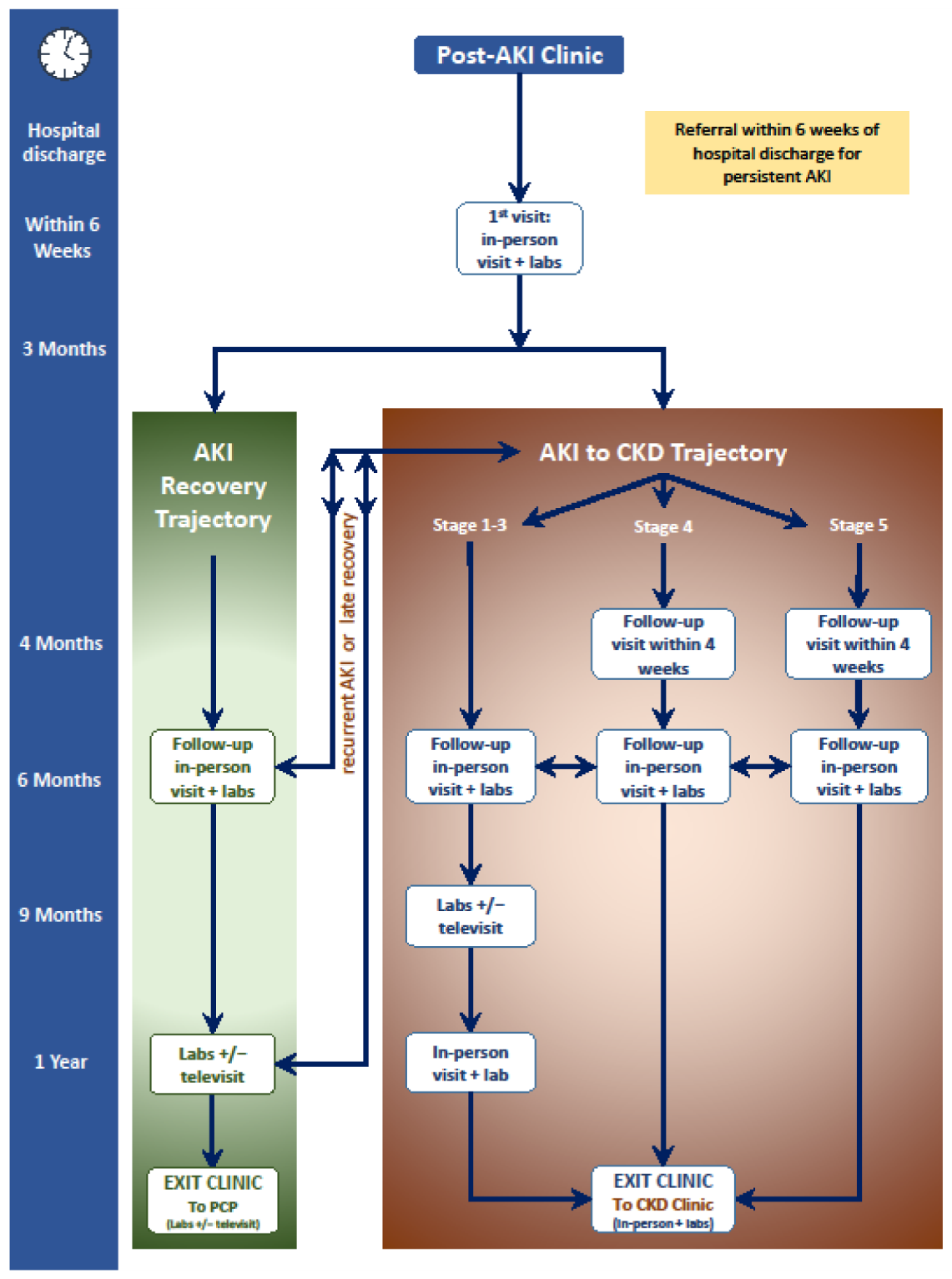
6.5. Acute Kidney Injury (AKI) Survivor Follow-Up Pathways
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zimmerman, J.E.; Kramer, A.A.; Knaus, W.A. Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012. Crit. Care 2013, 17, R81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, G.S.; Mannino, D.M.; Eaton, S.; Moss, M. The epidemiology of sepsis in the United States from 1979 through 2000. N. Engl. J. Med. 2003, 348, 1546–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, J.L.; Bristow, P.; Solomon, P.J.; George, C.; Hatt, G.K.; Ca, A.N.Z.I. Mortality and length-of-stay outcomes, 1993–2003, in the binational Australian and New Zealand intensive care adult patient database. Crit. Care Med. 2008, 36, 46–61. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, A.; Durand, M.A.; Grieve, R.; Harrison, D.; Rowan, K.; Green, J.; Cairns, J.; Black, N. Evaluation of modernisation of adult critical care services in England: Time series and cost effectiveness analysis. BMJ Brit. Med. J. 2009, 339. [Google Scholar] [CrossRef] [Green Version]
- Girard, K.; Raffin, T.A. The chronically critically ill: To save or let die? Respir Care 1985, 30, 339–347. [Google Scholar]
- Kahn, J.M.; Le, T.; Angus, D.C.; Cox, C.E.; Hough, C.L.; White, D.B.; Yende, S.; Carson, S.S.; ProVent Study Group Investigators. The epidemiology of chronic critical illness in the United States. Crit. Care Med. 2015, 43, 282–287. [Google Scholar] [CrossRef]
- Lokhandwala, S.; Escobar, B.; Chahin, A.; McCague, N.; Ghassemi, M.; Feng, M.; Celi, L.A. Risk factors for death in chronic critical illness. Intensive Care Med. Exp. 2015, 3, A449. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute Kidney Injury and Chronic Kidney Disease as Interconnected Syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Chronic Kidney Disease Prognosis Consortium; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.; Hutchison, A. Cardiovascular disease in patients with chronic kidney disease. Vasc. Health Risk Manag. 2009, 5, 713–722. [Google Scholar] [CrossRef] [Green Version]
- Braam, B.; Joles, J.A.; Danishwar, A.H.; Gaillard, C.A. Cardiorenal syndrome--current understanding and future perspectives. Nat. Rev. Nephrol. 2014, 10, 48–55. [Google Scholar] [CrossRef]
- Ronco, C.; McCullough, P.; Anker, S.D.; Anand, I.; Aspromonte, N.; Bagshaw, S.M.; Bellomo, R.; Berl, T.; Bobek, I.; Cruz, D.N.; et al. Cardio-renal syndromes: Report from the consensus conference of the acute dialysis quality initiative. Eur. Heart J. 2010, 31, 703–711. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Raymond, S.L.; Stortz, J.A.; Horiguchi, H.; Brakenridge, S.C.; Gardner, A.; Efron, P.A.; Bihorac, A.; Segal, M.; Moore, F.A.; et al. Chronic Critical Illness and the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome. Front. Immunol. 2018, 9, 1511. [Google Scholar] [CrossRef]
- Rosenthal, M.D.; Kamel, A.Y.; Rosenthal, C.M.; Brakenridge, S.; Croft, C.A.; Moore, F.A. Chronic Critical Illness: Application of What We Know. Nutr. Clin. Pr. 2018, 33, 39–45. [Google Scholar] [CrossRef]
- Iwashyna, T.J.; Hodgson, C.L.; Pilcher, D.; Bailey, M.; van Lint, A.; Chavan, S.; Bellomo, R. Timing of onset and burden of persistent critical illness in Australia and New Zealand: A retrospective, population-based, observational study. Lancet Respir. Med. 2016, 4, 566–573. [Google Scholar] [CrossRef]
- Mira, J.C.; Cuschieri, J.; Ozrazgat-Baslanti, T.; Wang, Z.K.; Ghita, G.L.; Loftus, T.J.; Stortz, J.A.; Raymond, S.L.; Lanz, J.D.; Hennessy, L.V.; et al. The Epidemiology of Chronic Critical Illness after Severe Traumatic Injury at Two Level-One Trauma Centers*. Crit. Care Med. 2017, 45, 1989–1996. [Google Scholar] [CrossRef]
- Stortz, J.A.; Mira, J.C.; Raymond, S.L.; Loftus, T.J.; Ozrazgat-Baslanti, T.; Wang, Z.K.; Ghita, G.L.; Leeuwenburgh, C.; Segal, M.S.; Bihorac, A.; et al. Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients. J. Trauma Acute Care Surg. 2018, 84, 342–349. [Google Scholar] [CrossRef]
- Nelson, J.E.; Tandon, N.; Mercado, A.F.; Camhi, S.L.; Ely, W.; Morrison, S. Brain dysfunction–Another burden for the chronically critically ill. Arch. Intern. Med. 2006, 166, 1993–1999. [Google Scholar] [CrossRef] [Green Version]
- Cox, C.E.; Carson, S.S.; Lindquist, J.H.; Olsen, M.K.; Govert, J.A.; Chelluri, L.; Quality of Life After Mechanical Ventilation in the Aged (QOL-MV) Investigators. Differences in one-year health outcomes and resource utilization by definition of prolonged mechanical ventilation: A prospective cohort study. Crit. Care 2007, 11, R9. [Google Scholar] [CrossRef] [Green Version]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Executive summary: Heart disease and stroke statistics--2013 update: A report from the American Heart Association. Circulation 2013, 127, 143–152. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [Green Version]
- Lewington, A.J.; Cerda, J.; Mehta, R.L. Raising awareness of acute kidney injury: A global perspective of a silent killer. Kidney Int. 2013, 84, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Li, P.K.; Burdmann, E.A.; Mehta, R.L.; World Kidney Day Steering Committee. Acute kidney injury: Global health alert. Kidney Int. 2013, 83, 372–376. [Google Scholar] [CrossRef] [Green Version]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute Kidney Injury Increases Risk of ESRD among Elderly. J. Am. Soc. Nephrol. 2009, 20, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients—A multinational, multicenter study. JAMA-J. Am. Med. Assoc. 2005, 294, 813–818. [Google Scholar] [CrossRef] [Green Version]
- Ozrazgat-Baslanti, T.; Loftus, T.J.; Mohandas, R.; Wu, Q.; Brakenridge, S.; Brumback, B.; Efron, P.A.; Anton, S.; Moore, F.A.; Moldawer, L.L.; et al. Clinical Trajectories of Acute Kidney Injury in Surgical Sepsis: A Prospective Observational Study. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- van der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B.C.; Woodward, M.; Levey, A.; de Jong, P.; Gansevoort, R.T.; Chronic Kidney Disease Prognosis Consortium; van der Velde, M.; et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011, 79, 1341–1352. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Astor, B.C.; Coresh, J.; Heiss, G.; Pettitt, D.; Sarnak, M.J. Kidney function and anemia as risk factors for coronary heart disease and mortality: The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2006, 151, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Kottgen, A.; Russell, S.D.; Loehr, L.R.; Crainiceanu, C.M.; Rosamond, W.D.; Chang, P.P.; Chambless, L.E.; Coresh, J. Reduced kidney function as a risk factor for incident heart failure: The Atherosclerosis Risk in Communities (ARIC) study. J. Am. Soc. Nephrol. 2007, 18, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Lopez, F.L.; Matsushita, K.; Loehr, L.R.; Agarwal, S.K.; Chen, L.Y.; Soliman, E.Z.; Astor, B.C.; Coresh, J. Chronic Kidney Disease Is Associated With the Incidence of Atrial Fibrillation The Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2011, 123, U2946–U2981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramson, J.L.; Jurkovitz, C.T.; Vaccarino, V.; Weintraub, W.S.; McClellan, W. Chronic kidney disease, anemia, and incident stroke in a middle-aged, community-based population: The ARIC Study. Kidney Int. 2003, 64, 610–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wattanakit, K.; Folsom, A.R.; Selvin, E.; Coresh, J.; Hirsch, A.T.; Weatherley, B.D. Kidney function and risk of peripheral arterial disease: Results from the Atherosclerosis Risk in Communities (ARIC) Study. J. Am. Soc. Nephrol. 2007, 18, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.T.; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Chronic Kidney Disease Prognosis Consortium. Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011, 80, 93–104. [Google Scholar] [CrossRef] [Green Version]
- Keith, D.S.; Nichols, G.A.; Gullion, C.M.; Brown, J.B.; Smith, D.H. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch. Intern. Med. 2004, 164, 659–663. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.; Singer, J.; Thompson, C.R.; Ross, H.; Lewis, M. Prevalent left ventricular hypertrophy in the predialysis population: Identifying opportunities for intervention. Am. J. Kidney Dis. 1996, 27, 347–354. [Google Scholar] [CrossRef]
- Levin, A.; Foley, R.N. Cardiovascular disease in chronic renal insufficiency. Am. J. Kidney Dis. 2000, 36, S24–S30. [Google Scholar] [CrossRef]
- Schiffrin, E.L.; Lipman, M.L.; Mann, J.F. Chronic kidney disease: Effects on the cardiovascular system. Circulation 2007, 116, 85–97. [Google Scholar] [CrossRef] [Green Version]
- Pannier, B.; Guerin, A.P.; Marchais, S.J.; Safar, M.E.; London, G.M. Stiffness of capacitive and conduit arteries: Prognostic significance for end-stage renal disease patients. Hypertension 2005, 45, 592–596. [Google Scholar] [CrossRef] [Green Version]
- Drechsler, C.; Krane, V.; Winkler, K.; Dekker, F.W.; Wanner, C. Changes in adiponectin and the risk of sudden death, stroke, myocardial infarction, and mortality in hemodialysis patients. Kidney Int. 2009, 76, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Green, D.; Roberts, P.R.; New, D.I.; Kalra, P.A. Sudden cardiac death in hemodialysis patients: An in-depth review. Am. J. Kidney Dis. 2011, 57, 921–929. [Google Scholar] [CrossRef]
- Krane, V.; Wanner, C. Statins, inflammation and kidney disease. Nat. Rev. Nephrol. 2011, 7, 385–397. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Torio, C.M.; Andrews, R.M. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011: Statistical Brief #160. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006. [Google Scholar]
- Poston, J.T.; Koyner, J.L. Sepsis associated acute kidney injury. BMJ 2019, 364, k4891. [Google Scholar] [CrossRef]
- Bellomo, R.; Kellum, J.A.; Ronco, C.; Wald, R.; Martensson, J.; Maiden, M.; Bagshaw, S.M.; Glassford, N.J.; Lankadeva, Y.; Vaara, S.T.; et al. Acute kidney injury in sepsis. Intensive Care Med. 2017, 43, 816–828. [Google Scholar] [CrossRef] [Green Version]
- White, L.E.; Hassoun, H.T.; Bihorac, A.; Moore, L.J.; Sailors, R.M.; McKinley, B.A.; Valdivia, A.; Moore, F.A. Acute kidney injury is surprisingly common and a powerful predictor of mortality in surgical sepsis. J. Trauma Acute Care Surg. 2013, 75, 432–438. [Google Scholar] [CrossRef] [Green Version]
- White, L.E.; Chaudhary, R.; Moore, L.J.; Moore, F.A.; Hassoun, H.T. Surgical sepsis and organ crosstalk: The role of the kidney. J. Surg. Res 2011, 167, 306–315. [Google Scholar] [CrossRef] [Green Version]
- Bihorac, A.; Brennan, M.; Ozrazgat-Baslanti, T.; Bozorgmehri, S.; Efron, P.A.; Moore, F.A.; Segal, M.S.; Hobson, C.E. National surgical quality improvement program underestimates the risk associated with mild and moderate postoperative acute kidney injury. Crit. Care Med. 2013, 41, 2570–2583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and Mortality Associated With Postoperative Acute Kidney Injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Spies, C.; Haude, V.; Fitzner, R.; Schroder, K.; Overbeck, M.; Runkel, N.; Schaffartzik, W. Serum cardiac troponin T as a prognostic marker in early sepsis. Chest 1998, 113, 1055–1063. [Google Scholar] [CrossRef]
- Turner, A.; Tsamitros, M.; Bellomo, R. Myocardial cell injury in septic shock. Crit. Care Med. 1999, 27, 1775–1780. [Google Scholar] [CrossRef]
- Arlati, S.; Brenna, S.; Prencipe, L.; Marocchi, A.; Casella, G.P.; Lanzani, M.; Gandini, C. Myocardial necrosis in ICU patients with acute non-cardiac disease: A prospective study. Intensive Care Med. 2000, 26, 31–37. [Google Scholar] [CrossRef]
- Mehta, N.J.; Khan, I.A.; Gupta, V.; Jani, K.; Gowda, R.M.; Smith, P.R. Cardiac troponin I predicts myocardial dysfunction and adverse outcome in septic shock. Int. J. Cardiol. 2004, 95, 13–17. [Google Scholar] [CrossRef]
- Ammann, P.; Maggiorini, M.; Bertel, O.; Haenseler, E.; Joller-Jemelka, H.I.; Oechslin, E.; Minder, E.I.; Rickli, H.; Fehr, T. Troponin as a risk factor for mortality in critically ill patients without acute coronary syndromes. J. Am. Coll. Cardiol. 2003, 41, 2004–2009. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Hirshberg, E.L.; Wilson, E.L.; Stanfield, V.; Kuttler, K.G.; Majercik, S.; Beesley, S.J.; Orme, J.; Hopkins, R.O.; Brown, S.M. Impact of Critical Illness on Resource Utilization: A Comparison of Use in the Year Before and After ICU Admission. Crit. Care Med. 2019, 47, 1497–1504. [Google Scholar] [CrossRef]
- Mira, J.C.; Brakenridge, S.C.; Moldawer, L.L.; Moore, F.A. Persistent Inflammation, Immunosuppression and Catabolism Syndrome. Crit. Care Clin. 2017, 33, 245. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, C.; Hussain, S.N.A.; Mathur, S.; Picard, M.; Herridge, M.; Correa, J.; Bain, A.; Guo, Y.T.; Advani, A.; Advani, S.L.; et al. Mechanisms of Chronic Muscle Wasting and Dysfunction after an Intensive Care Unit Stay. Am. J. Respir. Crit. Care 2016, 194, 821–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puthucheary, Z.A.; Rewal, J.; McPhail, M.J.W.; Dew, T.; Phadke, R.; Rowlerson, A.; Harridge, S.D.R.; Montgomery, H.E.; Hart, N. Tumour Necrosis Factor Receptor 1 Shedding Is Related to Acute Skeletal Muscle Wasting in Critical Illness. Thorax 2014, 69, A75-A75. [Google Scholar] [CrossRef] [Green Version]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA J. Am. Med. Assoc. 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, L.F.; Cuenca, A.G.; Efron, P.A.; Ang, D.; Bihorac, A.; McKinley, B.A.; Moldawer, L.L.; Moore, F.A. Persistent inflammation and immunosuppression: A common syndrome and new horizon for surgical intensive care. J. Trauma. Acute. Care Surg. 2012, 72, 1491–1501. [Google Scholar] [CrossRef] [Green Version]
- Szummer, K.; Lundman, P.; Jacobson, S.H.; Schon, S.; Lindback, J.; Stenestrand, U.; Wallentin, L.; Jernberg, T.; Swedeheart. Relation between renal function, presentation, use of therapies and in-hospital complications in acute coronary syndrome: Data from the SWEDEHEART register. J. Intern. Med. 2010, 268, 40–49. [Google Scholar] [CrossRef]
- Charytan, D.M.; Setoguchi, S.; Solomon, D.H.; Avorn, J.; Winkelmayer, W.C. Clinical presentation of myocardial infarction contributes to lower use of coronary angiography in patients with chronic kidney disease. Kidney Int. 2007, 71, 938–945. [Google Scholar] [CrossRef] [Green Version]
- Apple, F.S.; Murakami, M.M.; Pearce, L.A.; Herzog, C.A. Predictive value of cardiac troponin I and T for subsequent death in end-stage renal disease. Circulation 2002, 106, 2941–2945. [Google Scholar] [CrossRef] [Green Version]
- James, M.T.; Pannu, N.; Hemmelgarn, B.R.; Austin, P.C.; Tan, Z.; McArthur, E.; Manns, B.J.; Tonelli, M.; Wald, R.; Quinn, R.R.; et al. Derivation and External Validation of Prediction Models for Advanced Chronic Kidney Disease Following Acute Kidney Injury. JAMA 2017, 318, 1787–1797. [Google Scholar] [CrossRef]
- Damen, J.A.; Hooft, L.; Schuit, E.; Debray, T.P.; Collins, G.S.; Tzoulaki, I.; Lassale, C.M.; Siontis, G.C.; Chiocchia, V.; Roberts, C.; et al. Prediction models for cardiovascular disease risk in the general population: Systematic review. BMJ 2016, 353, i2416. [Google Scholar] [CrossRef] [Green Version]
- Birkhead, G.S.; Klompas, M.; Shah, N.R. Uses of electronic health records for public health surveillance to advance public health. Annu. Rev. Public Health 2015, 36, 345–359. [Google Scholar] [CrossRef] [Green Version]
- Adler-Milstein, J.; Holmgren, A.J.; Kralovec, P.; Worzala, C.; Searcy, T.; Patel, V. Electronic health record adoption in US hospitals: The emergence of a digital “advanced use” divide. J. Am. Med. Inf. Assoc. 2017, 24, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Stanford Medicine 2017 Health Trends Report: Harnessing the Power of Data in Health. Available online: http://med.stanford.edu/content/dam/sm/sm-news/documents/StanfordMedicineHealthTrendsWhitePaper2017.pdf (accessed on 23 February 2019).
- Lysak, N.; Hashemighouchani, H.; Davoudi, A.; Pourafshar, N.; Loftus, T.J.; Ruppert, M.; Efron, P.A.; Rashidi, P.; Bihorac, A.; Ozrazgat-Baslanti, T. Cardiovascular death and progression to end-stage renal disease after major surgery in elderly patients. BJS Open 2020, 4, 145–156. [Google Scholar] [CrossRef]
- Bleyer, A.J.; Shemanski, L.R.; Burke, G.L.; Hansen, K.J.; Appel, R.G. Tobacco, hypertension, and vascular disease: Risk factors for renal functional decline in an older population. Kidney Int. 2000, 57, 2072–2079. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.P.; Wai, J.P.M.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.D.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X.F. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Stack, A.G.; Molony, D.A.; Rives, T.; Tyson, J.; Murthy, B.V. Association of physical activity with mortality in the US dialysis population. Am. J. Kidney Dis. 2005, 45, 690–701. [Google Scholar] [CrossRef]
- Robinson, E.S.; Fisher, N.D.; Forman, J.P.; Curhan, G.C. Physical activity and albuminuria. Am. J. Epidemiol. 2010, 171, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Weijs, P.J.; Cynober, L.; DeLegge, M.; Kreymann, G.; Wernerman, J.; Wolfe, R.R. Proteins and amino acids are fundamental to optimal nutrition support in critically ill patients. Crit. Care 2014, 18, 591. [Google Scholar] [CrossRef] [Green Version]
- Weijs, P.J.M.; Looijaard, W.G.P.M.; Beishuizen, A.; Girbes, A.R.J.; Oudemans-van Straaten, H.M. Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients. Crit. Care 2014, 18. [Google Scholar] [CrossRef] [Green Version]
- Allingstrup, M.J.; Esmailzadeh, N.; Knudsen, A.W.; Espersen, K.; Jensen, T.H.; Wiis, J.; Perner, A.; Kondrup, J. Provision of protein and energy in relation to measured requirements in intensive care patients. Clin. Nutr. 2012, 31, 462–468. [Google Scholar] [CrossRef]
- Compher, C.; Chittams, J.; Sammarco, T.; Nicolo, M.; Heyland, D.K. Greater Protein and Energy Intake May Be Associated With Improved Mortality in Higher Risk Critically Ill Patients: A Multicenter, Multinational Observational Study. Crit. Care Med. 2017, 45, 156–163. [Google Scholar] [CrossRef]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.R.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herndon, D.N.; Tompkins, R.G. Support of the metabolic response to burn injury. Lancet 2004, 363, 1895–1902. [Google Scholar] [CrossRef]
- Striker, G.E.; Hirschman, G.H.; Anderson, A.; Edington, B.; Norwood, E.; Klahr, S.; Levey, A.S.; Steinman, T.; Rosa, R.; Johnson, A.; et al. The Modification of Diet in Renal-Disease Study–Design, Methods, and Results from the Feasibility Study. Am. J. Kidney Dis. 1992, 20, 18–33. [Google Scholar]
- Ruggenenti, P.; Perticucci, E.; Cravedi, P.; Gambara, V.; Costantini, M.; Sharma, S.K.; Perna, A.; Remuzzi, G. Role of remission clinics in the longitudinal treatment of CKD. J. Am. Soc. Nephrol. 2008, 19, 1213–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtkamp, F.A.; de Zeeuw, D.; de Graeff, P.A.; Laverman, G.D.; Berl, T.; Remuzzi, G.; Packham, D.; Lewis, J.B.; Parving, H.H.; Lambers Heerspink, H.J. Albuminuria and blood pressure, independent targets for cardioprotective therapy in patients with diabetes and nephropathy: A post hoc analysis of the combined RENAAL and IDNT trials. Eur. Heart J. 2011, 32, 1493–1499. [Google Scholar] [CrossRef]
- Jafar, T.H.; Schmid, C.H.; Landa, M.; Giatras, I.; Toto, R.; Remuzzi, G.; Maschio, G.; Brenner, B.M.; Kamper, A.; Zucchelli, P.; et al. Angiotensin-converting enzyme inhibitors and progression of nondiabetic renal disease. A meta-analysis of patient-level data. Ann. Intern. Med. 2001, 135, 73–87. [Google Scholar] [CrossRef]
- de Zeeuw, D.; Parekh, R.; Soman, S. CKD treatment: Time to alter the focus to albuminuria? Adv. Chronic Kidney Dis. 2011, 18, 222–223. [Google Scholar] [CrossRef]
- Appel, L.J.; Wright, J.T., Jr.; Greene, T.; Agodoa, L.Y.; Astor, B.C.; Bakris, G.L.; Cleveland, W.H.; Charleston, J.; Contreras, G.; Faulkner, M.L.; et al. Intensive blood-pressure control in hypertensive chronic kidney disease. N. Engl. J. Med. 2010, 363, 918–929. [Google Scholar] [CrossRef] [Green Version]
- Kalantar-Zadeh, K.; Kuwae, N.; Regidor, D.L.; Kovesdy, C.P.; Kilpatrick, R.D.; Shinaberger, C.S.; McAllister, C.J.; Budoff, M.J.; Salusky, I.B.; Kopple, J.D. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006, 70, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Block, G.A.; Klassen, P.S.; Lazarus, J.M.; Ofsthun, N.; Lowrie, E.G.; Chertow, G.M. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, T.; Yonemura, K.; Maruyama, Y.; Takahashi, T.; Takita, T.; Furuhashi, M.; Hishida, A. Impact of serum parathyroid hormone concentration and its regulatory factors on arterial stiffness in patients undergoing maintenance hemodialysis. Blood Purif. 2004, 22, 293–297. [Google Scholar] [CrossRef]
- Investigators, E.T.; Chertow, G.M.; Block, G.A.; Correa-Rotter, R.; Drueke, T.B.; Floege, J.; Goodman, W.G.; Herzog, C.A.; Kubo, Y.; London, G.M.; et al. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N. Engl. J. Med. 2012, 367, 2482–2494. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Dickstein, K.; Cohen-Solal, A.; Filippatos, G.; McMurray, J.J.; Ponikowski, P.; Poole-Wilson, P.A.; Stromberg, A.; van Veldhuisen, D.J.; Atar, D.; Hoes, A.W.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur. Heart J. 2008, 29, 2388–2442. [Google Scholar] [CrossRef]
- Tatsumi, E.; Nakatani, T.; Imachi, K.; Umezu, M.; Kyo, S.E.; Sase, K.; Takatani, S.; Matsuda, H. Domestic and foreign trends in the prevalence of heart failure and the necessity of next-generation artificial hearts: A survey by the Working Group on Establishment of Assessment Guidelines for Next-Generation Artificial Heart Systems. J. Artif. Organs 2007, 10, 187–194. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Wald, R. Strategies for the optimal timing to start renal replacement therapy in critically ill patients with acute kidney injury. Kidney Int. 2017, 91, 1022–1032. [Google Scholar] [CrossRef]
- Himmelfarb, J.; Ikizler, T.A. Hemodialysis. N. Engl. J. Med. 2010, 363, 1833–1845. [Google Scholar] [CrossRef]
- Fox, C.S.; Muntner, P.; Chen, A.Y.; Alexander, K.P.; Roe, M.T.; Cannon, C.P.; Saucedo, J.F.; Kontos, M.C.; Wiviott, S.D.; Acute Coronary, T.; et al. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: A report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation 2010, 121, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Gaede, P.; Vedel, P.; Larsen, N.; Jensen, G.V.; Parving, H.H.; Pedersen, O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N. Engl. J. Med. 2003, 348, 383–393. [Google Scholar] [CrossRef] [Green Version]
- Force, Remission Clinic Task; Clinical Research Center “Aldo e Cele Daccò”. The Remission Clinic approach to halt the progression of kidney disease. J. Nephrol. 2011, 24, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Gaede, P.; Lund-Andersen, H.; Parving, H.H.; Pedersen, O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N. Engl. J. Med. 2008, 358, 580–591. [Google Scholar] [CrossRef] [Green Version]
- Zeng, X.; McMahon, G.M.; Brunelli, S.M.; Bates, D.W.; Waikar, S.S. Incidence, outcomes, and comparisons across definitions of AKI in hospitalized individuals. Clin. J. Am. Soc. Nephrol. 2014, 9, 12–20. [Google Scholar] [CrossRef]
- Wu, V.C.; Wu, P.C.; Wu, C.H.; Huang, T.M.; Chang, C.H.; Tsai, P.R.; Ko, W.J.; Chen, L.; Wang, C.Y.; Chu, T.S.; et al. The impact of acute kidney injury on the long-term risk of stroke. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Anzai, A.; Anzai, T.; Naito, K.; Kaneko, H.; Mano, Y.; Jo, Y.; Nagatomo, Y.; Maekawa, Y.; Kawamura, A.; Yoshikawa, T.; et al. Prognostic significance of acute kidney injury after reperfused ST-elevation myocardial infarction: Synergistic acceleration of renal dysfunction and left ventricular remodeling. J. Card Fail. 2010, 16, 381–389. [Google Scholar] [CrossRef]
- Hansen, M.K.; Gammelager, H.; Mikkelsen, M.M.; Hjortdal, V.E.; Layton, J.B.; Johnsen, S.P.; Christiansen, C.F. Post-operative acute kidney injury and five-year risk of death, myocardial infarction, and stroke among elective cardiac surgical patients: A cohort study. Crit. Care 2013, 17, R292. [Google Scholar] [CrossRef] [Green Version]
- Watabe, H.; Sato, A.; Hoshi, T.; Takeyasu, N.; Abe, D.; Akiyama, D.; Kakefuda, Y.; Nishina, H.; Noguchi, Y.; Aonuma, K. Association of contrast-induced acute kidney injury with long-term cardiovascular events in acute coronary syndrome patients with chronic kidney disease undergoing emergent percutaneous coronary intervention. Int. J. Cardiol. 2014, 174, 57–63. [Google Scholar] [CrossRef]
- Kashani, K.; Rosner, M.H.; Haase, M.; Lewington, A.J.P.; O’Donoghue, D.J.; Wilson, F.P.; Nadim, M.K.; Silver, S.A.; Zarbock, A.; Ostermann, M.; et al. Quality Improvement Goals for Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2019, 14, 941–953. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Medication | Application for Cardiovascular and Renal Disease in Chronic Critical Illness |
|---|---|
| Angiotensin II receptor blockers | Reduce albuminuria by at least 50%, reduce systolic blood pressure to less than 140/90 mmHg for general populations and less than 130/80 mmHg for patients with chronic kidney disease and albuminuria |
| Angiotensin receptor-nephrilysin inhibitors | Reduce albuminuria and blood pressure while increasing blood levels of endogenous natriuretic peptides |
| Angiotensin-converting enzyme inhibitors | Reduce albuminuria by at least 50%, reduce systolic blood pressure to less than 140/90 mmHg for general populations and less than 130/80 mmHg for patients with chronic kidney disease and albuminuria |
| Beta-adrenergic receptor blockers | Decrease heart rate, dysrhythmias, and beta-adrenergic receptor overstimulation among patients with chronic left ventricular dysfunction |
| Calcium and vitamin D supplements | Abrogate hypocalcemia among patients with chronic kidney disease and secondary hyperparathyroidism |
| Diuretic therapy | Optimize preload and restore normal interstitial water volumes while maintaining intravascular euvolemia |
| Erythropoietin | Increase hemoglobin levels during critical illness; decrease mortality among critically ill trauma patients |
| Phosphate binders | Abrogate hyperphospatemia among patients with chronic kidney disease and secondary hyperparathyroidism |
| Sodium-glucose contransporter-2 inhibitors | Prevent cardiovascular and renal disease and progression among patients with type 2 diabetes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loftus, T.J.; Filiberto, A.C.; Ozrazgat-Baslanti, T.; Gopal, S.; Bihorac, A. Cardiovascular and Renal Disease in Chronic Critical Illness. J. Clin. Med. 2021, 10, 1601. https://doi.org/10.3390/jcm10081601
Loftus TJ, Filiberto AC, Ozrazgat-Baslanti T, Gopal S, Bihorac A. Cardiovascular and Renal Disease in Chronic Critical Illness. Journal of Clinical Medicine. 2021; 10(8):1601. https://doi.org/10.3390/jcm10081601
Chicago/Turabian StyleLoftus, Tyler J., Amanda C. Filiberto, Tezcan Ozrazgat-Baslanti, Saraswathi Gopal, and Azra Bihorac. 2021. "Cardiovascular and Renal Disease in Chronic Critical Illness" Journal of Clinical Medicine 10, no. 8: 1601. https://doi.org/10.3390/jcm10081601
APA StyleLoftus, T. J., Filiberto, A. C., Ozrazgat-Baslanti, T., Gopal, S., & Bihorac, A. (2021). Cardiovascular and Renal Disease in Chronic Critical Illness. Journal of Clinical Medicine, 10(8), 1601. https://doi.org/10.3390/jcm10081601