
Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
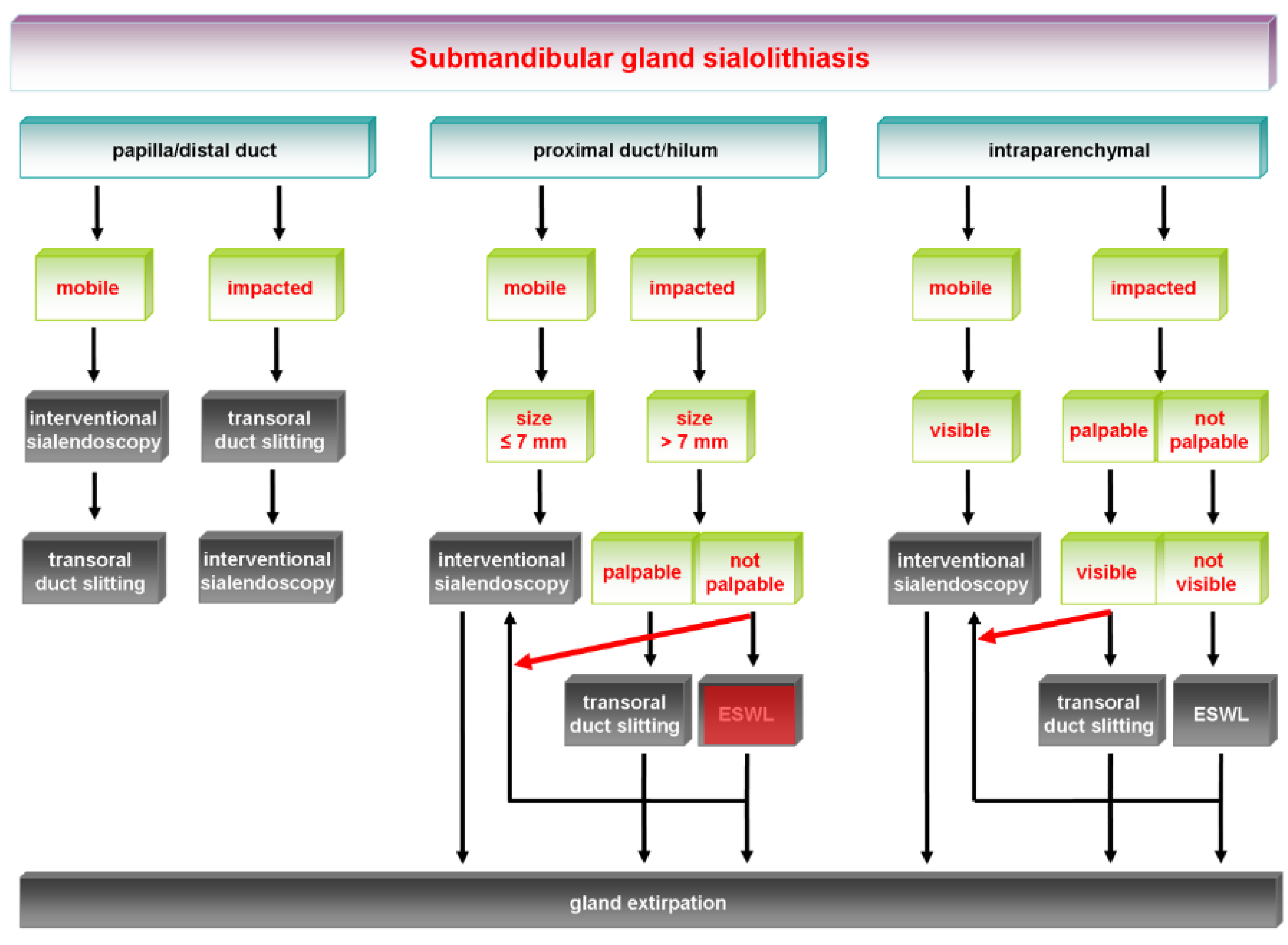
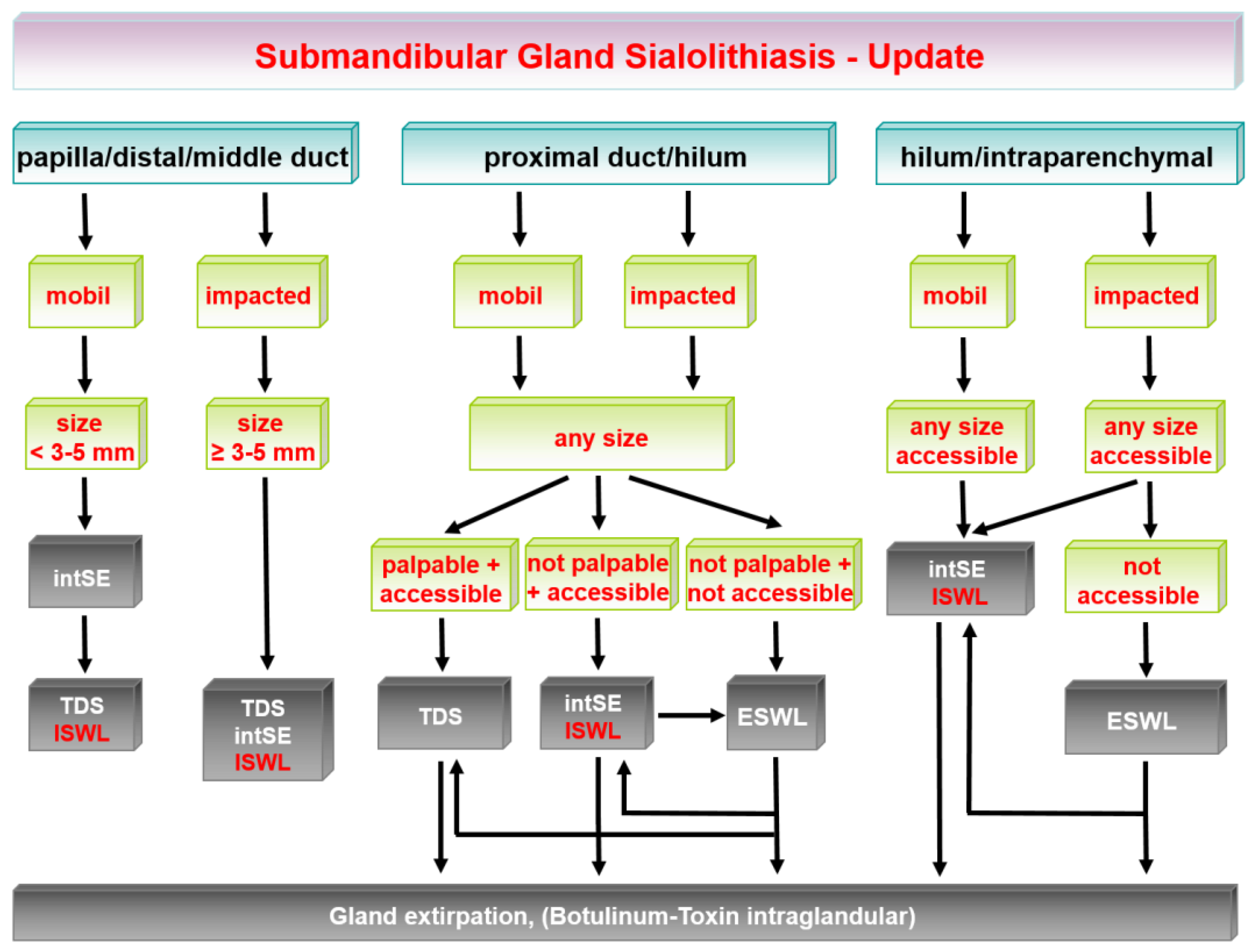
2. Updated Treatment Algorithm for Submandibular Gland Stones
2.1. Stones at the Papilla and in the Distal and Middle Duct
2.2. Stones in the Proximal to Hilar Duct System
2.3. Posthilar to Intraparenchymal Stones
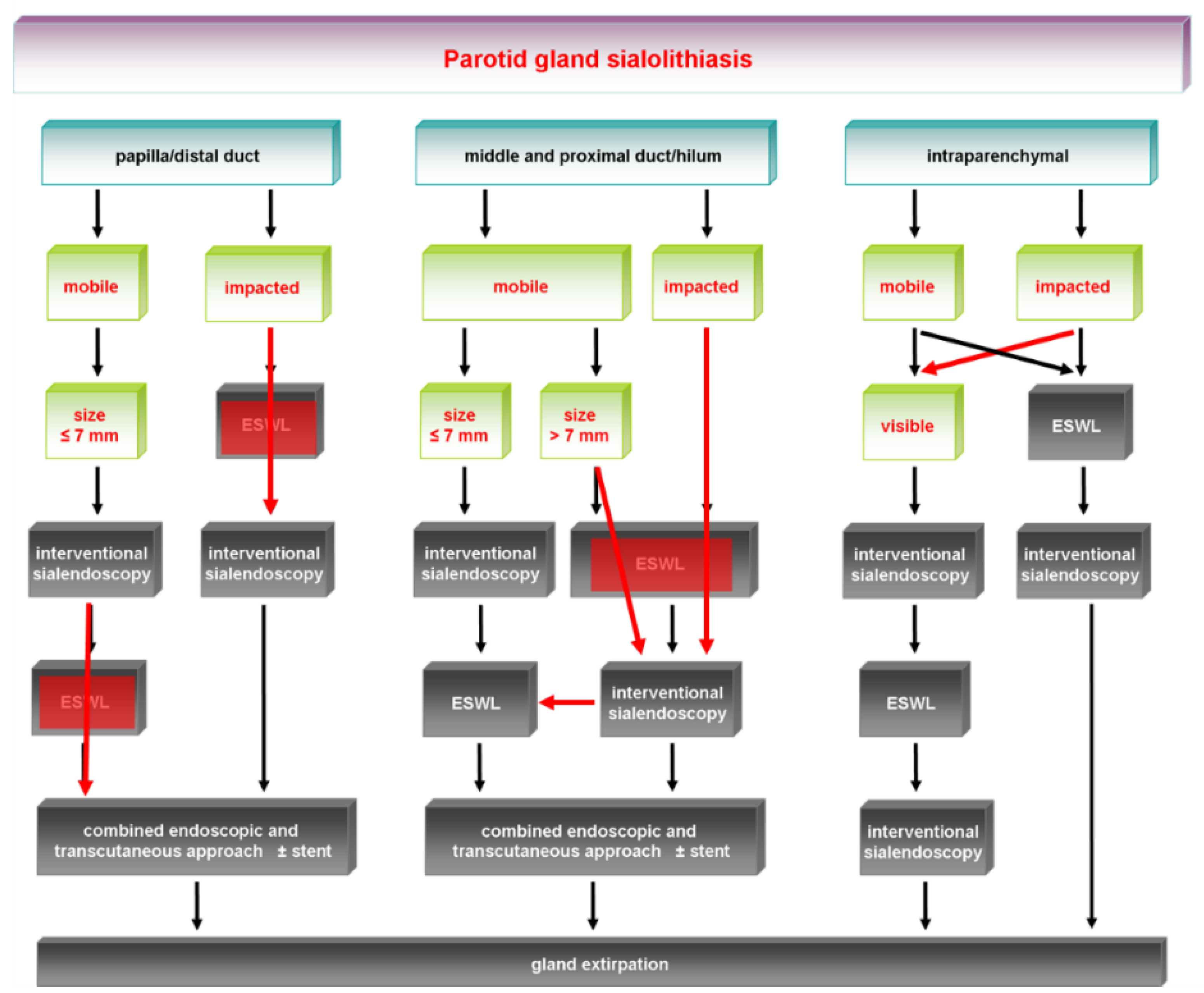
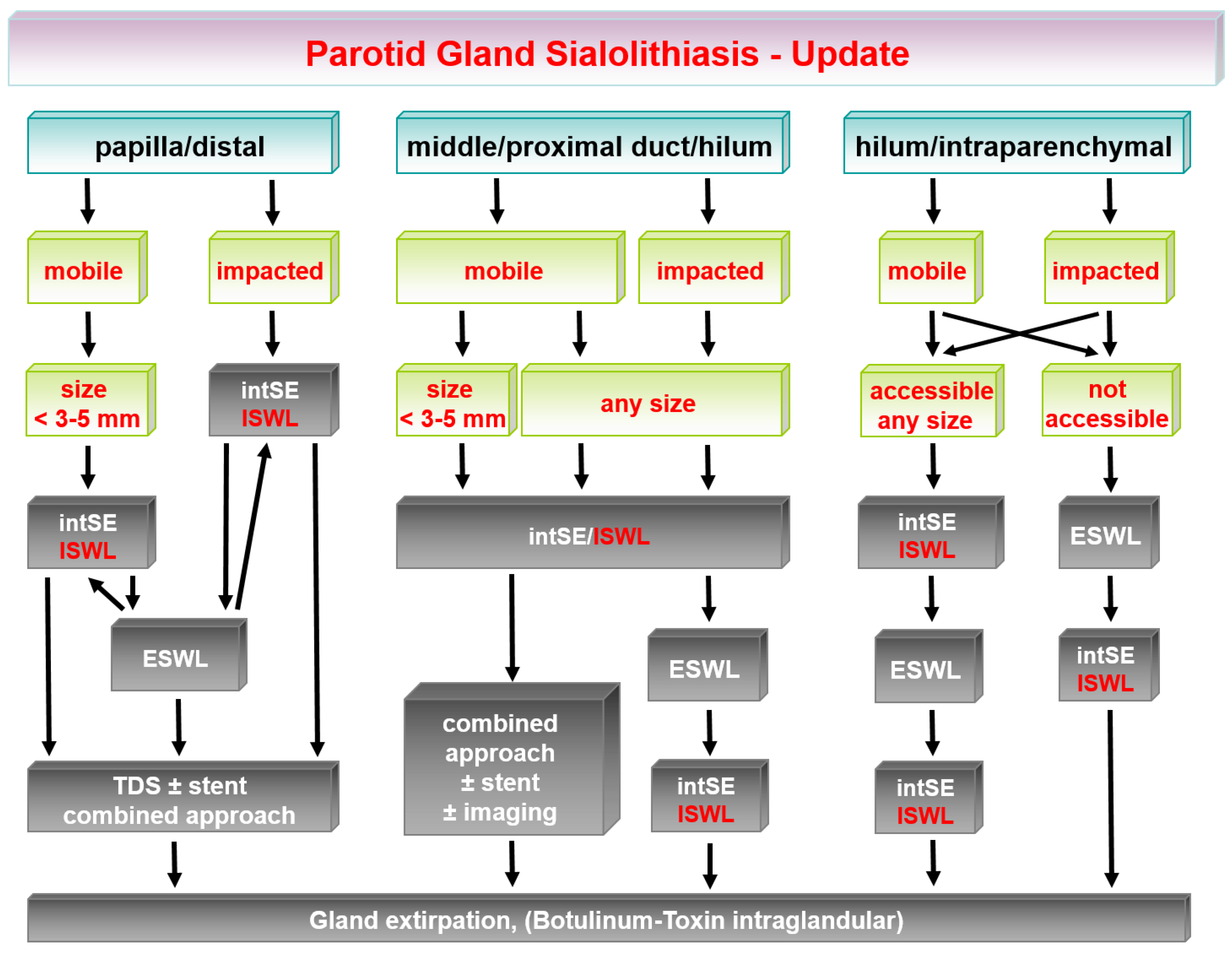
3. Updated Treatment Algorithm for Parotid Gland Stones
3.1. Stones in the Papilla and Distal Excretory Duct
3.2. Stones in the Middle or Proximal Duct and Hilar Region
3.3. Hilar to Intraparenchymal Stones
4. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Capaccio, P.; Torretta, S.; Pignataro, L.; Koch, M. Salivary lithotripsy in the era of sialendoscopy. Acta Otorhinolaryngol. Ital. 2017, 37, 113–121. [Google Scholar]
- Sigismund, P.E.; Zenk, J.; Koch, M.; Schapher, M.; Rudes, M.; Iro, H. Nearly 3000 salivary stones: Some clinical and epidemiologic aspects. Laryngoscope 2015, 125, 1879–1882. [Google Scholar] [CrossRef]
- McGurk, M.; Makdissi, J.; Brown, J. Intra-oral removal of stones from the hilum of the submandibular gland: Report of technique and morbidity. Int. J. Oral Maxillofac. Surg. 2004, 33, 683–686. [Google Scholar] [CrossRef]
- Zenk, J.; Gottwald, F.; Bozzato, A.; Iro, H. Submandibular sialoliths. Stone removal with organ preservation. HNO 2005, 53, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Capaccio, P.; Torretta, S.; Ottavian, F.; Sambataro, G.; Pignataro, L. Modern management of obstructive salivary diseases. Acta Otorhinolaryngol. Ital. 2007, 27, 161–172. [Google Scholar]
- Iro, H.; Benzel, W.; Zenk, J.; Schneider, T.; Waldfahrer, F.; Ell, C. Extracorporeal Shock Wave Lithotripsy of Parotid Stones. Ann. Otol. Rhinol. Laryngol. 1998, 107, 860–864. [Google Scholar] [CrossRef]
- Capaccio, P.; Ottaviani, F.; Manzo, R.; Schindler, A.; Cesana, B. Extracorporeal Lithotripsy for Salivary Calculi: A Long-Term Clinical Experience. Laryngoscope 2004, 114, 1069–1073. [Google Scholar] [CrossRef]
- Escudier, M.P.; Brown, J.; Drage, N.; McGurk, M. Extracorporeal shockwave lithotripsy in the management of salivary calculi. BJS 2003, 90, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Zenk, J.; Bozzato, A.; Gottwald, F.; Winter, M.; Iro, H. Extracorporeal Shock Wave Lithotripsy of Submandibular Stones: Evaluation after 10 Years. Ann. Otol. Rhinol. Laryngol. 2004, 113, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Katz, P. New techniques for the treatment of salivary lithiasis: Sialoendoscopy and extracorporal lithotripsy: 1773 cases. Ann. Otolaryngol. Chir. Cervicofac 2004, 121, 123–132. [Google Scholar] [CrossRef]
- Marchal, F.; Dulguerov, P.; Becker, M.; Barki, G.; Disant, F.; Lehmann, W. Specificity of Parotid Sialendoscopy. Laryngoscope 2001, 111, 264–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchal, F.; Barki, G.; Dulguerov, P.; Disant, F.; Becker, M.; Lehmann, W. Submandibular diagnostic and interventional sialendoscopy: New procedure for ductal disorders. Ann. Otol. Rhinol. Laryngol. 2002, 111, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahlieli, O.; Shacham, R.; Bar, T.; Eliav, E. Endoscopic mechanical retrieval of sialoliths. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 95, 396–402. [Google Scholar] [CrossRef]
- Koch, M.; Zenk, J.; Iro, H. Diagnostic and interventional sialoscopy in obstructive diseases of the salivary glands. HNO 2008, 56, 139–144. [Google Scholar] [CrossRef]
- Capaccio, P.; Torretta, S.; Pignataro, L. The Role of Adenectomy for Salivary Gland Obstructions in the Era of Sialendoscopy and Lithotripsy. Otolaryngol. Clin. N. Am. 2009, 42, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Iro, H.; Zenk, J.; Escudier, M. Outcome of minimally invasive management of salivary calculi in 4691 patients. Laryngoscope 2009, 119, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Ryan, W.R.; Ba, K.A.P.; Gurman, Z.R.; Aubin-Pouliot, A.; Chang, J.L. One-Year symptom outcomes after sialolithiasis treatment with sialendoscopy-assisted salivary duct surgery. Laryngoscope 2019, 129, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Nahlieli, O.; London, D.; Zagury, A.; Eliav, E. Combined approach to impacted parotid stones. J. Oral Maxillofac. Surg. 2002, 60, 1418–1423. [Google Scholar] [CrossRef]
- McGurk, M.; MacBean, A.; Fan, K.; Sproat, C.; Darwish, C. Endoscopically assisted operative retrieval of parotid stones. Br. J. Oral Maxillofac. Surg. 2006, 44, 157–160. [Google Scholar] [CrossRef]
- Marchal, F. A Combined Endoscopic and External Approach for Extraction of Large Stones with Preservation of Parotid and Submandibular Glands. Laryngoscope 2007, 117, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Marchal, F.; Dulguerov, P. Sialolithiasis management: The state of the art. Arch. Otolaryngol.-Head Neck Surg. 2003, 129, 951–956. [Google Scholar] [CrossRef] [Green Version]
- McGurk, M.; Escudier, M.P.; Brown, J. Modern management of salivary calculi. Br. J. Surg. 2004, 92, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Luers, J.C.; Grosheva, M.; Reifferscheid, V.; Stenner, M.; Beutner, D. Sialendoscopy for sialolithiasis: Early treatment, better outcome. Head Neck 2012, 34, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, M.; Schapher, M.; Iro, H.; Wuest, W.; Mantsopoulos, K.; Koch, M. Value of Sonography in the Diagnosis of Sialolithiasis: Comparison with the Reference Standard of Direct Stone Identification. J. Ultrasound Med. 2017, 36, 2227–2235. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, M.; Mantsopoulos, K.; Schapher, M.L.; Zenk, J.; Bozzato, A.; Kuenzel, J.; Zengel, P.; Iro, H.; Koch, M. Interrater Reliability of Ultrasound in the Diagnosis of Sialolithiasis. Ultraschall Med.-Eur. J. Ultrasound 2019, 40, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Zenk, J.; Iro, H. Algorithms for Treatment of Salivary Gland Obstructions. Otolaryngol. Clin. N. Am. 2009, 42, 1173–1192. [Google Scholar] [CrossRef]
- Fritsch, M.H. Algorithms for Treatment of Salivary Gland Obstructions without Access to Extracorporeal Lithotripsy. Otolaryngol. Clin. N. Am. 2009, 42, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Lommen, J.; Schorn, L.; Roth, B.; Naujoks, C.; Handschel, J.; Holtmann, H.; Kübler, N.R.; Sproll, C. Sialolithiasis: Retrospective analysis of the effect of an escalating treatment algorithm on patient-perceived health-related quality of life. Head Face Med. 2021, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Bozzato, A.; Iro, H.; Zenk, J. Combined Endoscopic and Transcutaneous Approach for Parotid Gland Sialolithiasis: Indications, Technique, and Results. Otolaryngol.-Head Neck Surg. 2010, 142, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Eun, Y.G.; Chung, D.H.; Kwon, K.H. Advantages of intraoral removal over submandibular gland resection for proximal submandibular stones: A prospective randomized study. Laryngoscope 2010, 120, 2189–2192. [Google Scholar] [CrossRef]
- Capaccio, P.; Clemente, I.A.; McGurk, M.; Bossi, A.; Pignataro, L. Transoral removal of hiloparenchymal submandibular calculi: A long-term clinical experience. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1081–1086. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, J.W.; Lee, Y.M.; Oh, C.W.; Chang, H.S.; Lee, S.W. Long-term Study of Sialodochoplasty for Preventing Submandibular Sialolithiasis Recurrence. Clin. Exp. Otorhinolaryngol. 2012, 5, 34–38. [Google Scholar] [CrossRef]
- Kim, J.; Shin, S.; Lee, H.; Lee, S. Factors affecting long-term outcome of transoral surgery for submandibular stones: A follow-up study of 125 patients. Clin. Otolaryngol. 2016, 41, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Schapher, M.; Mantsopoulos, K.; Messbacher, M.-E.; Iro, H.; Koch, M. Transoral submandibulotomy for deep hilar submandibular gland sialolithiasis. Laryngoscope 2017, 127, 2038–2044. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Zhao, J.; Hze-Khoong, E.P.; Liu, S.; Yin, X.; Hu, Y. A gland-sparing, intraoral sialolithotomy approach for hilar and intraparenchymal multiple stones in the submandibular gland. Sci. Rep. 2020, 10, 8495. [Google Scholar] [CrossRef]
- Zhao, Y.N.; Zhang, Y.Q.; Zhang, L.Q.; Xie, X.Y.; Liu, D.G.; Yu, G.Y. Treatment strategy of hilar and intraglandular stones in wharton’s duct: A 12-year experience. Laryngoscope 2020, 130, 2360–2365. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.-G.; Jiang, L.; Xie, X.-Y.; Zhang, Z.-Y.; Zhang, L.; Yu, G.-Y. Sialoendoscopy-Assisted Sialolithectomy for Submandibular Hilar Calculi. J. Oral Maxillofac. Surg. 2013, 71, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, N.; Hazkani, I.; Goshen, S. Combined approach sialendoscopy for management of submandibular gland sialolithiasis. Am. J. Otolaryngol. 2015, 36, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.-Q.; Sun, H.-J.; Qiao, Q.-H.; Bao, X.; Wu, C.-B.; Zhou, Q. Evaluation of Sialendoscopy-Assisted Treatment of Submandibular Gland Stones. J. Oral Maxillofac. Surg. 2017, 75, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Capaccio, P.; Gaffuri, M.; Rossi, V.; Pignataro, L. Sialendoscope-assisted transoral removal of hilo-parenchymal sub-mandibular stones: Surgical results and subjective scores. Acta Otorhinolaryngol. Ital. 2017, 37, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Sproll, C.; Naujoks, C.; Holtmann, H.; Kübler, N.R.; Singh, D.D.; Rana, M.; Lommen, J. Removal of stones from the superficial lobe of the submandibular gland (SMG) via an intraoral endoscopy-assisted sialolithotomy. Clin. Oral Investig. 2019, 23, 4145–4156. [Google Scholar] [CrossRef] [PubMed]
- Razavi, C.; Pascheles, C.; Samara, G.; Marzouk, M. Robot-assisted sialolithotomy with sialendoscopy for the management of large submandibular gland stones. Laryngoscope 2015, 126, 345–351. [Google Scholar] [CrossRef]
- Capaccio, P.; Montevecchi, F.; Meccariello, G.; D’Agostino, G.; Cammaroto, G.; Pelucchi, S.; Vicini, C. Transoral robotic surgery for hilo-parenchymal submandibular stones: Step-by-step description and reasoned approach. Int. J. Oral Maxillofac. Surg. 2019, 48, 1520–1524. [Google Scholar] [CrossRef]
- Tampio, A.J.F.; Marzouk, M.F. Robot-assisted sialolithotomy with sialoendoscopy: A review of safety, efficacy and cost. J. Robot. Surg. 2021, 15, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Frost, A.S.; Byrnes, Y.M.; Wen, C.Z.; Rassekh, C.H. Single-port transoral robotic combined approach with sialendoscopy for sialolithiasis: Case report and review of the literature. Head Neck 2020, 42, E12–E15. [Google Scholar] [CrossRef] [PubMed]
- Vergez, S.; Cheval, M.; Chabrillac, E. Transoral robotic removal of submandibular sialolith combined with sialendoscopic assistance. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138 (Suppl. 2), 65–66. [Google Scholar] [CrossRef] [PubMed]
- Anicin, A.; Urbancic, J. Sialendoscopy and CT navigation assistance in the surgery of sialolithiasis. Radiol. Oncol. 2021, 55, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Capaccio, P.; Torretta, S.; Pignataro, L. Extracorporeal Lithotripsy Techniques for Salivary Stones. Otolaryngol. Clin. N. Am. 2009, 42, 1139–1159. [Google Scholar] [CrossRef] [PubMed]
- Escudier, M.P.; Brown, J.E.; Putcha, V.; Capaccio, P.; McGurk, M. Factors influencing the outcome of extracorporeal shock wave lithotripsy in the management of salivary calculi. Laryngoscope 2010, 120, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Guerre, A.; Katz, P. Extracorporeal shockwave lithotripsy (ESWL) for salivary gland stones: A retrospective study of 1571 patients. Rev. Stomatol. Chir. Maxillo-Faciale 2011, 112, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Zenk, J.; Koch, M.; Klintworth, N.; König, B.; Konz, K.; Gillespie, M.B.; Iro, H. Sialendoscopy in the diagnosis and treatment of sialolithiasis: A study on more than 1000 patients. Otolaryngol.-Head Neck Surg. 2012, 147, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Desmots, F.; Chossegros, C.; Salles, F.; Gallucci, A.; Moulin, G.; Varoquaux, A. Lithotripsy for salivary stones with prospective US assessment on our first 25 consecutive patients. J. Oral Maxillofac. Surg. 2014, 42, 577–582. [Google Scholar] [CrossRef]
- Nahlieli, O.; Shacham, R.; Zaguri, A. Combined External Lithotripsy and Endoscopic Techniques for Advanced Sialolithiasis Cases. J. Oral Maxillofac. Surg. 2010, 68, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Foletti, J.M.; Chossegros, C.; Salles, F.; Guyot, L. Transoral approach for Stensen’s duct lithiasis. Laryngoscope 2011, 121, 1893–1895. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Xie, L.; Wang, Z.; Shi, H.; Cao, N.; Yu, C. Endoscopic-assisted gland preserving therapy for the management of parotid gland sialolithiasis: Our preliminary experience. J. Cranio-Maxillofac. Surg. 2015, 43, 1650–1654. [Google Scholar] [CrossRef]
- Samani, M.; Hills, A.J.; Holden, A.M.; Man, C.-B.; McGurk, M. Minimally-invasive surgery in the management of symptomatic parotid stones. Br. J. Oral Maxillofac. Surg. 2016, 54, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Zhang, Y.-Q.; Xie, X.-Y.; Liu, D.-G.; Zhang, L.; Yu, G.-Y. Transoral and transcutaneous approach for removal of parotid gland calculi: A 10-year endoscopic experience. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Walvekar, R.R.; Bomeli, S.R.; Carrau, R.L.; Schaitkin, B. Combined approach technique for the management of large salivary stones. Laryngoscope 2009, 119, 1125–1129. [Google Scholar] [CrossRef]
- Overton, A.; Combes, J.; McGurk, M. Outcome after endoscopically assisted surgical retrieval of symptomatic parotid stones. Int. J. Oral Maxillofac. Surg. 2012, 41, 248–251. [Google Scholar] [CrossRef]
- Koch, M.; Iro, H.; Zenk, J. Combined endoscopic–transcutaneous surgery in parotid gland sialolithiasis and other ductal diseases: Reporting medium- to long-term objective and patients′ subjective outcomes. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 1933–1940. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, T.; Szyfter, W.; Wierzbicka, M. Sialoendoscopy and combined approach for the management of salivary gland stones. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 219–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capaccio, P.; Gaffuri, M.; Pignataro, L. Sialendoscopy-assisted transfacial surgical removal of parotid stones. J. Cranio-Maxillo-Facial Surg. 2014, 42, 1964–1969. [Google Scholar] [CrossRef]
- Konstantinidis, I.; Chatziavramidis, A.; Iakovou, I.; Constantinidis, J. Long-term results of combined approach in parotid sialolithiasis. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 3533–3538. [Google Scholar] [CrossRef]
- Numminen, J.; Sillanpää, S.; Virtanen, J.; Sipilä, M.; Rautiainen, M. Retrospective Analysis of a Combined Endoscopic and Transcutaneous Technique for the Management of Parotid Salivary Gland Stones. ORL J. Otorhinolaryngol. Relat. Spec. 2014, 76, 282–287. [Google Scholar] [CrossRef]
- Klein, H.; Ardekian, L. The Treatment of Large Sialoliths by Sialendoscopic Combined Approach. J. Oral Maxillofac. Surg. 2014, 72, 737–743. [Google Scholar] [CrossRef]
- Mikolajczak, S.; Bremke, M.; Beutner, D.; Lüers, J.C. Combined endoscopic and transcutaneous approach for immobile parotid stones. Acta Oto-Laryngol. 2014, 135, 85–89. [Google Scholar] [CrossRef]
- Carroll, W.W.; Walvekar, R.R.; Gillespie, M.B. Transfacial Ultrasound-Guided Gland-Preserving Resection of Parotid Sialoliths. Otolaryngol.-Head Neck Surg. 2012, 148, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.S.; Sood, A.J. Ultrasound-Guided Needle Localization during Open Parotid Sialolithotomy. Otolaryngol.-Head Neck Surg. 2014, 151, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Capaccio, P.; Bresciani, L.; Di Pasquale, D.; Gaffuri, M.; Torretta, S.; Pignataro, L. CT Navigation and sialendoscopy-assisted transfacial removal of a parotid stone: A technical note. Laryngoscope 2019, 129, 2295–2298. [Google Scholar] [CrossRef] [PubMed]
- Witt, R.L.; Iro, H.; Koch, M.; McGurk, M.; Nahlieli, O.; Zenk, J. Minimally invasive options for salivary calculi. Laryngoscope 2012, 122, 1306–1311. [Google Scholar] [CrossRef] [PubMed]
- Strychowsky, J.E.; Sommer, D.D.; Gupta, M.K.; Cohen, N.; Nahlieli, O. Sialendoscopy for the management of obstructive salivary gland disease: A systematic review and meta-analysis. Arch. Otolaryngol.—Head Neck Surg. 2012, 138, 541–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foletti, J.M.; Graillon, N.; Avignon, S.; Guyot, L.; Chossegros, C. Salivary Calculi Removal by Minimally Invasive Techniques: A Decision Tree Based on the Diameter of the Calculi and Their Position in the Excretory Duct. J. Oral Maxillofac. Surg. 2018, 76, 112–118. [Google Scholar] [CrossRef]
- Zenk, J.; Hosemann, W.G.; Iro, H. Diameters of the main excretory ducts of the adult human submandibular and parotid gland: A histologic study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 576–580. [Google Scholar] [CrossRef]
- Marchal, F.; Dulguerov, P.; Lehmann, W. Interventional Sialendoscopy. N. Engl. J. Med. 1999, 341, 1242–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchal, F.; Becker, M.; Dulguerov, P.; Lehmann, W. Interventional Sialendoscopy. Laryngoscope 2000, 110, 318. [Google Scholar] [CrossRef] [Green Version]
- Zenk, J.; Koch, M.; Bozzato, A.; Iro, H. Sialoscopy—initial experiences with a new endoscope. Br. J. Oral Maxillofac. Surg. 2004, 42, 293–298. [Google Scholar] [CrossRef]
- Koch, M.; Zenk, J.; Bozzato, A.; Bumm, K.; Iro, H. Sialoscopy in Cases of Unclear Swelling of the Major Salivary Glands. Otolaryngol.-Head Neck Surg. 2005, 133, 863–868. [Google Scholar] [CrossRef]
- Zenk, J.; Koch, M.; Iro, H. Extracorporeal and Intracorporeal Lithotripsy of Salivary Gland Stones: Basic Investigations. Otolaryngol. Clin. N. Am. 2009, 42, 1115–1137. [Google Scholar] [CrossRef]
- Königsberger, R.; Feyh, J.; Goetz, A.; Kastenbauer, E. Endoscopically-controlled electrohydraulic intracorporeal shock wave lithotripsy (EISL) of salivary stones. J. Otolaryngol. 1993, 22, 12–13. [Google Scholar]
- Iro, H.; Zenk, J.; Hosemann, W.G.; Benzel, W. Electrohydraulic intracorporeal lithotripsy of salivary calculi. In vitro and animal experiment studies. HNO 1993, 41, 389–395. [Google Scholar]
- Iro, H.; Benzel, W.; Göde, U.; Zenk, J. Pneumatic intracorporeal lithotripsy of salivary calculi. In vitro and animal experiment studies. HNO 1995, 43, 172–176. [Google Scholar] [PubMed]
- Bayar, N.; Kaymaz, F.; Apan, A.; Yilmaz, E.; Çakar, A. Effects of electrohydraulic extracorporeal shock wave lithotripsy on submandibular gland in the rat: Electron microscopic evaluation. Int. J. Pediatr. Otorhinolaryngol. 2002, 63, 223–233. [Google Scholar] [CrossRef]
- Nakayama, E.; Okamura, K.; Mitsuyasu, T.; Kawazu, T.; Nakamura, N.; Nakamura, S.; Yoshiura, K. A Newly Developed Interventional Sialendoscope for a Completely Nonsurgical Sialolithectomy Using Intracorporeal Electrohydraulic Lithotripsy. J. Oral Maxillofac. Surg. 2007, 65, 1402–1405. [Google Scholar] [CrossRef] [PubMed]
- Modayil, P.C.; Jacob, V.; Manjaly, G.; Watson, G. Intracorporeal electrokinetic lithotripsy: An advancement in minimally invasive management of parotid duct calculus. J. Laryngol. Otol. 2008, 122, 428–431. [Google Scholar] [CrossRef]
- Konigsberger, R.; Feyh, J.; Goetz, A.; Schilling, V.; Kastenbauer, E. Endoscopic controlled laser lithotripsy in the treatment of sialolithiasis. Laryngo-Rhino-Otologie 1990, 69, 322–323. [Google Scholar]
- Gundlach, P.; Scherer, H.; Hopf, J.; Leege, N.; Müller, G.; Hirst, L.; Scholz, C. Endoscopic-controlled laser lithotripsy of salivary calculi. In vitro studies and initial clinical use. HNO 1990, 38, 247–250. [Google Scholar] [PubMed]
- Iro, H.; Zenk, J.; Benzel, W. Laser Lithotripsy of Salivary Duct Stones. Adv. Otorhinolaryngol. 1995, 49, 148–152. [Google Scholar] [CrossRef]
- Ito, H.; Baba, S. Pulsed dye laser lithotripsy of submandibular gland salivary calculus. J. Laryngol. Otol. 1996, 110, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Arzoz, E.; Santiago, A.; Esnal, F.; Palomero, R. Endoscopic intracorporeal lithotripsy for sialolithiasis. J. Oral Maxillofac. Surg. 1996, 54, 847–850. [Google Scholar] [CrossRef]
- Chu, D.; Chow, T.-L.; Lim, B.-H.; Kwok, S.-Y. Endoscopic management of submandibular sialolithiasis. Surg. Endosc. 2003, 17, 876–879. [Google Scholar] [CrossRef]
- Raif, J.; Vardi, M.; Nahlieli, O.; Gannot, I. An Er:YAG laser endoscopic fiber delivery system for lithotripsy of salivary stones. Lasers Surg. Med. 2006, 38, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Angiero, F.; Benedicenti, S.; Romanos, G.E.; Crippa, R. Sialolithiasis of the Submandibular Salivary Gland Treated with the 810- to 830-nm Diode Laser. Photomed. Laser Surg. 2008, 26, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.E.; McCain, J.P.; Kim, K.; Katz, R.L.; Kaban, L.B.; Troulis, M.J. Interventional Sialoendoscopy: Early Clinical Results. J. Oral Maxillofac. Surg. 2008, 66, 954–962. [Google Scholar] [CrossRef]
- Chiesa-Estomba, C.M.; Saga-Gutierrez, C.; Calvo-Henriquez, C.; Lechien, J.R.; Cartier, C.; Mayo-Yanez, M.; Larruscain-Sarasola, E.; Ayad, T.; Walvekar, R.R. Laser-Assisted Lithotripsy with Sialendoscopy: Systematic Review of YO-IFOS Head and Neck Study Group. Ear Nose Throat J. 2021, 100, 42S–50S. [Google Scholar] [CrossRef]
- Durbec, M.; Dinkel, E.; Vigier, S.; Disant, F.; Marchal, F.; Faure, F. Thulium-YAG laser sialendoscopy for parotid and submandibular sialolithiasis. Lasers Surg. Med. 2012, 44, 783–786. [Google Scholar] [CrossRef]
- Schrötzlmair, F.; Müller, M.; Pongratz, T.; Eder, M.; Johnson, T.; Vogeser, M.; von Holzschuher, V.; Zengel, P.; Sroka, R. Laser lithotripsy of salivary stones: Correlation with physical and radiological parameters. Lasers Surg. Med. 2015, 47, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Martellucci, S.; Gallo, A.; Pagliuca, G.; De Vincentiis, M.; Gallipoli, C.; Rosato, C.; Benedetti, F.N. Ho:Yag laser for sialolithiasis of Wharton’s duct. Otolaryngol.-Head Neck Surg. 2013, 148, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.; Withrow, K. Outcomes of Holmium Laser–Assisted Lithotripsy with Sialendoscopy in Treatment of Sialolithiasis. Otolaryngol.-Head Neck Surg. 2014, 150, 962–967. [Google Scholar] [CrossRef]
- Sionis, S.; Caria, R.; Trucas, M.; Brennan, P.; Puxeddu, R. Sialoendoscopy with and without holmium:YAG laser-assisted lithotripsy in the management of obstructive sialadenitis of major salivary glands. Br. J. Oral Maxillofac. Surg. 2014, 52, 58–62. [Google Scholar] [CrossRef]
- Sun, Y.-T.; Lee, K.-S.; Hung, S.-H.; Su, C.-H. Sialendoscopy With Holmium:YAG Laser Treatment for Multiple Large Sialolithiases of the Wharton Duct: A Case Report and Literature Review. J. Oral Maxillofac. Surg. 2014, 72, 2491–2496. [Google Scholar] [CrossRef]
- Su, C.H.; Lee, K.S.; Tseng, T.M.; Hung, S.H. Endoscopic Holmium: YAG laser-assisted lithotripsy: A Preliminary Report. B-ENT 2015, 11, 57–61. [Google Scholar]
- Guenzel, T.; Hoch, S.; Heinze, N.; Wilhelm, T.; Gueldner, C.; Franzen, A.; Coordes, A.; Lieder, A.; Wiegand, S. Sialendoscopy plus laser lithotripsy in sialolithiasis of the submandibular gland in 64 patients: A simple and safe procedure. Auris Nasus Larynx 2019, 46, 797–802. [Google Scholar] [CrossRef]
- Koch, M.; Hung, S.-H.; Su, C.-H.; Lee, K.-S.; Iro, H.; Mantsopoulos, K. Intraductal lithotripsy in sialolithiasis with two different Ho:YAG lasers: Presetting parameters, effectiveness, success rates. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 5548–5557. [Google Scholar]
- Koch, M.; Schapher, M.; Mantsopoulos, K.; Iro, H. Intraductal Lithotripsy in Sialolithiasis Using the Calculase III™ Ho:YAG Laser: First Experiences. Lasers Surg. Med. 2020, 53, 488–498. [Google Scholar] [CrossRef]
- Koch, M.; Mantsopoulos, K.; Schapher, M.; Von Scotti, F.; Iro, H. Intraductal pneumatic lithotripsy for salivary stones with the StoneBreaker: Preliminary experience. Laryngoscope 2016, 126, 1545–1550. [Google Scholar] [CrossRef]
- Serbetci, E.; Celikoyar, M.M.; Altundag, A. Sialendoscopic Pneumatic Lithotripsy for Salivary Calculi: A New Technique and a Long-term Clinical Experience. Otolaryngol.-Head Neck Surg. 2017, 157, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Schapher, M.; Sievert, M.; Mantsopoulos, K.; Iro, H. Intraductal Fragmentation in Sialolithiasis Using Pneumatic Lithotripsy: Initial Experience and Results. Otolaryngol.-Head Neck Surg. 2021, 2021. [Google Scholar] [CrossRef]
- Ozdemir, S. Outcomes of Pneumatic Lithotripsy Versus Holmium Laser-Assisted Lithotripsy with Sialendoscopy in Management of Submandibular Sialolithiasis. J. Craniofac. Surg. 2020, 31, 1974–1977. [Google Scholar] [CrossRef]
- Koch, M.; Schapher, M.; Mantsopoulos, K.; Von Scotti, F.; Goncalves, M.; Iro, H. Multimodal treatment in difficult sialolithiasis: Role of extracorporeal shock-wave lithotripsy and intraductal pneumatic lithotripsy. Laryngoscope 2018, 128, E332–E338. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Schapher, M.; Mantsopoulos, K.; Goncalves, M.; Iro, H. Intraductal Pneumatic Lithotripsy after Extended Transoral Duct Surgery in Submandibular Sialolithiasis. Otolaryngol.-Head Neck Surg. 2018, 160, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Schapher, M.L.; Mantsopoulos, K.; Goncalves, M.; Iro, H. Simultaneous Application of Ultrasound and Sialendoscopy and its Value in the Management of Sialolithiasis. Ultraschall Med. 2020. [Google Scholar] [CrossRef]
- Nguyen Hong, L. Ultrasound-Guided Sialendoscopy with Holmium: Yttrium Aluminum Garnet (YAG) Laser Treatment of Parotid Sialolithiasis. Am. J. Case Rep. 2021, 22, e929883. [Google Scholar] [CrossRef] [PubMed]
- Geisthoff, U.W.; Lehnert, B.K.; Verse, T. Ultrasound-guided mechanical intraductal stone fragmentation and removal for sialolithiasis: A new technique. Surg. Endosc. 2006, 20, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Liang, L.; Shao, X.; Han, X. Trans-Oral Robotic Surgery of Submandibular Gland Removal with Preservation of Sublingual Gland and Wharton’s Duct. J. Craniofac. Surg. 2019, 30, 237–238. [Google Scholar] [CrossRef]
- Capaccio, P.; Montevecchi, F.; Meccariello, G.; Cammaroto, G.; Magnuson, J.S.; Pelucchi, S.; Bresciani, L.; Vicini, C. Transoral robotic submandibular sialadenectomy: How and when. Gland. Surg. 2020, 9, 423–429. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, M.; Mantsopoulos, K.; Müller, S.; Sievert, M.; Iro, H. Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature. J. Clin. Med. 2022, 11, 231. https://doi.org/10.3390/jcm11010231
Koch M, Mantsopoulos K, Müller S, Sievert M, Iro H. Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature. Journal of Clinical Medicine. 2022; 11(1):231. https://doi.org/10.3390/jcm11010231
Chicago/Turabian StyleKoch, Michael, Konstantinos Mantsopoulos, Sarina Müller, Matti Sievert, and Heinrich Iro. 2022. "Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature" Journal of Clinical Medicine 11, no. 1: 231. https://doi.org/10.3390/jcm11010231
APA StyleKoch, M., Mantsopoulos, K., Müller, S., Sievert, M., & Iro, H. (2022). Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature. Journal of Clinical Medicine, 11(1), 231. https://doi.org/10.3390/jcm11010231