
Lung Aeration in COVID-19 Pneumonia by Ultrasonography and Computed Tomography

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Demographic, Clinical, and Laboratory Data
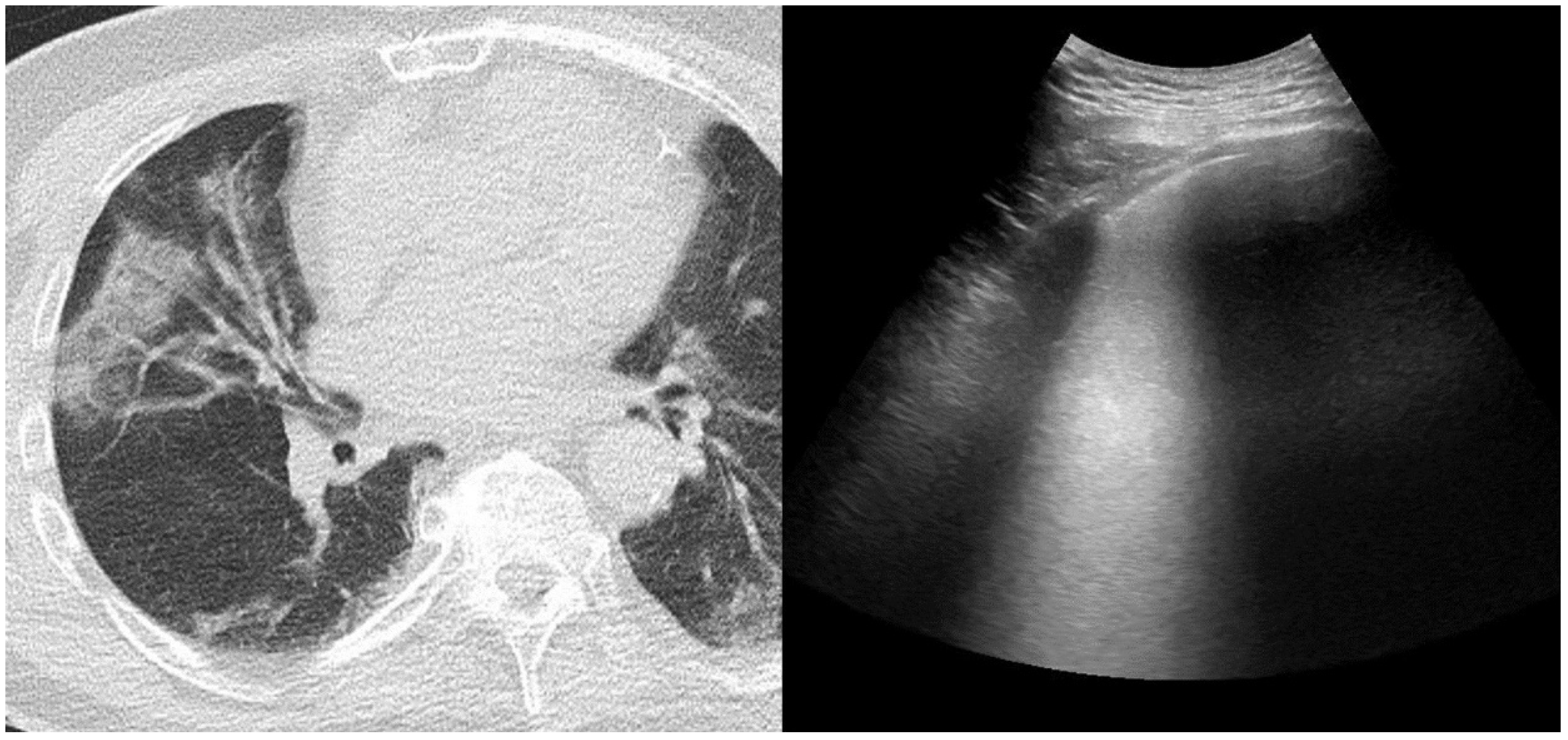
2.3. Chest Computed Tomography and Score Assessment
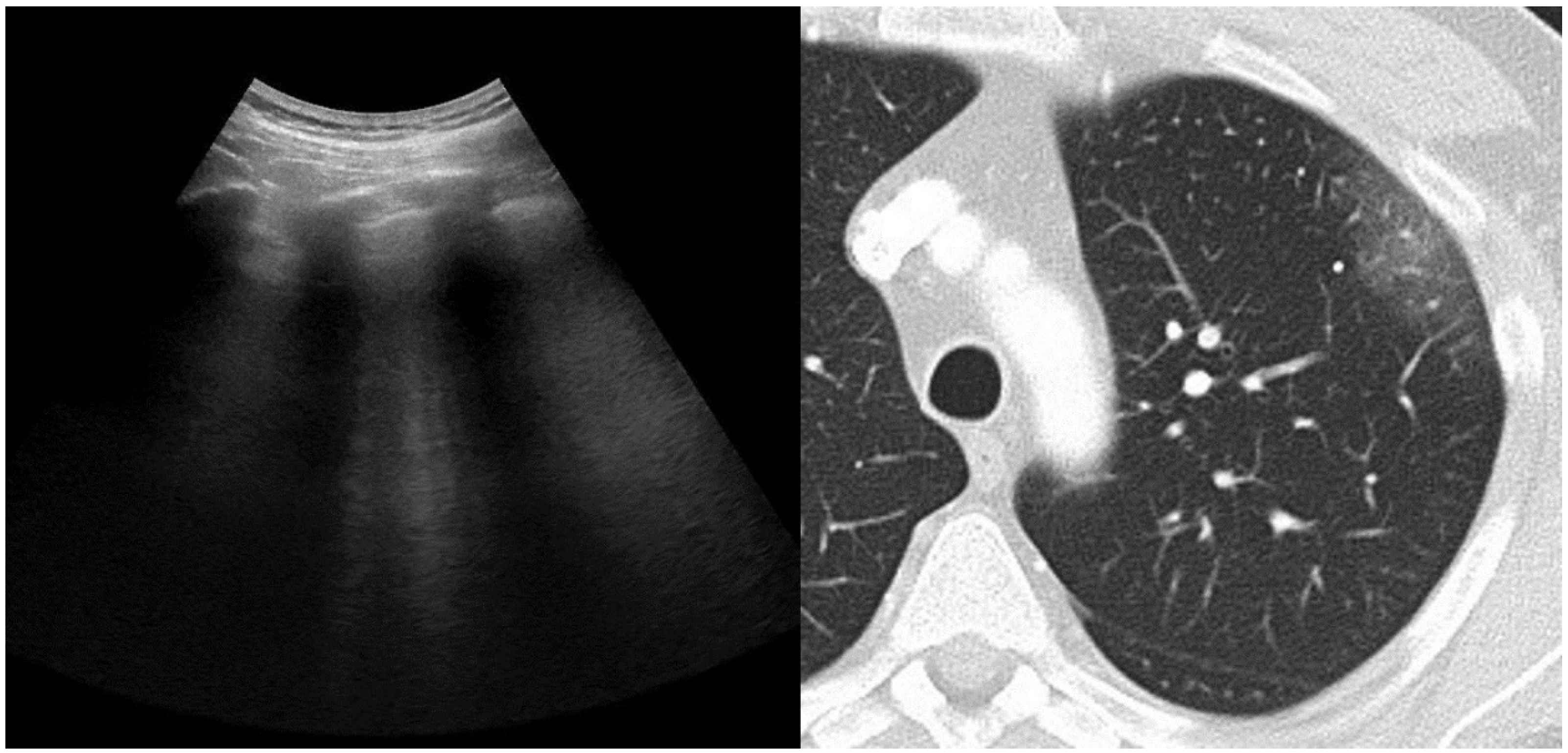
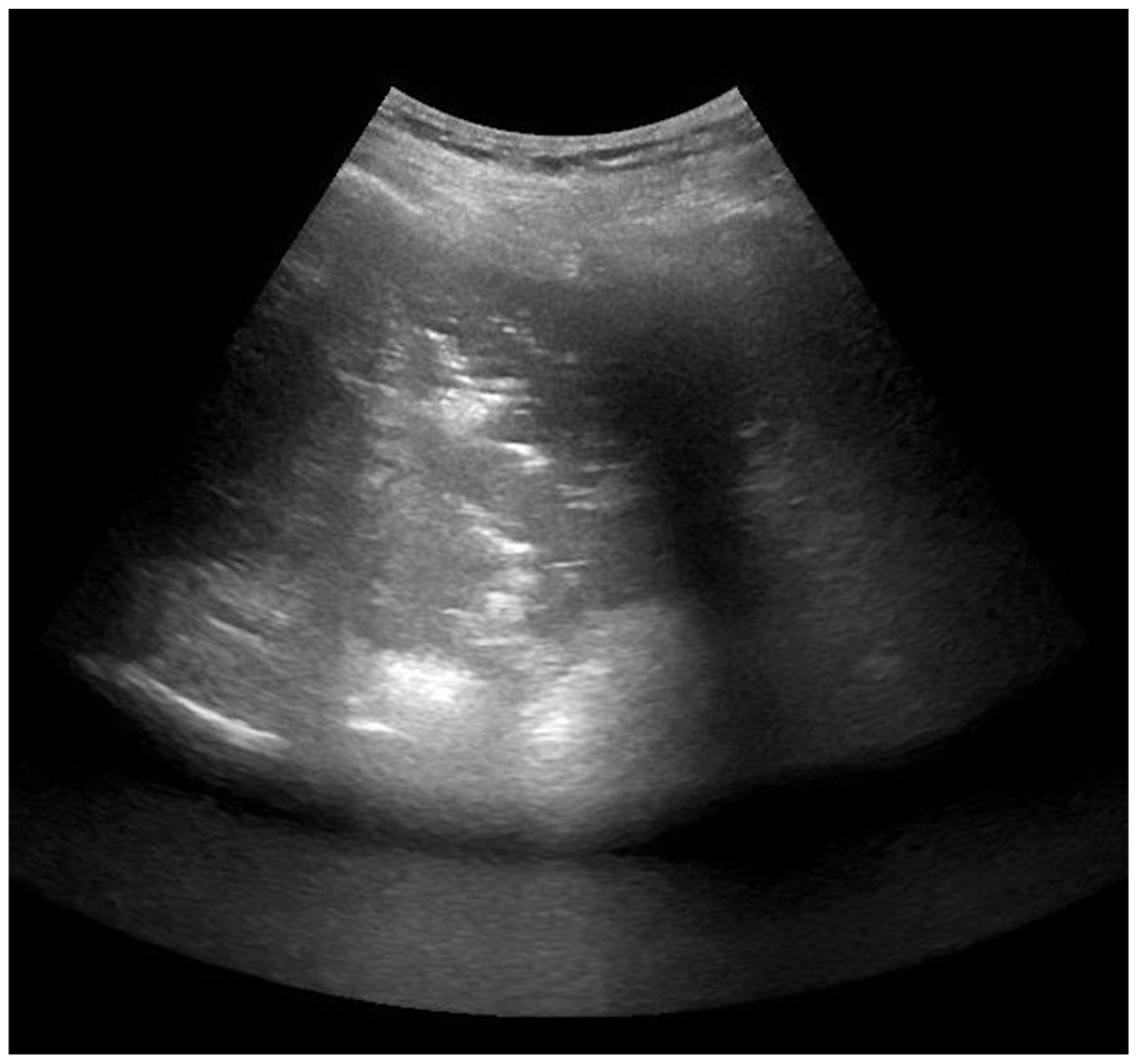
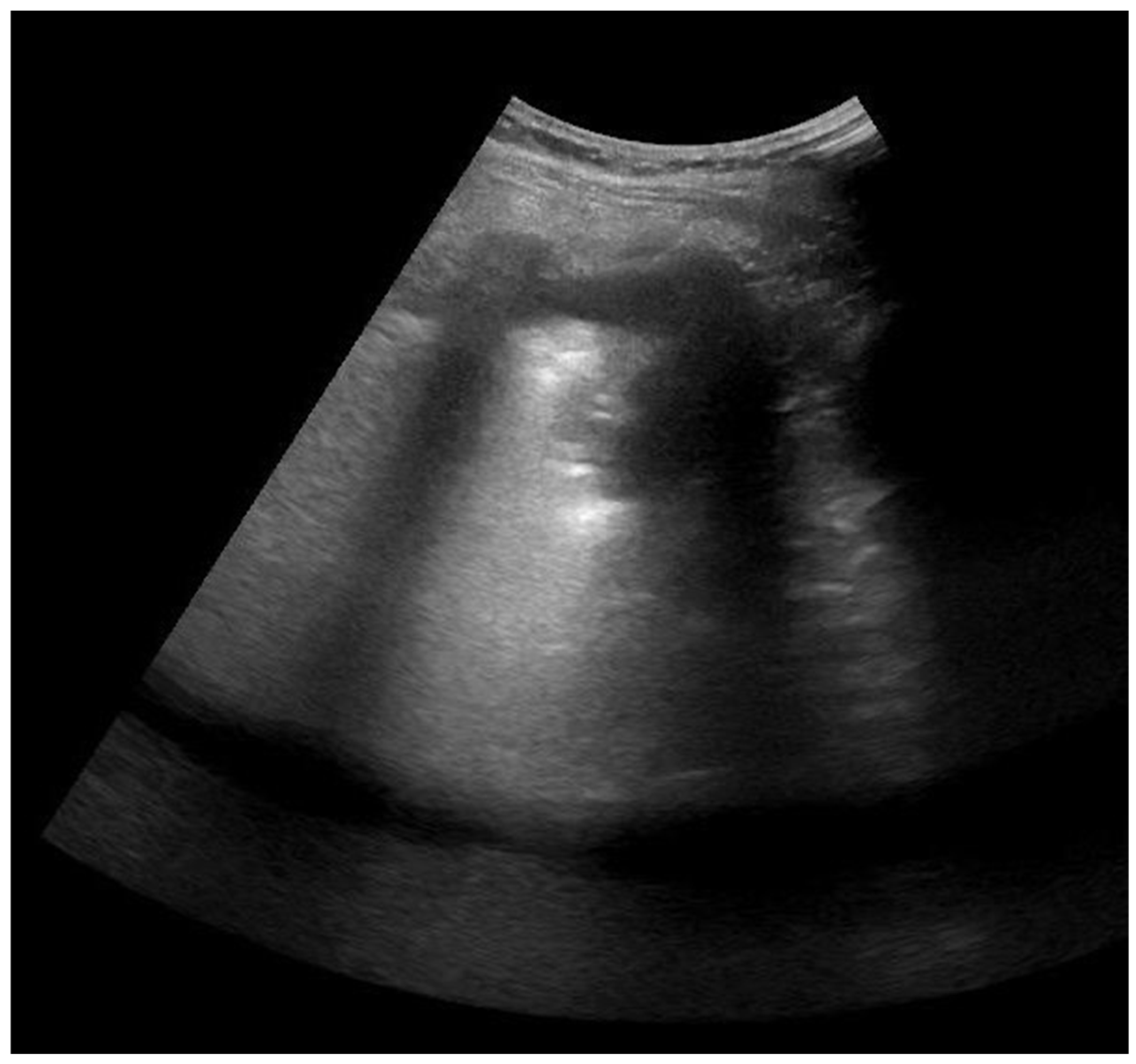
2.4. Lung Ultrasonography and Score Assessment
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Chest Computed Tomography (CT) and Lung Ultrasound (LUS) Scores
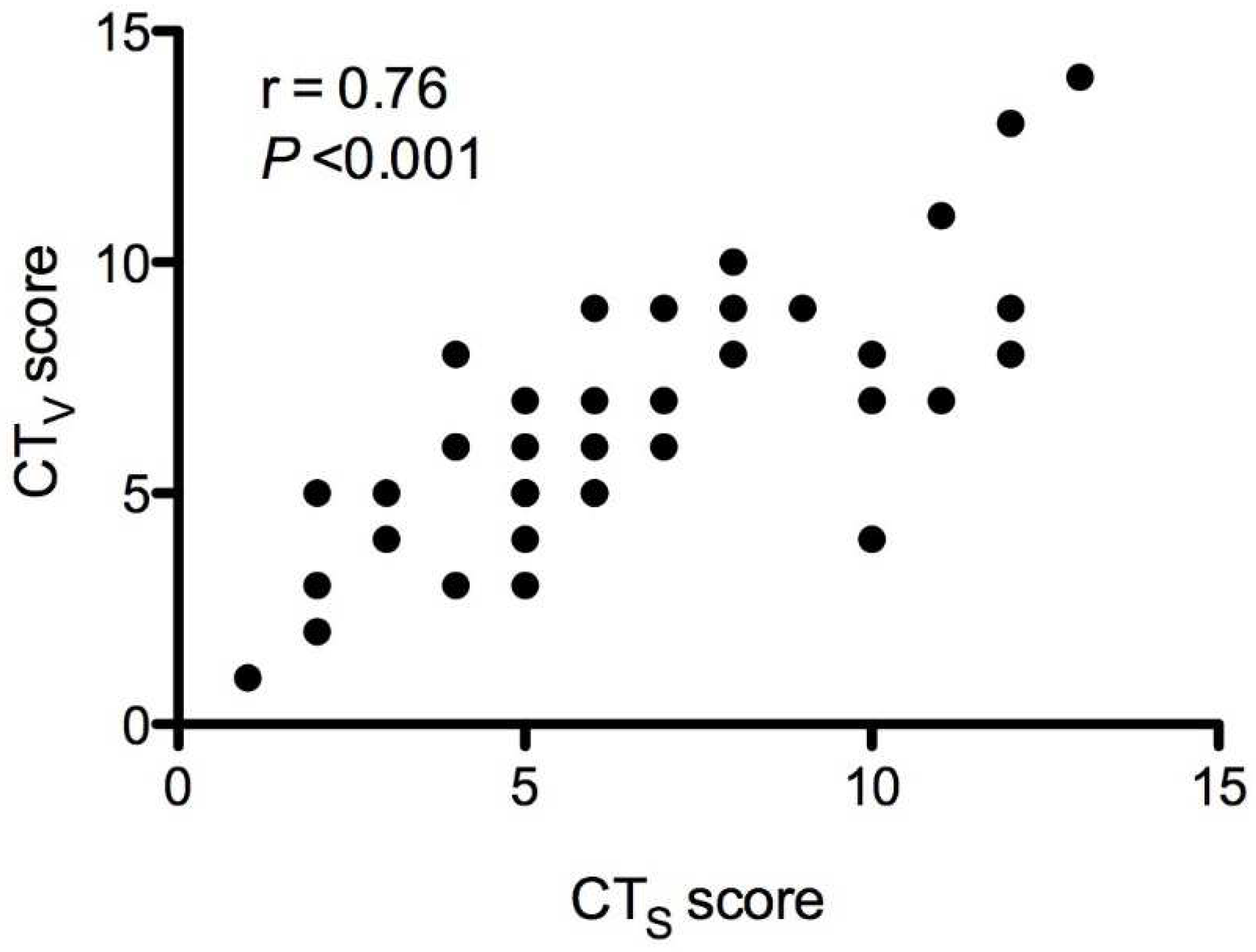
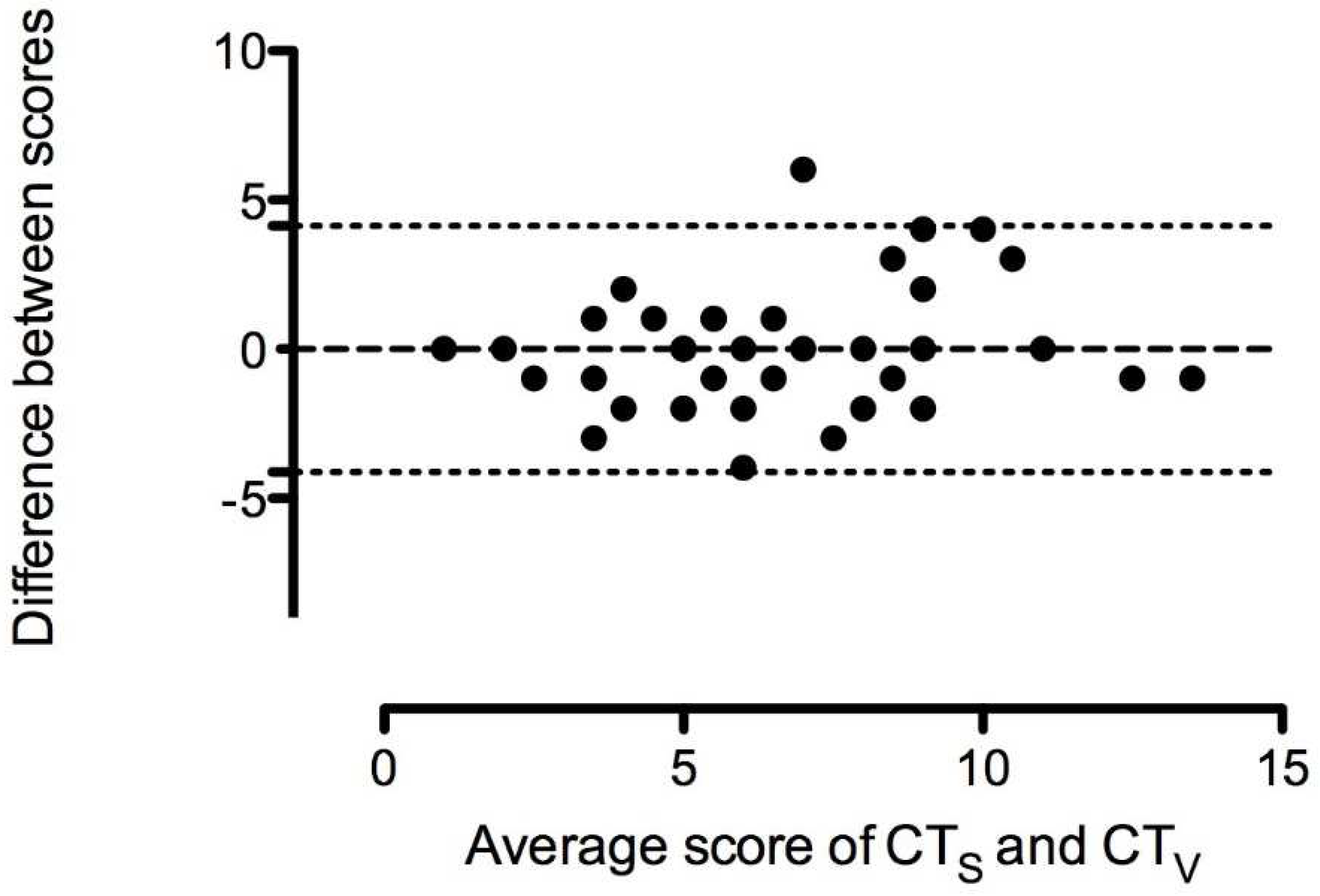
3.3. Agreement between CT-Software (CTs) and CT-Estimated (CTV) Scores
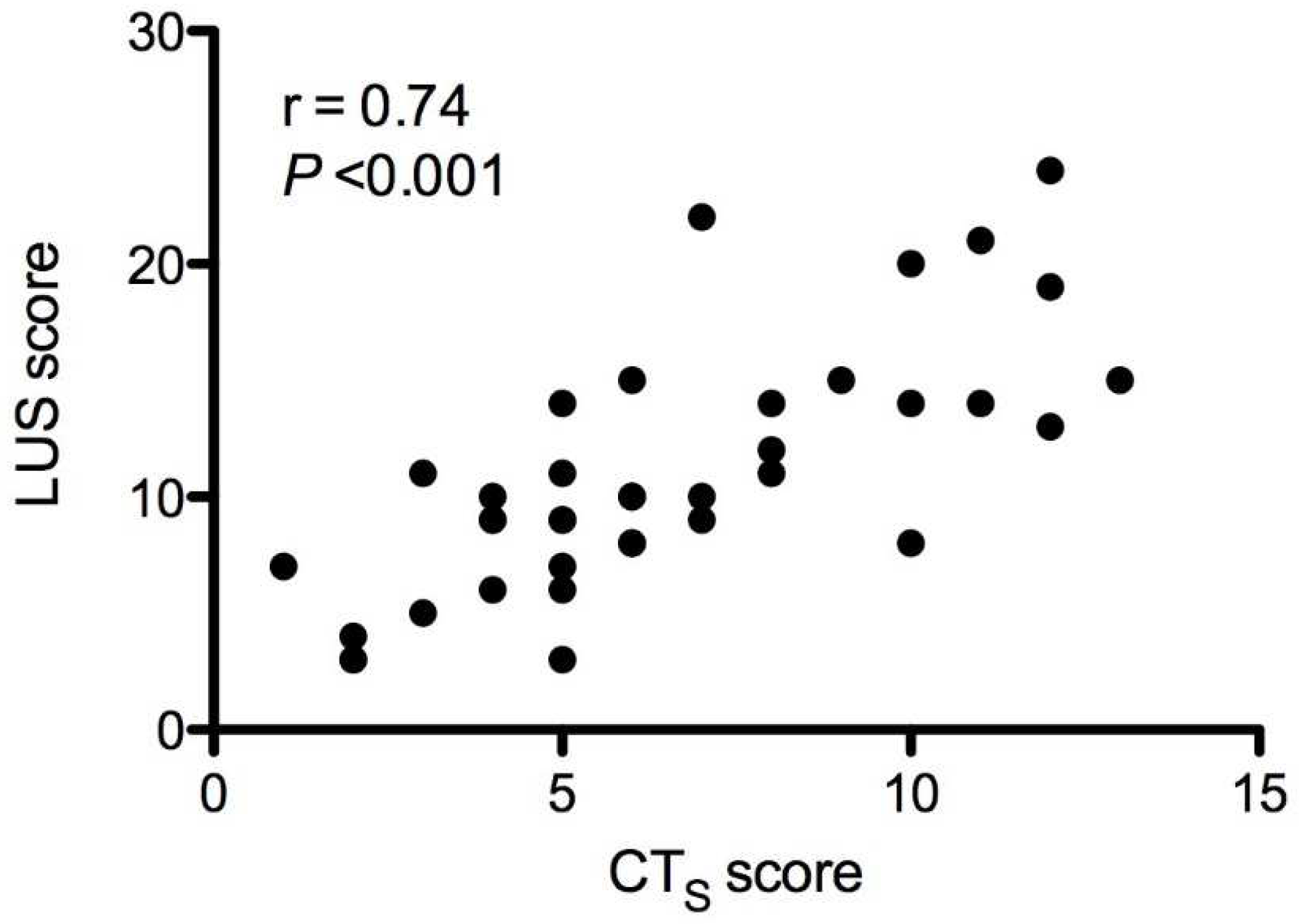
3.4. Correlation between Lung Ultrasound Score (LUS) and CT-Software (CTS) Score and Other Clinical Variables
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A





References
- Bao, L.; Deng, W.; Huang, B.; Gao, H.; Liu, J.; Ren, L.; Wei, Q.; Yu, P.; Xu, Y.; Qi, F.; et al. The pathogenicity of SARS-CoV-2 in hACE2 transgenic mice. Nature 2020, 583, 830–833. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Xu, L.; Xie, X.; Yan, H.; Xie, B.; Xu, W.; Liu, X.; Kang, G.; Jiang, W.; Yuan, J. Pulmonary Pathology of Early Phase COVID-19 Pneumonia in a Patient with a Benign Lung Lesion. Histopathology 2020, 77, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.T.; Leung, S.T.; Chin, T.W.Y.; Lo, C.S.Y.; Lui, M.M.S.; Lee, J.C.Y.; Chiu, K.W.H.; Chung, T.W.H.; et al. Frequency and Distribution of Chest Radiographic Findings in COVID-19 Positive Patients. Radiology 2019, 296, E72–E78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Radiology (ACR). Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (accessed on 22 April 2020).
- Rodrigues, J.; Hare, S.; Edey, A.; Devaraj, A.; Jacob, J.; Johnstone, A.; McStay, R.; Nair, A.; Robinson, G.; Rodrigues, J.; et al. An update on COVID-19 for the radiologist—A British society of Thoracic Imaging statement. Clin. Radiol. 2020, 75, 323–325. [Google Scholar] [CrossRef] [Green Version]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT findings in coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptinve study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Reissig, A.; Copetti, R.; Mathis, G.; Mempel, C.; Schuler, A.; Zechner, P.; Aliberti, S.; Neumann, R.; Kroegel, C.; Hoyer, H. Lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia: A prospective, multicenter, diagnostic accuracy study. Chest 2012, 142, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Bourcier, J.-E.; Paquet, J.; Seinger, M.; Gallard, E.; Redonnet, J.-P.; Cheddadi, F.; Garnier, D.; Bourgeois, J.-M.; Geeraerts, T. Performance comparison of lung ultrasound and chest X-ray for the diagnosis of pneumonia in the ED. Am. J. Emerg. Med. 2014, 32, 115–118. [Google Scholar] [CrossRef]
- Llamas-Álvarez, A.M.; Tenza-Lozano, E.M.; Latour-Pérez, J. Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults: Systematic Review and Meta-Analysis. Chest 2017, 151, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Hendin, A.; Koenig, S.; Millington, S.J. Better with Ultrasound: Thoracic Ultrasound. Chest 2020, 158, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Gardiner, E. Point of care and intensive care lung ultrasound: A reference guide for practitioners during COVID-19. Radiography 2020, 26, e297–e302. [Google Scholar] [CrossRef] [PubMed]
- Kalkanis, A.; Wauters, E.; Testelmans, D.; Yserbyt, J.; Lorent, N.; Louvaris, Z.; Godinas, L.; Van Mol, P.; Wauters, J.; Eleftheriou, M.; et al. Early lung ultrasound assessment for the prognosis of patients hospitalized for COVID-19 pneumonia. A pilot study. Respir. Med. Res. 2021, 80, 100832. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with ommunity-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic ociety and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 22 April 2020).
- Available online: https://marketplace.teamplay.siemens.com/app/detail/Frontier-Pneumonia-Analysis?product=syngo.via (accessed on 22 April 2020).
- Chang, Y.C.; Yu, C.J.; Chang, S.C.; Galvin, J.R.; Liu, H.M.; Hsiao, C.H.; Kuo, P.H.; Chen, K.Y.; Franks, T.J.; Huang, K.M.; et al. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: Evaluation with thin-section CT. Radiology 2005, 236, 1067–1075. [Google Scholar] [CrossRef]
- Bouhemad, B.; Zhang, M.; Lu, Q.; Rouby, J.J. Clinical review: Bedside lung ultrasound in critical care practice. Crit. Care 2007, 11, 205. [Google Scholar] [CrossRef]
- Bouhemad, B.; Mongodi, S.; Via, G.; Rouquette, I. Ultrasound for “Lung Monitoring” of Ventilated Patients. Anesthesiology 2015, 122, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Mongodi, S.; Bouhemad, B.; Orlando, A.; Stella, A.; Tavazzi, G.; Via, G.; Iotti, G.A.; Braschi, A.; Mojoli, F. Modified Lung Ultrasound Score for Assessing and Monitoring Pulmonary Aeration. Ultraschall. Med. 2017, 38, 530–537. [Google Scholar] [CrossRef]
- Bujang, M.; Baharum, N. Sample Size Guideline for Correlation Analysis. World J. Soc. Sci. Res. 2016, 3, 37–46. [Google Scholar] [CrossRef]
- Buonsenso, D.; Pata, D.; Chiaretti, A. COVID-19 outbreak: Less stethoscope, more ultrasound. Lancet Respir. Med. 2020, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mongodi, S.; Via, G.; Girard, M.; Rouquette, I.; Misset, B.; Braschi, A.; Mojoli, F.; Bouhemad, B. Lung Ultrasound for Early Diagnosis of Ventilator-Associated Pneumonia. Chest 2016, 149, 969–980. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, S.; Shrestha, P.S.; Shrestha, G.S.; Marhatta, M.N. Clinical impact of lung ultrasound monitoring for diagnosis of ventilator associated pneumonia: A diagnostic randomized controlled trial. J. Crit. Care 2020, 58, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Soummer, A.; Perbet, S.; Brisson, H.; Arbelot, C.; Constantin, J.-M.; Lu, Q.; Rouby, J.-J. Lung Ultrasound Study Group. Ultrasound assessment of lung aeration loss during a successful weaning trial predicts postextubation distress. Crit. Care Med. 2012, 40, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Mongodi, S.; Algieri, I.; Vergani, G.L.; Orlando, A.; Via, G.; Crimella, F.; Cressoni, M.; Mojoli, F. Assessment of Lung Aeration and Recruitment by CT Scan and Ultrasound in Acute Respiratory Distress Syndrome Patients. Crit. Care Med. 2018, 46, 1761–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiumello, D.; Umbrello, M.; Papa, G.F.S.; Angileri, A.; Gurgitano, M.; Formenti, P.; Coppola, S.; Froio, S.; Cammaroto, A.; Carrafiello, G. Global and Regional Diagnostic Accuracy of Lung Ultrasound Compared to CT in Patients with Acute Respiratory Distress Syndrome. Crit. Care Med. 2019, 47, 1599–1606. [Google Scholar] [CrossRef]
- Fiala, M.J. Ultrasound in COVID-19: A timeline of ultrasound findings in relation to CT. Clin. Radiol. 2020, 75, 553–554. [Google Scholar] [CrossRef]
- Poggiali, E.; Dacrema, A.; Bastoni, D.; Tinelli, V.; Demichele, E.; Mateo Ramos, P.; Marcianò, T.; Silva, M.; Vercelli, A.; Magnacavallo, A. Can Lung US Help Critical Care Clinicians in the Early Diagnosis of Novel Coronavirus (COVID-19) Pneumonia? Radiology 2020, 295, E6. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | % or Median (IQR 25–75%) |
|---|---|
| Age, years | 64 (57–72) |
| Gender, % male | 63% |
| BMI, kg/m2 | 27 (25–31) |
| Presenting symptom, % fever or respiratory | 82% |
| Days from onset of illness to lung ultrasound | 6.5 (4–10) |
| ATS pneumonia severity, % severe | 18% |
| China NHC clinical classification, % severe | 76% |
| Pulse oximetry (SpO2), % | 92 (91–93) |
| Supplemental Oxygen NC, L/min | 2 (1–3) |
| White blood cell count, 103/µL | 5890 (4010–7645) |
| Neutrophil count, 103/µL | 4000 (2550–6100) |
| Lymphocyte count, 103/µL | 900 (600–1450) |
| Neutrophil-to-lymphocyte ratio | 4 (3–7) |
| Platelet count, 103/µL | 191,000 (156,500–270,750) |
| C-reactive protein, mg/L | 58 (25–106) |
| Lactate dehydrogenase, U/L | 300 (245–442) |
| Haemoglobin A1c, % | 6 (5.7–6.9) |
| D-dimer, ng/mL | 673 (372–1106) |
| Creatinine Clearance, mL/min/1.73 m2 | 80 (63–97) |
| Appearance of CT Findings | Any, n (%) | Predominant, n (%) |
|---|---|---|
| Ground-glass opacity (±crazy paving) | 36 (95%) | 32 (84%) |
| Consolidation (±ground-glass opacity) | 11 (29%) | 6 (16%) |
| Distribution of CT findings | ||
| Peripheral (±central) | 38 (100%) | |
| Bilateral | 36 (95%) | |
| Number of lobes affected, mean | 4 ± 1 | |
| 1 or 2 | 4 (10%) | |
| 3 | 7 (18%) | |
| 4 | 10 (26%) | |
| 5 | 17 (45%) | |
| Appearance of LUS findings | Any, n(%) | Predominant, n (%) |
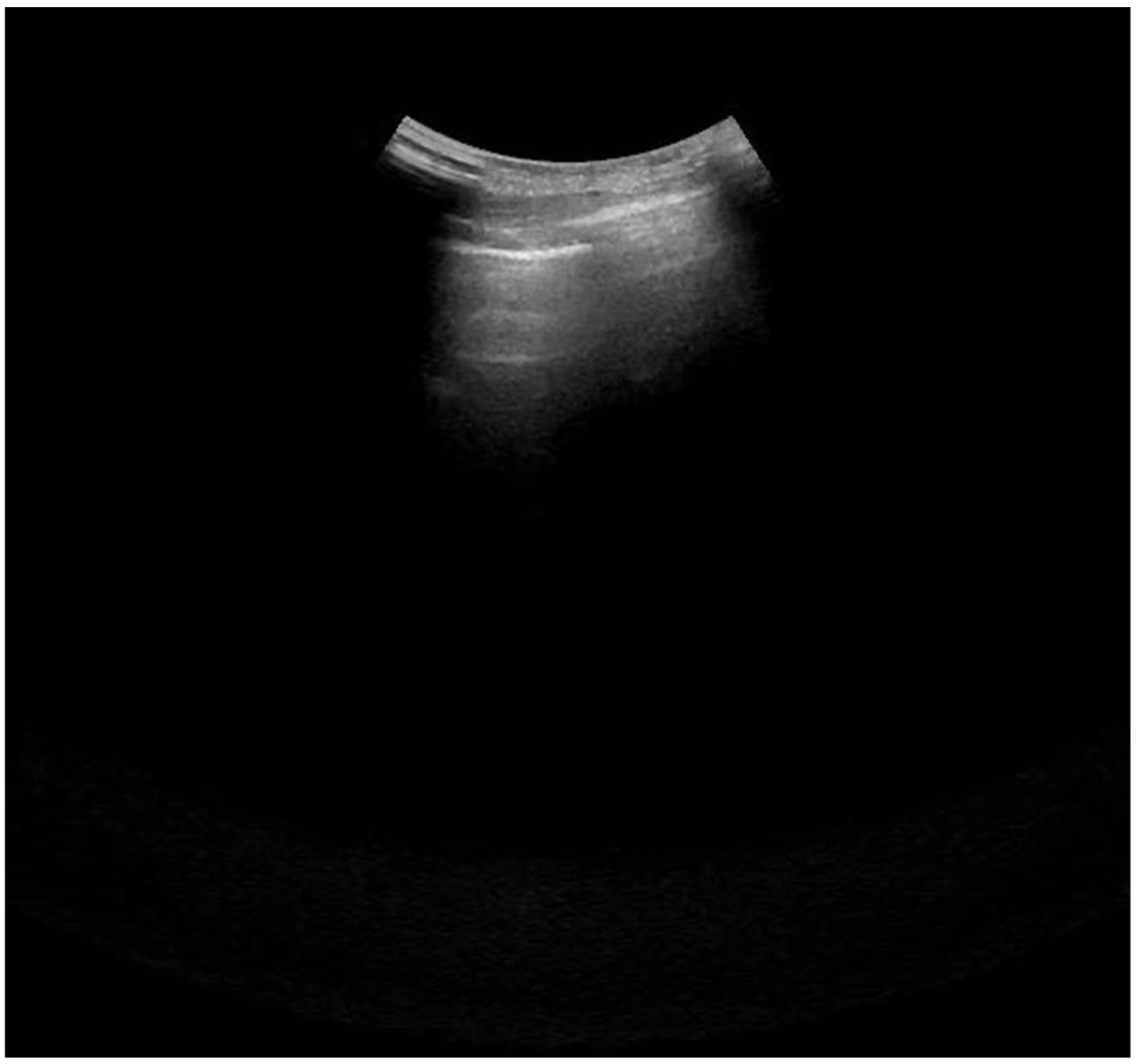
| Interstitial Edema (B1 pattern) | 35 (92%) | 23 (61%) |
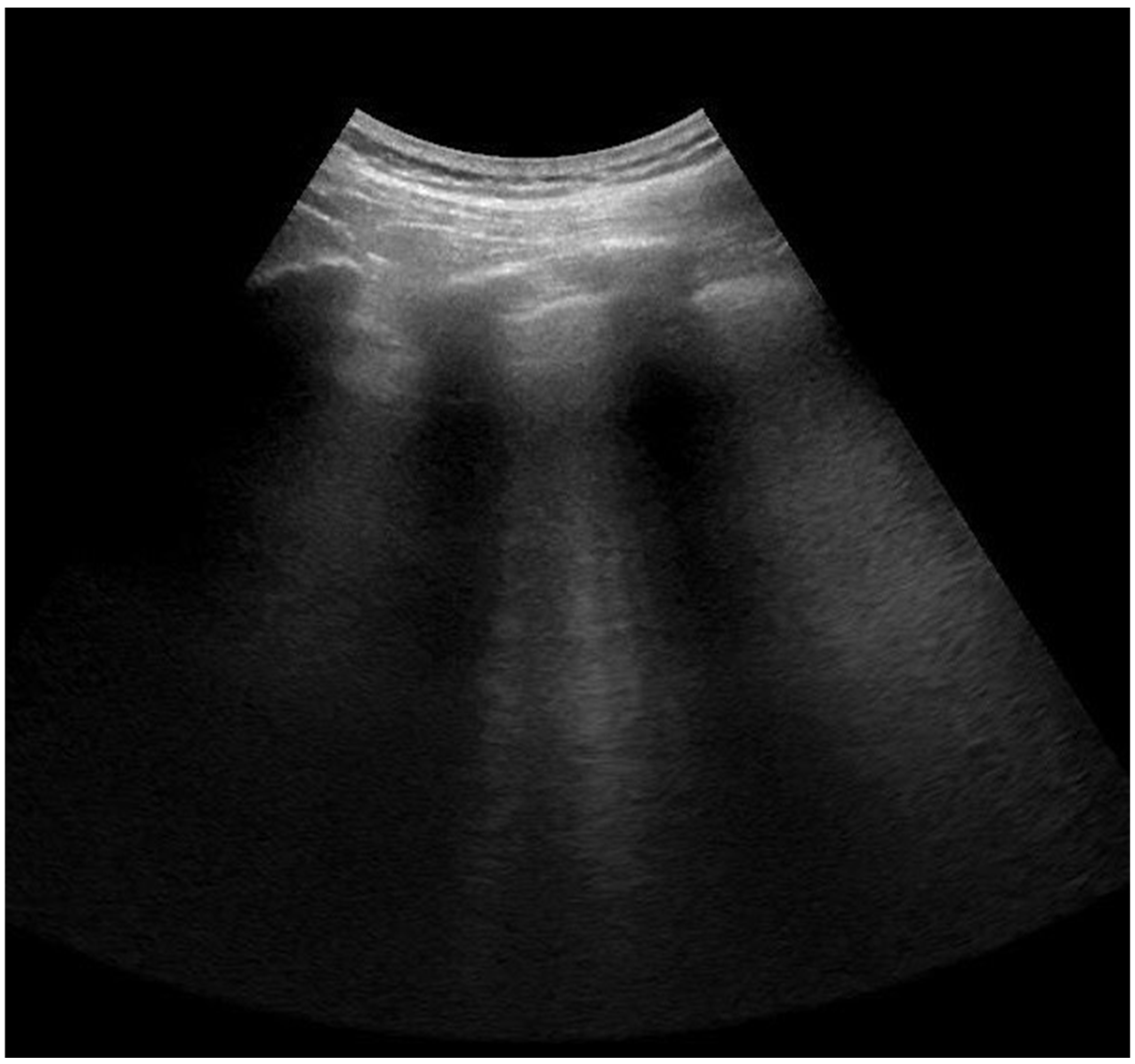
| Alveolar Edema (B2 pattern) | 31 (82%) | 16 (42%) |
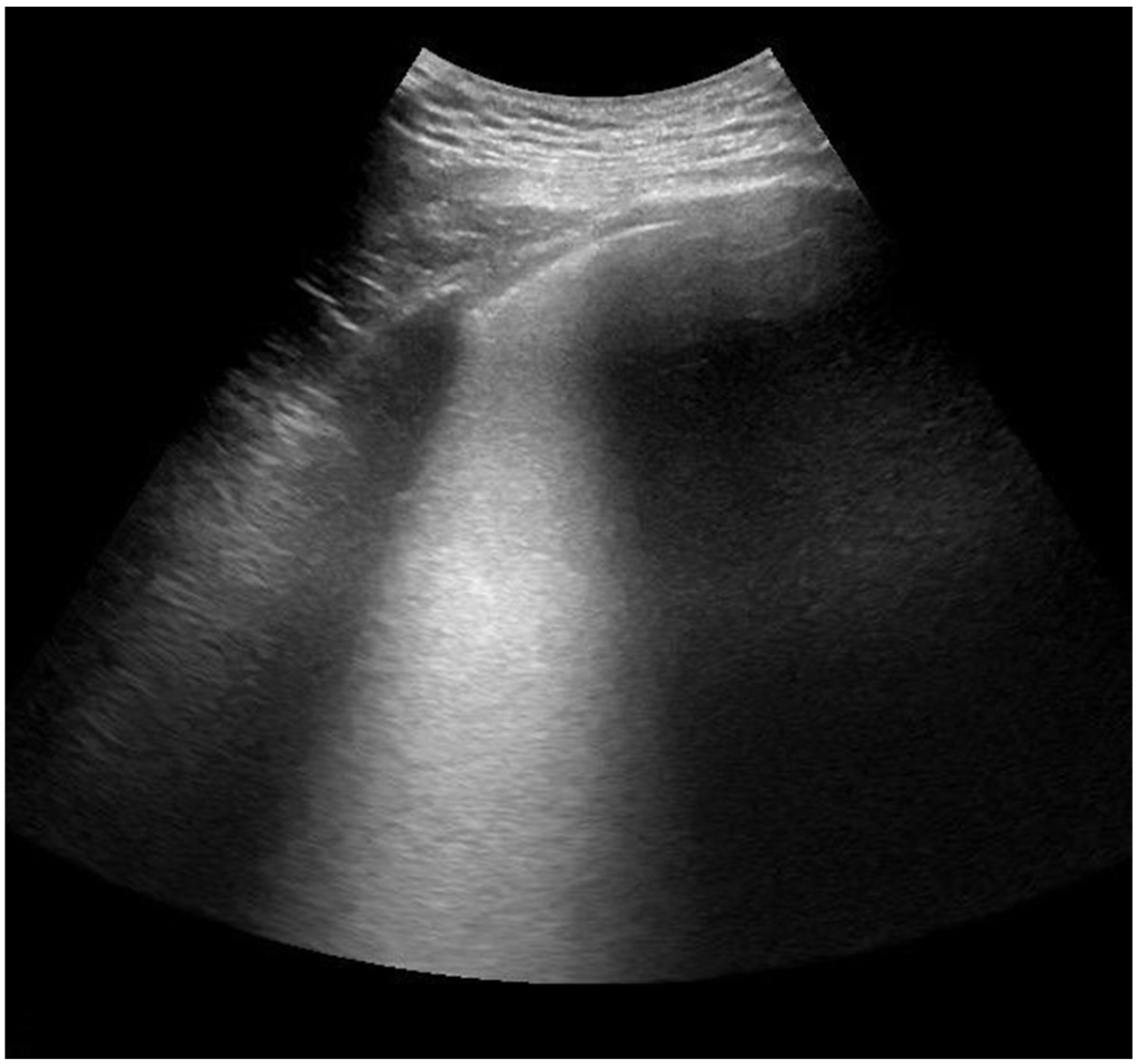
| Consolidation (C) | 11 (29%) | 4 (11%) |
| Pleural fluid | 2 (5%) | na |
| Distribution of LUS findings | ||
| Bilateral | 37 (97%) | |
| N of regions (out of 12) affected, mean | 7 ± 3 |
| Computed Tomography Software (CTs) | Lung Ultrasound(LUS) | |||
|---|---|---|---|---|
| Global ScoreMedian (IQR) | p-Value | Global ScoreMedian (IQR) | p-Value | |
| Age | ||||
| <median (64 years, n = 17) | 7 (5–10) | 0.38 | 11 (8–15) | 0.54 |
| ≥median (64 years, n = 21) | 5 (2–8) | 9 (8–14) | ||
| Gender | ||||
| male (n = 24) | 7 (4–10) | 0.39 | 11 (8–15) | 0.21 |
| female (n = 14) | 6 (4–7) | 9 (6–14) | ||
| BMI | ||||
| <median (27 kg/m2, n = 19) | 6 (5–10) | 0.65 | 10 (8–14) | 0.99 |
| ≥median (27 kg/m2, n = 19) | 5 (4–9) | 10 (7–14) | ||
| O2 saturation | ||||
| >median (92%, n = 17) | 5 (4–6) | 0.012 | 9 (7–11) | 0.018 |
| ≤median (92%, n = 21) | 8 (5–11) | 14 (8–17) | ||
| ChinaNHC classification | ||||
| moderate cases (n = 9) | 4 (3–6) | 0.007 | 9 (3–10) | 0.023 |
| severe cases (n = 29) | 7 (5–10) | 11 (8–15) | ||
| ATS severity | ||||
| non-severe (n = 31) | 5 (4–8) | 0.045 | 10 (7–14) | 0.14 |
| severe (n = 7) | 10 (6–12) | 15 (8–20) | ||
| Neutrophil count | ||||
| <median (4000 103/µL, n = 19) | 5 (4–8) | 0.17 | 9 (6–12) | 0.20 |
| ≥median (4000 103/µL, n = 19) | 7 (5–10) | 12 (8–15) | ||
| NLR | ||||
| <median (4, n = 19) | 6 (4–9) | 0.20 | 9 (6–14) | 0.11 |
| ≥median (4, n = 19) | 7 (5–11) | 12 (10–14) | ||
| C-reactive protein | ||||
| <median (58 mg/L, n = 19) | 5 (3–7) | 0.017 | 9 (5–10) | 0.002 |
| ≥median (58 mg/L, n = 19) | 8 (5–10) | 14 (9–15) | ||
| D-dimer | ||||
| <median (673 ng/mL, n = 19) | 5 (4–7) | 0.04 | 9 (6–11) | 0.06 |
| ≥median (673 ng/mL, n = 19) | 7 (5–11) | 13 (8–19) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalkanis, A.; Schepers, C.; Louvaris, Z.; Godinas, L.; Wauters, E.; Testelmans, D.; Lorent, N.; Van Mol, P.; Wauters, J.; De Wever, W.; et al. Lung Aeration in COVID-19 Pneumonia by Ultrasonography and Computed Tomography. J. Clin. Med. 2022, 11, 2718. https://doi.org/10.3390/jcm11102718
Kalkanis A, Schepers C, Louvaris Z, Godinas L, Wauters E, Testelmans D, Lorent N, Van Mol P, Wauters J, De Wever W, et al. Lung Aeration in COVID-19 Pneumonia by Ultrasonography and Computed Tomography. Journal of Clinical Medicine. 2022; 11(10):2718. https://doi.org/10.3390/jcm11102718
Chicago/Turabian StyleKalkanis, Alexandros, Christophe Schepers, Zafeiris Louvaris, Laurent Godinas, Els Wauters, Dries Testelmans, Natalie Lorent, Pierre Van Mol, Joost Wauters, Walter De Wever, and et al. 2022. "Lung Aeration in COVID-19 Pneumonia by Ultrasonography and Computed Tomography" Journal of Clinical Medicine 11, no. 10: 2718. https://doi.org/10.3390/jcm11102718
APA StyleKalkanis, A., Schepers, C., Louvaris, Z., Godinas, L., Wauters, E., Testelmans, D., Lorent, N., Van Mol, P., Wauters, J., De Wever, W., & Dooms, C. (2022). Lung Aeration in COVID-19 Pneumonia by Ultrasonography and Computed Tomography. Journal of Clinical Medicine, 11(10), 2718. https://doi.org/10.3390/jcm11102718