
Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases

 ,
, 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
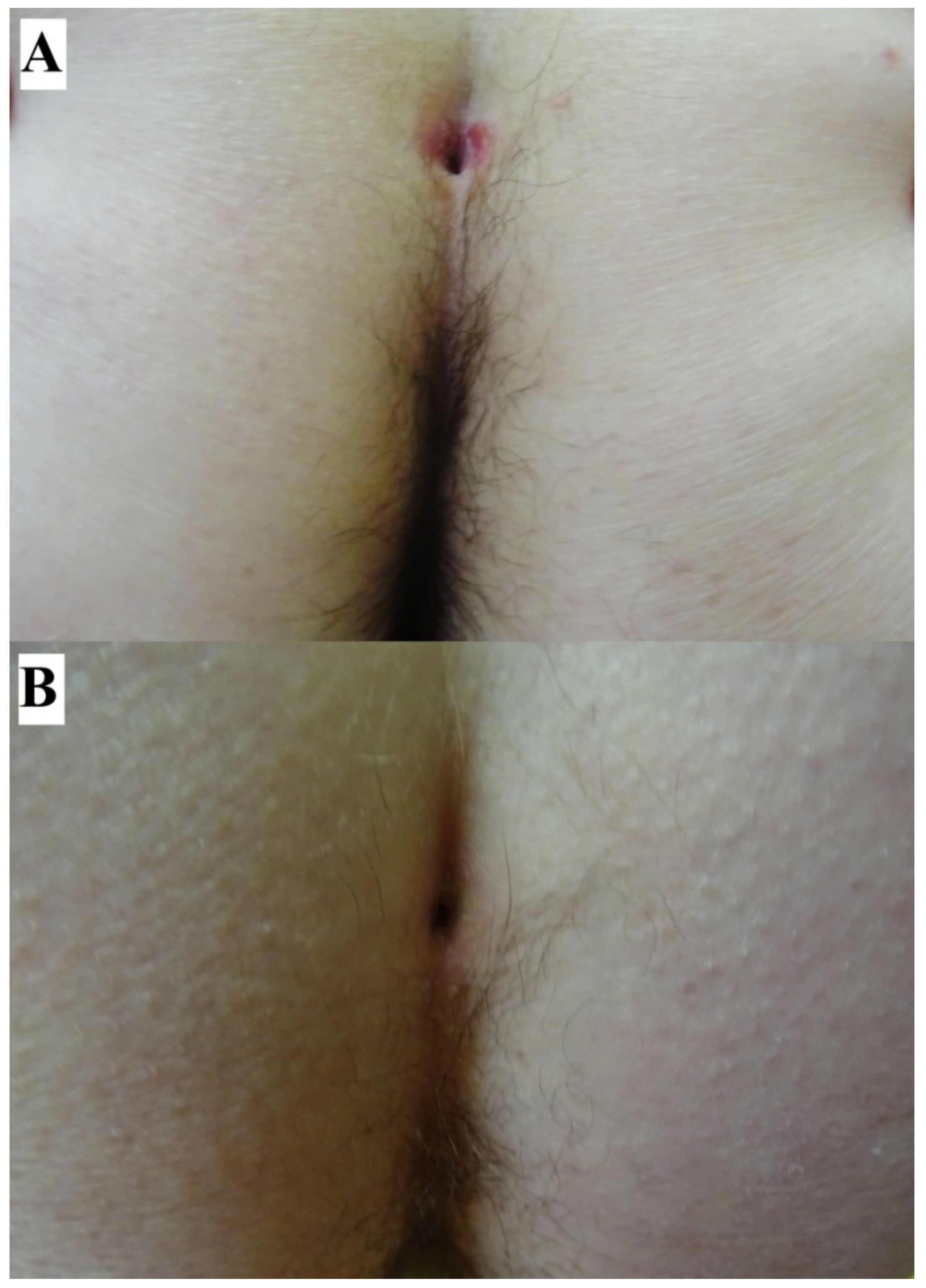
2. Case Report: Sacral Dimple Involvement
3. Case Report: Ocular Involvement
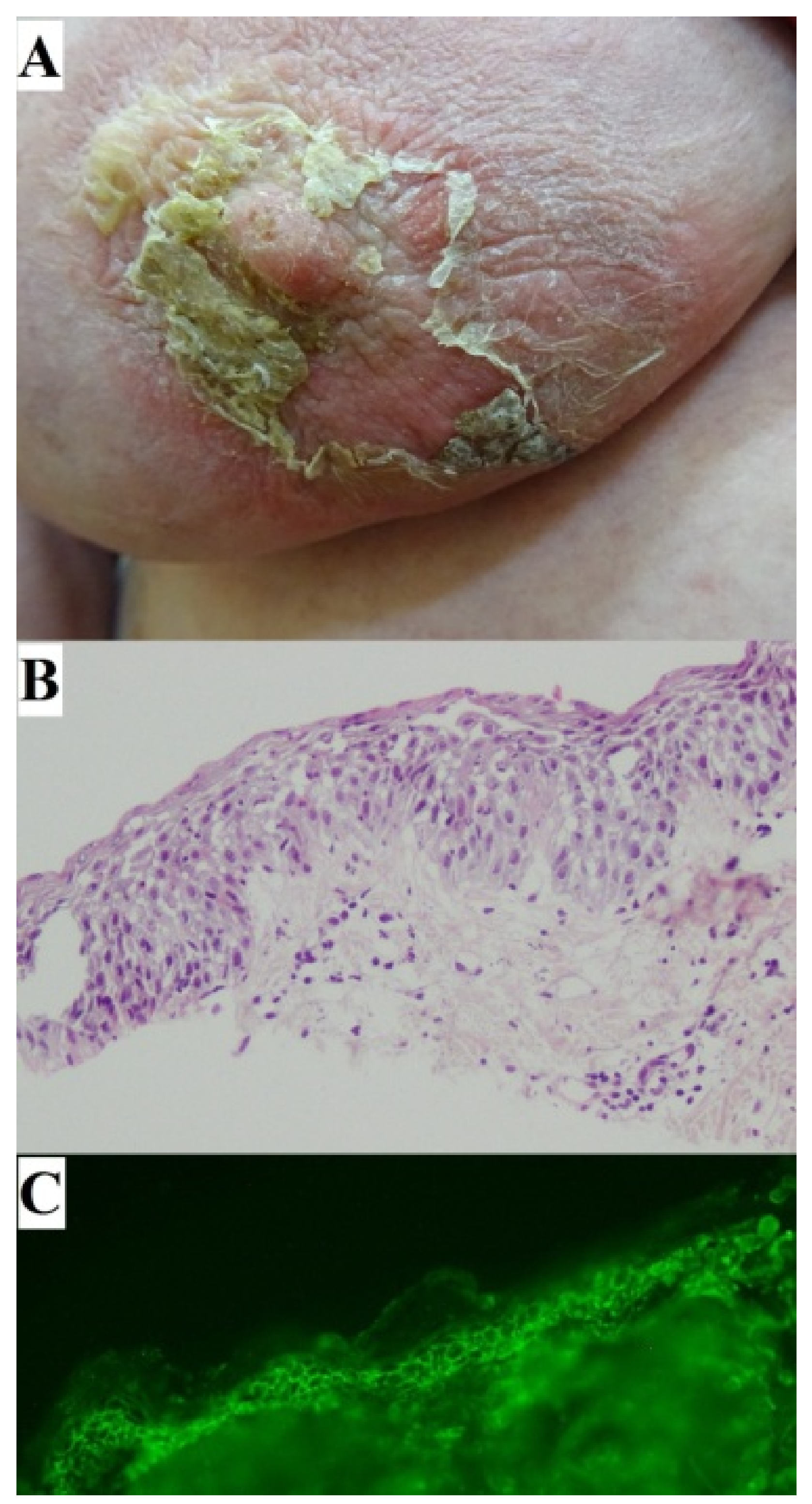
4. Case Report: Nipple Involvement
5. Discussion of the Issues Common to the Described PV Locations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Didona, D.; Maglie, R.; Eming, R.; Hertl, M. Pemphigus: Current and future therapeutic strategies. Front. Immunol. 2019, 10, 1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feizi, S.; Roshandel, D. Ocular manifestations and management of autoimmune bullous diseases. J. Ophthalmic Vis. Res. 2019, 14, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Ohki, M.; Kikuchi, S. Nasal, oral, and pharyngolaryngeal manifestations of pemphigus vulgaris: Endoscopic ororhinolaryngologic examination. Ear Nose Throat J. 2017, 96, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Kavala, M.; Altıntaş, S.; Kocatürk, E.; Zindancı, İ.; Can, B.; Ruhi, Ç.; Turkoglu, Z. Ear, nose and throat involvement in patients with pemphigus vulgaris: Correlation with severity, phenotype and disease activity. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1324–1327. [Google Scholar] [CrossRef]
- Robati, R.M.; Rahmati-Roodsari, M.; Dabir-Moghaddam, P. Mucosal manifestations of pemphigus vulgaris in ear, nose, and throat; before and after treatment. J. Am. Acad. Dermatol. 2012, 67, 249–252. [Google Scholar] [CrossRef]
- Malik, M.; Razzaque, A. Involvement of the female genital tract in pemphigus vulgaris. Obstet. Gynecol. 2005, 106 Pt 1, 1005–1012. [Google Scholar] [CrossRef]
- Pietkiewicz, P.; Bowszyc-Dmochowska, M.; Gornowicz-Porowska, J.; Dmochowski, M. Involvement of nail apparatus in pemphigus vulgaris in ethnic Poles is infrequent. Front. Med. 2018, 5, 227. [Google Scholar] [CrossRef]
- Dmochowski, M. Natural body orifices and mucous membranes in pemphigus vulgaris. Dermatol. Klin. 2007, 9, 124–131. [Google Scholar]
- Jałowska, M.; Gornowicz-Porowska, J.; Seraszek-Jaros, A.; Bowszyc-Dmochowska, M.; Kaczmarek, E.; Dmochowski, M. Clinical significance of umbilical region involvement in pemphigus vulgaris in a series of 81 ethnic Poles: A comparative analysis of the distribution of lesions in two infrequent locations. Adv. Dermatol. Allergol. Post. Derm. Alerg. 2022, 39, 281–285. [Google Scholar] [CrossRef]
- Aoki, W.; Maruta, C.; Santi, C. Umbilical involvement in pemphigus vulgaris. J. Am. Acad. Dermatol. 2010, 62, AB79. [Google Scholar]
- Lee, A.C.; Kwong, N.S. Management of sacral dimples detected on routine newborn examination: A case series and review. HK J. Paediatr. 2007, 12, 93–95. [Google Scholar]
- Mostafa, M.; Nasef, N.; Barakat, T.; El-Hawary, A.K.; Abdel-Hady, H. Acute flaccid paralysis in a patient with sacral dimple. World J. Clin. Pediatr. 2013, 2, 26–30. [Google Scholar] [CrossRef]
- Gloushankova, N.A.; Rubtsova, S.N.; Zhitnyak, I.Y. Cadherin-mediated cell-cell interactions in normal and cancer cells. Tissue Barriers 2017, 5, e1356900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraga-Babi, M.; Stefanovi, V.; Saraga, M.; Wartiovaara, J.; Lehtonen, E. Expression of intermediate filaments and desmosomal proteins during differentiation of the human spinal cord. Acta Histochemica 2002, 104, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Vielmuth, F.; Rötzer, V.; Hartlieb, E.; Hirneiß, C.; Waschke, J.; Spindler, V. Pemphigus autoantibodies induce blistering in human conjunctiva. Invest. Ophthalmol. Vis. Sci. 2016, 57, 4442–4449. [Google Scholar] [CrossRef] [Green Version]
- Memar, O.; Jabbehdari, S.; Caughlin, B.; Djalilian, A.R. Ocular surface involvement in pemphigus vulgaris: An interdisciplinary review. Ocul. Surf. 2020, 18, 40–46. [Google Scholar] [CrossRef]
- Daoud, Y.J.; Cervantes, R.; Foster, C.S.; Ahmed, A.R. Ocular pemphigus. J. Am. Acad. Dermatol. 2005, 53, 585–590. [Google Scholar] [CrossRef]
- Akhyani, M.; Keshtkar-Jafari, A.; Chams-Davatchi, C.; Lajevardi, V.; Beigi, S.; Aghazadeh, N.; Rayati Damavandi, M.; Arami, S. Ocular involvement in pemphigus vulgaris. J. Dermatol. 2014, 41, 618–621. [Google Scholar] [CrossRef]
- Gianniou, C.; Dirani, A.; Ferrini, W.; Marchionno, L.; Decugis, D.; Deli, A.; Ambresin, A.; Mantel, I. Cicatricial changes in ocular pemphigus. Eye 2014, 28, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Baykal, H.E.; Pleyer, U.; Sonnichsen, K.; Thiel, H.J.; Zierhut, M. Severe eye involvement in pemphigus vulgaris. Ophthalmologe 1995, 92, 854–857. [Google Scholar]
- Alkatan, H.; Alzahem, T. Histopathology of the Ocular Surface. In Histopathology: An Update; Srivastava, S., Ed.; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Gornowicz-Porowska, J.; Seraszek-Jaros, A.; Bowszyc-Dmochowska, M.; Bartkiewicz, P.; Kaczmarek, E.; Dmochowski, M. Clinical evaluation of a multiparametric ELISA as a rapid tool for routinely diagnosing IgG-mediated autoimmune blistering dermatoses in ethnic Slavs. J. Clin. Lab. Anal. 2018, 32, e22336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolnicu, S. Histology of the Normal Breast, Normal Changes, and Abnormalities of Breast Development. In Practical Atlas of Breast Pathology; Stolnicu, S., Alvarado-Cabrero, I., Eds.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Cieśla, S.; Wichtowski, M.; Poźniak-Balicka, R.; Murawa, D. The surgical anatomy of the mammary gland (part 1.) General structure, embryogenesis, histology, the nipple-areolar complex, the fascia of the glandular tissue and the chest wall. J. Oncol. 2020, 70, 211–219. [Google Scholar] [CrossRef]
- Maglie, R.; Montefusco, F.; Senatore, S.; Massimiliano D’Erme, A.; Bagnoni, G.; Antiga, E. Localized pemphigus exacerbation associated with underlying breast cancer. JAAD Case Rep. 2020, 6, 1268–1270. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Souto, F. Eroded plaques involving the breasts: A unique location of pemphigus vulgaris. An. Bras. Dermatol. 2020, 95, 670–671. [Google Scholar] [CrossRef] [PubMed]
- Guyton, D.P.; Stakleff, K.S.; Regula, E. Pemphigus vulgaris mimicking Paget’s disease of the breast. Breast J. 2003, 9, 319–322. [Google Scholar] [CrossRef]
- Pietkiewicz, P.; Gornowicz-Porowska, J.; Bowszyc-Dmochowska, M.; Jagielska, J.; Helak-Łapaj, C.; Kaczmarek, E.; Dmochowski, M. Discordant expression of desmoglein 2 and 3 at the mRNA and protein levels in nodular and superficial basal cell carcinoma revealed by immunohistochemistry and fluorescent in situ hybridization. Clin. Exp. Dermatol. 2014, 39, 628–635. [Google Scholar] [CrossRef]
- Çağlar, B.; Saral, C.; Akay, B.N.; Kundakçı, N. Paraneoplastic pemphigus and nipple hyperkeratosis triggered with Castleman disease. Turk. J. Dermatol. 2019, 13, 49–51. [Google Scholar] [CrossRef]
- Rashid, A.; Wang, J.; Fu, P.; Wang, W.; Xie, H. Pemphigus vulgaris associated with surgery: A rare association. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 299–301. [Google Scholar] [CrossRef]
- Xue, J.; Su, W.; Chen, Z.; Ke, Y.; Du, X.; Zhou, Q. Overexpression of interleukin-23 and interleukin-17 in the lesion of pemphigus vulgaris: A preliminary study. Mediat. Inflamm. 2014, 2014, 463–928. [Google Scholar] [CrossRef]
- Nagel, A.; Lang, A.; Engel, D.; Podstawa, E.; Hunzelmann, N.; de Pita, O.; Borradori, L.; Uter, W.; Hertl, M. Clinical activity of pemphigus vulgaris relates to IgE autoantibodies against desmoglein 3. Clin. Immunol. 2010, 134, 320–330. [Google Scholar] [CrossRef]
- Teh, M.T.; Fortun, F.; Kenneth, E.; Wan, H. A molecular study of desmosomes identifies a desmoglein isoform switch in head and neck squamous cell carcinoma. J. Oral Pathol. Med. 2011, 40, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Delva, E.; Tucker, D.K.; Kowalczyk, A.P. The Desmosome. Cold Spring Harb. Perspect. Biol. 2009, 1, a002543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elias, P.M.; Matsuyoshi, N.; Wu, H.; Lin, C.; Wang, Z.H.; Brown, B.E.; Stanley, J.R. Desmoglein isoform distribution affects stratum corneum structure and function. J. Cell Biol. 2001, 153, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, H.; Yuan, M.; Simpson, C.; Allen, K.; Gavins, F.N.; Ikram, M.S.; Basu, S.; Baksh, N.; O’Toole, E.A.; Hart, I.R. Stem/progenitor cell-like properties of desmoglein 3dim cells in primary and immortalized keratinocyte lines. Stem Cells 2007, 25, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Koster, M.I.; Kim, S.; Roop, D.R. P63 deficiency: A failure of lineage commitment or stem cell maintenance? J. Investig. Dermatol. Symp. Proc. 2005, 10, 118–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehman, A.; Cai, Y.; Hünefeld, C.; Jedličková, H.; Huang, Y.; Teck Teh, M.; Sharif Ahmad, U.; Uttagomol, J.; Wang, Y.; Kang, A.; et al. The desmosomal cadherin desmoglein-3 acts as a keratinocyte anti-stress protein via suppression of p53. Cell Death Dis. 2019, 10, 750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, H.W.; Chun, S.H.; Lee, J.M.; Jeon, J.; Hashimoto, T.; Kim, I.H. Radiotherapy-induced pemphigus vulgaris. J. Dermatol. 2014, 41, 851–852. [Google Scholar] [CrossRef]
- Mehregan, D.R.; Roenigk, R.K.; Gibson, L.E. Postsurgical pemphigus. Arch. Dermatol. 1992, 128, 414–415. [Google Scholar] [CrossRef]
- Duick, M.G.; Zaks, B.; Moy, L.R.; Kaplan, R.P. Mohs micrographic surgery-induced pemphigus. Dermatol. Surg. 2001, 27, 895–897. [Google Scholar] [CrossRef]
- Jetter, N.; Cerci, F.B.; Pandher, K.; Krunic, A.L. Pemphigus vegetans developing after Mohs micrographic surgery and cryotherapy. An. Bras. Dermatol. 2021, 96, 520–523. [Google Scholar] [CrossRef]
- Sagi, L.; Trau, H. The Koebner phenomenon. Clin. Dermatol. 2011, 29, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Daneshpazhooh, M.; Fatehnejad, M.; Rahbar, Z.; Balighi, K.; Ghandi, N.; Ghiasi, M. Trauma-induced pemphigus: A case series of 36 patients. J. Dtsch. Dermatol. Ges. 2016, 14, 166–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinay, K.; Kanwar, A.J.; Saikia, U.N. Pemphigus occurring at tuberculin injection site: Role of cytokines in acantholysis. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 539–541. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.M.; Gibson, F.T.; Amber, K.T. Recurrent pemphigus foliaceus at the site of a surgical scar following total knee arthroplasty. J. Clin. Aesthet. Dermatol. 2020, 13, 12. [Google Scholar] [PubMed]
- Milani-Nejad, N.; Chung, C.; Kaffenberger, J. Recurrence of localized pemphigus foliaceus induced by knee replacement. J. Clin. Aesthet. Dermatol. 2019, 12, 12. [Google Scholar]
- Tolkachjov, S.N.; Frith, M.; Cooper, L.D.; Harmon, C.B. Pemphigus foliaceus demonstrating pathergy after Mohs micrographic surgery. Dermatol. Surg. 2018, 44, 1352–1353. [Google Scholar] [CrossRef]
- Rotunda, A.M.; Bhupathy, A.R.; Dye, R.; Soriano, T.T. Pemphigus foliaceus masquerading as postoperative wound infection: Report of a case and review of the Koebner and related phenomenon following surgical procedures. Dermatol. Surg. 2005, 31, 226–231. [Google Scholar] [CrossRef]
- Zhou, S.; Liu, Z.; Yuan, H.; Zhao, X.; Zou, Y.; Zheng, J.; Pan, M. Autoreactive B cell differentiation in diffuse ectopic lymphoid-like structures of inflamed pemphigus lesions. J. Investig. Dermatol. 2020, 140, 309–318. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jałowska, M.; Gornowicz-Porowska, J.; Bowszyc-Dmochowska, M.; Dmochowski, M. Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases. J. Clin. Med. 2022, 11, 2855. https://doi.org/10.3390/jcm11102855
Jałowska M, Gornowicz-Porowska J, Bowszyc-Dmochowska M, Dmochowski M. Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases. Journal of Clinical Medicine. 2022; 11(10):2855. https://doi.org/10.3390/jcm11102855
Chicago/Turabian StyleJałowska, Magdalena, Justyna Gornowicz-Porowska, Monika Bowszyc-Dmochowska, and Marian Dmochowski. 2022. "Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases" Journal of Clinical Medicine 11, no. 10: 2855. https://doi.org/10.3390/jcm11102855
APA StyleJałowska, M., Gornowicz-Porowska, J., Bowszyc-Dmochowska, M., & Dmochowski, M. (2022). Sacral Dimple, Conjunctiva, and Nipple as Less Obvious Pemphigus Vulgaris Locations around Natural Body Orifices: A Report of Three Cases. Journal of Clinical Medicine, 11(10), 2855. https://doi.org/10.3390/jcm11102855