
Artificial Intelligence-Enhanced Echocardiography for Systolic Function Assessment



Abstract
:1. Left Ventricular Systolic Function Assessment in Clinical Practice
2. AI’s Application in Left Ventricular Systolic Function Assessment
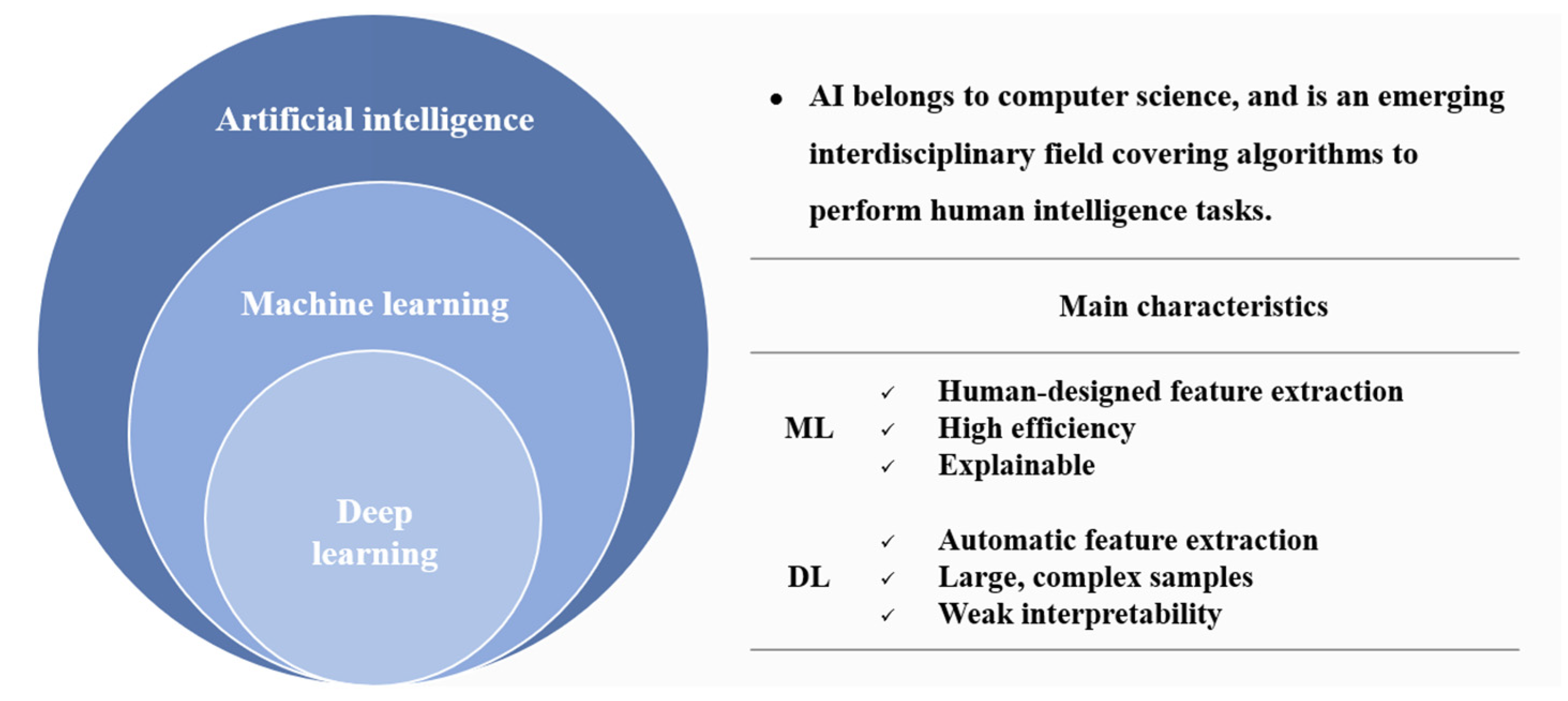
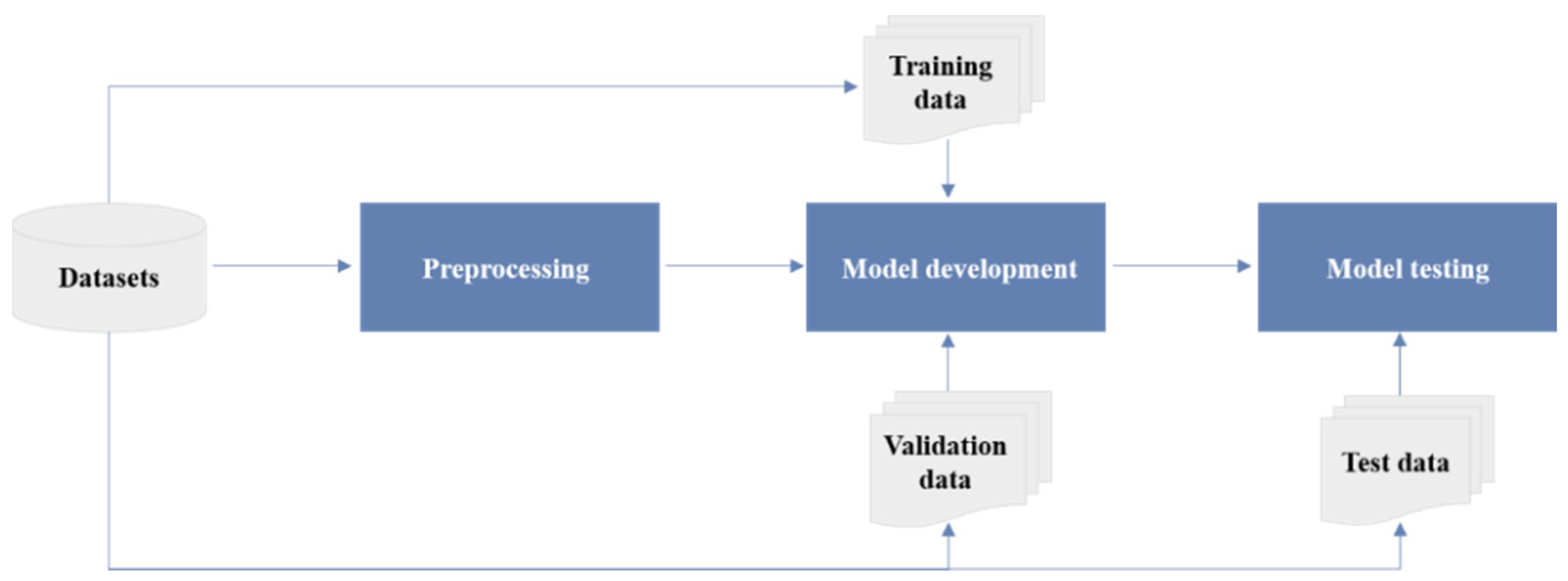
2.1. Key Concepts in AI
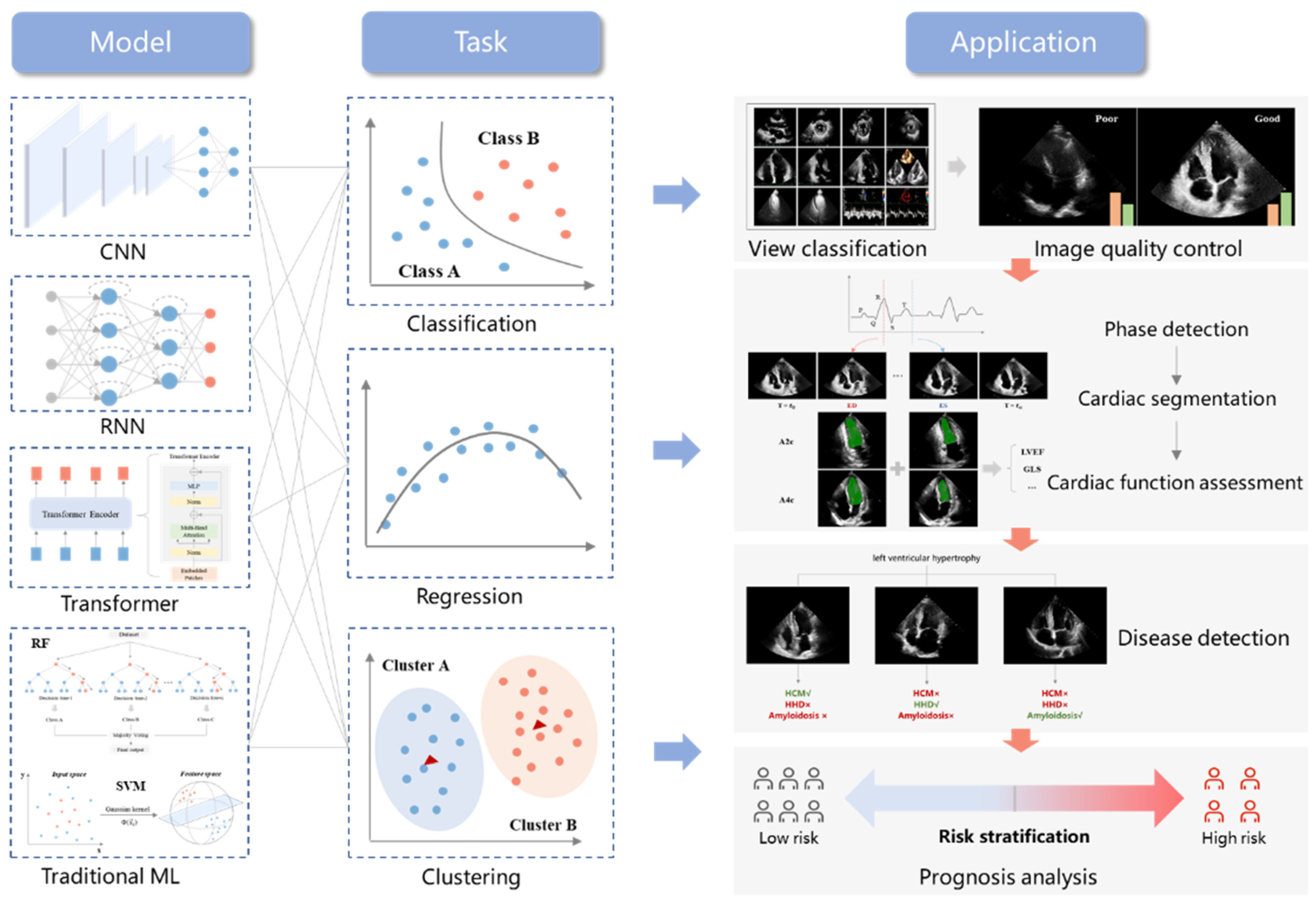
2.2. AI in Echocardiography
3. AI’s Application in Left Ventricular Systolic Function—LVEF
3.1. Cardiac Segmentation
3.2. Automatic Assessment of LVEF
3.3. Disease Diagnosis

{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Task | Model | Dataset | Results |
|---|---|---|---|---|---|
| Leclerc S. et al. [16] | 2019 | LV segmentation | U-Net | 500 subjects | Accuracy in LV volumes (MAE = 9.5 mL, r = 0.95). |
| Smistad E. et al. [17] | 2019 | LV segmentation | U-Net | 606 subjects | Accuracy for LV segmentation (DSC 0.776–0.786). |
| Leclerc S. et al. [18] | 2020 | LV segmentation | LU-Net | 500 subjects | Accuracy in LV volumes (MAE = 7.6 mL, r = 0.96). |
| Wei H. et al. [28] | 2020 | LV segmentation | CLAS | 500 subjects | Accuracy for LVEF assessment (r = 0.926, bias = 0.1%). |
| Reynaud H. et al. [29] | 2021 | LVEF assessment | Transformer | 10,030 subjects | Accuracy for LVEF assessment (MAE = 5.95%, R2 = 0.52). |
| Ouyang et al. [19] | 2020 | LVEF assessment | EchoNet-Dynamic | 10,030 subjects | Accuracy for LV segmentation (DSC = 0.92), LVEF assessment (MAE = 4.1%), and HFpEF classification (AUC 0.97). |
| Asch F.M. et al. [20] | 2019 | LVEF assessment | CNN | >50,000 studies | AutoEF values show agreement with GT: r = 0.95, bias = 1.0%, with sensitivity 0.90 and specificity 0.92 for detection of EF less than 35%. |
| Zhang J. et al. [21] | 2018 | LVEF assessment GLS assessment Disease detection | CNN | 14,035 studies | Agreement with GT: for LVEF, MAE = 9.7%; for GLS, and MAE = 7.5% and 9.0% (within 2 cohorts). Disease detection: HCM, Amyloid, and PAH (AUC 0.93, 0.87, and 0.85). |
| Tromp J. et al. [30] | 2022 | LVEF assessment | CNN | 43,587 studies | Accuracy for LVEF assessment (MAE 6–10%). |
| Narang A. et al. [15] | 2021 | LVEF assessment | Caption Guidance | 240 subjects | LV size, function, and pericardial effusion in 237 cases (98.8%) and RV size in 222 cases (92.5%) are of diagnostic quality. |
| Asch F.M. et al. [32] | 2021 | LVEF assessment | Caption Health | 166 subjects (Protocol 1) 67 subjects (Protocol 2) | Protocol 1: agreement with GT: ICC 0.86–0.95, bias < 2%. Protocol 2: agreement with GT: ICC = 0.84, bias 2.5 ± 6.4%. |
| Tokodi M. et al. [24] | 2020 | Disease detection (HFpEF) | TDA | 1334 subjects | Region 4 relative to 1: HR = 2.75, 95%CI 1.27–45.95, p = 0.01. Correlation of NYHA and ACC/AHA stages with regions: r = 0.56 and 0.67. |
4. AI’s Application in Left Ventricular Systolic Function—GLS
4.1. Automatic Assessment of GLS
4.2. Disease Diagnosis
| Authors | Year | Task | Models | Dataset | Results |
|---|---|---|---|---|---|
| Kawakami H. et al. [34] | 2021 | GLS assessment | AutoStrain | 561 subjects | Automated vs. manual GLS: r = 0.685, bias = 0.99%. Semi-automated vs. manual GLS: r = 0.848, bias = −0.90%. Automated vs. semi-automated GLS: r = 0.775, bias = 1.89%. |
| Salte I.M. et al. [22] | 2021 | GLS assessment | EchoPWC-Net | 200 studies | EchoPWC-Net vs. EchoPAC: r = 0.93, MD 0.3 ± 0.3%. |
| Evain E. et al. [36] | 2022 | GLS assessment | PWC-Net | >60,000 images | Automated vs. Manual GLS: r = 0.77, MAE 2.5 ± 2.1%. |
| Narula S. et al. [25] | 2016 | Disease detection (ATH vs. HCM) | Ensemble model (SVM, RF, ANN) | 77 ATH, 62 HCM patients | Sensitivity 0.96; specificity 0.77. |
| Sengupta P.P. et al. [26] | 2016 | Disease detection (CP vs. RCM) | AMC | 50 CP patients, 44 RCM patients, and 47 controls | AUC 0.96. |
| Zhang J. et al. [27] | 2021 | Disease detection(CHD) | Two-step stacking | 217 CHD patients, 207 controls | Sensitivity 0.903; specificity 0.843; AUC 0.904. |
| Loncaric F. et al. [37] | 2021 | Disease detection (HT) | ML | 189 HT patients, 97 controls | HT is divided into 4 phenotypes. |
| Yahav A. et al. [38] | 2020 | Disease detection (strain curve classification) | ML | 424 subjects | Strain curve is divided into physiological, non-physiological, and uncertain categories (accuracy 86.4%). |
| Pournazari P. et al. [39] | 2021 | Prognosis analysis (COVID-19) | ML | 724 subjects | BC (AUC 0.79). BC + Laboratory data + Vital signs (AUC 0.86). BC + Laboratory data + Vital signs + Echos (AUC 0.92). |
| Przewlocka-Kosmala M. et al. [40] | 2019 | Prognosis analysis (HFpEF) | Clustering | 177 HFpEF patients, 51 asymptomatic controls | HFpEF is divided into 3 prognostic phenotypes. |
5. Challenges and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Nauta, J.F.; Jin, X.; Hummel, Y.M.; Voors, A.A. Markers of left ventricular systolic dysfunction when left ventricular ejection fraction is normal. Eur. J. Heart Fail. 2018, 20, 1636–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C. How Artificial Intelligence Will Change Medicine. Nature 2019, 576, S48. [Google Scholar] [CrossRef]
- Litjens, G.; Ciompi, F.; Wolterink, J.M.; de Vos, B.D.; Leiner, T.; Teuwen, J.; Išgum, I. State-of-the-Art Deep Learning in Cardiovascular Image Analysis. JACC Cardiovasc. Imaging 2019, 12, 1549–1565. [Google Scholar] [CrossRef]
- Davis, A.; Billick, K.; Horton, K.; Jankowski, M.; Knoll, P.; Marshall, J.E.; Paloma, A.; Palma, R.; Adams, D.B. Artificial Intelligence and Echocardiography: A Primer for Cardiac Sonographers. J. Am. Soc. Echocardiogr. 2020, 33, 1061–1066. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Krittanawong, C.; Johnson, K.W.; Rosenson, R.S.; Wang, Z.; Aydar, M.; Baber, U.; Min, J.K.; Tang, W.H.W.; Halperin, J.L.; Narayan, S.M. Deep learning for cardiovascular medicine: A practical primer. Eur. Heart J. 2019, 40, 2058–2073. [Google Scholar] [CrossRef]
- Nolan, M.T.; Thavendiranathan, P. Automated Quantification in Echocardiography. JACC Cardiovasc. Imaging 2019, 12, 1073–1092. [Google Scholar] [CrossRef] [PubMed]
- Khamis, H.; Zurakhov, G.; Azar, V.; Raz, A.; Friedman, Z.; Adam, D. Automatic apical view classification of echocardiograms using a discriminative learning dictionary. Med. Image Anal. 2017, 36, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.; Ong, J.R.; Tibrewal, A.; Mofrad, M.R.K. Deep echocardiography: Data-efficient supervised and semi-supervised deep learning towards automated diagnosis of cardiac disease. NPJ Digit. Med. 2018, 1, 59. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.; Arnaout, R.; Mofrad, M.; Arnaout, R. Fast and accurate view classification of echocardiograms using deep learning. NPJ Digit. Med. 2018, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.; Bae, R.; Hong, H.; Thomas, Y.; Surette, S.; Cadieu, C.; Chaudhry, A.; Martin, R.P.; McCarthy, P.M.; Rubenson, D.S.; et al. Utility of a Deep-Learning Algorithm to Guide Novices to Acquire Echocardiograms for Limited Diagnostic Use. JAMA Cardiol. 2021, 6, 624–632. [Google Scholar] [CrossRef]
- Leclerc, S.; Smistad, E.; Pedrosa, J.; Ostvik, A.; Cervenansky, F.; Espinosa, F.; Espeland, T.; Berg, E.A.R.; Jodoin, P.-M.; Grenier, T.; et al. Deep Learning for Segmentation Using an Open Large-Scale Dataset in 2D Echocardiography. IEEE Trans. Med. Imaging 2019, 38, 2198–2210. [Google Scholar] [CrossRef] [Green Version]
- Smistad, E.; Salte, I.M.; Ostvik, A.; Leclerc, S.; Bernard, O.; Lovstakken, L. Segmentation of apical long axis, four-and two-chamber views using deep neural networks. In Proceedings of the IEEE International Ultrasonics Symposium, Glasgow, UK, 6–9 October 2019. [Google Scholar]
- Leclerc, S.; Smistad, E.; Ostvik, A.; Cervenansky, F.; Espinosa, F.; Espeland, T.; Rye Berg, E.A.; Belhamissi, M.; Israilov, S.; Grenier, T.; et al. LU-Net: A Multistage Attention Network to Improve the Robustness of Segmentation of Left Ventricular Structures in 2-D Echocardiography. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 2519–2530. [Google Scholar] [CrossRef]
- Ouyang, D.; He, B.; Ghorbani, A.; Yuan, N.; Ebinger, J.; Langlotz, C.P.; Heidenreich, P.A.; Harrington, R.A.; Liang, D.H.; Ashley, E.A.; et al. Video-based AI for beat-to-beat assessment of cardiac function. Nature 2020, 580, 252–256. [Google Scholar] [CrossRef]
- Asch, F.M.; Poilvert, N.; Abraham, T.; Jankowski, M.; Cleve, J.; Adams, M.; Romano, N.; Hong, H.; Mor-Avi, V.; Martin, R.P.; et al. Automated Echocardiographic Quantification of Left Ventricular Ejection Fraction without Volume Measurements Using a Machine Learning Algorithm Mimicking a Human Expert. Circ. Cardiovasc. Imaging 2019, 12, e009303. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully Automated Echocardiogram Interpretation in Clinical Practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Salte, I.M.; Østvik, A.; Smistad, E.; Melichova, D.; Nguyen, T.M.; Karlsen, S.; Brunvand, H.; Haugaa, K.H.; Edvardsen, T.; Lovstakken, L.; et al. Artificial Intelligence for Automatic Measurement of Left Ventricular Strain in Echocardiography. JACC Cardiovasc. Imaging 2021, 14, 1918–1928. [Google Scholar] [CrossRef] [PubMed]
- Quer, G.; Arnaout, R.; Henne, M.; Arnaout, R. Machine Learning and the Future of Cardiovascular Care: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Tokodi, M.; Shrestha, S.; Bianco, C.; Kagiyama, N.; Casaclang-Verzosa, G.; Narula, J.; Sengupta, P.P. Interpatient Similarities in Cardiac Function: A Platform for Personalized Cardiovascular Medicine. JACC Cardiovasc. Imaging 2020, 13, 1119–1132. [Google Scholar] [CrossRef] [PubMed]
- Narula, S.; Shameer, K.; Salem Omar, A.M.; Dudley, J.T.; Sengupta, P.P. Machine-Learning Algorithms to Automate Morphological and Functional Assessments in 2D Echocardiography. J. Am. Coll. Cardiol. 2016, 68, 2287–2295. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.P.; Huang, Y.-M.; Bansal, M.; Ashrafi, A.; Fisher, M.; Shameer, K.; Gall, W.; Dudley, J.T. Cognitive Machine-Learning Algorithm for Cardiac Imaging: A Pilot Study for Differentiating Constrictive Pericarditis From Restrictive Cardiomyopathy. Circ. Cardiovasc. Imaging 2016, 9, e004330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhu, H.; Chen, Y.; Yang, C.; Cheng, H.; Li, Y.; Zhong, W.; Wang, F. Ensemble machine learning approach for screening of coronary heart disease based on echocardiography and risk factors. BMC Med. Inform. Decis. Mak. 2021, 21, 187. [Google Scholar] [CrossRef]
- Wei, H.; Cao, H.; Cao, Y.; Zhou, Y.; Xue, W.; Ni, D.; Li, S. Temporal-consistent Segmentation of Echocardiography with Co-learning from Appearance and Shape. In Proceedings of the Medical Image Computing and Computer Assisted Intervention, Lima, Peru, 29 June 2020. [Google Scholar]
- Reynaud, H.; Vlontzos, A.; Hou, B.; Beqiri, A.; Leeson, P.; Kainz, B. Ultrasound Video Transformers for Cardiac Ejection Fraction Estimation. arXiv 2021, arXiv:2107.00977. [Google Scholar]
- Tromp, J.; Seekings, P.J.; Hung, C.-L.; Iversen, M.B.; Frost, M.J.; Ouwerkerk, W.; Jiang, Z.; Eisenhaber, F.; Goh, R.S.M.; Zhao, H.; et al. Automated interpretation of systolic and diastolic function on the echocardiogram: A multicohort study. Lancet. Digit. Health 2022, 4, e46–e54. [Google Scholar] [CrossRef]
- Díaz-Gómez, J.L.; Mayo, P.H.; Koenig, S.J. Point-of-Care Ultrasonography. N. Engl. J. Med. 2021, 385, 1593–1602. [Google Scholar] [CrossRef]
- Asch, F.M.; Mor-Avi, V.; Rubenson, D.; Goldstein, S.; Saric, M.; Mikati, I.; Surette, S.; Chaudhry, A.; Poilvert, N.; Hong, H.; et al. Deep Learning-Based Automated Echocardiographic Quantification of Left Ventricular Ejection Fraction: A Point-of-Care Solution. Circ. Cardiovasc. Imaging 2021, 14, e012293. [Google Scholar] [CrossRef]
- Čelutkienė, J.; Plymen, C.M.; Flachskampf, F.A.; de Boer, R.A.; Grapsa, J.; Manka, R.; Anderson, L.; Garbi, M.; Barberis, V.; Filardi, P.P.; et al. Innovative imaging methods in heart failure: A shifting paradigm in cardiac assessment. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 1615–1633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawakami, H.; Wright, L.; Nolan, M.; Potter, E.L.; Yang, H.; Marwick, T.H. Feasibility, Reproducibility, and Clinical Implications of the Novel Fully Automated Assessment for Global Longitudinal Strain. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2021, 34, 136–145. [Google Scholar] [CrossRef]
- Leeson, P.; Fletcher, A.J. Let AI Take the Strain. JACC. Cardiovasc. Imaging 2021, 14, 1929–1931. [Google Scholar] [CrossRef] [PubMed]
- Evain, E.; Sun, Y.; Faraz, K.; Garcia, D.; Saloux, E.; Gerber, B.L.; De Craene, M.; Bernard, O. Motion estimation by deep learning in 2D echocardiography: Synthetic dataset and validation. IEEE Trans. Med. Imaging 2022. [Google Scholar] [CrossRef] [PubMed]
- Loncaric, F.; Marti Castellote, P.-M.; Sanchez-Martinez, S.; Fabijanovic, D.; Nunno, L.; Mimbrero, M.; Sanchis, L.; Doltra, A.; Montserrat, S.; Cikes, M.; et al. Automated Pattern Recognition in Whole-Cardiac Cycle Echocardiographic Data: Capturing Functional Phenotypes with Machine Learning. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2021, 34, 1170–1183. [Google Scholar] [CrossRef]
- Yahav, A.; Zurakhov, G.; Adler, O.; Adam, D. Strain Curve Classification Using Supervised Machine Learning Algorithm with Physiologic Constraints. Ultrasound Med. Biol. 2020, 46, 2424–2438. [Google Scholar] [CrossRef] [PubMed]
- Pournazari, P.; Spangler, A.L.; Ameer, F.; Hagan, K.K.; Tano, M.E.; Chamsi-Pasha, M.; Chebrolu, L.H.; Zoghbi, W.A.; Nasir, K.; Nagueh, S.F. Cardiac involvement in hospitalized patients with COVID-19 and its incremental value in outcomes prediction. Sci. Rep. 2021, 11, 19450. [Google Scholar] [CrossRef]
- Przewlocka-Kosmala, M.; Marwick, T.H.; Dabrowski, A.; Kosmala, W. Contribution of Cardiovascular Reserve to Prognostic Categories of Heart Failure With Preserved Ejection Fraction: A Classification Based on Machine Learning. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2019, 32, 604–615. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Zhu, Y.; Liu, M.; Zhang, Z.; Zhao, Y.; Yang, X.; Xie, M.; Zhang, L. Artificial Intelligence-Enhanced Echocardiography for Systolic Function Assessment. J. Clin. Med. 2022, 11, 2893. https://doi.org/10.3390/jcm11102893
Zhang Z, Zhu Y, Liu M, Zhang Z, Zhao Y, Yang X, Xie M, Zhang L. Artificial Intelligence-Enhanced Echocardiography for Systolic Function Assessment. Journal of Clinical Medicine. 2022; 11(10):2893. https://doi.org/10.3390/jcm11102893
Chicago/Turabian StyleZhang, Zisang, Ye Zhu, Manwei Liu, Ziming Zhang, Yang Zhao, Xin Yang, Mingxing Xie, and Li Zhang. 2022. "Artificial Intelligence-Enhanced Echocardiography for Systolic Function Assessment" Journal of Clinical Medicine 11, no. 10: 2893. https://doi.org/10.3390/jcm11102893
APA StyleZhang, Z., Zhu, Y., Liu, M., Zhang, Z., Zhao, Y., Yang, X., Xie, M., & Zhang, L. (2022). Artificial Intelligence-Enhanced Echocardiography for Systolic Function Assessment. Journal of Clinical Medicine, 11(10), 2893. https://doi.org/10.3390/jcm11102893