
Feasibility, Prediction and Association of Right Ventricular Free Wall Longitudinal Strain with 30-Day Mortality in Severe COVID-19 Pneumonia: A Prospective Study

Abstract
:1. Introduction
2. Materials and Methods
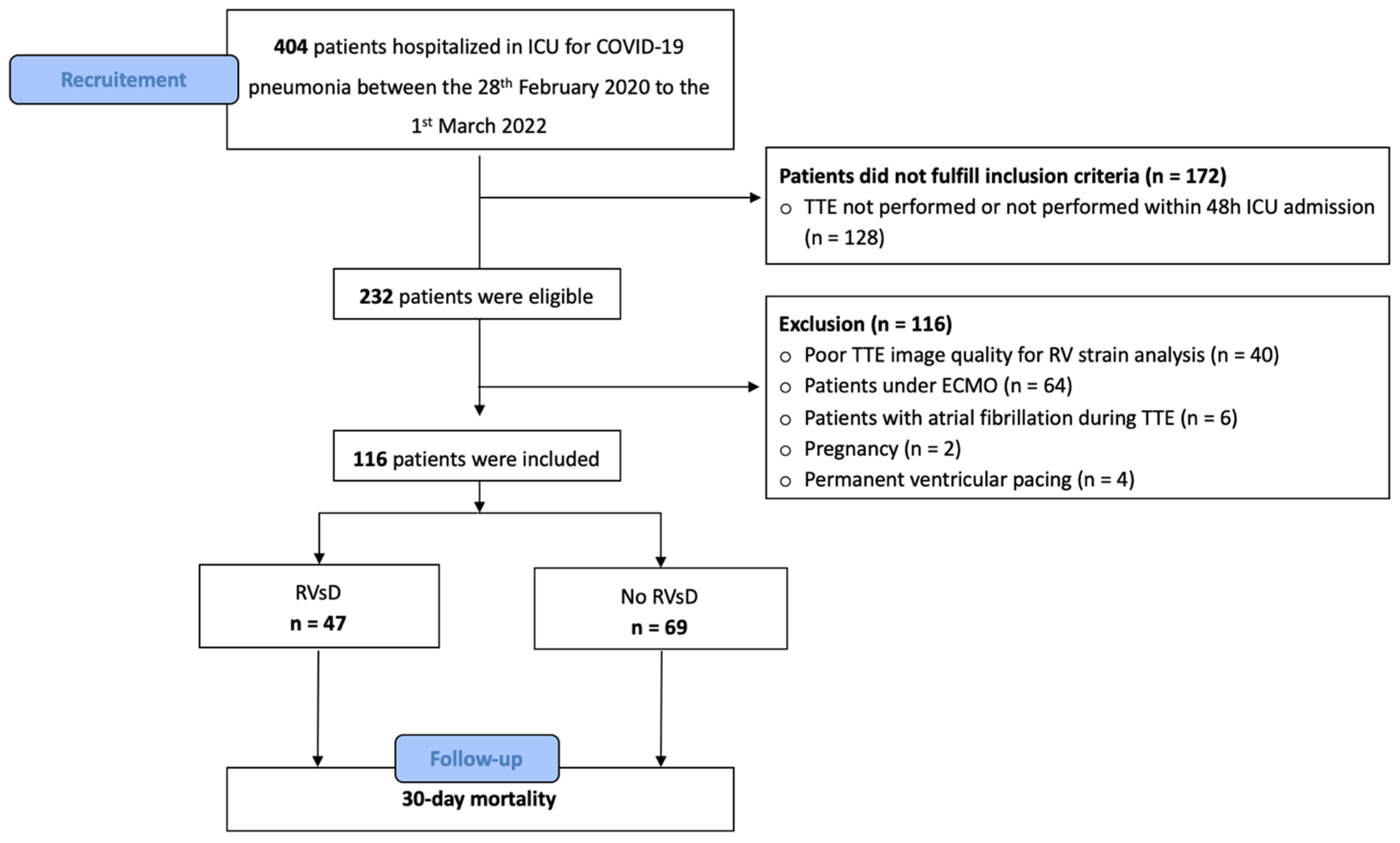
2.1. Population
2.2. Ethics
2.3. Data
2.4. TTE Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. RV-FWLS and RV Dysfunction
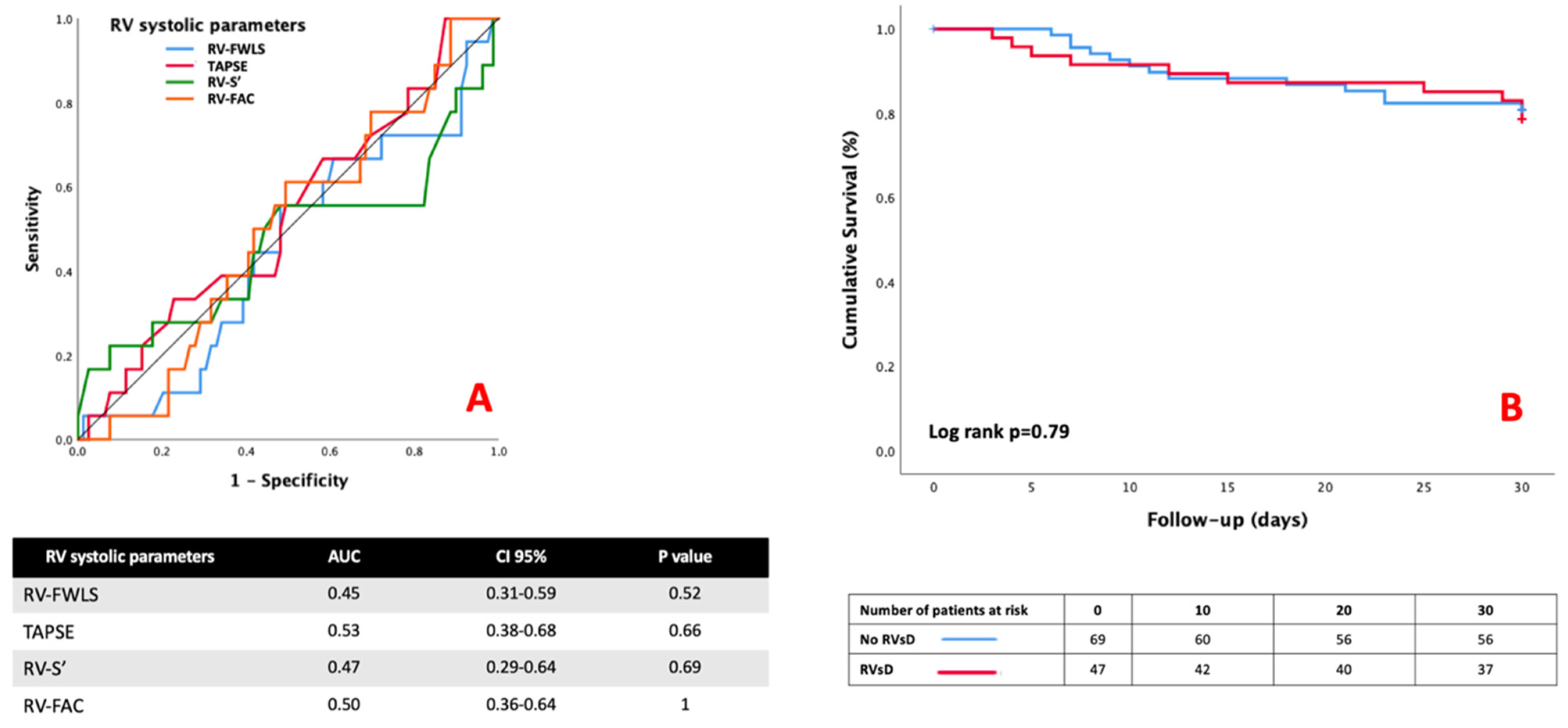
4.2. Performance of RV Parameters for Predicting 30-Day Mortality
4.3. RV-FWLS and 30-Day Mortality
4.4. Feasibility of RV-FWLS in Critically Ill Patients
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| ICC for Intra-Operator | CI 95% | ICC for Inter-Operator | CI 95% | |
|---|---|---|---|---|
| TAPSE | 0.97 | 0.80–0.99 | 0.95 | 0.94–0.98 |
| Onde S’ | 0.98 | 0.97–0.99 | 0.95 | 0.93–0.97 |
| RV-FAC | 0.79 | 0.64–0.96 | 0.80 | 0.68–0.96 |
| RV-FWLS | 0.87 | 0.55–0.97 | 0.84 | 0.57–0.96 |
References
- Bonnemain, J.; Ltaief, Z.; Liaudet, L. The Right Ventricle in COVID-19. JCM 2021, 10, 2535. [Google Scholar] [CrossRef] [PubMed]
- Corica, B.; Marra, A.M.; Basili, S.; Cangemi, R.; Cittadini, A.; Proietti, M.; Romiti, G.F. Prevalence of right ventricular dysfunction and impact on all-cause death in hospitalized patients with COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 17774. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, F.; Huang, S.; Herpain, A.; Balik, M.; Chew, M.S.; Clau-Terré, F.; Corredor, C.; De Backer, D.; Fletcher, N.; Geri, G.; et al. The PRICES statement: An ESICM expert consensus on methodology for conducting and reporting critical care echocardiography research studies. Intensive Care Med. 2021, 47, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Skulstad, H.; Cosyns, B.; Popescu, B.A.; Galderisi, M.; Salvo, G.D.; Donal, E.; Petersen, S.; Gimelli, A.; Haugaa, K.H.; Muraru, D.; et al. COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions, indications, prioritization, and protection for patients and healthcare personnel. Eur. Heart J.-Cardiovasc. Imaging 2020, 21, 592–598. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J.-Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Muraru, D.; Onciul, S.; Peluso, D.; Soriani, N.; Cucchini, U.; Aruta, P.; Romeo, G.; Cavalli, G.; Iliceto, S.; Badano, L.P. Sex- and Method-Specific Reference Values for Right Ventricular Strain by 2-Dimensional Speckle-Tracking Echocardiography. Circ. Cardiovasc. Imaging 2016, 9, e003866. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Li, H.; Zhu, S.; Xie, Y.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; Wu, C.; et al. Prognostic Value of Right Ventricular Longitudinal Strain in Patients with COVID-19. JACC Cardiovasc. Imaging 2020, 13, 2287–2299. [Google Scholar] [CrossRef]
- Gibson, L.E.; Di Fenza, R.; Lang, M.; Capriles, M.I.; Li, M.D.; Kalpathy-Cramer, J.; Little, B.P.; Arora, P.; Mueller, A.L.; Ichinose, F.; et al. Right Ventricular Strain Is Common in Intubated COVID-19 Patients and Does Not Reflect Severity of Respiratory Illness. J. Intensive Care Med. 2021, 36, 900–909. [Google Scholar] [CrossRef]
- Park, J.; Kim, Y.; Pereira, J.; Hennessey, K.C.; Faridi, K.F.; McNamara, R.L.; Velazquez, E.J.; Hur, D.J.; Sugeng, L.; Agarwal, V. Understanding the role of left and right ventricular strain assessment in patients hospitalized with COVID-19. Am. Heart J. Plus Cardiol. Res. Pract. 2021, 6, 100018. [Google Scholar] [CrossRef]
- Beyls, C.; Daumin, C.; Hermida, A.; Booz, T.; Ghesquieres, T.; Crombet, M.; Martin, N.; Huette, P.; Jounieaux, V.; Dupont, H.; et al. Association between the Right Ventricular Longitudinal Shortening Fraction and Mortality in Acute Respiratory Distress Syndrome Related to COVID-19 Infection: A Prospective Study. JCM 2022, 11, 2625. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, C.; Singh, S.; Garfield, B.; Morosin, M.; Surkova, E.; Mandalia, M.S.; Dias, B.; Androulakis, E.; Price, L.C.; McCabe, C.; et al. Right ventricular dysfunction in critically ill COVID-19 ARDS. Int. J. Cardiol. 2020, 327, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA J. Am. Med. Assoc. 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Nicoara, A.; Skubas, N.; Ad, N.; Finley, A.; Hahn, R.T.; Mahmood, F.; Mankad, S.; Nyman, C.B.; Pagani, F.; Porter, T.R.; et al. Guidelines for the Use of Transesophageal Echocardiography to Assist with Surgical Decision-Making in the Operating Room: A Surgery-Based Approach. J. Am. Soc. Echocardiogr. 2020, 33, 692–734. [Google Scholar] [CrossRef]
- Popescu, B.A.; Andrade, M.J.; Badano, L.P.; Fox, K.F.; Flachskampf, F.A.; Lancellotti, P.; Varga, A.; Sicari, R.; Evangelista, A.; Nihoyannopoulos, P.; et al. European Association of Echocardiography recommendations for training, competence, and quality improvement in echocardiography. Eur. J. Echocardiogr. 2009, 10, 893–905. [Google Scholar] [CrossRef] [Green Version]
- Fichet, J.; Moreau, L.; Genée, O.; Legras, A.; Mercier, E.; Garot, D.; Dequin, P.-F.; Perrotin, D. Feasibility of Right Ventricular Longitudinal Systolic Function Evaluation with Transthoracic Echocardiographic Indices Derived from Tricuspid Annular Motion: A Preliminary Study in Acute Respiratory Distress Syndrome: Longitudinal RV Function in ARDS. Echocardiography 2012, 29, 513–521. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Loo, J.; A Spittle, D.; Newnham, M. COVID-19, immunothrombosis and venous thromboembolism: Biological mechanisms. Thorax 2021, 76, 412–420. [Google Scholar] [CrossRef]
- Muraru, D.; Haugaa, K.; Donal, E.; Stankovic, I.; Voigt, J.-U.; E Petersen, S.; A Popescu, B.; Marwick, T. Right ventricular longitudinal strain in the clinical routine: A state-of-the-art review. Eur. Heart J.-Cardiovasc. Imaging 2022, 23, 898–912. [Google Scholar] [CrossRef]
- Soulat-Dufour, L.; Fauvel, C.; Weizman, O.; Barbe, T.; Pezel, T.; Mika, D.; Cellier, J.; Geneste, L.; Panagides, V.; Marsou, W.; et al. Prognostic value of right ventricular dilatation in patients with COVID-19: A multicentre study. Eur. Heart J.-Cardiovasc. Imaging 2021, 23, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Wibowo, A.; Pranata, R.; Astuti, A.; Tiksnadi, B.B.; Martanto, E.; Martha, J.W.; Purnomowati, A.; Akbar, M.R. Left and right ventricular longitudinal strains are associated with poor outcome in COVID-19: A systematic review and meta-analysis. J. Intensive Care 2021, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Nam, J.-H.; Son, J.-W.; Kim, S.O.; Son, N.-H.; Ahn, C.-M.; Shim, C.Y.; Hong, G.-R.; Kim, I.-C.; Choi, J.; et al. Cardiac Manifestations of Coronavirus Disease 2019 (COVID-19): A Multicenter Cohort Study. J. Korean Med. Sci. 2020, 35, e366. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.-U.; Cvijic, M. 2- and 3-Dimensional Myocardial Strain in Cardiac Health and Disease. JACC Cardiovasc. Imaging 2019, 12, 1849–1863. [Google Scholar] [CrossRef]
- Beyls, C.; Bohbot, Y.; Huette, P.; Booz, T.; Daumin, C.; Abou-Arab, O.; Mahjoub, Y. Usefulness of right ventricular longitudinal shortening fraction to detect right ventricular dysfunction in acute cor pulmonale related to COVID-19. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3594–3603. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, L.; Li, M.; Li, H.; Zhu, S.; Wang, B.; He, L.; Zhang, D.; Zhang, Y.; Yuan, H.; et al. Biventricular Longitudinal Strain Predict Mortality in COVID-19 Patients. Front. Cardiovasc. Med. 2021, 7, 632434. [Google Scholar] [CrossRef]
- Gil-Rodríguez, J.; de Rojas, J.P.; Aranda-Laserna, P.; Benavente-Fernández, A.; Martos-Ruiz, M.; Peregrina-Rivas, J.-A.; Guirao-Arrabal, E. Ultrasound findings of lung ultrasonography in COVID-19: A systematic review. Eur. J. Radiol. 2022, 148, 110156. [Google Scholar] [CrossRef]
- Cameli, M.; Bernazzali, S.; Lisi, M.; Tsioulpas, C.; Croccia, M.; Lisi, G.; Maccherini, M.; Mondillo, S. Right Ventricular Longitudinal Strain and Right Ventricular Stroke Work Index in Patients With Severe Heart Failure: Left Ventricular Assist Device Suitability for Transplant Candidates. Transplant. Proc. 2012, 44, 2013–2015. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Toulouse, E.; Masseguin, C.; Lafont, B.; McGurk, G.; Harbonn, A.; A Roberts, J.; Granier, S.; Dupeyron, A.; Bazin, J.E. French legal approach to clinical research. Anaesth. Crit. Care Pain Med. 2018, 37, 607–614. [Google Scholar] [CrossRef] [Green Version]



| Variables | No RVsD (n = 69) | RVsD (n = 47) | p |
|---|---|---|---|
| Age (years) | 60 (59–68) | 62 (59–73) | 0.39 |
| BMI (kg m−2) | 30.4 (25.7–34.1) | 30.2 (26.6–34.9) | 0.67 |
| Male gender (n; %) | 45 (65) | 33 (70) | 0.68 |
| SAPS II score | 32 (20–56) | 39 (24–61) | 0.29 |
| Medical history | |||
| No history | 10 (14) | 7 (15) | 0.99 |
| Hypertension | 34 (49) | 24 (51) | 0.99 |
| Diabetes | 16 (23) | 14 (30) | 0.51 |
| Dyslipidemia | 18 (26) | 18 (38) | 0.22 |
| Smoking (former or active) | 12 (17) | 10 (21) | 0.63 |
| Chronic renal disease | 5 (7) | 5 (10 | 0.52 |
| COPD/asthma | 16 (23) | 4 (9) | 0.08 |
| Coronary or peripheral artery disease | 4 (6) | 7 (15) | 0.17 |
| Valvular heart disease | 2 (3) | 5 (10) | 0.12 |
| CT scan (n = 107/116) | 62 (89) | 45 (95) | |
| Frosted glass | 59 (95) | 44 (97) | 0.63 |
| Consilodation | 37 (62) | 27 (64) | 0.99 |
| Crazy Paving | 19 (32) | 9 (22) | 0.36 |
| Lung involvement > 50% | 30 (43) | 22 (46) | 0.99 |
| Pulmonary embolism | 1 (2) | 4 (9) | 0.15 |
| Biological data before TTE | |||
| Lactate (mmol−1) | 1.7 (1.3–2.1) | 1.9 (1.3–2.3) | 0.16 |
| Serum creatinine (µmol L−1) | 66 (54–88) | 70 (54–88) | 0.61 |
| BNP (pg mL−1) | 59 (31–101) | 79 (34–243) | 0.12 |
| Troponin Tc HS (ng mL−1) | 16 (6–36) | 27 (8–95) | 0.06 |
| Procalcitonin (µg L−1) | 0.40 (0.18–0.75) | 0.57 (0.13–1.60) | 0.47 |
| C reactive protein (mg L−1) | 150 (96–215) | 160 (84–268) | 0.62 |
| Time to first symptom to ICU admission (days) | 8 (5–10) | 8 (6–12) | 0.44 |
| Period of hospitalization in ICU * | |||
| 16 (23) | 9 (19) | 0.65 |
| 13 (19) | 6 (13) | 0.45 |
| 40 (58) | 32 (68) | 0.33 |
| No RVsD (n = 69) | RVsD (n = 47) | p | |
|---|---|---|---|
| Hemodynamic parameters during TTE | |||
| Heart rate (bpm) | 82 (74–92) | 87 (74–102) | 0.14 |
| Systolic arterial pressure (mmHg) | 130 (114–144) | 127 (113–146) | 0.71 |
| Mean arterial pressure (mmHg) | 86 (73–97) | 86 (80–95) | 0.53 |
| Diastolic arterial pressure (mmHg) | 70 (58–80) | 69 (61–79) | 0.44 |
| Mechanical ventilation, n (%) | 37 (54) | 32 (70) | 0.12 |
| PaO2 (mmHg) | 76 (65–92) | 80 (71–107) | 0.12 |
| Vasopressor use, n (%) | 19 (27) | 13 (28) | 0.99 |
| TTE parameters | |||
| RV basal dimension (mm) | 45 (40–51) | 44 (38–50) | 0.21 |
| RV mid-cavity dimension (mm) | 38 (29–43) | 37 (32–41) | 0.54 |
| RV longitudinal dimension (mm) | 77 (69–85) | 76 (70–84) | 0.83 |
| RV EDA (cm2) | 21 (16–26) | 21 (17–24) | 0.94 |
| RV ESA (cm2) | 11 (7–14) | 11 (9.5–15) | 0.23 |
| RV EDA/LV EDA | 0.68 (0.55–0.92) | 0.67 (0.57–0.87) | 0.91 |
| Acute cor pulmonale, n (%) | 18 (26) | 18 (38) | 0.22 |
| RA volume (mL) | 33 (27–35) | 32 (27–40) | 0.63 |
| RA area (cm2) | 14.6 (9.6–19.2) | 14.6 (7.1–20.5) | 0.61 |
| Left ventricular ejection fraction (%) | 64 (53–70) | 63 (53–73) | 0.57 |
| RV Systolic Function Parameters | |||
| TAPSE (mm) | 24 (21–27) | 21 (19–25) | 0.03 |
| RV-S’ (cm s−1) | 16 (13–19) | 16 (13–19) | 0.91 |
| RV-FAC (%) | 47 (41–54) | 41 (34–47) | 0.006 |
| RV-FWLS (%) | 26.7 (24.1–30.1) | 17.5 (15.3–19.0) | 0.0001 |
| Outcomes (n,%) | |||
| Ventilator acquired pneumonia | 34 (49) | 28 (61) | 0.56 |
| Renal replacement therapy | 10 (14) | 7 (15) | 0.99 |
| Pulmonary embolism | 4 (6) | 5 (11) | 0.48 |
| Cardiogenic shock | 3 (4) | 6 (13) | 0.15 |
| Veno-venous ECMO | 8 (12) | 4 (9) | 0.76 |
| Tracheotomy | 10 (15) | 3 (7) | 0.23 |
| Time under mechanical ventilation (days) | 18 (11–30) | 18 (10–27) | 0.47 |
| 30-day mortality | 13 (19) | 10 (21) | 0.82 |
| ICU mortality | 17 (25) | 10 (21) | 0.81 |
| ICU stay (days) | 11 (6–29) | 17 (7–31) | 0.27 |
| Variables | 30 Days Mortality | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| HR (95%CI) | p | HR (95%CI) | p | |
| SAPS II (for each point) | 1.03 (1.01–1.05) | 0.02 | 1.04 (1.01–1.06) | 0.005 |
| Age > 65 years old | 5.01 (2.10–12.37) | 0.001 | 7.51 (2.63–21.44) | 0.0001 |
| Mechanical ventilation * | 1.41 (0.57–3.46) | 0.45 | - | - |
| RV-FWLS < 21% | 1.12 (0.49–2.55) | 0.78 | - | - |
| Acute cor pulmonale * | 3.48 (1.48–8.14) | 0.004 | 7.53 (2.58–21.9) | 0.0001 |
| Pulmonary embolism before TTE | 0.91 (0.12–6.77) | 0.92 | - | - |
| SOFA cv * | 1.47 (0.61–3.51) | 0.38 | - | - |
| Period of inclusion | ||||
| 0.54 (0.24–2.11) | 0.72 | - | - |
| 0.72 (0.21–2.41) | 0.59 | - | - |
| 1.15 (0.62–3.68) | 0.36 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beyls, C.; Ghesquières, T.; Hermida, A.; Booz, T.; Crombet, M.; Martin, N.; Huette, P.; Jounieaux, V.; Dupont, H.; Abou-Arab, O.; et al. Feasibility, Prediction and Association of Right Ventricular Free Wall Longitudinal Strain with 30-Day Mortality in Severe COVID-19 Pneumonia: A Prospective Study. J. Clin. Med. 2022, 11, 3629. https://doi.org/10.3390/jcm11133629
Beyls C, Ghesquières T, Hermida A, Booz T, Crombet M, Martin N, Huette P, Jounieaux V, Dupont H, Abou-Arab O, et al. Feasibility, Prediction and Association of Right Ventricular Free Wall Longitudinal Strain with 30-Day Mortality in Severe COVID-19 Pneumonia: A Prospective Study. Journal of Clinical Medicine. 2022; 11(13):3629. https://doi.org/10.3390/jcm11133629
Chicago/Turabian StyleBeyls, Christophe, Tristan Ghesquières, Alexis Hermida, Thomas Booz, Maxime Crombet, Nicolas Martin, Pierre Huette, Vincent Jounieaux, Hervé Dupont, Osama Abou-Arab, and et al. 2022. "Feasibility, Prediction and Association of Right Ventricular Free Wall Longitudinal Strain with 30-Day Mortality in Severe COVID-19 Pneumonia: A Prospective Study" Journal of Clinical Medicine 11, no. 13: 3629. https://doi.org/10.3390/jcm11133629
APA StyleBeyls, C., Ghesquières, T., Hermida, A., Booz, T., Crombet, M., Martin, N., Huette, P., Jounieaux, V., Dupont, H., Abou-Arab, O., & Mahjoub, Y. (2022). Feasibility, Prediction and Association of Right Ventricular Free Wall Longitudinal Strain with 30-Day Mortality in Severe COVID-19 Pneumonia: A Prospective Study. Journal of Clinical Medicine, 11(13), 3629. https://doi.org/10.3390/jcm11133629