
Expert Multinational Consensus Statement for Total Intravenous Anaesthesia (TIVA) Using the Delphi Method †

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Methods
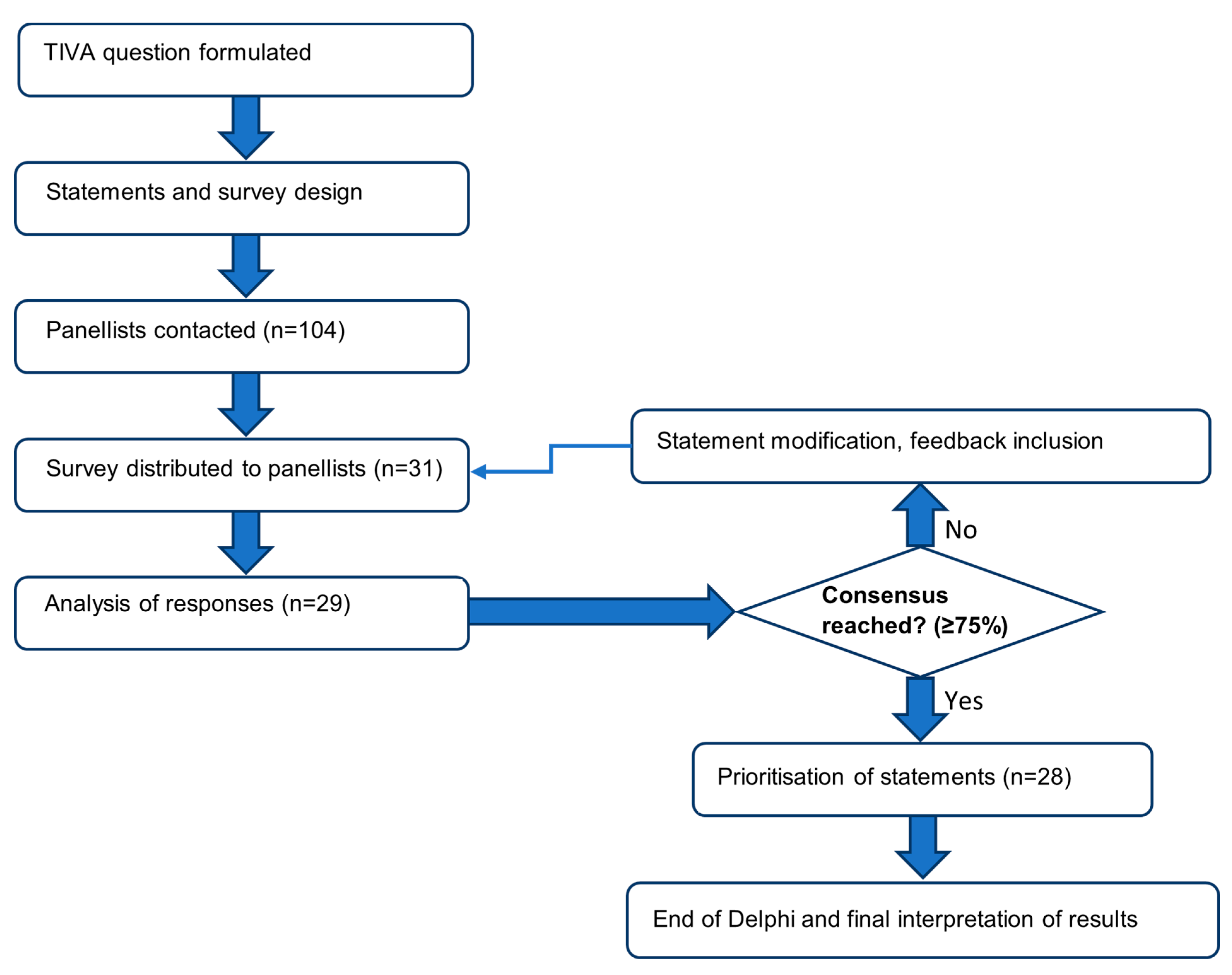
2.1. Model
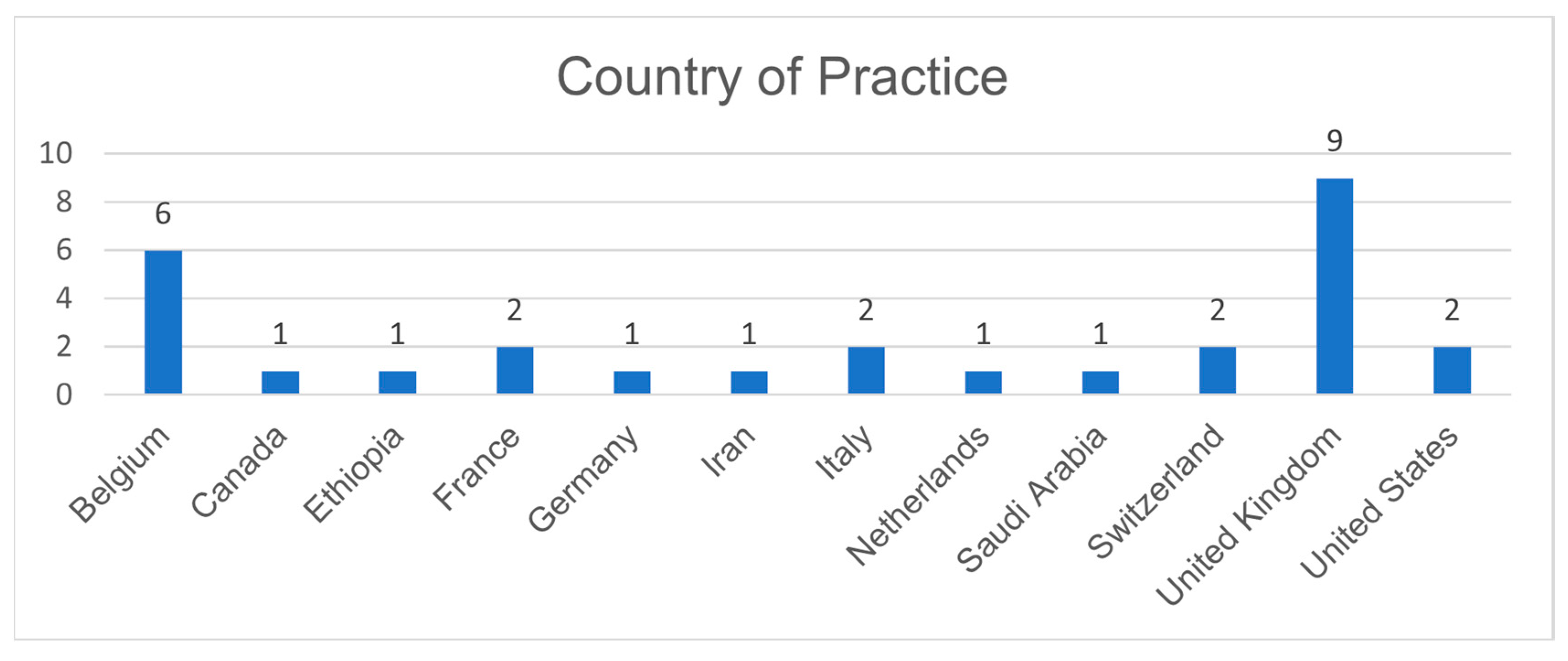
2.2. Panellist Recruitment
2.3. Statements
2.4. Survey Design and Data Collection
2.5. Data Analysis
2.6. Ethical Review
3. Results
3.1. Round 1
3.2. Round 2
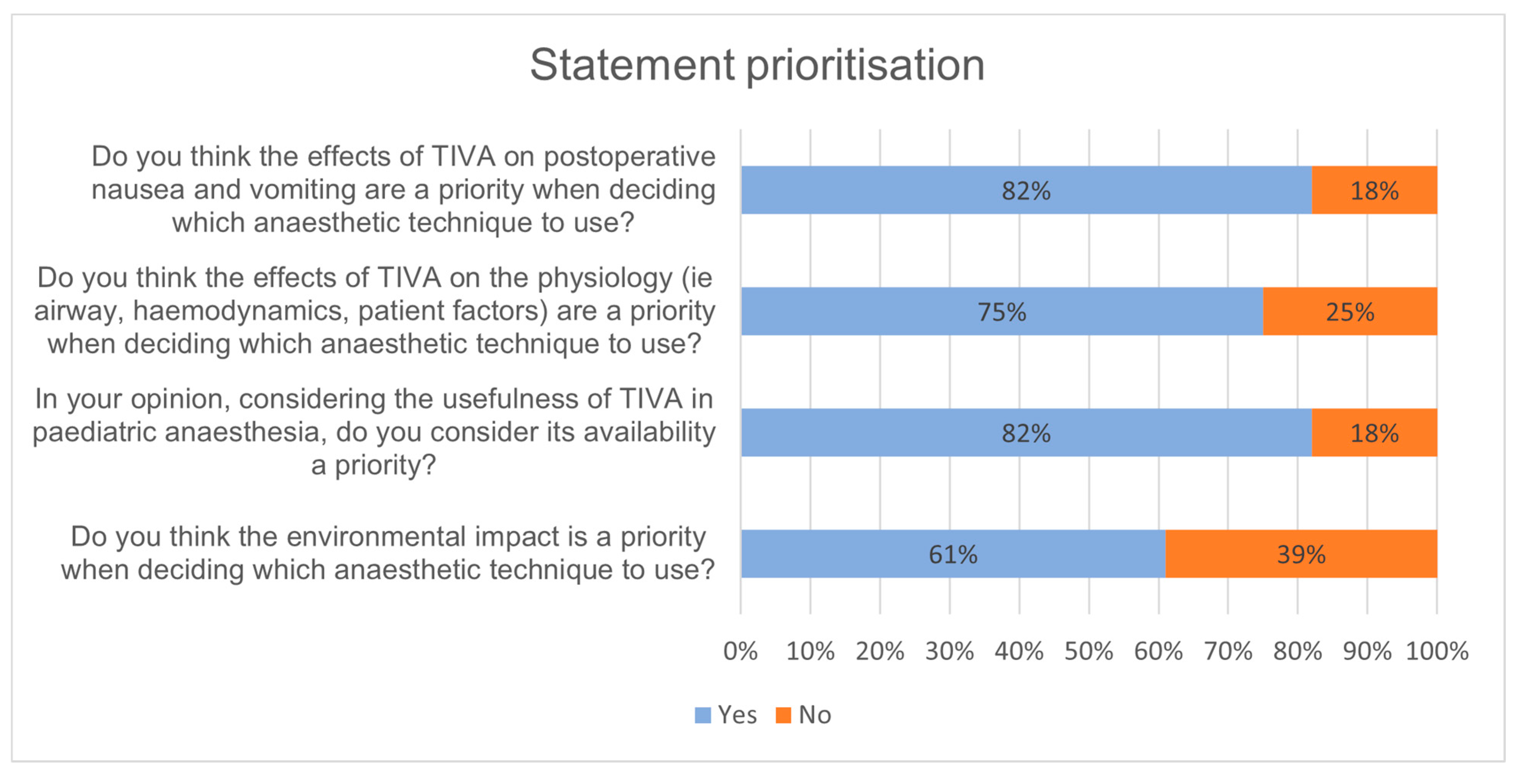
3.3. Round 3
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Panellists’ Fields of Interest | No. |
|---|---|
| Airway Management | 1 |
| Ambulatory Anaesthesia | 1 |
| Burn Care | 1 |
| Cardiothoracic Anaesthesia | 1 |
| Cardiovascular Anaesthesia | 4 |
| Critical/Intensive Care | 4 |
| Education and Teaching | 2 |
| Emergency Anaesthesia | 1 |
| General Anaesthesia | 5 |
| Locoregional Anaesthesia | 1 |
| Malignant Hyperthermia | 2 |
| Myopathies | 1 |
| Neuro-Anaesthesia | 3 |
| Neuromuscular Blockers and Monitoring | 1 |
| Non-Operating Room Anaesthesia | 3 |
| Not specified | 2 |
| Obstetric Anaesthesia | 3 |
| Onco-Anaesthesia | 1 |
| Opioid-Free Anaesthesia | 1 |
| Orthopaedics | 2 |
| Paediatric Anaesthesia | 2 |
| Pain Management | 5 |
| Quality and Safety | 1 |
| Regional Anaesthesia | 5 |
| Total Intravenous Anaesthesia | 1 |
| Transfusions | 1 |
| Vascular Anaesthesia | 1 |
Appendix B
| Statement 1. | Round 1: Whether the use of total intravenous anaesthesia may have benefits over volatile anaesthesia for reducing greenhouse gases and waste anaesthetic gases is important for me. | 82.8% |
| Round 2: Statement unmodified. | 89.6% | |
| Statement 2 | Round 1: There is a strong body of evidence supporting the use of total intravenous anaesthesia for reducing the incidence of emergence agitation compared with volatile anaesthesia. | 62.1% |
| Round 2: Statement unmodified. | 68.9% | |
| Round 3: In paediatric anaesthesia, there is a strong body of evidence supporting the use of total intravenous anaesthesia for reducing the incidence of emergence agitation compared with volatile anaesthesia. | 74.1% | |
| Statement 3 | Round 1: The potential effect of total intravenous anaesthesia on cancer biology is an important aspect for me. | 51.7% |
| Round 2: Statement unmodified. | 53.6% | |
| Statement 4 | Round 1: In paediatric anaesthesia, total intravenous anaesthesia is an impractical technique compared with volatile anaesthesia. | 34.4% |
| Round 2: In paediatric and adult anaesthesia, practicality aspects (e.g., changing syringes, local resources and availability of drugs, pumps and anaesthesia monitoring, duration and type of procedure) influence the use of TIVA compared with volatile anaesthesia. | 64.3% | |
| Statement 5 | Round 1: In paediatric anaesthesia, total intravenous anaesthesia is a useful technique. | 79.3% |
| Round 2: Statement unmodified. | 82.7% | |
| Statement 6 | Round 1: The risk of awareness during total intravenous anaesthesia compared with volatile anaesthesia is an obstacle for its use. | 20.6% |
| Round 2: Statement unmodified. | 21.5% | |
| Statement 7 | Round 1: The financial cost of the anaesthetic technique in the context of total intravenous anaesthesia and volatile anaesthesia is important for me. | 44.8% |
| Round 2: Statement unmodified. | 50% | |
| Statement 8 | Round 1: Departmental preferences and guidelines influence my technique choice, in the context of total intravenous anaesthesia versus volatile anaesthesia. | 44.8% |
| Round 2: Departmental preferences, resistance to change, or guidelines influence my (or colleagues’) technique choice, in the context of total intravenous anaesthesia versus volatile anaesthesia. | 53.6% | |
| Statement 9 | Round 1: Lack of familiarity and/or training with the use of total intravenous anaesthesia (compared with volatile anaesthesia) is a key reason why myself, or colleagues I know, do not use it. | 41.4% |
| Round 2: Statement unmodified. | 46.4% | |
| Statement 10 | Round 1: The effects of total intravenous anaesthesia on the physiology (airway, haemodynamics) influence my technique choice when compared with volatile anaesthesia. | 55.1% |
| Round 2: My technique choice is influenced by the effects of TIVA on the physiology such as airway, haemodynamics, or other patient related factors (not including malignant hyperthermia, which is universally considered an absolute contraindication for the use of volatile agents). | 75.8% | |
| Statement 11 | Round 1: The effect of total intravenous anaesthesia on postoperative nausea and vomiting risk influences my choice. | 79.3% |
| Round 2: Statement unmodified. | 86.2% | |
| Statement 12 | Round 1: Total intravenous anaesthesia is becoming more widely used in my clinical practice or the clinical practice of my department. | 62.1% |
| Round 2: The use of total intravenous anaesthesia is in expansion in my clinical practice or the clinical practice of my department, where not already widely used. | 60.7% |
References
- Nimmo, A.F.; Absalom, A.; Bagshaw, O.; Biswas, A.; Cook, T.M.; Costello, A.; Grimes, S.; Mulvey, D.; Shinde, S.; Whitehouse, T.; et al. Guidelines for the safe practice of total intravenous anaesthesia (TIVA): Joint Guidelines from the Association of Anaesthetists and the Society for Intravenous Anaesthesia. Anaesthesia 2018, 74, 211–224. Available online: https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.14428 (accessed on 14 December 2021). [CrossRef] [PubMed] [Green Version]
- Sherman, J.; Le, C.; Lamers, V.; Eckelman, M. Life cycle greenhouse gas emissions of anesthetic drugs. Anesth. Analg. 2012, 114, 1086–1090. Available online: https://journals.lww.com/anesthesia-analgesia/Fulltext/2012/05000/Life_Cycle_Greenhouse_Gas_Emissions_of_Anesthetic.25.aspx (accessed on 2 November 2021). [CrossRef] [PubMed]
- Koch, S.; Pecher, S. Neue Herausforderungen für die Anästhesie durch den Klimawandel [New challenges for anesthesia due to the climate change]. Anaesthesist 2020, 69, 453–462. Available online: https://link.springer.com/article/10.1007/s00101-020-00770-1 (accessed on 2 November 2021). [CrossRef] [PubMed]
- Jo, J.Y.; Jung, K.W.; Kim, H.J.; Park, S.U.; Park, H.; Ku, S.; Choi, S.S. Effect of Total Intravenous Anesthesia vs Volatile Induction with Maintenance Anesthesia on Emergence Agitation after Nasal Surgery: A Randomized Clinical Trial. AMA Otolaryngol.-Head Neck Surg. 2019, 145, 117–123. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6440219/ (accessed on 2 November 2021). [CrossRef] [PubMed]
- Talih, G.; Yüksek, A.; Şahin, E. Evaluation of emergence agitation after general anaesthesia in rhinoplasty patients: Inhalation anaesthesia versus total intravenous anaesthesia. Am. J. Otolaryngol. 2020, 41, 102387. Available online: https://www.sciencedirect.com/science/article/pii/S0196070919311378 (accessed on 2 November 2021). [CrossRef] [PubMed]
- Wigmore, T.J.; Mohammed, K.; Jhanji, S. Long-term survival for patients undergoing volatile versus IV anesthesia for cancer surgery: A retrospective analysis. Anesthesiology 2016, 124, 69–79. Available online: https://pubs.asahq.org/anesthesiology/article/124/1/69/14249/Long-term-Survival-for-Patients-Undergoing (accessed on 2 November 2021). [CrossRef] [PubMed]
- Yap, A.; Lopez-Olivo, M.A.; Dubowitz, J.; Hiller, J.; Riedel, B.; Global Onco-Anesthesia Research Collaboration Group. Anesthetic technique and cancer outcomes: A meta-analysis of total intravenous versus volatile anesthesia. Can. J. Anaesth. 2019, 66, 546–561. Available online: https://pubmed.ncbi.nlm.nih.gov/30834506/ (accessed on 2 November 2021). [CrossRef] [PubMed] [Green Version]
- Chang, C.Y.; Wu, M.Y.; Chien, Y.J.; Su, I.M.; Wang, S.C.; Kao, M.C. Anesthesia and Long-term Oncological Outcomes: A Systematic Review and Meta-analysis. Anesth Analg. 2021, 132, 623–634. Available online: https://oce.ovid.com/article/00000539-202103000-00006/HTML (accessed on 14 December 2021). [CrossRef] [PubMed]
- Grundmann, U.; Uth, M.; Eichner, A.; Wilhelm, W.; Larsen, R. Total intravenous anaesthesia with propofol and remifentanil in paediatric patients: A comparison with a desflurane-nitrous oxide inhalation anaesthesia. Acta Anaesthesiol. Scand. 1998, 42, 845–850. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1399-6576.1998.tb05332.x?saml_referrer (accessed on 2 November 2021). [CrossRef] [PubMed]
- Anderson, B.J.; Bagshaw, O. Practicalities of Total Intravenous Anesthesia and Target-controlled Infusion in Children. Anesthesiology 2019, 131, 164–185. Available online: https://pubs.asahq.org/anesthesiology/article/131/1/164/18098/Practicalities-of-Total-Intravenous-Anesthesia-and (accessed on 2 November 2021). [CrossRef] [PubMed]
- Hill, M.; Peat, W.; Courtman, S. A national survey of propofol infusion use by paediatric anaesthetists in Great Britain and Ireland. Pediatr. Anesth. 2008, 18, 488–493. Available online: https://onlinelibrary.wiley.com/doi/10.1111/j.1460-9592.2008.02459.x (accessed on 14 December 2021). [CrossRef] [PubMed]
- Lauder, G.R.; Thomas, M.; von Ungern-Sternberg, B.S.; Engelhardt, T. Volatiles or TIVA: Which is the standard of care for pediatric airway procedures? A pro-con discussion. Pediatr. Anesth. 2020, 30, 209–220. Available online: https://onlinelibrary.wiley.com/doi/10.1111/pan.13809 (accessed on 16 December 2021). [CrossRef] [PubMed]
- Lauder, G.R. Total intravenous anesthesia will supercede inhalational anesthesia in pediatric anesthetic practice. Pediatric Anesth. 2015, 25, 52–64. Available online: https://onlinelibrary.wiley.com/doi/10.1111/pan.12553 (accessed on 2 November 2021). [CrossRef] [PubMed]
- Smith, I. Total Intravenous Anaesthesia. CNS Drugs 2003, 17, 609–619. Available online: https://link.springer.com/article/10.2165/00023210-200317090-00001 (accessed on 2 November 2021). [CrossRef] [PubMed]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. Available online: https://journals.sagepub.com/doi/10.1177/0269216317690685?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed (accessed on 23 November 2021). [CrossRef] [PubMed] [Green Version]
- Forget, P.; Patullo, C.; Hill, D.; Ambekar, A.; Baldacchino, A.; Cata, J.; Chetty, S.; Cox, F.J.; de Boer, H.D.; Dinwoodie, K.; et al. System-level policies on appropriate opioid use, a multi-stakeholder consensus. BMC Health Serv. Res. 2022, 22, 329. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2700030/ (accessed on 14 December 2021). [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. REDCap Consortium, The REDCap consortium: Building an international community of software partners. J. Biomed. Inform. 2019, 95, 103208. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7254481/ (accessed on 16 December 2021). [CrossRef] [PubMed]
- REDCap. Citations. 2021. Available online: https://projectredcap.org/resources/citations/ (accessed on 16 December 2021).



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uitenbosch, G.; Sng, D.; Carvalho, H.N.; Cata, J.P.; De Boer, H.D.; Erdoes, G.; Heytens, L.; Lois, F.J.; Rousseau, A.-F.; Pelosi, P.; et al. Expert Multinational Consensus Statement for Total Intravenous Anaesthesia (TIVA) Using the Delphi Method . J. Clin. Med. 2022, 11, 3486. https://doi.org/10.3390/jcm11123486
Uitenbosch G, Sng D, Carvalho HN, Cata JP, De Boer HD, Erdoes G, Heytens L, Lois FJ, Rousseau A-F, Pelosi P, et al. Expert Multinational Consensus Statement for Total Intravenous Anaesthesia (TIVA) Using the Delphi Method . Journal of Clinical Medicine. 2022; 11(12):3486. https://doi.org/10.3390/jcm11123486
Chicago/Turabian StyleUitenbosch, Giulia, Daniel Sng, Hugo N. Carvalho, Juan P. Cata, Hans D. De Boer, Gabor Erdoes, Luc Heytens, Fernande Jane Lois, Anne-Françoise Rousseau, Paolo Pelosi, and et al. 2022. "Expert Multinational Consensus Statement for Total Intravenous Anaesthesia (TIVA) Using the Delphi Method " Journal of Clinical Medicine 11, no. 12: 3486. https://doi.org/10.3390/jcm11123486
APA StyleUitenbosch, G., Sng, D., Carvalho, H. N., Cata, J. P., De Boer, H. D., Erdoes, G., Heytens, L., Lois, F. J., Rousseau, A. -F., Pelosi, P., Forget, P., & Nesvadba, D. (2022). Expert Multinational Consensus Statement for Total Intravenous Anaesthesia (TIVA) Using the Delphi Method . Journal of Clinical Medicine, 11(12), 3486. https://doi.org/10.3390/jcm11123486