
Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors

 ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data Collection
2.3. Online Questionnaires
2.4. Data and Statistical Analysis
3. Results
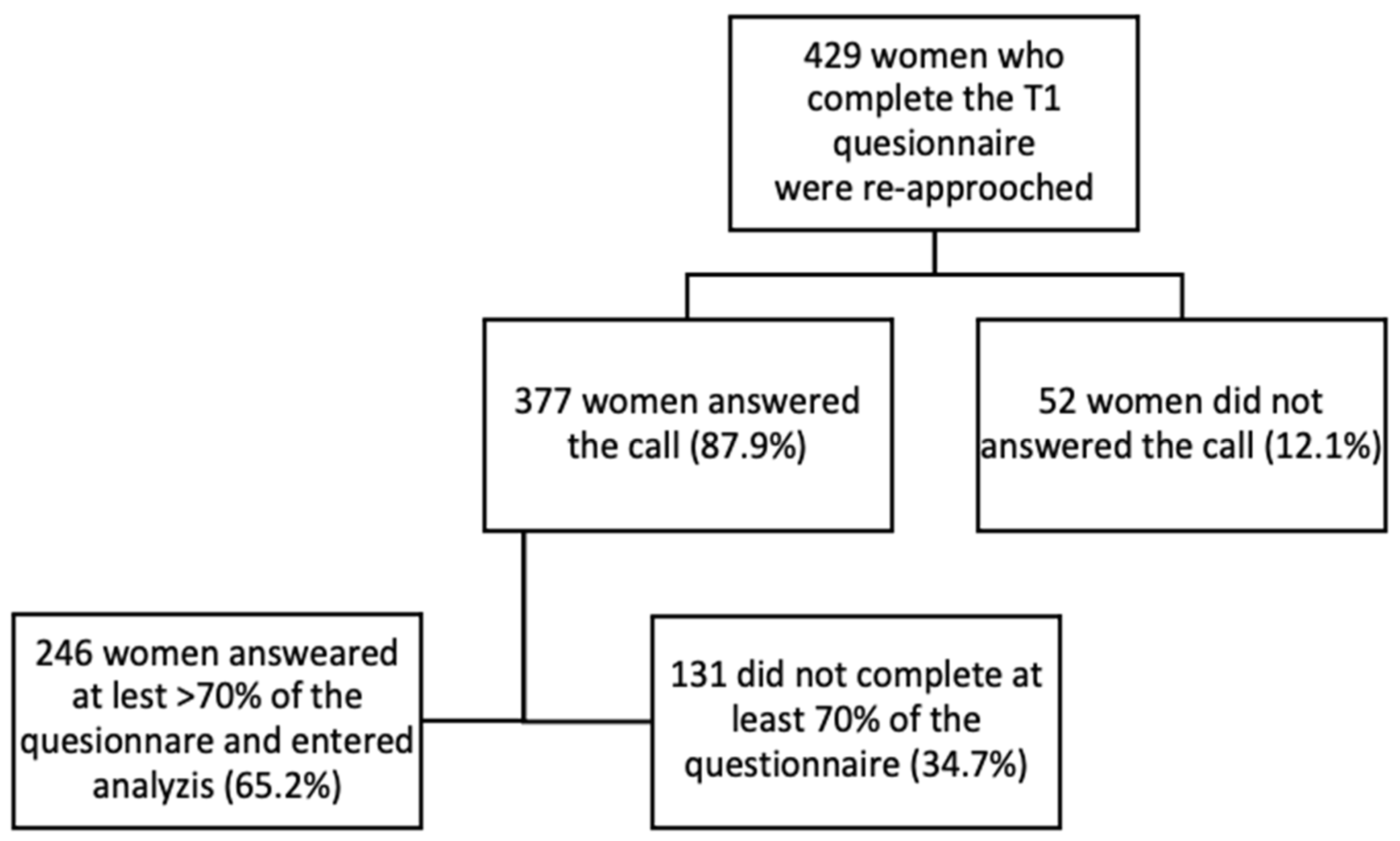
3.1. Study Population
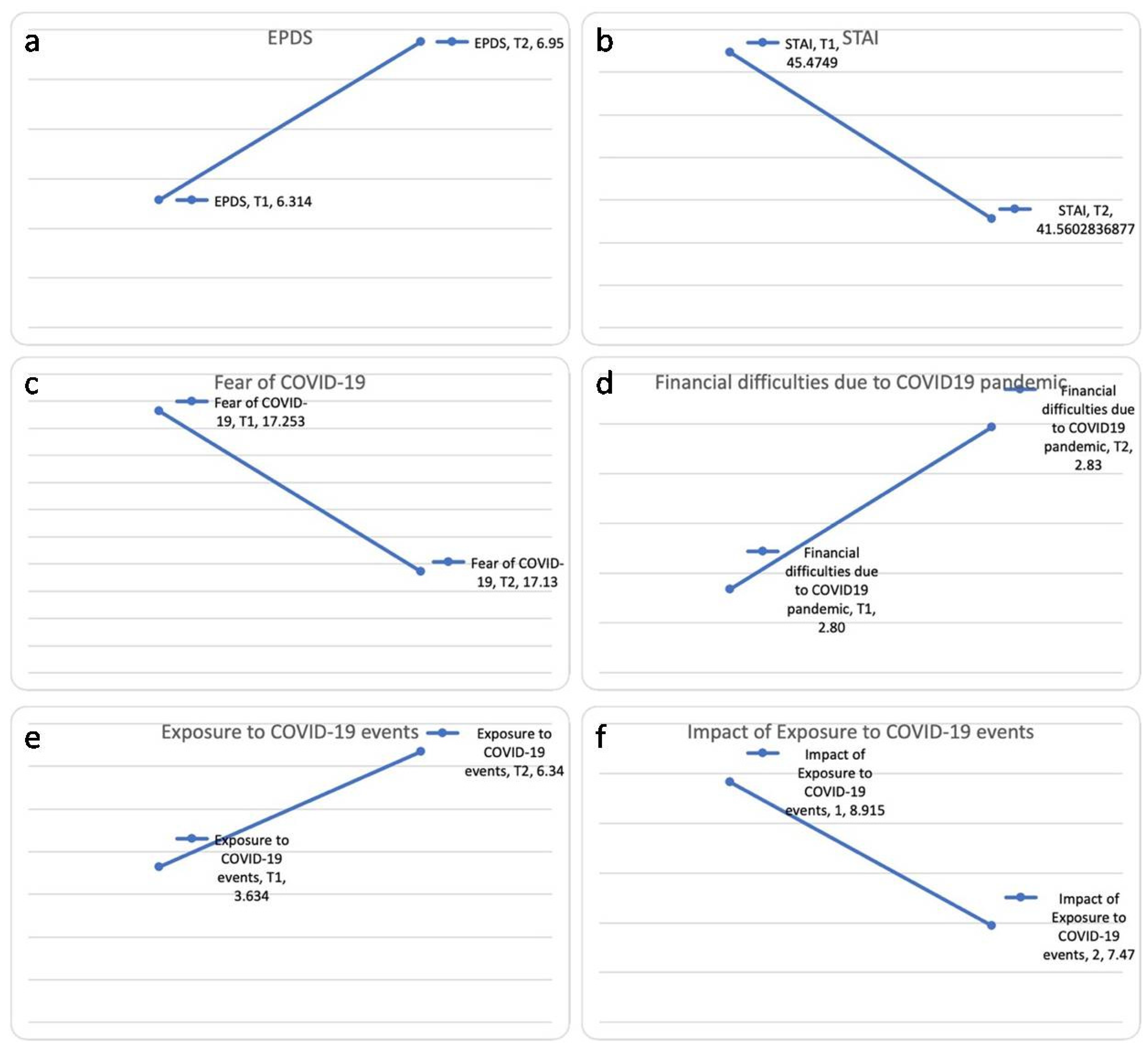
3.2. PPD Symptoms and COVID-19 Related Questionnaires
3.3. PPD Symptoms and Other Control Variables
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kontoangelos, K.; Economou, M.; Papageorgiou, C. Mental Health Effects of COVID-19 Pandemia: A Review of Clinical and Psychological Traits. Psychiatry Investig. 2020, 17, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Hamel, L.; Kearney, A.; Kirzinger, A.; Lopes, L.; Muñana, C.; Brodie, M. Health Tracking Poll–June 2020. Available online: https://www.kff.org/report-section/kff-health-tracking-poll-june-2020-social-distancing-delayed-health-care-and-a-look-ahead-to-the-2020-election/ (accessed on 21 June 2021).
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Nanjundaswamy, M.H.; Shiva, L.; Desai, G.; Ganjekar, S.; Kishore, T.; Ram, U.; Satyanarayana, V.; Thippeswamy, H.; Chandra, P.S. COVID-19-related anxiety and concerns expressed by pregnant and postpartum women-a survey among obstetricians. Arch. Women’s Ment. Health 2020, 23, 787–790. [Google Scholar] [CrossRef]
- Payne, J.L. Depression: Is pregnancy protective? J. Women’s Health 2012, 21, 809–810. [Google Scholar] [CrossRef]
- Hendrick, V.; Altshuler, L.L.; Suri, R. Hormonal changes in the postpartum and implications for postpartum depression. Psychosomatics 1998, 39, 93–101. [Google Scholar] [CrossRef]
- Vieira, L.G.; Camargo, E.L.J.S.; Schneider, G.; da Silva, G.P.R.; Thomazini, M.; Possani, M.A.; Matioli, M.R.; de Sousa Ibiapina, A.R. Repercussions of the COVID-19 pandemic on the mental health of pregnant and puerperal women: A systematic review. MedRxiv 2020. [Google Scholar] [CrossRef]
- Coxon, K.; Turienzo, C.F.; Kweekel, L.; Goodarzi, B.; Brigante, L.; Simon, A.; Lanau, M.M. The impact of the coronavirus (COVID-19) pandemic on maternity care in Europe. Midwifery 2020, 88, 102779. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.R.; Bloom, N.; Davis, S.J.; Terry, S.J. COVID-Induced Economic Uncertainty; NBER Working Papers 26983; National Bureau of Economic Research, Inc.: Cambridge, MA, USA, 2020. [Google Scholar]
- Salehi, L.; Rahimzadeh, M.; Molaei, E.; Zaheri, H.; Esmaelzadeh-Saeieh, S. The relationship among fear and anxiety of COVID-19, pregnancy experience, and mental health disorder in pregnant women: A structural equation model. Brain Behav. 2020, 10, e01835. [Google Scholar] [CrossRef] [PubMed]
- Haruna, M.; Nishi, D. Perinatal mental health and COVID-19 in Japan. Psychiatry Clin. Neurosci. 2020, 74, 502–503. [Google Scholar] [CrossRef] [PubMed]
- Gluska, H.; Mayer, Y.; Shiffman, N.; Daher, R.; Elyasyan, L.; Elia, N.; Weiner, M.S.; Miremberg, H.; Kovo, M.; Biron-Shental, T.; et al. The use of personal protective equipment as an independent factor for developing depressive and post-traumatic stress symptoms in the postpartum period. Eur. Psychiatry 2021, 64, e34. [Google Scholar] [CrossRef]
- Ravaldi, C.; Wilson, A.; Ricca, V.; Homer, C.; Vannacci, A. Pregnant women voice their concerns and birth expectations during the COVID-19 pandemic in Italy. Women Birth. 2021, 34, 335–343. [Google Scholar] [CrossRef]
- Polachek, I.S.; Harari, L.H.; Baum, M.; Strous, R.D. Postpartum post-traumatic stress disorder symptoms: The uninvited birth companion. Isr. Med. Assoc. J. 2012, 14, 347–353. [Google Scholar]
- Gluska, H.; Shiffman, N.; Mayer, Y.; Elyasyan, L.; Elia, N.; Daher, R.; Weiner, M.S.; Miremberg, H.; Kovo, M.; Biron-Shental, T.; et al. Maternal fear of COVID-19 and prevalence of postnatal depression symptoms, risk and protective factors. J. Psychiatr. Res. 2022, 148, 214–219. [Google Scholar] [CrossRef]
- Creedy, D.K.; Shochet, I.M.; Horsfall, J. Childbirth and the development of acute trauma symptoms: Incidence and contributing factors. Birth 2000, 27, 104–111. [Google Scholar] [CrossRef]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Fetal Neonatal Med. 2022, 35, 205–211. [Google Scholar] [CrossRef]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13, published correction appears in J. Affect. Disord. 2021, 279, 377–379. [Google Scholar] [CrossRef]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, M.; Horiguchi, H. The COVID-19 Pandemic and Mental Well-Being of Pregnant Women in Japan: Need for Economic and Social Policy Interventions. Disaster Med. Public Health Prep. 2020, 16, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Oskovi-Kaplan, Z.A.; Buyuk, G.N.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Ozbas, A.; Moraloglu Tekin, O. The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: A Preliminary Study. Psychiatr. Q. 2021, 92, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Zanardo, V.; Manghina, V.; Giliberti, L.; Vettore, M.; Severino, L.; Straface, G. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int. J. Gynaecol. Obstet. 2020, 150, 184–188. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Psychological distress and adaptation to the COVID-19 crisis in the United States. J. Psychiatr. Res. 2021, 136, 603–609. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Barouki, R.; Kogevinas, M.; Audouze, K.; Belesova, K.; Bergman, A.; Birnbaum, L.; Boekhold, S.; Denys, S.; Desseille, C.; Drakvik, E. The COVID-19 pandemic and global environmental change: Emerging research needs. Environ. Int. 2021, 146, 106272. [Google Scholar] [CrossRef]
- Moraes, G.P.; Lorenzo, L.; Pontes, G.A.; Montenegro, M.C.; Cantilino, A. Screening and diagnosing postpartum depression: When and how? Trends Psychiatry Psychother. 2017, 39, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, J.; Holden, J. Perinatal Mental Health: A Guide to the Edinburgh Postnatal Depression Scale (EPDS); Royal College of Psychiatrists: London, UK, 2003. [Google Scholar]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306, published correction appears in Br. J. Clin. Psychol. 2020, 59, 276. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1990, 55, 610–617. [Google Scholar] [CrossRef]
- Central Bureau of Statistics: Population of Israel on the Eve of 2021. Media Release 31 December 2020, 438/2020. Available online: https://www.cbs.gov.il/en/mediarelease/Pages/2020/Population-of-Israel-on-the-Eve-of-2021.aspx (accessed on 21 June 2021).
- Horowitz, J.A.; Goodman, J. A longitudinal study of maternal postpartum depression symptoms. Res. Theory Nurs. Pract. 2004, 18, 149–163. [Google Scholar] [CrossRef]
- López-Morales, H.; Del Valle, M.V.; Canet-Juric, L.; Andrés, M.L.; Galli, J.I.; Poó, F.; Urquijo, S. Mental health of pregnant women during the COVID-19 pandemic: A longitudinal study. Psychiatry Res. 2021, 295, 113567. [Google Scholar] [CrossRef]
- Wilf-Miron, R.; Myers, V.; Saban, M. Incentivizing Vaccination Uptake: The “Green Pass” Proposal in Israel. JAMA 2021, 325, 1503–1504. [Google Scholar] [CrossRef]
- Yesilcinar, I.; Yavan, T.; Karasahin, K.E.; Yenen, M.C. The identification of the relationship between the perceived social support, fatigue levels and maternal attachment during the postpartum period. J. Matern. Fetal Neonatal Med. 2017, 30, 1213–1220. [Google Scholar] [CrossRef]
- Yirmiya, K.; Yakirevich-Amir, N.; Preis, H.; Lotan, A.; Atzil, S.; Reuveni, I. Women’s depressive symptoms during the COVID-19 pandemic: The role of pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 4298. [Google Scholar] [CrossRef]
- Aldossari, M.; Chaudhry, S. Women and burnout in the context of a pandemic. Gend. Work Organ. 2021, 28, 826–834. [Google Scholar] [CrossRef]
- Vigod, S.N.; Villegas, L.; Dennis, C.L.; Ross, L.E. Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: A systematic review. BJOG 2010, 117, 540–550. [Google Scholar] [CrossRef]
- Nelson, A.M. Transition to motherhood. J. Obstet. Gynecol. Neonatal Nurs. 2003, 32, 465–477. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Postpartum depression effects on early interactions, parenting, and safety practices: A review. Infant Behav. Dev. 2010, 33, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, R.; Granat, A.; Pariente, C.; Kanety, H.; Kuint, J.; Gilboa-Schechtman, E. Maternal depression and anxiety across the postpartum year and infant social engagement, fear regulation, and stress reactivity. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Ng, Q.X.; Chee, K.T.; De Deyn, M.L.; Chua, Z. Staying connected during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2020, 66, 519–520. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| T1, n = 246 | T2, n = 246 | |
|---|---|---|
| Maternal characteristic | ||
| Maternal age, years | 32.14 ± 5.1 | |
| Nulliparity | 65 (26.4%) | |
| Ethnicity: | ||
| • Jewish | 186 (75.6%) | |
| • Arabic | 60 (24.4) | |
| Religious level (scale 1–5: 1—secular to 5—very religious) | 1.77 ± 0.92 | |
| Marital Status: | ||
| • Married | 219 (89%) | |
| • In a relationship | 10 (4.5%) | |
| • Separated/single | 16 (6.5%) | |
| Education: | ||
| • Elementary | 1 (0.4%) | |
| • High school | 78 (31.7%) | |
| • Bachelor’s degree | 105 (42.7%) | |
| • Master’s degree | 55 (22.4%) | |
| • Doctorate | 7 (2.8%) | |
| Delivery characteristics | ||
| Gestational age at delivery | 39.50 ± 1.1 | |
| Neonatal birth weight | 3286.86 ± 11.0 | |
| Delivery mode | ||
| Vaginal delivery | 198 (80.5%) | |
| Cesarean section | 48 (19.5%) | |
| Maternal mental health and confounders | ||
| Delivery to questionnaire interval, weeks | 11.03 ± 1.6 | 28.48 ± 2.1 |
| EPDS @ (scale 0–30) | 6.31 ± 5.6 | 6.92 ± 5.9 |
| Financial difficulties due to the COVID-19 pandemic (scale 1–5: 1—“not worried at all”, 5—“worried all the time”). | 2.80 ± 1.2 | 2.83 ± 1.1 |
| Exposure to COVID-19 events, number of exposures | 3.63 ± 1.8 | 6.34 ± 2.3 |
| Impact of exposure to COVID-19 events | 8.91 ± 4.6 | 7.47 ± 4.1 |
| Fear of COVID-19 (scale 7–35) | 17.25 ± 5.3 | 17.10 ± 5.3 |
| STAI # (scale 20–80) | 45.35 ± 16.4 | 41.47 ± 14.0 |
| Total score MSPSS $ (scale 1–7) | 5.99 ± 1.1 | 5.88 ± 1.2 |
| • MSPSS $–significant other (scale 1–7) | 6.30 ± 1.2 | 6.24 ± 1.2 |
| • MSPSS $–family (scale 1–7) | 6.10 ± 1.3 | 5.91 ± 1.4 |
| • MSPSS $–friends (scale 1–7) | 5.58 ± 1.5 | 5.48 ± 1.7 |
| T1 to T2 Delta | Mean | Std. Deviation | Std. Error Mean | 95% Confident Interval | t | df | Sig. | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| EPDS @ | −0.64 | 4.59 | 0.29 | −1.21 | −0.06 | −2.17 | 244 | 0.031 |
| Exposure to COVID-19 events | −2.71 | 2.50 | 0.16 | −3.02 | −2.39 | −16.98 | 245 | 0.000 |
| Impact of exposure to COVID-19 events | 1.45 | 4.91 | 0.31 | 0.83 | 2.06 | 4.62 | 245 | 0.000 |
| Fear of COVID-19 | 0.12 | 4.43 | 0.28 | −0.44 | 0.67 | 0.42 | 244 | 0.676 |
| STAI # | 3.91 | 13.67 | 0.89 | 2.16 | 5.67 | 4.39 | 234 | 0.000 |
| MSPSS $ total score | 0.11 | 0.85 | 0.06 | −0.01 | 0.22 | 1.87 | 219 | 0.062 |
| MSPSS $ significant other | 0.06 | 1.08 | 0.07 | −0.09 | 0.20 | 0.78 | 219 | 0.438 |
| MSPSS $ family | 0.17 | 0.92 | 0.06 | 0.04 | 0.29 | 2.68 | 216 | 0.008 |
| MSPSS $ friends | 0.10 | 1.31 | 0.09 | −0.08 | 0.27 | 1.10 | 219 | 0.271 |
| Financial difficulties due to the COVID-19 pandemic | 0.00 | 0.34 | 0.02 | −0.03 | 0.05 | 0.37 | 245 | 0.706 |
| Sum of Squares | df | Mean Square | F | Sig. | |
|---|---|---|---|---|---|
| Delta of MSPSS $ family (T2-T1) | 38.401 | 1 | 38.401 | 4.308 | 0.039 |
| Delta of exposure to COVID-19 events (T2-T1) | 6.756 | 1 | 6.756 | 0.758 | 0.385 |
| Delta of impact of exposure to COVID-19 (T2-T1) | 44.908 | 1 | 44.908 | 5.038 | 0.026 |
| Delta of STAI # (T2-T1) | 285.135 | 1 | 285.135 | 31.988 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gluska, H.; Shiffman, N.; Mayer, Y.; Margalit, S.; Daher, R.; Elyasyan, L.; Sharon Weiner, M.; Miremberg, H.; Kovo, M.; Biron-Shental, T.; et al. Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors. J. Clin. Med. 2022, 11, 3488. https://doi.org/10.3390/jcm11123488
Gluska H, Shiffman N, Mayer Y, Margalit S, Daher R, Elyasyan L, Sharon Weiner M, Miremberg H, Kovo M, Biron-Shental T, et al. Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors. Journal of Clinical Medicine. 2022; 11(12):3488. https://doi.org/10.3390/jcm11123488
Chicago/Turabian StyleGluska, Hadar, Noga Shiffman, Yael Mayer, Shiri Margalit, Rawan Daher, Lior Elyasyan, Maya Sharon Weiner, Hadas Miremberg, Michal Kovo, Tal Biron-Shental, and et al. 2022. "Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors" Journal of Clinical Medicine 11, no. 12: 3488. https://doi.org/10.3390/jcm11123488
APA StyleGluska, H., Shiffman, N., Mayer, Y., Margalit, S., Daher, R., Elyasyan, L., Sharon Weiner, M., Miremberg, H., Kovo, M., Biron-Shental, T., Helpman, L., & Gabbay-Benziv, R. (2022). Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors. Journal of Clinical Medicine, 11(12), 3488. https://doi.org/10.3390/jcm11123488