
What’s New in Intravenous Anaesthesia? New Hypnotics, New Models and New Applications

 ,
,
Abstract
:1. Introduction
2. New Hypnotic Agents
2.1. Mechanism of Hypnotic Agents
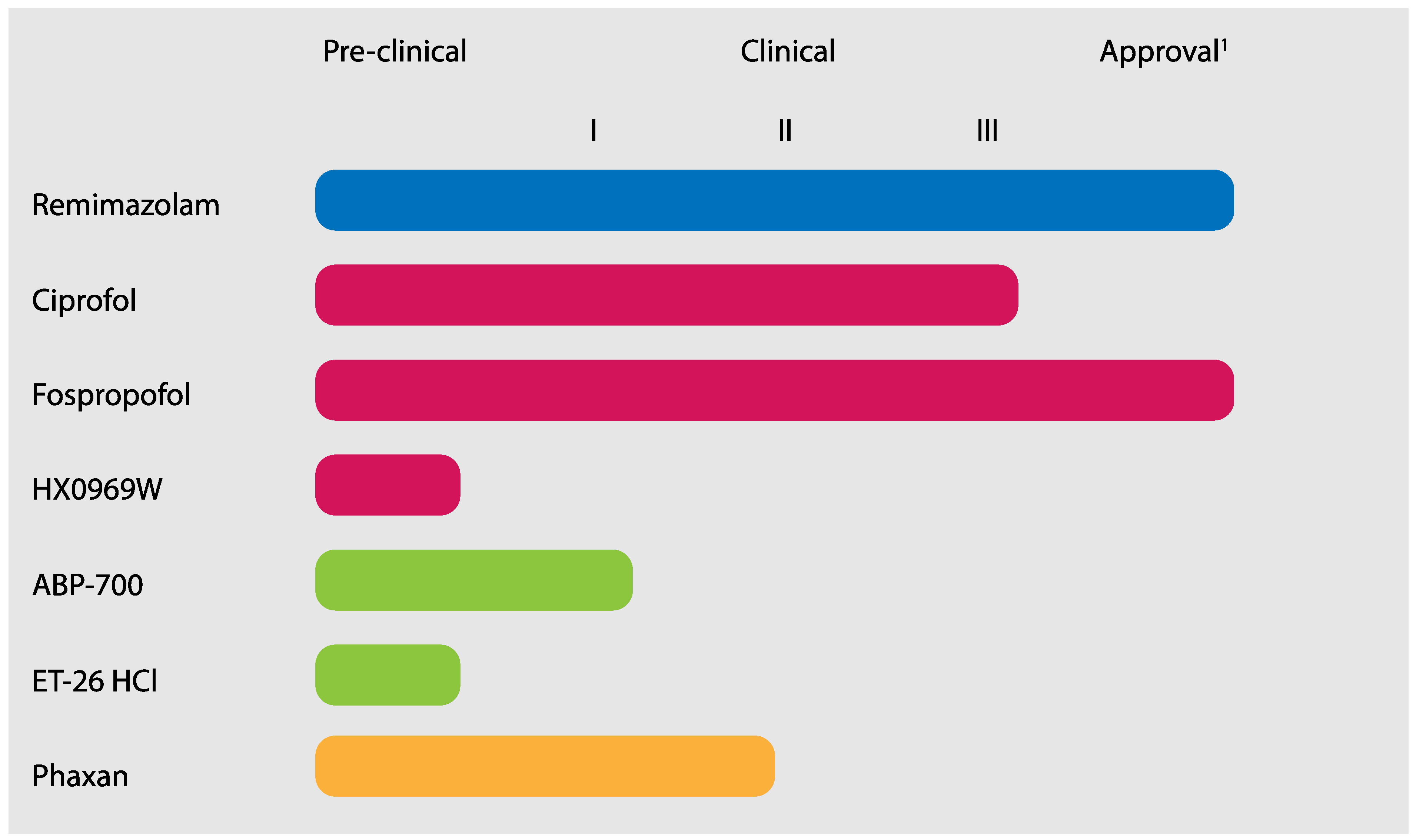
2.2. New Hypnotic Agents Approved for Clinical Use
2.2.1. Remimazolam
2.2.2. 2,6-Disubstituted Phenol Derivatives
2.2.3. Propofol Analogues
Ciprofol
Fospropofol
HX0969W
2.2.4. Etomidate Analogues
ABP-700
Preclinical Developments
2.2.5. Neurosteroids
3. New PK-PD Models for Existing Anaesthetic Drugs for TCI Application
4. New Drug Applications
5. Conclusions/Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eger, E.I. Characteristics of anesthetic agents used for induction and maintenance of general anesthesia. Am. J. Health Pharm. AJHP Off. J. Am. Soc. Health Pharm. 2004, 61 (Suppl. S4), 3. [Google Scholar] [CrossRef] [PubMed]
- Sahinovic, M.M.; Struys, M.M.R.F.; Absalom, A.R. Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clin. Pharmacokinet. 2018, 57, 1539–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valk, B.I.; Struys, M.M.R.F. Etomidate and its Analogs: A Review of Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 2021, 60, 1253–1269. [Google Scholar] [CrossRef] [PubMed]
- Peltoniemi, M.A.; Hagelberg, N.M.; Olkkola, K.T.; Saari, T.I. Ketamine: A Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy. Clin. Pharmacokinet. 2016, 55, 1059–1077. [Google Scholar] [CrossRef]
- Dundee, J.W.; Halliday, N.J.; Harper, K.W.; Brogden, R.N. Midazolam. A review of its pharmacological properties and therapeutic use. Drugs 1984, 28, 519–543. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Gambus, P.L.; Rigby-Jones, A.E. Current status of perioperative hypnotics, role of benzodiazepines, and the case for remimazolam: A narrative review. Br. J. Anaesth. 2021, 127, 41–55. [Google Scholar] [CrossRef]
- Schüttler, J.; Eisenried, A.; Lerch, M.; Fechner, J.; Jeleazcov, C.; Ihmsen, H. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers Part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology 2020, 132, 636–651. [Google Scholar] [CrossRef]
- Teng, Y.; Ou, M.-C.; Wang, X.; Zhang, W.-S.; Liu, X.; Liang, Y.; Zuo, Y.-X.; Zhu, T.; Liu, B.; Liu, J. Pharmacokinetic and pharmacodynamic properties of ciprofol emulsion in Chinese subjects: A single center, open-label, single-arm dose-escalation phase 1 study. Am. J. Transl. Res. 2021, 13, 13791–13802. [Google Scholar]
- Struys, M.M.R.F.; Valk, B.I.; Eleveld, D.J.; Absalom, A.R.; Meyer, P.; Meier, S.; Den Daas, I.; Chou, T.; Van Amsterdam, K.; Campagna, J.A.; et al. A Phase 1, Single-center, Double-blind, Placebo-controlled Study in Healthy Subjects to Assess the Safety, Tolerability, Clinical Effects, and Pharmacokinetics-Pharmacodynamics of Intravenous Cyclopropyl-methoxycarbonylmetomidate (ABP-700) after a Single. Anesthesiology 2017, 127, 20–35. [Google Scholar] [CrossRef]
- Goodchild, C.S.; Serrao, J.M.; Sear, J.W.; Anderson, B.J. Pharmacokinetic and Pharmacodynamic Analysis of Alfaxalone Administered as a Bolus Intravenous Injection of Phaxan in a Phase 1 Randomized Trial. Anesth. Analg. 2020, 130, 704–714. [Google Scholar] [CrossRef]
- Monagle, J.; Siu, L.; Worrell, J.; Goodchild, C.S.; Serrao, J.M. A Phase 1c Trial Comparing the Efficacy and Safety of a New Aqueous Formulation of Alphaxalone with Propofol. Anesth. Analg. 2015, 121, 914–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franks, N.P.; Lieb, W.R. Molecular and cellular mechanisms of general anaesthesia. Nature 1994, 367, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Hales, T.G.; Lambert, J.J. The actions of propofol on inhibitory amino acid receptors of bovine adrenomedullary chromaffin cells and rodent central neurones. Br. J. Pharmacol. 1991, 104, 619–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belelli, D.; Pistis, M.; Peters, J.A.; Lambert, J.J. General anaesthetic action at transmitter-gated inhibitory amino acid receptors. Trends Pharmacol. Sci. 1999, 20, 496–502. [Google Scholar] [CrossRef]
- Krasowski, M.D.; Harrison, N.L. General anaesthetic actions on ligand-gated ion channels. Cell. Mol. life Sci. C 1999, 55, 1278–1303. [Google Scholar] [CrossRef]
- Weir, C.J.; Mitchell, S.J.; Lambert, J.J. Role of GABA A receptor subtypes in the behavioural effects of intravenous general anaesthetics. Br. J. Anaesth. 2017, 119, i167–i175. [Google Scholar] [CrossRef] [Green Version]
- Kilpatrick, G.J. Remimazolam: Non-Clinical and Clinical Profile of a New Sedative/Anesthetic Agent. Front. Pharmacol. 2021, 12, 1850. [Google Scholar] [CrossRef]
- Worthington, M.T.; Antonik, L.J.; Goldwater, D.R.; Lees, J.P.; Wilhelm-Ogunbiyi, K.; Borkett, K.M.; Mitchell, M.C. A phase ib, dose-finding study of multiple doses of remimazolam (cns 7056) in volunteers undergoing colonoscopy. Anesth. Analg. 2013, 117, 1093–1100. [Google Scholar] [CrossRef]
- Sheng, X.Y.; Liang, Y.; Yang, X.Y.; Li, L.; Ye, X.; Zhao, X.; Cui, Y.M. Safety, pharmacokinetic and pharmacodynamic properties of single ascending dose and continuous infusion of remimazolam besylate in healthy Chinese volunteers. Eur. J. Clin. Pharmacol. 2020, 76, 383–391. [Google Scholar] [CrossRef]
- Eisenried, A.; Schüttler, J.; Lerch, M.; Ihmsen, H.; Jeleazcov, C. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: Part II. Pharmacodynamics of Electroencephalogram Effects. Anesthesiology 2020, 132, 652–666. [Google Scholar] [CrossRef] [Green Version]
- Borkett, K.M.C.; Riff, D.S.; Schwartz, H.I.; Winkle, P.J.; Pambianco, D.J.; Lees, J.P.C.; Wilhelm-Ogunbiyi, K. A Phase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus midazolam for sedation in upper gastrointestinal endoscopy. Anesth. Analg. 2015, 120, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Wiltshire, H.R.; Kilpatrick, G.J.; Tilbrook, G.S.; Borkett, K.M. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): Part II. Population pharmacokinetic and pharmacodynamic modeling and simulation. Anesth. Analg. 2012, 115, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Pambianco, D.J.; Borkett, K.M.; Riff, D.S.; Winkle, P.J.; Schwartz, H.I.; Melson, T.I.; Wilhelm-Ogunbiyi, K. A phase IIb study comparing the safety and efficacy of remimazolam and midazolam in patients undergoing colonoscopy. Gastrointest. Endosc. 2016, 83, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Rex, D.K.; Bhandari, R.; Desta, T.; DeMicco, M.P.; Schaeffer, C.; Etzkorn, K.; Barish, C.F.; Pruitt, R.; Cash, B.D.; Quirk, D.; et al. A phase III study evaluating the efficacy and safety of remimazolam (CNS 7056) compared with placebo and midazolam in patients undergoing colonoscopy. Gastrointest. Endosc. 2018, 88, 427–437.e6. [Google Scholar] [CrossRef] [Green Version]
- Dai, G.; Pei, L.; Duan, F.; Liao, M.; Zhang, Y.; Zhu, M.; Zhao, Z.; Zhang, X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021, 87, 1073–1079. [Google Scholar] [CrossRef]
- Doi, M.; Hirata, N.; Suzuki, T.; Morisaki, H.; Morimatsu, H.; Sakamoto, A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): Results of a multicenter, randomized, double-blind, parallel-group comparative trial. J. Anesth. 2020, 34, 491–501. [Google Scholar] [CrossRef]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and safety of remimazolam versus propofol for general anesthesia: A multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J. Anesth. 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Sasaki, H.; Hoshijima, H.; Mizuta, K. Ringer’s Acetate Solution-Induced Precipitation of Remimazolam. Br. J. Anaesth. 2021, 126, e87–e89. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Rigby-Jones, A.E. Remimazolam for Anaesthesia or Sedation. Curr. Opin. Anaesthesiol. 2020, 33, 506–511. [Google Scholar] [CrossRef]
- Nordström, O.; Sandin, R. Recall during intermittent propofol anaesthesia. Br. J. Anaesth. 1996, 76, 699–701. [Google Scholar] [CrossRef]
- Smith, I.; Monk, T.G.; White, P.F.; Ding, Y. Propofol infusion during regional anesthesia: Sedative, amnestic, and anxiolytic properties. Anesth. Analg. 1994, 79, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Borgeat, A.; Stirnemann, H.R. Antiemetic effect of propofol. Anaesthesist 1998, 47, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Hug, C.C.; McLeskey, C.H.; Nahrwold, M.L.; Roizen, M.F.; Stanley, T.H.; Thisted, R.A.; Walawander, C.A.; White, P.F.; Apfelbaum, J.L.; Grasela, T.H. Hemodynamic effects of propofol: Data from over 25,000 patients. Anesth. Analg. 1993, 77, 21. [Google Scholar]
- Marik, P.E. Propofol: Therapeutic indications and side-effects. Curr. Pharm. Des. 2004, 10, 3639–3649. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Ren, L.; Wan, S.; Liu, G.; Luo, X.; Liu, Z.; Li, F.; Yu, Y.; Liu, J.; Wei, Y. Design, Synthesis, and Evaluation of Novel 2,6-Disubstituted Phenol Derivatives as General Anesthetics. J. Med. Chem. 2017, 60, 3606–3617. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Ou, X.; Teng, Y.; Shu, S.; Wang, Y.; Zhu, X.; Kang, Y.; Miao, J. Sedation Effects Produced by a Ciprofol Initial Infusion or Bolus Dose Followed by Continuous Maintenance Infusion in Healthy Subjects: A Phase 1 Trial. Adv. Ther. 2021, 38, 5484–5500. [Google Scholar] [CrossRef] [PubMed]
- Bian, Y.; Zhang, H.; Ma, S.; Jiao, Y.; Yan, P.; Liu, X.; Ma, S.; Xiong, Y.; Gu, Z.; Yu, Z.; et al. Mass balance, pharmacokinetics and pharmacodynamics of intravenous HSK3486, a novel anaesthetic, administered to healthy subjects. Br. J. Clin. Pharmacol. 2021, 87, 93–105. [Google Scholar] [CrossRef]
- Kalman, S.; Koch, P.; Ahlén, K.; Kanes, S.J.; Barassin, S.; Björnsson, M.A.; Norberg, Å. First Human Study of the Investigational Sedative and Anesthetic Drug AZD3043: A Dose-Escalation Trial to Assess the Safety, Pharmacokinetics, and Efficacy of a 30-Minute Infusion in Healthy Male Volunteers. Anesth. Analg. 2015, 121, 885–893. [Google Scholar] [CrossRef]
- Teng, Y.; Ou, M.; Wang, X.; Zhang, W.; Liu, X.; Liang, Y.; Li, K.; Wang, Y.; Ouyang, W.; Weng, H.; et al. Efficacy and safety of ciprofol for the sedation/anesthesia in patients undergoing colonoscopy: Phase IIa and IIb multi-center clinical trials. Eur. J. Pharm. Sci. 2021, 164, 105904. [Google Scholar] [CrossRef]
- Luo, Z.; Tu, H.; Zhang, X.; Wang, X.; Ouyang, W.; Wei, X.; Zou, X.; Zhu, Z.; Li, Y.; Shangguan, W.; et al. Efficacy and Safety of HSK3486 for Anesthesia/Sedation in Patients Undergoing Fiberoptic Bronchoscopy: A Multicenter, Double-Blind, Propofol-Controlled, Randomized, Phase 3 Study. CNS Drugs 2022, 36, 301–313. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, C.; Liu, N.; Tong, L.; Nie, Y.; Wu, J.; Liu, X.; Gao, W.; Tang, L.; Guan, X. Efficacy and Safety of Ciprofol Sedation in ICU Patients with Mechanical Ventilation: A Clinical Trial Study Protocol. Adv. Ther. 2021, 38, 5412–5423. [Google Scholar] [CrossRef] [PubMed]
- Hsk3486—Haisco-USA Pharmaceutical Company, Inc. Available online: https://haisco-usa.com/r-%26-d (accessed on 27 March 2022).
- Garnock-Jones, K.P.; Scott, L.J. Fospropofol. Drugs 2010, 70, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Luo, C.; Liu, J.; Zhang, W.; Li, Y.; Xu, J. Efficacy and Safety of FospropofolFD Compared to Propofol When Given During the Induction of General Anaesthesia: A Phase II, Multi-centre, Randomized, Parallel-Group, Active-Controlled, Double-Blind, Double-Dummy Study. Basic Clin. Pharmacol. Toxicol. 2016, 119, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.J.; Jiang, Y.Y.; Wang, H.Y.; Wang, B.; Yang, J.; Kang, Y.; Chen, J.; Liu, J.; Zhang, W.S. The preclinical pharmacological study on HX0969W, a novel water-soluble pro-drug of propofol, in rats. PeerJ 2020, 8, e8922. [Google Scholar] [CrossRef] [Green Version]
- Forman, S.A. Clinical and molecular pharmacology of etomidate. Anesthesiology 2011, 114, 695–707. [Google Scholar] [CrossRef] [Green Version]
- Ledingham, I.M.; Watt, I. Influence of sedation on mortality in critically ill multiple trauma patients. Lancet 1983, 321, 1270. [Google Scholar] [CrossRef]
- Wagner, R.L.; White, P.F.; Kan, P.B.; Rosenthal, M.H.; Feldman, D. Inhibition of adrenal steroidogenesis by the anesthetic etomidate. N. Engl. J. Med. 1984, 310, 1415–1421. [Google Scholar] [CrossRef]
- Husain, S.S.; Pejo, E.; Ge, R.; Raines, D.E. Modifying methoxycarbonyl etomidate inter-ester spacer optimizes in vitro metabolic stability and in vivo hypnotic potency and duration of action. Anesthesiology 2012, 117, 1027–1036. [Google Scholar] [CrossRef] [Green Version]
- Campagna, J.A.; Pojasek, K.; Grayzel, D.; Randle, J.; Raines, D.E. Advancing novel anesthetics: Pharmacodynamic and pharmacokinetic studies of cyclopropyl-methoxycarbonyl metomidate in dogs. Anesthesiology 2014, 121, 1203–1216. [Google Scholar] [CrossRef] [Green Version]
- Valk, B.I.; Absalom, A.R.; Meyer, P.; Meier, S.; den Daas, I.; van Amsterdam, K.; Campagna, J.A.; Sweeney, S.P.; Struys, M.M.R.F. Safety and clinical effect of i.v. infusion of cyclopropyl-methoxycarbonyl etomidate (ABP-700), a soft analogue of etomidate, in healthy subjects. Br. J. Anaesth. 2018, 120, 1401–1411. [Google Scholar] [CrossRef] [Green Version]
- Valk, B.I.; Eleveld, D.J.; Meyer, P.; Meier, S.; den Daas, I.; van Amsterdam, K.; Campagna, J.A.; Sweeney, S.P.; Absalom, A.R.; Struys, M.M.R.F. Modeling the Effect of Excitation on Depth of Anesthesia Monitoring in γ-Aminobutyric Acid Type A Receptor Agonist ABP-700. Anesthesiology 2020, 134, 35–51. [Google Scholar] [CrossRef]
- Wang, B.; Yang, J.; Chen, J.; Kang, Y.; Yang, L.H.; Liu, J.; Zhang, W.S. An Etomidate Analogue with Less Adrenocortical Suppression, Stable Hemodynamics, and Improved Behavioral Recovery in Rats. Anesth. Analg. 2017, 125, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Chen, S.; Yang, J.; Yang, L.; Liu, J.; Zhang, W. ET-26 hydrochloride (ET-26 HCl) has similar hemodynamic stability to that of etomidate in normal and uncontrolled hemorrhagic shock (UHS) rats. PLoS ONE 2017, 12, e0183439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prys-roberts, C.; Sear, J. Steroid anaesthesia. Br. J. Anaesth. 1980, 52, 363–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottrell, G.A.; Lambert, J.J.; Peters, J.A. Modulation of GABAA receptor activity by alphaxalone. Br. J. Pharmacol. 1987, 90, 491–500. [Google Scholar] [CrossRef] [Green Version]
- Sear, J.W. Challenges of bringing a new sedative to market! Curr. Opin. Anaesthesiol. 2018, 31, 423–430. [Google Scholar] [CrossRef]
- Goodchild, C.S.; Serrao, J.M.; Kolosov, A.; Boyd, B.J. Alphaxalone Reformulated: A Water-Soluble Intravenous Anesthetic Preparation in Sulfobutyl-Ether-β-Cyclodextrin. Anesth. Analg. 2015, 120, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Hannivoort, L.N.; Absalom, A.R.; Struys, M.M.R.F. The role of pharmacokinetics and pharmacodynamics in clinical anaesthesia practice. Curr. Opin. Anaesthesiol. 2020, 33, 483–489. [Google Scholar] [CrossRef]
- Varvel, J.R.; Donoho, D.L.; Shafer, S.L. Measuring the predictive performance of computer-controlled infusion pumps. J. Pharmacokinet. Biopharm. 1992, 20, 63–94. [Google Scholar] [CrossRef]
- Schüttler, J.; Kloos, S.; Schwilden, H.; Stoeckel, H. Total intravenous anaesthesia with propofol and alfentanil by computer-assisted infusion. Anaesthesia 1988, 43, 2–7. [Google Scholar] [CrossRef]
- Glass, P.; Shafer, S.; Reves, J.G. Intravenous drug delivery systems. In Miller’s Anesthesia; Miller, R.D., Ed.; Elsevier Churchill Livingstone: Amsterdam, The Netherlands, 2005; pp. 439–480. [Google Scholar]
- Vandemoortele, O.; Hannivoort, L.N.; Vanhoorebeeck, F.; Struys, M.M.R.F.; Vereecke, H.E.M. General Purpose Pharmacokinetic-Pharmacodynamic Models for Target-Controlled Infusion of Anaesthetic Drugs: A Narrative Review. J. Clin. Med. 2022, 11, 2487. [Google Scholar] [CrossRef] [PubMed]
- Marsh, B.; White, M.; Morton, N.; Kenny, G.N. Pharmacokinetic model driven infusion of propofol in children. Br. J. Anaesth. 1991, 67, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Schnider, T.W.; Minto, C.F.; Gambus, P.L.; Andressen, C.; Goodale, D.B.; Shafer, S.L.; Youngs, E.J. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Schnider, T.W.; Minto, C.F.; Shafer, S.L.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Youngs, E.J. The influence of age on propofol pharmacodynamics. Anesthesiology 1999, 90, 1502–1516. [Google Scholar] [CrossRef] [PubMed]
- Kataria, B.K.; Ved, S.A.; Nicodemus, H.F.; Hoy, G.R.; Lea, D.; Dubois, M.Y.; Mandema, J.W.; Shafer, S.L. The Pharmacokinetics of Propofol in Children Using Three Different Data Analysis Approaches. Anesthesiology 1994, 80, 104–122. [Google Scholar] [CrossRef]
- Absalom, A.; Kenny, G. ‘Paedfusor’ pharmacokinetic data set. Br. J. Anaesth. 2005, 95, 110. [Google Scholar] [CrossRef] [Green Version]
- Vellinga, R.; Hannivoort, L.N.; Introna, M.; Touw, D.J.; Absalom, A.R.; Eleveld, D.J.; Struys, M.M.R.F. Prospective clinical validation of the Eleveld propofol pharmacokinetic-pharmacodynamic model in general anaesthesia. Br. J. Anaesth. 2021, 126, 386–394. [Google Scholar] [CrossRef]
- Eleveld, D.J.; Colin, P.; Absalom, A.R.; Struys, M.M.R.F. Pharmacokinetic–pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br. J. Anaesth. 2018, 120, 942–959. [Google Scholar] [CrossRef] [PubMed]
- Vellinga, R.; Hannivoort, L.N.; Koomen, J.V.; Colin, P.; Absalom, A.R.; Struys, M.M.R.F.; Eleveld, D.J. Clinical validation of pharmacokinetic/pharmacodynamic models for propofol infusion. Response to Br. J. Anaesth. 2021: 126: e172-4. Br. J. Anaesth. 2021, 127, e3–e5. [Google Scholar] [CrossRef]
- Short, T.G.; Campbell, D.; Egan, T.D. Increasing the utility of target-controlled infusions: One model to rule them all. Br. J. Anaesth. 2018, 120, 887–890. [Google Scholar] [CrossRef] [Green Version]
- Dyck, J.B.; Maze, M.; Haack, C.; Azarnoff, D.L.; Vuorilehto, L.; Shafer, S.L. Computer-controlled infusion of intravenous dexmedetomidine hydrochloride in adult human volunteers. Anesthesiology 1993, 78, 821–828. [Google Scholar] [CrossRef]
- Colin, P.J.; Hannivoort, L.N.; Eleveld, D.J.; Reyntjens, K.M.E.M.; Absalom, A.R.; Vereecke, H.E.M.; Struys, M.M.R.F. Dexmedetomidine pharmacodynamics in healthy volunteers: 2. Haemodynamic profile. Br. J. Anaesth. 2017, 119, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Colin, P.J.; Hannivoort, L.N.; Eleveld, D.J.; Reyntjens, K.M.E.M.; Absalom, A.R.; Vereecke, H.E.M.; Struys, M.M.R.F. Dexmedetomidine pharmacokinetic-pharmacodynamic modelling in healthy volunteers: 1. Influence of arousal on bispectral index and sedation. Br. J. Anaesth. 2017, 119, 200–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannivoort, L.N.; Eleveld, D.J.; Proost, J.H.; Reyntjens, K.M.E.M.; Absalom, A.R.; Vereecke, H.E.M.; Struys, M.M.R.F. Development of an Optimized Pharmacokinetic Model of Dexmedetomidine Using Target-controlled Infusion in Healthy Volunteers. Anesthesiology 2015, 123, 357–367. [Google Scholar] [CrossRef]
- Alvarez-Jimenez, R.; Weerink, M.A.S.; Hannivoort, L.N.; Su, H.; Struys, M.M.R.F.; Loer, S.A.; Colin, P.J. Dexmedetomidine Clearance Decreases with Increasing Drug Exposure: Implications for Current Dosing Regimens and Target-controlled Infusion Models Assuming Linear Pharmacokinetics. Anesthesiology 2022, 136, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Leonowens, C.; Ivaturi, V.D.; Lohmer, L.L.; Curd, L.; Ossig, J.; Schippers, F.; Petersen, K.U.; Stoehr, T.; Schmith, V. Population pharmacokinetic/pharmacodynamic modeling for remimazolam in the induction and maintenance of general anesthesia in healthy subjects and in surgical subjects. J. Clin. Anesth. 2020, 66, 109899. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Curd, L.; Lohmer, L.R.L.; Delpratt, N.; Ossig, J.; Schippers, F.; Stoehr, T.; Schmith, V.D. A population pharmacodynamic Markov mixed-effects model for determining remimazolam-induced sedation when co-administered with fentanyl in procedural sedation. Clin. Transl. Sci. 2021, 14, 1554–1565. [Google Scholar] [CrossRef] [PubMed]
- Nooh, N.; Sheta, S.A.; Abdullah, W.A.; Abdelhalim, A.A. Intranasal atomized dexmedetomidine for sedation during third molar extraction. Int. J. Oral Maxillofac. Surg. 2013, 42, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Bai, X.; Zhang, Q.; Wang, X.; Lu, L. The safety and efficacy of intranasal dexmedetomidine during electrochemotherapy for facial vascular malformation: A double-blind, randomized clinical trial. J. Oral Maxillofac. Surg. 2013, 71, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Yuen, V.M.; Irwin, M.G.; Hui, T.W.; Yuen, M.K.; Lee, L.H.Y. A double-blind, crossover assessment of the sedative and analgesic effects of intranasal dexmedetomidine. Anesth. Analg. 2007, 105, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Broderick, D.; Clarke, M.; Stassen, L. Midazolam and drug-drug interactions in dental conscious sedation. J. Ir. Dent. Assoc. 2014, 60, 38–43. [Google Scholar] [PubMed]
- Bouw, M.R.; Chung, S.S.; Gidal, B.; King, A.; Tomasovic, J.; Wheless, J.W.; Van Ess, P.J. Clinical pharmacokinetic and pharmacodynamic profile of midazolam nasal spray. Epilepsy Res. 2021, 171, 106567. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Yuen, V.M.; Goulay-Dufaÿ, S.; Sheng, Y.; Standing, J.F.; Kwok, P.C.L.; Leung, M.K.M.; Leung, A.S.; Wong, I.C.K.; Irwin, M.G. Pharmacokinetic and pharmacodynamic study of intranasal and intravenous dexmedetomidine. Br. J. Anaesth. 2018, 120, 960–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barends, C.R.M.; Driesens, M.K.; Struys, M.M.R.F.; Visser, A.; Absalom, A.R. Intranasal dexmedetomidine in elderly subjects with or without beta blockade: A randomised double-blind single-ascending-dose cohort study. Br. J. Anaesth. 2020, 124, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Knoester, P.D.; Jonker, D.M.; Van Der Hoeven, R.T.M.; Vermeij, T.A.C.; Edelbroek, P.M.; Brekelmans, G.J.; De Haan, G.J. Pharmacokinetics and pharmacodynamics of midazolam administered as a concentrated intranasal spray. A study in healthy volunteers. Br. J. Clin. Pharmacol. 2002, 53, 501–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wermeling, D.P.; Record, K.A.; Archer, S.M.; Rudy, A.C. A pharmacokinetic and pharmacodynamic study, in healthy volunteers, of a rapidly absorbed intranasal midazolam formulation. Epilepsy Res. 2009, 83, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.K.; Myrvik, M.J.; Van Ess, P.J. Pharmacokinetics, pharmacodynamics, and tolerability of USL261, midazolam nasal spray: Randomized study in healthy geriatric and non-geriatric adults. Epilepsy Behav. 2017, 71, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barends, C.R.M.; Absalom, A.R.; Visser, A. Intranasal midazolam for the sedation of geriatric patients with care-resistant behaviour during essential dental treatment: An observational study. Gerodontology 2021, 39, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Wermeling, D.P.; Record, K.A.; Kelly, T.H.; Archer, S.M.; Clinch, T.; Rudy, A.C. Pharmacokinetics and pharmacodynamics of a new intranasal midazolam formulation in healthy volunteers. Anesth. Analg. 2006, 103, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steven, L. Shafer The evolution of pharmacokinetics. Br. J. Anaesth. 2020, 124, 664–665. [Google Scholar] [CrossRef]


{kind=link}
| Mechanism of Action | Elimination Half-Life (min) | Clearance (mLkg−1min−1) | Vdss (L kg−1) | Time to Onset (s) | Effect on | Reversal with Flumazenil | Significant Side Effects | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heart Rate | Blood Pressure | Respiration | Amnesia | PONV | Analgesia | Pain on Injection | ||||||||
| Propofol [2] | GABAA receptor | 116–834 | 25.4–32.6 | 2.27–11 | <30 | o | -- | -- | ++ | -- | o | ++ | o | Propofol infusion syndrome |
| Etomidate [3] | GABAA receptor | 174–330 | 9.9–25.0 | 0.15–4.7 | <30 | o | o | o | + | o | + | o | Adrenal suppression; Excitation | |
| Ketamine [4] | NMDA receptor | 120–240 | 14.3–35.0 | 2.28–7.86 | <60 | ++ | ++ | o | + | - | ++ | o | o | Psychedelic effects, Elevated Intracranial pressure |
| Midazolam [5] | GABAA receptor | 102–156 | 6.4–11 | 1.1–1.7 | 120–180 | + | - | + | ++ | + | o | o | + | |
| Remimazolam [6,7] | GABAA receptor | 70 ± 10 | 1.15 ± 0.12 | 35.4 ± 4.2 | 60–90 | + | - | + | ++ | + | o | o | + | |
| Ciprofol [8] | GABAA receptor | 105.6–125.3 | 21.7–24.6 | 3.6–4.3 | 60–120 | - | - | ? | ? | o | ? | o | o | |
| ABP-700 [3,9] | GABAA receptor | 13.1–16.2 | 27.8 | ? | <30 | + | + | + | ? | + | o | o | o | |
| Phaxan [10,11] | GABAA receptor | ? | 15.4 | 0.38 | <60 | o | - | o | ? | o | ? | o | o | |
| Arterial Samples | MdPE (%) | MdAPE (%) | ΔMdAPE (%) | p-Value | Wobble (%) | ΔWobble (%) | p-Value |
|---|---|---|---|---|---|---|---|
| Eleveld PK-PD | |||||||
| Children | −4.42 (−35.1, 37.6) | 16.8 (1.92, 37.6) | 7.39 (0.77, 16.0) | ||||
| Adults | −14.1 (−43.3, 24.6) | 19.5 (4.86, 43.3) | 7.89 (2.01, 17.6) | ||||
| Elderly | −27.0 (−53.9, 7.75) | 29.5 (6.02, 53.9) | 7.28 (2.48, 24.7) | ||||
| Obese | −14.1 (−40.7, 11.6) | 18.3 (4.11, 40.7) | 6.80 (1.89, 14.1) | ||||
| Schnider | |||||||
| Adults | −2.11 (−35.6, 61.8) | 17.5 (6.04, 61.8) | −1.98 (−15.7, 37.2) | 0.020 | 8.81 (4.11, 22.2) | 0.92 (−3.54, 5.99) | 0.989 |
| Elderly | −5.13 (−44.0, 46.2) | 22.2 (5.68, 46.2) | −7.28 (−23.7, 36.2) | 0.043 | 9.46 (1.74, 25.8) | 2.18 (−1.65, 10.0) | 1.000 |
| Obese | 5.75 (−30.8, 56.2) | 22.1 (5.02, 56.2) | 3.80 (−21.1, 46.0) | 0.674 | 8.08 (1.97, 24.3) | 1.28 (−7.09, 12.1) | 0.971 |
| Marsh | |||||||
| Adults | −0.03 (−24.8, 53.1) | 16.4 (5.82, 53.1) | −3.14 (−25.3, 29.4) | 0.051 | 9.33 (3.33, 19.6) | 1.43 (−4.34, 8.01) | 0.996 |
| Elderly | 3.38 (−45.9, 80.4) | 26.2 (7.85, 80.4) | −3.23 (−32.5, 63.2) | 0.150 | 12.0 (4.53, 44.4) | 4.70 (−1.47, 19.8) | 1.000 |
| Obese | 17.0 (−32.7, 71.3) | 28.8 (6.48, 71.3) | 10.5 (−23.1, 62.7) | 0.965 | 9.46 (3.43, 18.6) | 2.66 (−5.20, 6.95) | 1.000 |
| Marsh (Servin-formula) | |||||||
| Obese | −10.7 (−46.2, 30.9) | 20.0 (2.16, 46.2) | 1.69 (−15.7, 22.3) | 0.914 | 7.30 (2.65, 14.0) | 0.50 (−6.74, 4.07) | 0.957 |
| Cortinez (Obese) | |||||||
| Obese | −7.48 (−47.3, 32.0) | 20.0 (4.22, 47.3) | 1.70 (−12.9, 23.4) | 0.738 | 7.67 (1.25, 18.8) | 0.87 (−3.73, 5.36) | 0.983 |
| Paedfusor | |||||||
| Children | −3.18 (−27.1, 38.1) | 15.5 (2.57, 38.1) | −1.37 (−13.9, 10.2) | 0.262 | 9.89 (2.06, 25.0) | 2.50 (−10.7, 15.9) | 0.995 |
| Kataria | |||||||
| Children | 26.2 (−12.9, 95.8) | 31.1 (7.59, 95.8) | 14.3 (−16.6, 70.1) | 0.995 | 12.6 (0.95, 38.1) | 5.25 (−5.28, 22.1) | 0.999 |
| BIS | MdPE (BIS) | MdAPE (BIS) | ΔMdAPE (BIS) | p−Value | Wobble (BIS) | ΔWobble (BIS) | p−Value |
| Eleveld PK-PD | |||||||
| Children | 1.95 (−21.7, 20.9) | 9.10 (3.43, 21.7) | 4.35 (1.73, 8.94) | ||||
| Adults | 0.29 (−15.2, 17.9) | 7.88 (1.95, 17.9) | 3.60 (1.55, 7.45) | ||||
| Elderly | 1.80 (−11.9, 13.1) | 7.57 (2.69, 13.1) | 4.46 (2.18, 8.28) | ||||
| Obese | 0.74 (−24.4, 31.3) | 9.61 (3.17, 31.3) | 3.50 (1.76, 6.03) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vellinga, R.; Valk, B.I.; Absalom, A.R.; Struys, M.M.R.F.; Barends, C.R.M. What’s New in Intravenous Anaesthesia? New Hypnotics, New Models and New Applications. J. Clin. Med. 2022, 11, 3493. https://doi.org/10.3390/jcm11123493
Vellinga R, Valk BI, Absalom AR, Struys MMRF, Barends CRM. What’s New in Intravenous Anaesthesia? New Hypnotics, New Models and New Applications. Journal of Clinical Medicine. 2022; 11(12):3493. https://doi.org/10.3390/jcm11123493
Chicago/Turabian StyleVellinga, Remco, Beatrijs I. Valk, Anthony R. Absalom, Michel M. R. F. Struys, and Clemens R. M. Barends. 2022. "What’s New in Intravenous Anaesthesia? New Hypnotics, New Models and New Applications" Journal of Clinical Medicine 11, no. 12: 3493. https://doi.org/10.3390/jcm11123493
APA StyleVellinga, R., Valk, B. I., Absalom, A. R., Struys, M. M. R. F., & Barends, C. R. M. (2022). What’s New in Intravenous Anaesthesia? New Hypnotics, New Models and New Applications. Journal of Clinical Medicine, 11(12), 3493. https://doi.org/10.3390/jcm11123493