
Usefulness of C2HEST Score in Predicting Clinical Outcomes of COVID-19 in Heart Failure and Non-Heart-Failure Cohorts
 , ,
, ,  , , , ,
, , , , 
 , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Endpoints and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Baseline Demographical and Clinical Features of the Studied Population
3.2. Treatment Applied during Hospitalization
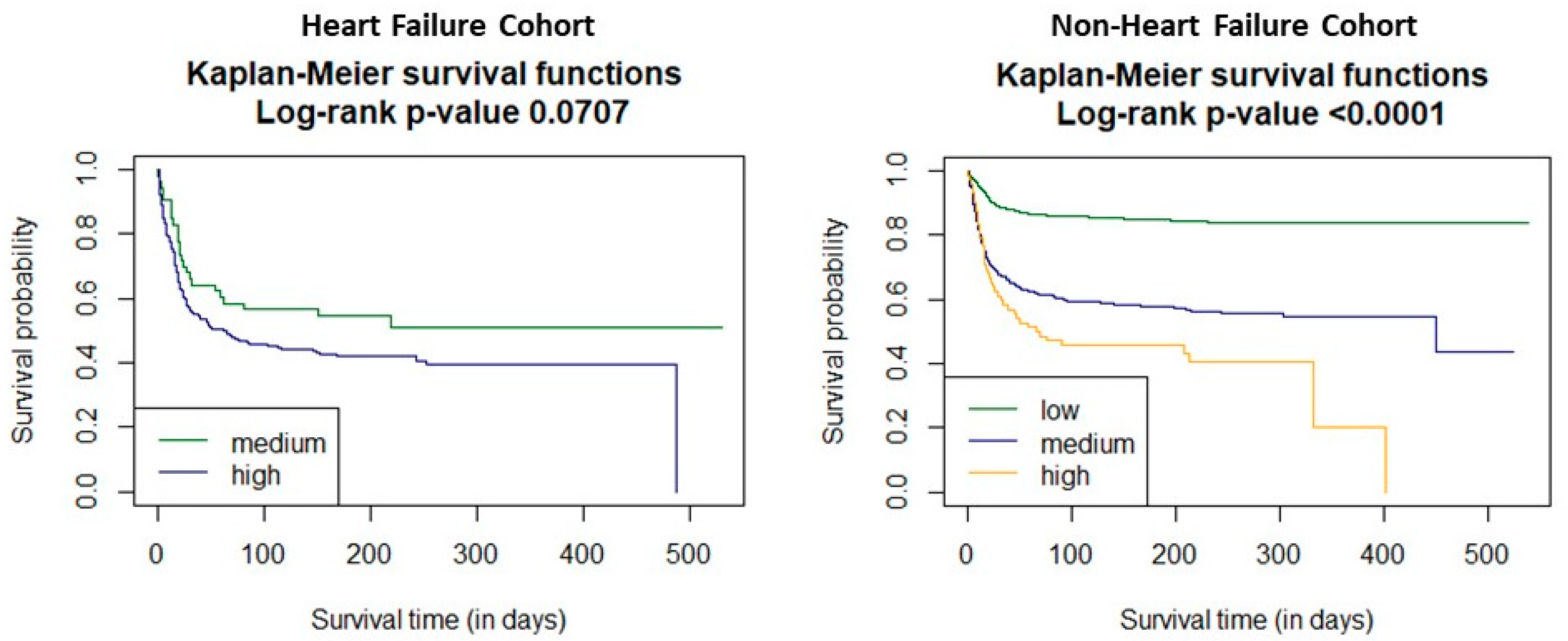
3.3. Association C2HEST Score with Results and Mortality
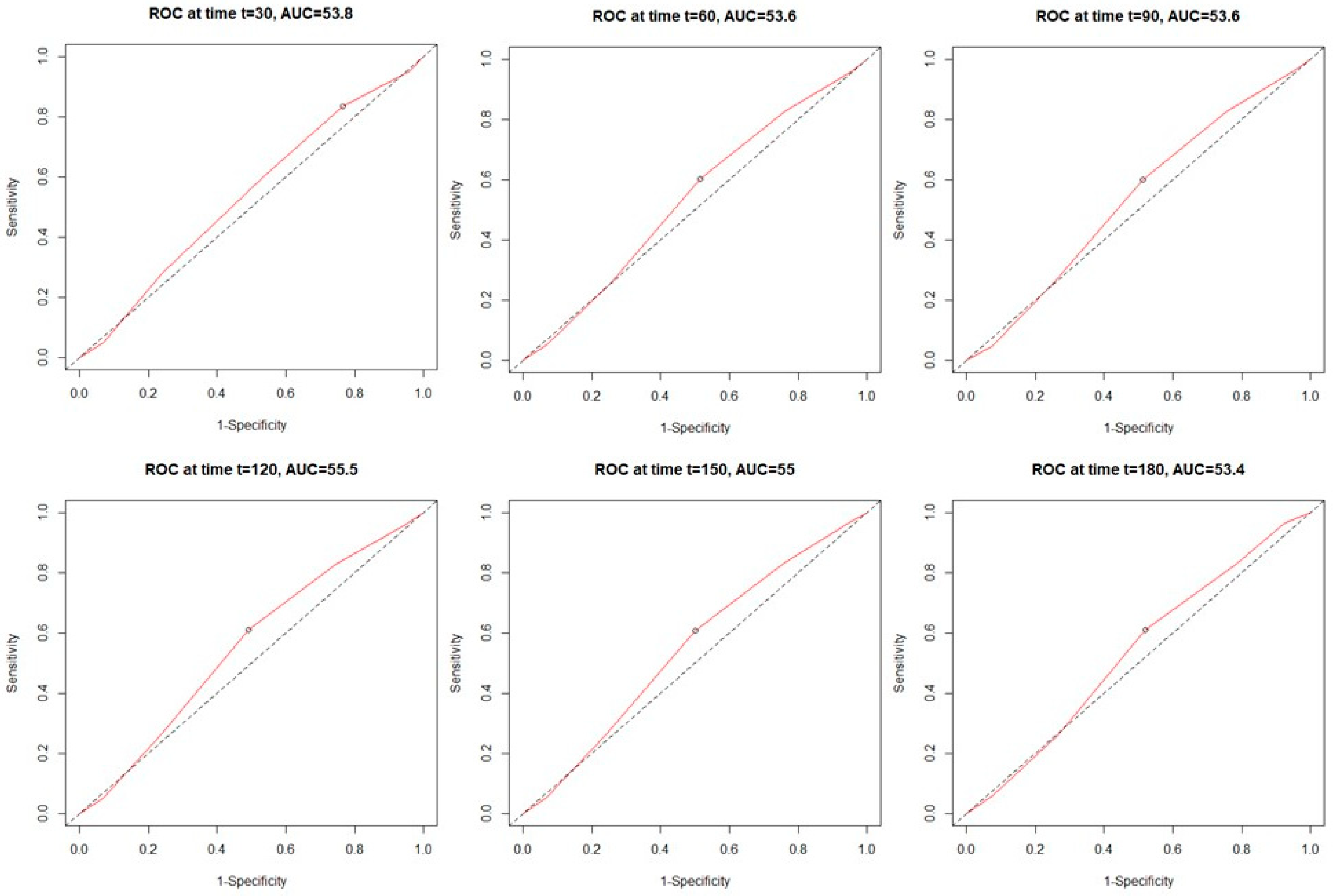
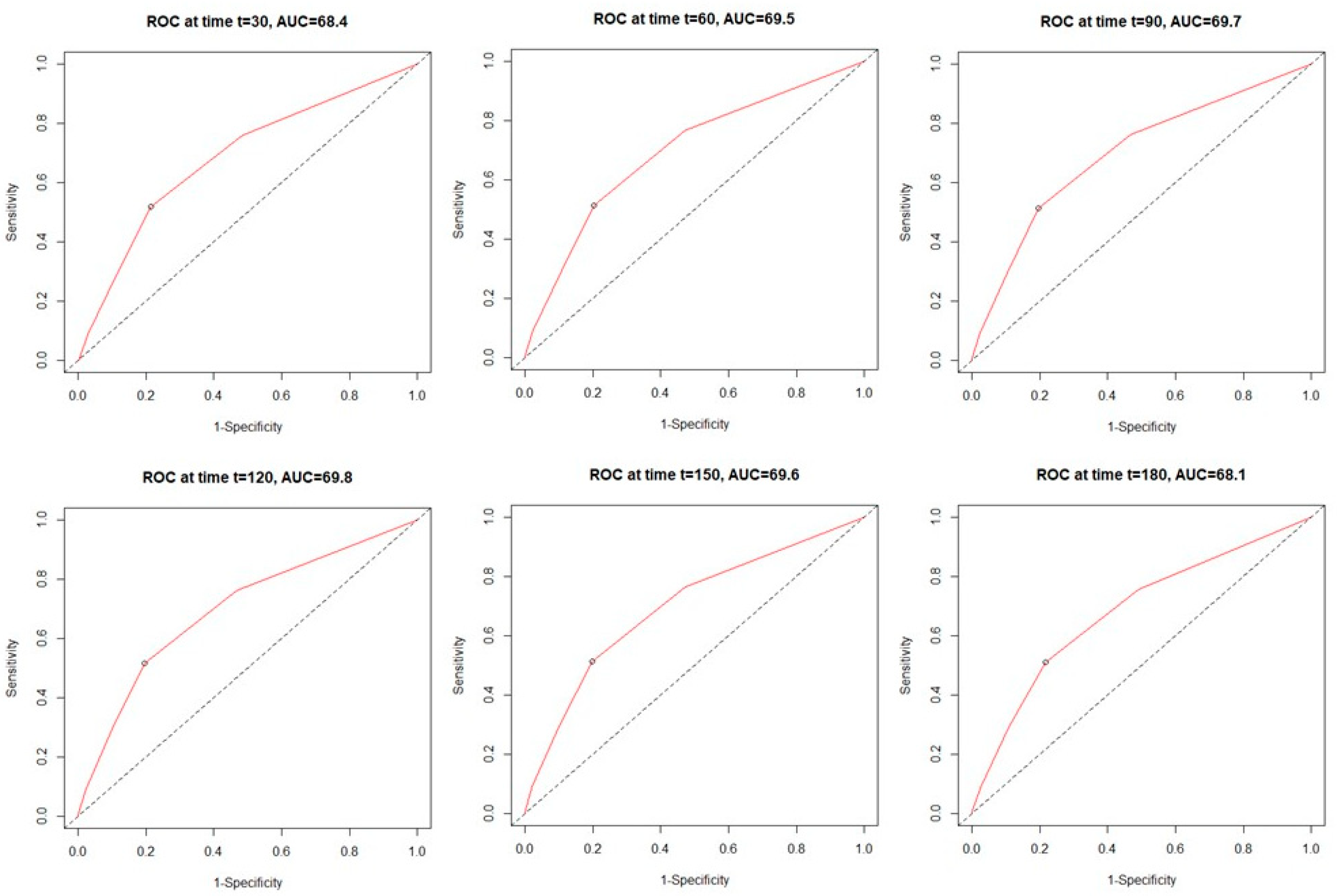
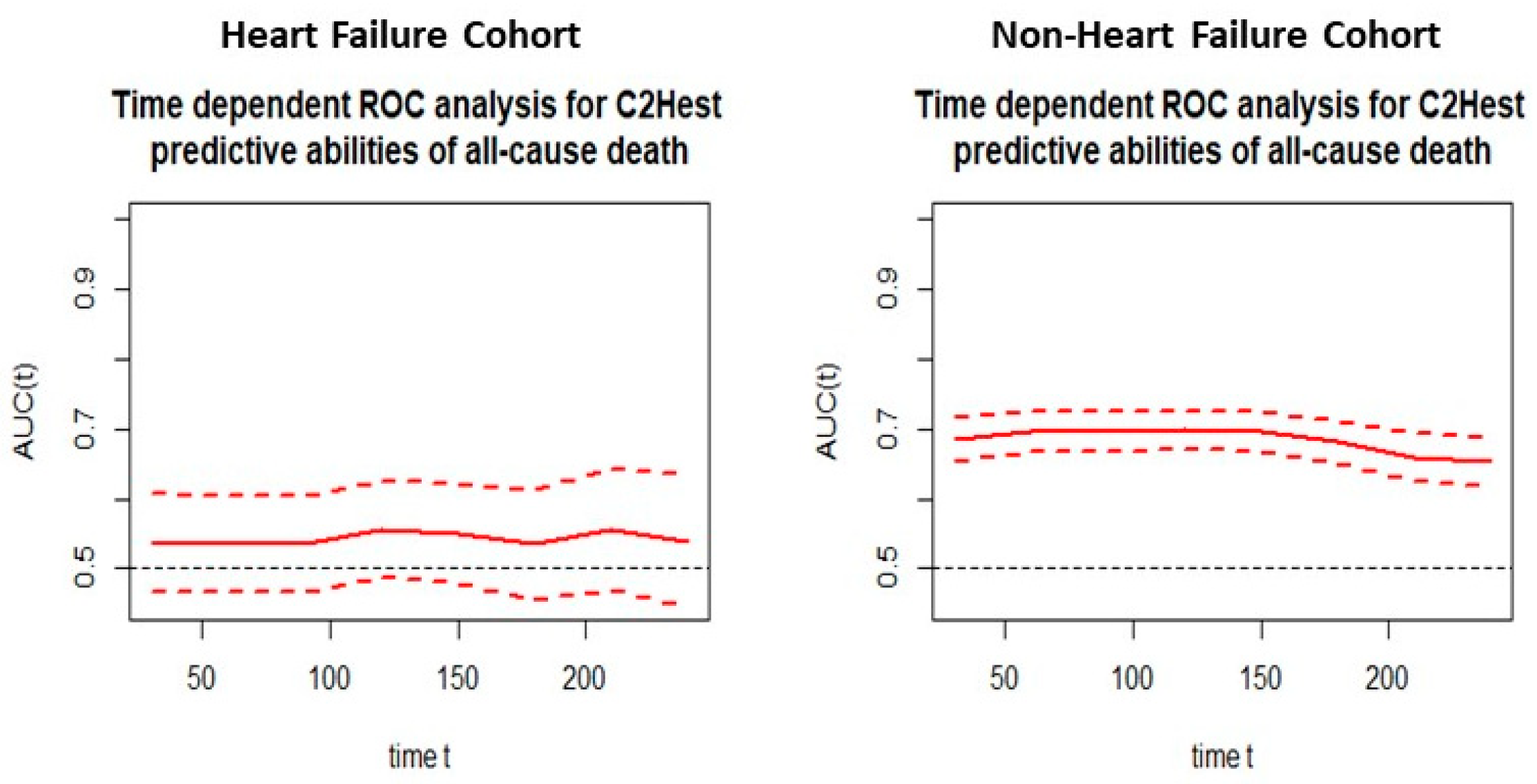
3.4. The All-Cause Mortality Discriminatory Performance of the C2HEST Score
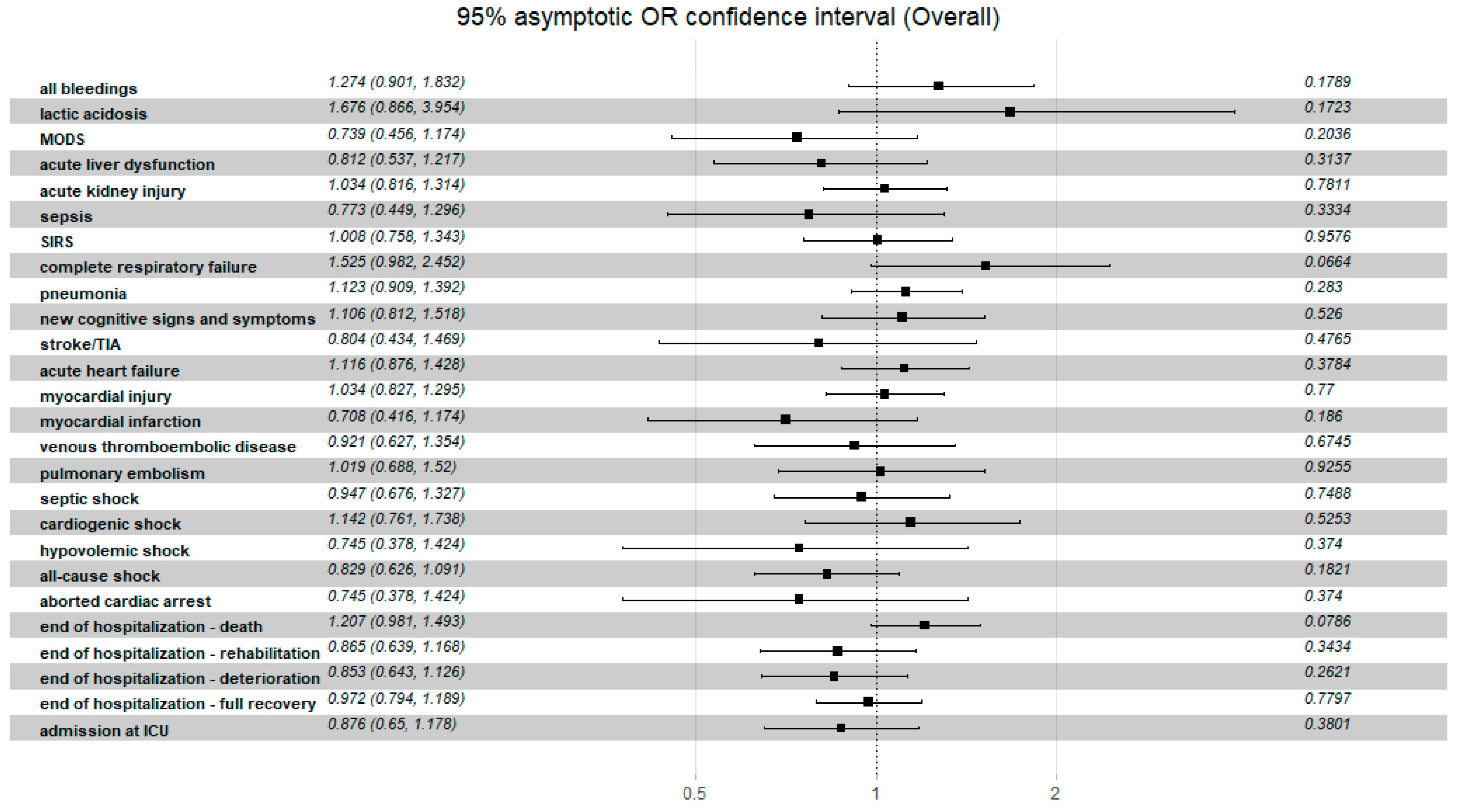
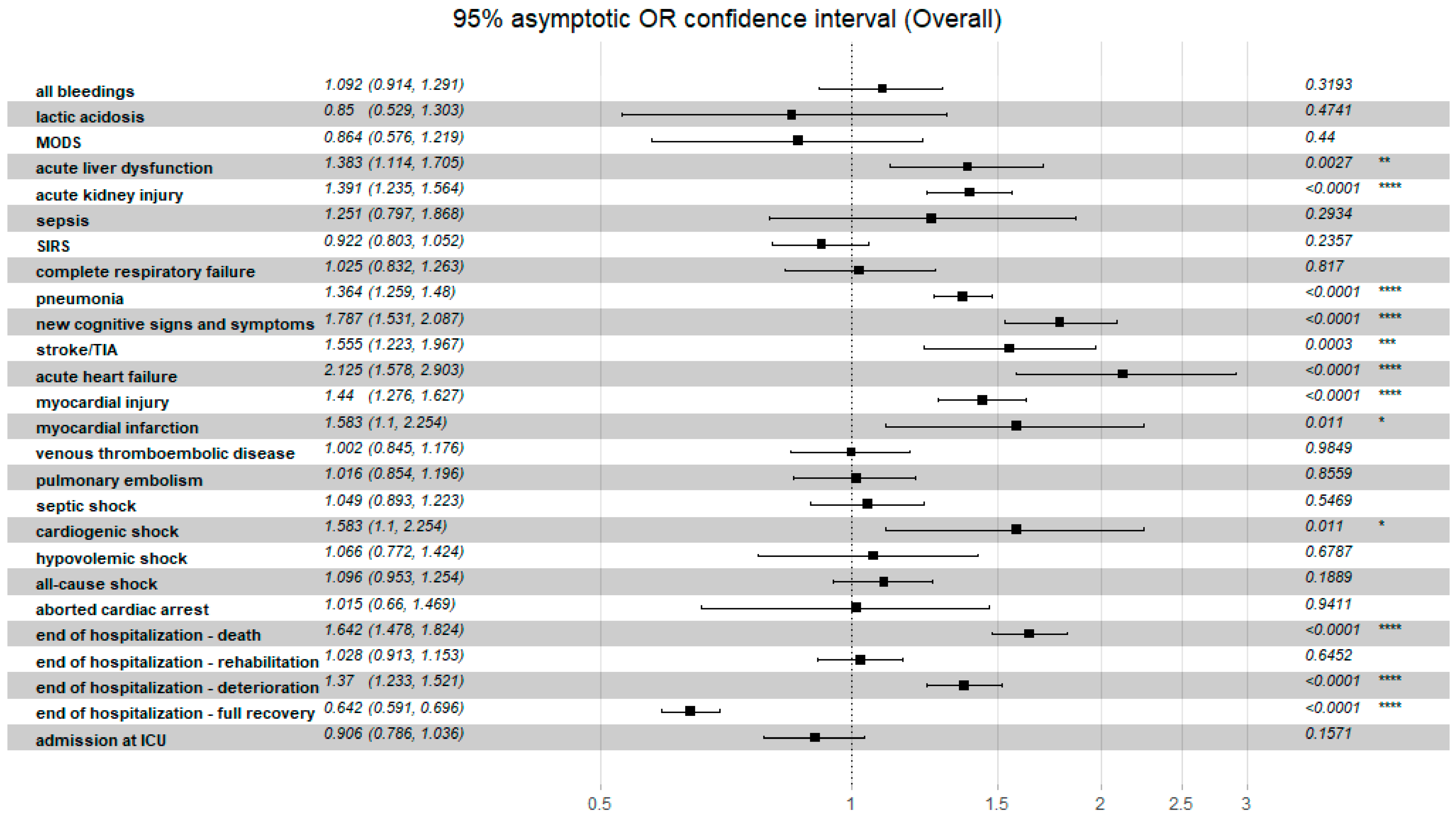
3.5. Association of C2HEST Score with Non-Fatal Outcomes
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Abejón, E.; Herrera-Gómez, F.; Martín-García, D.; Tamayo, E.; Álvarez, F.J. A Population-Based Registry Analysis on Hospitalized COVID-19 Patients with Previous Cardiovascular Disease: Clinical Profile, Treatment, and Predictors of Death. J. Cardiovasc. Dev. Dis. 2021, 8, 167. [Google Scholar] [CrossRef] [PubMed]
- Duca, A.; Piva, S.; Foca, E.; Latronico, N.; Rizzi, M. Calculated Decisions: Brescia-COVID Respiratory Severity Scale (BCRSS)/Algorithm. Emerg. Med. Pract. 2020, 22, CD1–CD2. [Google Scholar] [PubMed]
- Bader, F.; Manla, Y.; Atallah, B.; Starling, R.C. Heart failure and COVID-19. Heart Fail. Rev. 2020, 26, 1–10. [Google Scholar] [CrossRef]
- Ali, M.A.; Spinler, S.A. COVID-19 and thrombosis: From bench to bedside. Trends Cardiovasc. Med. 2021, 31, 143–160. [Google Scholar] [CrossRef]
- Li, Y.G.; Pastori, D.; Farcomeni, A.; Yang, P.S.; Jang, E.; Joung, B.; Wang, Y.T.; Guo, Y.T.; Lip, G. A simple clinical risk score (C2HEST) for predicting incident atrial fibrillation in Asian subjects: Derivation in 471,446 Chinese subjects, with internal validation and external application in 451,199 Korean subjects. Chest 2019, 155, 510–518. [Google Scholar] [CrossRef]
- Liang, W.; Wu, Y.; Xue, R.; Wu, Z.; Wu, D.; He, J.; Dong, Y.; Lip, G.Y.H.; Zhu, W.; Liu, C. C2HEST score predicts clinical outcomes in heart failure with preserved ejection fraction: A secondary analysis of the TOPCAT trial. BMC Med. 2021, 19, 44. [Google Scholar] [CrossRef]
- Rola, P.; Doroszko, A.; Trocha, M.; Giniewicz, K.; Kujawa, K.; Skarupski, M.; Gawryś, J.; Matys, T.; Szahidewicz-Krupska, E.; Gajecki, D.; et al. Mortality Predictive Value of the C2HEST Score in Elderly Subjects with COVID-19—A Subanalysis of the COLOS Study. J. Clin. Med. 2022, 11, 992. [Google Scholar] [CrossRef]
- Gajecki, D.; Doroszko, A.; Trocha, M.; Giniewicz, K.; Kujawa, K.; Skarupski, M.; Gawryś, J.; Matys, T.; Szahidewicz-Krupska, E.; Rola, P.; et al. Usefulness of the C2HEST Score in Predicting the Clinical Outcomes of COVID-19 in Diabetic and Non-Diabetic Cohorts. J. Clin. Med. 2022, 11, 873. [Google Scholar] [CrossRef]
- Rola, P.; Doroszko, A.; Trocha, M.; Giniewicz, K.; Kujawa, K.; Skarupski, M.; Gajecki, D.; Gawryś, J.; Matys, T.; Szahidewicz-Krupska, E.; et al. Sex-Dependent Differences in Predictive Value of the C2HEST Score in Subjects with COVID-19—A Secondary Analysis of the COLOS Study. Viruses 2022, 14, 628. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T. A Package for Survival Analysis in R. R Package Version 3.2-7. Available online: https://CRAN.R-project.org/package=survival (accessed on 14 June 2022).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Schratz, P. R Package ‘oddsratio’: Odds Ratio Calculation for GAM(M)s & GLM(M)s, Version: 1.0.2. Available online: https://cran.r-project.org/web/packages/oddsratio/oddsratio.pdf (accessed on 14 June 2022).
- Hothorn, T.; Hornik, K.; Van De Wiel, M.A.; Zeileis, A. A lego system for conditional inference. Am. Stat. 2006, 60, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; He, H. Assessing the accuracy of diagnostic tests. Shanghai Arch. Psychiatry 2018, 30, 207. [Google Scholar] [PubMed]
- Castagna, F.; Kataria, R.; Madan, S.; Ali, S.; Diab, K.; Leyton, C.; Arfaras-Melainis, A.; Kim, P.; Giorgi, F.; Vukelic, S.; et al. A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 77. [Google Scholar] [CrossRef]
- Villalba, G.C.; Amat-Santos, I.J.; Dueñas, C.; Otero, D.L.; Catala, P.; Aparisi, A.; López-Pais, J.; Antonio, C.E.C.; Candela, J.; Muiños, P.A.; et al. Impact of the presence of heart disease, cardiovascular medications and cardiac events on outcome in COVID-19. Cardiol. J. 2021, 28, 360–368. [Google Scholar] [CrossRef]
- Sokolski, M.; Reszka, K.; Suchocki, T.; Adamik, B.; Doroszko, A.; Drobnik, J.; Gorka-Dynysiewicz, J.; Jedrzejczyk, M.; Kaliszewski, K.; Kilis-Pstrusinska, K.; et al. History of Heart Failure in Patients Hospitalized Due to COVID-19: Relevant Factor of In-Hospital Complications and All-Cause Mortality up to Six Months. J. Clin. Med. 2022, 11, 241. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, B.Z.G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [Green Version]
- Labandeira-Garcia, J.L.; Labandeira, C.M.; Valenzuela, R.; Pedrosa, M.A.; Quijano, A.; Rodriguez-Perez, A.I. Drugs Modulating Renin-Angiotensin System in COVID-19 Treatment. Biomedicines 2022, 10, 502. [Google Scholar] [CrossRef]
- Polverino, F.; Stern, D.A.; Ruocco, G.; Balestro, E.; Bassetti, M.; Candelli, M.; Cirillo, B.; Contoli, M.; Corsico, A.; D’Amico, F.; et al. Comorbidities, Cardiovascular Therapies, and COVID-19 Mortality: A Nationwide, Italian Observational Study (ItaliCO). Front. Cardiovasc. Med. 2020, 7, 585866. [Google Scholar] [CrossRef]
- Aleksova, A.; Gagno, G.; Sinagra, G.; Beltrami, A.; Janjusevic, M.; Ippolito, G.; Zumla, A.; Fluca, A.; Ferro, F. Effects of SARS-CoV-2 on Cardiovascular System: The Dual Role of Angiotensin-Converting Enzyme 2 (ACE2) as the Virus Receptor and Homeostasis Regulator-Review. Int. J. Mol. Sci. 2021, 22, 4526. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.; Rai, D.; Tahir, M.; Wahab, A.; Bandyopadhyay, D.; Lesho, E.; Laguio-Vila, M.; Fentanes, E.; Tariq, R.; Naidu, S.; et al. Prevalence of comorbidities and symptoms stratified by severity of illness amongst adult patients with COVID-19: A systematic review. Arch. Med Sci. Atheroscler. Dis. 2022, 7, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Sisti, N.; Valente, S.; Mandoli, G.E.; Santoro, C.; Sciaccaluga, C.; Franchi, F.; Cameli, P.; Mondillo, S.; Cameli, M. COVID-19 in patients with heart failure: The new and the old epidemic. Postgrad. Med. J. 2020, 97, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Gerotziafas, G.T.; Catalano, M.; Colgan, M.-P.; Pecsvarady, Z.; Wautrecht, J.C.; Fazeli, B.; Olinic, D.-M.; Farkas, K.; Elalamy, I.; Falanga, A.; et al. Guidance for the Management of Patients with Vascular Disease or Cardiovascular Risk Factors and COVID-19: Position Paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb. Haemost. 2020, 120, 1597–1628. [Google Scholar] [CrossRef]
- Stanek, A.; Fazeli, B.; Bartuś, S.; Sutkowska, E. The Role of Endothelium in Physiological and Pathological States: New Data. BioMed Res. Int. 2018, 2018, 1098039. [Google Scholar] [CrossRef] [Green Version]
- Biegus, J.; Niewinski, P.; Josiak, K.; Kulej, K.; Ponikowska, B.; Nowak, K.; Zymlinski, R.; Ponikowski, P. Pathophysiology of Advanced Heart Failure. Hear. Fail. Clin. 2021, 17, 519–531. [Google Scholar] [CrossRef]
- Goodacre, S.; Thomas, B.; Sutton, L.; Burnsall, M.; Lee, E.; Bradburn, M.; Loban, A.; Waterhouse, S.; Simmonds, R.; Biggs, K.; et al. Derivation and validation of a clinical severity score for acutely ill adults with suspected COVID-19: The PRIEST observational cohort study. PLoS ONE 2021, 16, e0245840. [Google Scholar] [CrossRef]
- Espersen, C.; Platz, E.; Alhakak, A.S.; Sengeløv, M.; Simonsen, J.; Johansen, N.D.; Davidovski, F.S.; Christensen, J.; Bundgaard, H.; Hassager, C.; et al. Lung ultrasound findings following COVID-19 hospitalization: A prospective longitudinal cohort study. Respir. Med. 2022, 197, 106826. [Google Scholar] [CrossRef]
- Adatto, N.L.; Preisler, Y.; Shetrit, A.; Shepshelovich, D.; Hershkoviz, R.; Isakov, O. Rapid 8-Zone Lung Ultrasound Protocol is Comparable to a Full 12-Zone Protocol for Outcome Prediction in Hospitalized COVID -19 Patients. J. Ultrasound Med. 2021, 41, 15849. [Google Scholar] [CrossRef]
- Tana, C.; Ricci, F.; Coppola, M.G.; Mantini, C.; Lauretani, F.; Campanozzi, D.; Renda, G.; Gallina, S.; Lugará, M.; Cipollone, F.; et al. Prognostic Significance of Chest Imaging by LUS and CT in COVID-19 Inpatients: The ECOVID Multicenter Study. Respiration 2021, 101, 122–131. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables, Units (N) (HF/Non-HF) | Low Risk (0–1) | Medium Risk (2–3) | High Risk (≥4) | t-Test | OMNIBUS p Value | p Value for Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| Min–Max (N) or n/N (% of Risk Category) | Min–Max (N) or n/N (% of Risk Category) | Min–Max (N) or n/N (% of Risk Category) | |||||||
| HF | Non-HF | HF | Non-HF | HF | Non-HF | HF | Non-HF | ||
| Demographics | |||||||||
| Age, years (255/1929) | 51.11 ± 15.9 17–74 (1417) | 63.38 ± 9.76 36–74 (53) | 77.03 ± 11.1 29–100 (439) | 77.71 ± 10.39 38–100 (202) | 81.04 ± 4.93 73–94 (72) | <0.0001 c | <0.0001 | <0.0001 a,b,c | |
| Male gender (255/1929) | 735/1417 (51.87%) | 33/53 (62.26%) | 175/439 (39.86%) | 111/202 (54.95%) | 28/72 (38.89%) | 0.4236 c | <0.0001 | <0.0001 a 0.1274 b <0.0001 c | |
| BMI kg/m2 (69/485) | 28.28 ± 5.07 15.36–49.38 (397) | 29.36 ± 6.9 20.89–46.71 (17) | 29.27 ± 5.36 18.59–47.75 (73) | 28.12 ± 6.14 17.28–48.21 (52) | 26.67 ± 4.71 16.41–34.89 (15) | 0.5129 c | 0.146 | N/A | |
| Obesity (BMI ≥ 30 kg/m2) (69/485) | 132/397 (33.25%) | 8/17 (47.06%) | 30/73 (41.1%) | 17/52 (32.69%) | 4/15 (26.67%) | 0.7294 c | 0.3259 | N/A | |
| Cigarette smoking never previous current (255/1929) | 1337/1417 (94.35%) 46/1417 (3.25%) 34/1417 (2.4%) | 38/53 (71.7%) 8/53 (15.09%) 7/53 (13.29%) | 393/439 (90.14%) 27/439 (6.19%) 16/439 (3.67%) | 162/202 (80.2%) 24/202 (11.88%) 16/202 (7.92%) | 56/72 (78.87%) 12/72 (16.9%) 3/72 (4.23%) | 0.3396 c | <0.0001 | 0.0238 a <0.0001 b 0.0334 c | |
| Comorbidities | |||||||||
| Hypertension (255/1929) | 415/1417 (29.29%) | 36/53 (67.92%) | 321/439 (73.12%) | 179/202 (88.61%) | 70/72 (97.22%) | 0.0005 c | <0.0001 | <0.0001 a,b,c | |
| DM (255/1929) | 208/1417 (14.68%) | 20/53 (37.74%) | 126/439 (28.77%) | 94/202 (46.77%) | 24/72 (33.39%) | 0.4209 c | <0.0001 | <0.0001 a 0.0028 b 0.879 c | |
| Dyslipidemia (172/653) | 289/417 (69.3%) | 26/34 (76.47%) | 148/199 (74.37%) | 117/138 (84.78%) | 31/37 (83.78%) | 0.3661 c | 0.1034 | N/A | |
| Atrial fibrillation/flutter (255/1929) | 49/1417 (3.46%) | 22/53 (41.51%) | 84/439 (19.13%) | 112/202 (55.45%) | 23/72 (31.94%) | 0.0982 c | <0.0001 | <0.0001 a,b 0.061 c | |
| Previous coronary revascularization (255/1929) | 6/1417 (0.42%) | 4/53 (7.55%) | 33/439 (7.52%) | 89/202 (44.06%) | 22/72 (30.56%) | <0.0001 c | <0.0001 | <0.0001 a,b,c | |
| Previous myocardial infarction (255/1929) | 11/1417 (0.78%) | 4/53 (7.55%) | 59/439 (13.44%) | 88/202 (43.56%) | 29/72 (40.28%) | <0.0001 c | <0.0001 | <0.0001 a,b,c | |
| Heart failure (255/1929) | 0/1417 (0%) | 53/53 (100%) | 0/439 (0%) | 202/202 (100%) | 0/72 (0%) | <0.0001 c | <0.0001 | <0.0001 a,b,c | |
| Moderate/severe valvular heart disease or previous valve heart surgery (255/1929) | 13/1417 (0.92%) | 16/53 (30.19%) | 16/439 (3.64%) | 48/202 (23.76%) | 3/72 (4.17%) | 0.434 c | 0.0002 | 0.0007 a 0.1157 b 1.0 c | |
| Peripheral artery disease (255/1929) | 26/1417 (1.83%) | 6/53 (11.32%) | 25/439 (5.69%) | 37/202 (18.32%) | 6/72 (8.33%) | 0.3151 c | <0.0001 | 0.0002 a 0.0104 b 1.0 c | |
| Previous stroke/TIA (255/1929) | 47/1417 (3.32%) | 6/53 (11.32%) | 53/439 (12.07%) | 47/202 (23.27%) | 11/72 (15.28%) | 0.0859 c | <0.0001 | <0.0001 a 0.0002 b 1.0 c | |
| Chronic kidney disease (255/1929) | 70/1417 (4.94%) | 14/53 (26.42%) | 56/439 (12.76%) | 78/202 (38.61%) | 13/72 (18.06%) | 0.1375 c | <0.0001 | <0.0001 a,b 0.9041 c | |
| Hemodialysis (255/1929) | 19/1417 (1.34%) | 4/53 (7.55%) | 16/439 (3.64%) | 17/202 (8.42%) | 2/72 (2.78%) | 1.0 c | 0.0078 | 0.0121 a 0.8097 b 1.0 c | |
| Asthma (255/1929) | 54/1417 (3.81%) | 3/53 (5.66%) | 17/439 (3.87%) | 7/202 (3.47%) | 4/72 (5.56%) | 0.4379 c | 0.6782 | N/A | |
| COPD (255/1929) | 6/1417 (0.42%) | 0/53 (0%) | 25/439 (5.69%) | 29/202 (14.36%) | 15/72 (20.83%) | 0.0072 c | <0.0001 | <0.0001 a,b 0.0003 c | |
| Hypothyroidism (255/1929) | 76/1417 (5.36%) | 0/53 (0%) | 68/439 (15.49%) | 33/202 (16.34%) | 31/72 (43.06%) | 0.0004 c | <0.0001 | <0.0001 a,b,c | |
| Hyperthyroidism (255/1929) | 4/1417 (0.28%) | 0/53 (0%) | 10/439 (2.28%) | 7/202 (3.47%) | 0/72 (0%) | ||||
| Variables, Units (N) (HF/Non-HF) | Low-Risk (0–1) | Medium-Risk (2–3) | High-Risk (≥4) | t-Test | OMNIBUS p Value | p Value for Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| Min–Max (N) or n/N (% of Risk Category) | Min–Max (N) or n/N (% of Risk Category) | Min–Max (N) or n/N (% of Risk Category) | |||||||
| HF | Non-HF | HF | Non-HF | HF | Non-HF | HF | Non-HF | ||
| Patient-Reported Symptoms | |||||||||
| Cough (255/1929) | 455/1417 (31.11%) | 13/53 (24.53%) | 111/439 (25.28%) | 54/202 (26.73%) | 15/72 (20.83%) | 0.8814 c | 0.0053 | 0.0238 a 0.181 b 1.0 c | |
| Dyspnea (255/1929) | 569/1417 (40.16%) | 32/53 (60.38%) | 174/439 (39.64%) | 112/202 (55.45%) | 34/72 (47.22%) | 0.6249 c | 0.4661 | N/A | |
| Chest pain (255/1929) | 102/1417 (7.2%) | 8/53 (15.09%) | 26/439 (5.92%) | 21/202 (10.4%) | 6/72 (8.33%) | 0.4741 c | 0.5872 | N/A | |
| Hemoptysis (255/1929) | 9/1417 (0.64%) | 0/53 (0%) | 2/439 (0.46%) | 4/202 (1.98%) | 0/72 (0%) | 0.5831 c | 1.0 | N/A | |
| Smell dysfunction (255/1929) | 61/1417 (4.3%) | 1/53 (1.89%) | 9/439 (2.05%) | 3/202 (1.49%) | 2/72 (2.78%) | 1.0 c | 0.0731 | N/A | |
| Taste dysfunction (255/1929) | 49/1417 (3.46%) | 2/53 (3.77%) | 8/439 (1.82%) | 3/202 (1.49%) | 4/72 (5.56%) | 0.2782 c | 0.0851 | N/A | |
| Abdominal pain (255/1929) | 103/1417 (7.27%) | 2/53 (3.77%) | 24/439 (5.47%) | 14/202 (6.93%) | 3/72 (4.17%) | 0.5358 c | 0.3319 | N/A | |
| Diarrhea (255/1929) | 75/1417 (5.3%) | 2/53 (3.77%) | 31/439 (7.06%) | 14/202 (6.93%) | 5/72 (6.94%) | 0.5358 c | 0.325 | N/A | |
| Nausea/Vomiting (255/1929) | 57/1417 (4.02%) | 0/53 (0%) | 27/439 (6.15%) | 11/202 (5.45%) | 3/72 (4.17%) | 0.127 c | 0.1724 | N/A | |
| Measured Vital Signs | |||||||||
| Body temperature °C (139/1046) | 37.07 ± 0.88 34.4–40.5 (809) | 37.07 ± 1.19 35.2–40.0 (26) | 36.91 ± 0.87 35.0–40.0 (209) | 36.9 ± 0.81 35.2–40.0 (113) | 37.1 ± 1.02 36.0–40.0 (28) | 0.4907 c | 0.0797 | N/A | |
| Heart rate beats/minute (228/1444) | 86.41 ± 15.63 48–160 (1045) | 84.96 ± 17.79 54–120 (47) | 84.01 ± 16.31 50–160 (340) | 84.67 ± 19.71 36–170 (181) | 85.03 ± 15.78 54–140 (59) | 0.923 c | 0.1793 | N/A | |
| Respiratory rate breaths/minute (48/270) | 18.35 ± 5.78 12–50 (204) | 18.0 ± 4.33 14–28 (12) | 18.8 ± 5.68 12–45 (56) | 19.92 ± 6.42 12–50 (36) | 17.1 ± 4.23 12–24 (10) | 0.2538 c | 0.5575 | N/A | |
| Systolic blood pressure (231/1438) | 130.72 ± 21.28 60–240 (1040) | 126.85 ± 25.82 80–200 (46) | 135.24 ± 25.16 50–270 (339) | 134.71 ± 25.6 70-205 (185) | 133.85 ± 21.83 86-210 (59) | 0.0685 c | 0.0102 | 0.008 a 0.534 b 0.898 c | |
| Diastolic blood pressure (231/1430) | 78.55 ± 12.68 40-150 (1037) | 77.65 ± 14.27 50-110 (46) | 78.11 ± 13.6 40-157 (334) | 74.75 ± 15.24 40-120 (185) | 78.98 ± 15.16 51-143 (59) | 0.2267 c | 0.8443 | N/A | |
| SpO2 in room air, % (FiO2 = 21%) (161/1101) | 92.84 ± 7.13 48-100 (814) | 89.08 ± 11.85 50-99 (37) | 89.79 ± 9.29 50-100 (244) | 90.1 ± 9.39 50-99 (124) | 90.4 ± 5.48 74-98 (43) | 0.6345 c | <0.0001 | <0.0001 a 0.019 b 0.824 c | |
| Abnormalities Detected during Physical Examination | |||||||||
| Crackles (255/1929) | 154/1417 (10.87%) | 13/53 (24.53%) | 86/439 (19.59%) | 56/202 (27.72%) | 10/72 (13.89%) | 0.7701 c | <0.0001 | <0.0001 a 1.0 b 0.9737 c | |
| Wheezing (255/1929) | 94/1417 (6.62%) | 7/53 (13.21%) | 49/439 (11.16%) | 52/202 (25.74%) | 17/72 (23.61%) | 0.0813 c | <0.0001 | 0.0079 a <0.0001 b 0.019 c | |
| Pulmonary congestion (255/1929) | 184/1417 (12.99%) | 19/53 (35.85%) | 86/439 (19.59%) | 66/202 (32.67%) | 12/72 (16.67%) | 0.785 c | 0.0025 | 0.0024 a 1.0 b,c | |
| Peripheral oedema (255/1929) | 76/1417 (5.36%) | 14/53 (26.42%) | 46/439 (10.48%) | 44/202 (21.78%) | 9/72 (12.5%) | 0.5947 c | 0.0002 | 0.0011 a 0.0551 b 1.0 c | |
| Variables, Units (N) (HF/Non-HF) | Low-Risk (0–1) n/N | Medium-Risk (2–3) n/N | High-Risk (≥4) n/N | t-Test | OMNIBUS p Value | p Value for Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD Min–Max (N) or n/N (% of Risk Category) | Mean ± SD Min–Max (N) or n/N (% of Risk Category) | Mean ± SD Min–Max (N) or n/N (% of Risk Category) | |||||||
| HF | Non-HF | HF | Non-HF | HF | Non-HF | HF | Non-HF | ||
| Applied Treatment and Procedures | |||||||||
| The most advanced respiratory support applied during the hospitalization no oxygen (255/1928) | 0.4126 c | <0.0001 | 0.0007 a 0.0012 b 0.2081 c | ||||||
| 741/1417 | 19/53 | 183/439 | 61/202 | 28/72 | |||||
| (52.37%) | (35.85%) | (41.78%) | (30.2%) | (38.89%) | |||||
| low flow oxygen support (255/1928) | |||||||||
| 451/1417 | 19/53 | 169/439 | 90/202 | 34/72 | |||||
| (31.87%) | (35.85%) | (38.58%) | (44.55%) | (47.22%) | |||||
| high flow nasal cannula noninvasive ventilation (255/1928) | |||||||||
| 65/1417 | 3/53 | 36/439 | 21/202 | 6/72 | |||||
| (4.59%) | (5.66%) | (8.22%) | (10.4%) | (8.33%) | |||||
| invasive ventilation (255/1928) | |||||||||
| 141/1417 | 8/53 | 41/439 | 21/202 | 1/72 | |||||
| (9.96%) | (15.09%) | (9.36%) | (10.4%) | (1.39%) | |||||
| Oxygenation parameters from the period of qualification for advanced respiratory support: SpO2, % (87/544) | 90.63 ± 7.88 50–100 (410) | 88.33 ± 8.67 72–98 (12) | 86.31 ± 9.83 55–99 (121) | 84.63 ± 10.31 59–99 (75) | 91.08 ± 5.01 81–98 (13) | 0.2002 c | 0.0004 | <0.0001 a 0.948 b 0.022 c | |
| Therapy with catecholamines (255/1928) | 131/1417 (9.24%) | 7/53 (13.21%) | 38/439 (8.66%) | 38/202 (18.81%) | 4/72 (5.56%) | 0.4532 c | 0.5456 | N/A | |
| Coronary revascularization or/and an indication for coronary revascularization (255/1928) | 10/1417 (0.71%) | 4/53 (7.55%) | 8/439 (1.82%) | 8/202 (3.96%) | 0/72 (0%) | 0.2796 c | 0.0927 | N/A | |
| Hemodialysis (255/1928) | 46/1417 (3.25%) | 5/53 (9.43%) | 8/439 (1.82%) | 12/202 (5.94%) | 0/72 (0%) | 0.3601 c | 0.1196 | N/A | |
| Variables, Units (N) (HF/Non-HF) | Low-Risk (0–1) | Medium-Risk (2–3) | High-Risk (≥4) | t-Test | OMNIBUS p Value | p Value for Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| n/N (% of Risk Category) | n/N (% of Risk Category) | n/N (% of Risk Category) | |||||||
| HF | Non-HF | HF | Non-HF | HF | Non-HF | HF | Non-HF | ||
| All-Cause Mortality Rate | |||||||||
| In-hospital mortality (255/1928) | 119/1417 (8.4%) | 11/53 (20.75%) | 99/439 (22.55%) | 78/202 (38.61%) | 19/72 (26.39%) | 0.0235 c | <0.0001 | <0.0001 a,b 1.0 c | |
| 3-month mortality (255/1928) | 202/1417 (14.26%) | 23/53 (43.4%) | 175/439 (39.86%) | 109/202 (53.96%) | 38/72 (52.78%) | 0.2242 c | <0.0001 | <0.0001 a,b 0.1604 c | |
| 6-month mortality (220/1270) | 214/867 (24.68%) | 24/41 (58.54%) | 184/343 (53.64%) | 117/179 (65.36%) | 39/60 (65.0%) | 0.5212 c | <0.0001 | <0.0001 a,b 0.4074 c | |
| Total Death | |||
|---|---|---|---|
| Overall | HR | 95%CI | p Value |
| 1.100 | 0.968–1.250 | 0.143 | |
| Risk Strata | |||
| Medium-Risk vs. High-Risk | 1.465 | 0.951–2.259 | 0.085 |
| Total Death | |||
|---|---|---|---|
| Overall | HR | 95%CI | p Value |
| 1.623 | 1.518–1.734 | <0.0001 | |
| Risk Strata | |||
| Low-Risk vs. Medium-Risk | 3.414 | 2.811–4.148 | <0.0001 |
| Low-Risk vs. High-Risk | 4.953 | 3.570–6.873 | <0.0001 |
| Component | HR | CI Min. | CI Max. | p Value | |
|---|---|---|---|---|---|
| All-cause mortality | Coronary artery disease | 1.1759 | 0.8376 | 1.6509 | 0.3492 |
| COPD | 1.3432 | 0.8127 | 2.2201 | 0.2498 | |
| Age > 75 | 1.4743 | 1.0561 | 2.0581 | 0.0226 | |
| Thyroid disease | 0.5794 | 0.3476 | 0.9658 | 0.0363 | |
| Hypertension | 0.9133 | 0.5895 | 1.4151 | 0.6849 | |
| HFrEF | NA | NA | NA | NA |
| Component | HR | CI Min. | CI Max. | p Value | |
|---|---|---|---|---|---|
| All-cause mortality | Coronary artery disease | 1.8775 | 1.4009 | 2.5162 | <0.0001 |
| COPD | 1.6793 | 1.0969 | 2.5707 | 0.017 | |
| Age > 75 | 3.2112 | 2.6317 | 3.9183 | <0.0001 | |
| Thyroid disease | 0.8555 | 0.6201 | 1.1804 | 0.3421 | |
| Hypertension | 1.3936 | 1.1383 | 1.7062 | 0.0013 | |
| HFrEF | NA | NA | NA | NA |
| Variables, Units (N) (HF/Non-HF) | Low-Risk (0–1) | Medium-Risk (2–3) | High-Risk (≥4) | t-Test | OMNIBUS p Value | p Value for Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD Min–Max (N) or n/N (% of Risk Category) | Mean ± SD Min–Max (N) or n/N (% of Risk Category) | Mean ± SD Min–Max (N) or n/N (% of Risk Category) | |||||||
| HF | Non-HF | HF | Non-HF | HF | Non-HF | HF | Non-HF | ||
| Hospitalization | |||||||||
| Duration of hospitalization, days (255/1928) | 11.48 ± 13.66 1–131 (1417) | 13.34 ± 9.8 1–39 (53) | 13.16 ± 14.0 1–124 (439) | 16.02 ± 14.62 1–87 (202) | 16.25 ± 19.08 1–121 (72) | 0.1162 c | 0.0154 | 0.072 a 0.098 b 0.389 c | |
| Admission at ICU (255/1928) | 150/1417 (10.59%) | 7/53 (13.21%) | 31/439 (7.06%) | 25/202 (12.38%) | 8/72 (2.78%) | 1.0 c | 0.0125 | 0.1118 a 0.1589 b 0.7983 c | |
| End of hospitalization death (255/1928) | 119/1417 (8.4%) | 11/53 (20.75%) | 99/439 (22.55%) | 78/202 (38.61%) | 19/72 (26.39%) | 0.0606 c | <0.0001 | <0.0001 a,b 0.9339 c | |
| discharge to home– full recovery | 993/1417 (70.08%) | 23/53 (43.4%) | 197/439 (44.87%) | 75/202 (37.13%) | 20/72 (38.89%) | ||||
| transfer to another hospital—worsening | 139/1417 (9.81%) | 12/53 (22.64%) | 85/439 (19.36%) | 25/202 (12.38%) | 19/72 (26.39%) | ||||
| transfer to another hospital—in recovery | 166/1417 (11.71%) | 7/53 (13.21%) | 58/439 (13.21%) | 24/202 (11.88%) | 6/72 (8.33%) | ||||
| Aborted cardiac arrest (255/1928) | 15/1417 (1.06%) | 1/53 (1.89%) | 2/439 (0.46%) | 5/202 (2.48%) | 1/72 (1.59%) | 1.0 c | 0.3613 | N/A | |
| Shock (255/1928) | 108/1417 (7.62%) | 8/53 (15.09%) | 39/439 (8.66%) | 30/202 (14.85%) | 3/72 (4.17%) | 1.0 c | 0.3999 | N/A | |
| Hypovolemic shock (255/1928) | 22/1417 (1.55%) | 1/53 (1.89%) | 6/439 (1.37%) | 5/202 (2.48%) | 1/72 (1.39%) | 1.0 c | 1.0 | N/A | |
| Cardiogenic shock (255/1928) | 7/1417 (0.49%) | 3/53 (5.66%) | 8/439 (1.82%) | 13/202 (6.44%) | 1/72 (1.39%) | 1.0 c | 0.0196 | 0.036 a 0.9839 b 1.0 c | |
| Septic shock (255/1928) | 88/1417 (6.21%) | 4/53 (7.55%) | 26/439 (5.92%) | 20/202 (9.9%) | 2/72 (2.78%) | 0.793 c | 0.576 | N/A | |
| Venous thromboembolic disease (255/1928) | 83/1417 (5.86%) | 5/53 (9.43%) | 25/439 (5.69%) | 13/202 (6.44%) | 2/72 (2.78%) | 0.5451 c | 0.6649 | N/A | |
| Pulmonary embolism (255/1928) | 78/1417 (5.86%) | 4/53 (7.55%) | 24/439 (5.69%) | 13/202 (6.44%) | 2/72 (2.78%) | 0.2498 c | 0.98 | N/A | |
| Myocardial infarction (255/1928) | 8/1417 (0.56%) | 3/53 (5.66%) | 7/439 (0.59%) | 7/202 (3.47%) | 1/72 (1.39%) | 0.4379 c | 0.078 | N/A | |
| Myocardial injury (185/989) | 113/678 (16.67%) | 15/39 (38.46%) | 83/266 (31.2%) | 70/146 (47.95%) | 17/45 (37.78%) | 0.3816 c | <0.0001 | <0.0001 a 0.0023 b 1.0 c | |
| Acute heart failure (255/1928) | 8/1417 (0.56%) | 11/53 (20.75%) | 11/439 (2.51%) | 42/202 (20.79%) | 4/72 (5.56%) | 1.0 c | <0.0001 | 0.004 a 0.0056 b 0.7389 c | |
| Stroke/TIA (255/1928) | 18/1417 (1.27%) | 3/53 (5.66%) | 16/439 (3.64%) | 4/202 (1.98%) | 3/72 (4.17%) | 0.1591 c | 0.0023 | 0.0099 a 0.2315 b 1.0 c | |
| New cognitive signs and symptoms (255/1928) | 38/1417 (2.68%) | 7/53 (13.21%) | 44/439 (10.02%) | 22/202 (10.89%) | 10/72 (13.89%) | 0.8183 c | <0.0001 | <0.0001 a 0.0002 b 0.9175 c | |
| Pneumonia (255/1928) | 682/1417 (48.13%) | 35/53 (66.04%) | 270/439 (61.5%) | 141/202 (69.8%) | 45/72 (62.5%) | 0.7184 c | <0.0001 | <0.0001 a 0.0717 b 1.0 c | |
| Complete respiratory failure (60/216) | 57/121 (47.11%) | 5/10 (50.0%) | 41/78 (52.56%) | 36/50 (72.0%) | 7/17 (41.18%) | 0.2632 c | 0.6146 | N/A | |
| SIRS (255/1860) | 142/1352 (10.5%) | 8/53 (15.09%) | 34/436 (7.8%) | 27/202 (13.43%) | 9/72 (12.5%) | 0.9297 c | 0.1981 | N/A | |
| Sepsis (118/766) | 9/576 (1.56%) | 3/24 (12.5%) | 4/159 (2.52%) | 7/94 (7.45%) | 0/31 (0%) | 0.4228 c | 0.0077 | 0.3098 a 0.0256 b 0.9164 c | |
| Acute kidney injury (255/1928) | 110/1417 (7.76%) | 9/53 (16.98%) | 58/439 (13.21%) | 47/202 (23.27%) | 12/72 (16.67%) | 0.4252 c | 0.0003 | 0.0022 a 0.0409 b 1.0 c | |
| Acute liver dysfunction (239/1735) | 30/1256 (2.39%) | 5/50 (10.0%) | 17/415 (4.1%) | 11/189 (5.82%) | 3/64 (4.69%) | 0.338 c | 0.0951 | N/A | |
| Multiple organ dysfunction syndrome (255/1928) | 21/1417 (1.48%) | 4/53 (7.55%) | 4/439 (0.91%) | 8/202 (3.96%) | 0/72 (0%) | 0.2796 c | 0.5482 | N/A | |
| Lactic acidosis (55/190) | 9/105 (8.57%) | 0/10 (0%) | 5/69 (7.25%) | 8/45 (17.78%) | 0/16 (0%) | 0.3263 c | 0.7588 | N/A | |
| Bleedings (255/1928) | 64/1417 (4.52%) | 2/53 (3.77%) | 23/439 (5.24%) | 21/202 (10.4%) | 4/72 (5.56%) | 0.1802 c | 0.6717 | N/A | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rola, P.; Doroszko, A.; Trocha, M.; Giniewicz, K.; Kujawa, K.; Gawryś, J.; Matys, T.; Gajecki, D.; Madziarski, M.; Zieliński, S.; et al. Usefulness of C2HEST Score in Predicting Clinical Outcomes of COVID-19 in Heart Failure and Non-Heart-Failure Cohorts. J. Clin. Med. 2022, 11, 3495. https://doi.org/10.3390/jcm11123495
Rola P, Doroszko A, Trocha M, Giniewicz K, Kujawa K, Gawryś J, Matys T, Gajecki D, Madziarski M, Zieliński S, et al. Usefulness of C2HEST Score in Predicting Clinical Outcomes of COVID-19 in Heart Failure and Non-Heart-Failure Cohorts. Journal of Clinical Medicine. 2022; 11(12):3495. https://doi.org/10.3390/jcm11123495
Chicago/Turabian StyleRola, Piotr, Adrian Doroszko, Małgorzata Trocha, Katarzyna Giniewicz, Krzysztof Kujawa, Jakub Gawryś, Tomasz Matys, Damian Gajecki, Marcin Madziarski, Stanisław Zieliński, and et al. 2022. "Usefulness of C2HEST Score in Predicting Clinical Outcomes of COVID-19 in Heart Failure and Non-Heart-Failure Cohorts" Journal of Clinical Medicine 11, no. 12: 3495. https://doi.org/10.3390/jcm11123495
APA StyleRola, P., Doroszko, A., Trocha, M., Giniewicz, K., Kujawa, K., Gawryś, J., Matys, T., Gajecki, D., Madziarski, M., Zieliński, S., Skalec, T., Drobnik, J., Sebastian, A., Zubkiewicz-Zarębska, A., Adamik, B., Kaliszewski, K., Kiliś-Pstrusinska, K., Matera-Witkiewicz, A., Pomorski, M., ... Madziarska, K. (2022). Usefulness of C2HEST Score in Predicting Clinical Outcomes of COVID-19 in Heart Failure and Non-Heart-Failure Cohorts. Journal of Clinical Medicine, 11(12), 3495. https://doi.org/10.3390/jcm11123495