
The Narrowed Internal Auditory Canal: A Distinct Etiology of Pediatric Vestibular Paroxysmia

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Population
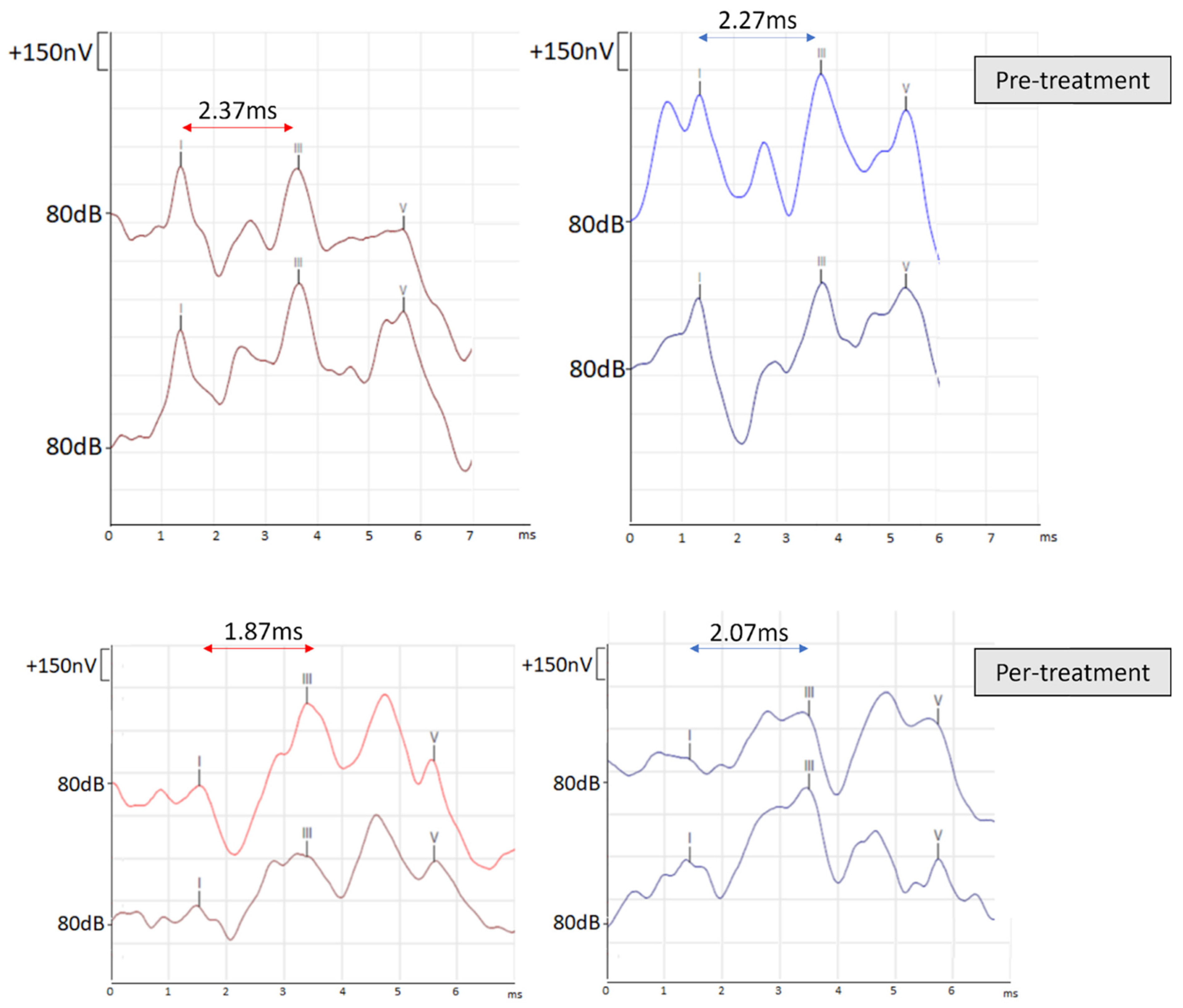
2.2. Cochleo-Vestibular Assessment
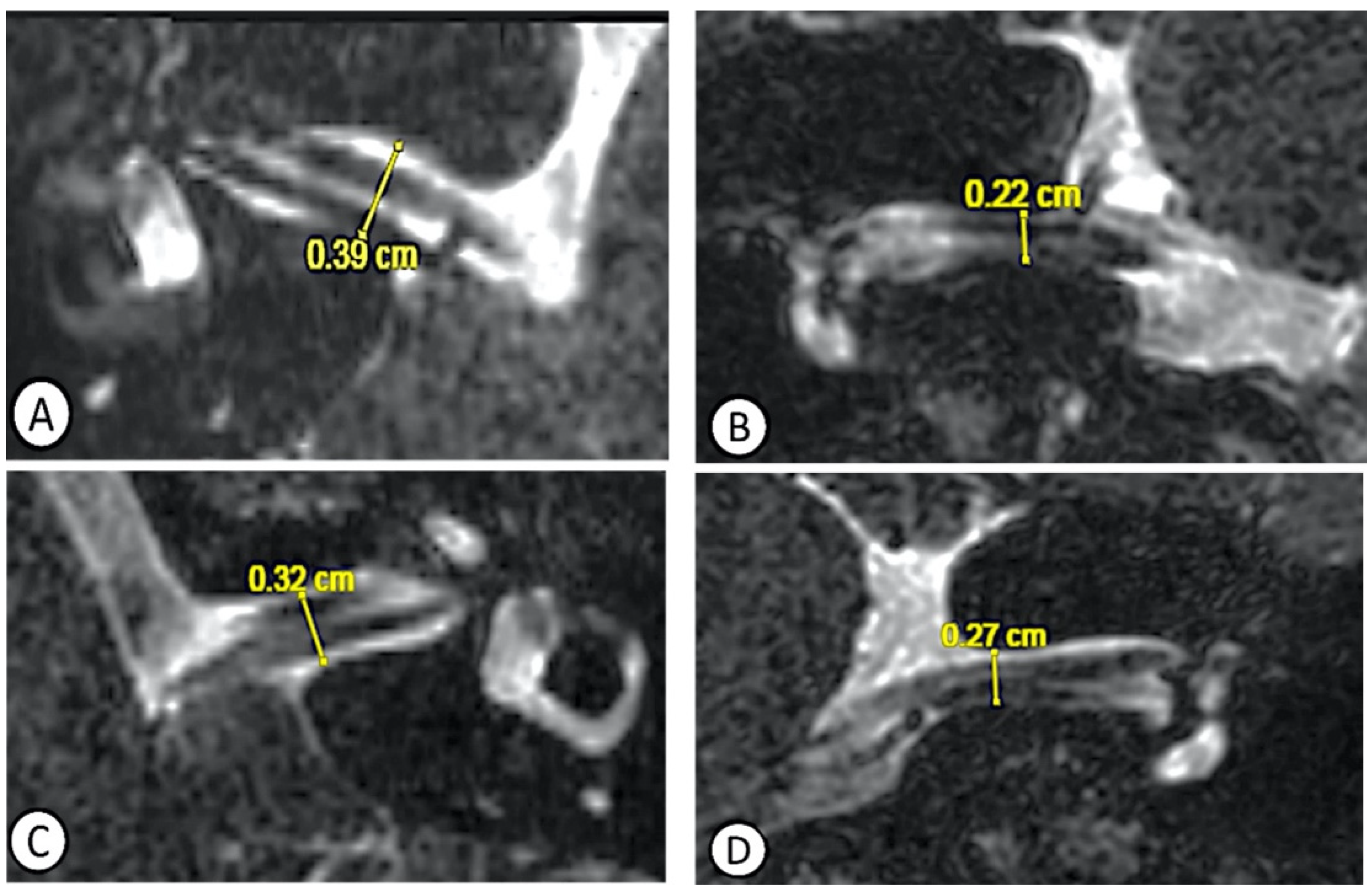
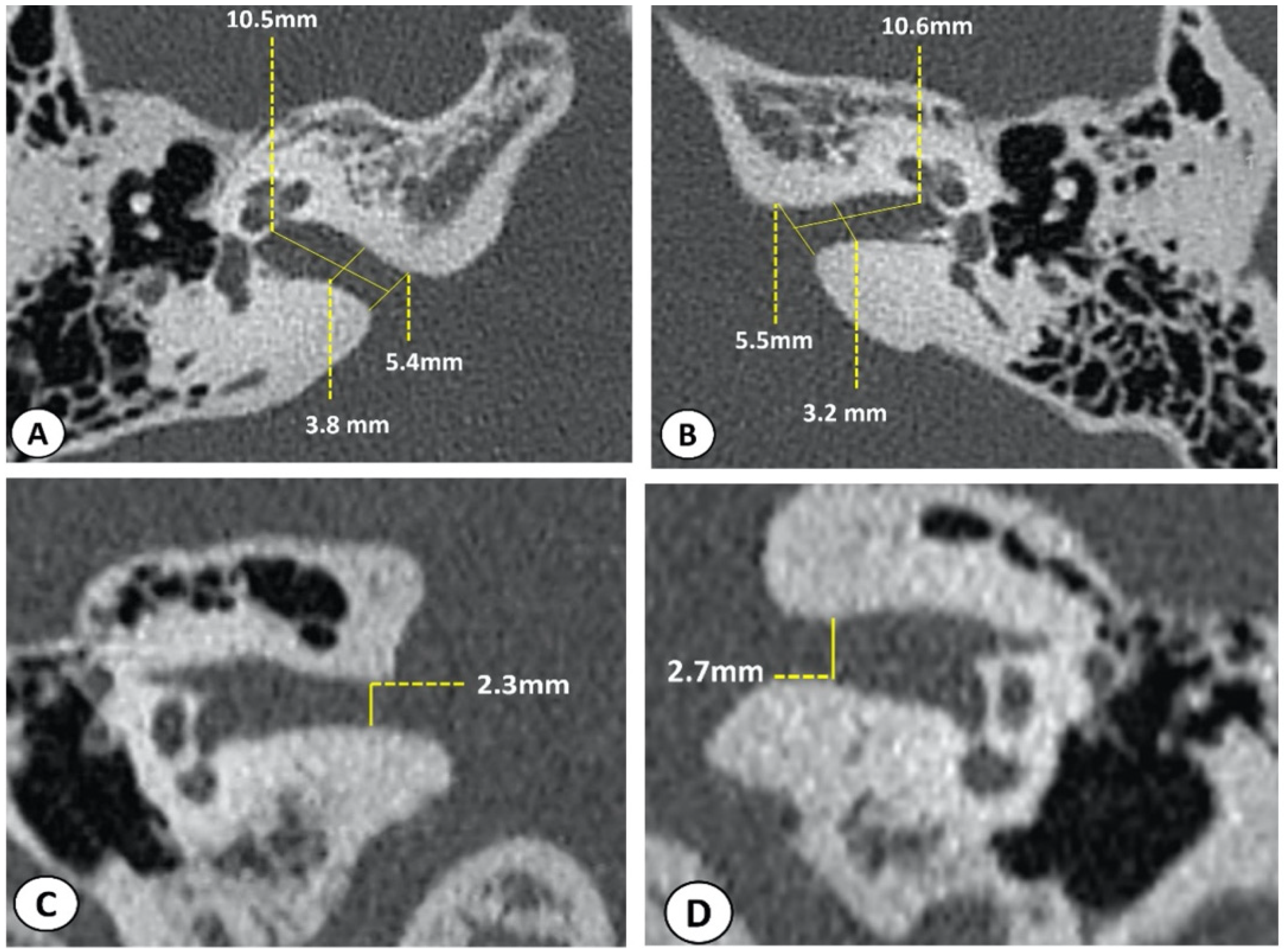
2.3. Radiological Assessment
2.4. Therapeutic Strategies
3. Results
3.1. Clinical Data
3.2. Cochleo-Vestibular Data
3.3. Radiologic Data
3.4. Therapeutic Data
3.5. Case Report
4. Discussion
4.1. The Narrowed Internal Auditory Canal
4.2. Morphometric Considerations
4.3. Therapeutic Considerations
4.4. Limitations and Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Li, N.; Georas, S.; Alexis, N.; Fritz, P.; Xia, T.; Williams, M.A.; Horner, E.; Nel, A. A Work Group Report on Ultrafine Particles (AAAAI) Why Ambient Ultrafine and Engineered Nanoparticles Should Receive Special Attention for Possible Adverse Health Outcomes in Humans. J. Allergy Clin. Immunol. 2016, 138, 386–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balzanelli, C.; Spataro, D.; Redaelli de Zinis, L.O. Prevalence of pediatric and adolescent balance disorders: Analysis of a mono-institutional series of 472 patients. Children 2021, 8, 1056. [Google Scholar] [CrossRef] [PubMed]
- Wiener-Vacher, S.R.; Quarez, J.; Priol, A. Le Epidemiology of Vestibular Impairments in a Pediatric Population. Semin. Hear. 2018, 39, 229–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodsky, J.R.; Lipson, S.; Bhattacharyya, N. Prevalence of Pediatric Dizziness and Imbalance in the United States. Otolaryngol. Head Neck Surg. 2020, 162, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Fancello, V.; Palma, S.; Monzani, D.; Pelucchi, S.; Genovese, E.; Ciorba, A. Vertigo and dizziness in children: An update. Children 2021, 8, 1025. [Google Scholar] [CrossRef]
- Brandt, T.; Dieterich, M.; Strupp, M. Vertigo and Dizziness-Common Complaints; Springer: London, UK, 2013. [Google Scholar]
- Strupp, M.; Lopez-Escamez, J.A.; Kim, J.S.; Straumann, D.; Jen, J.C.; Carey, J.; Bisdorff, A.; Brandt, T. Vestibular paroxysmia: Diagnostic criteria. J. Vestib. Res. Equilib. Orientat. 2016, 26, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Luo, R.-Z.; Wen, R.-J.; Huang, Z.-Y.; Zhou, J.-L.; Wang, X.-Y.; Chen, Q. Audiological characteristics and localization of lesions in children with retrocochlear auditory nerve impairment. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2008, 43, 336–340. [Google Scholar]
- Nachman, A.J. Retrocochlear hearing loss in infants: A case study of juvenile pilocytic astrocytoma. Int. J. Audiol. 2012, 51, 640–644. [Google Scholar] [CrossRef]
- Lehnen, N.; Langhagen, T.; Heinen, F.; Huppert, D.; Brandt, T.; Jahn, K. Vestibular paroxysmia in children: A treatable cause of short vertigo attacks. Dev. Med. Child Neurol. 2015, 57, 393–396. [Google Scholar] [CrossRef]
- Singh, N.K.; Singh, P.; Usha, M.; Akshay, M. Audio-vestibular findings in Vestibular Paroxysmia. Indian J. Otol. 2013, 19, 82–84. [Google Scholar] [CrossRef]
- Sheheitli, H.; Jirsa, V.K. A mathematical model of ephaptic interactions in neuronal fiber pathways: Could there be more than transmission along the tracts? Netw. Neurosci. 2020, 4, 595–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ridder, D.; Møller, A.; Verlooy, J.; Cornelissen, M.; Ridder, L. De Is the root entry/exit zone important in microvascular compression syndromes? Neurosurgery 2002, 51, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Brandt, T.; Strupp, M.; Dieterich, M. Vestibular paroxysmia: A treatable neurovascular cross-compression syndrome. J. Neurol. 2016, 263, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Bance, M.L.; O’ Driscoll, M.; Patel, N.; Ramsden, R.T. Vestibular disease unmasked by hyperventilation. Laryngoscope 1998, 108, 610–614. [Google Scholar] [CrossRef] [PubMed]
- CaLifano, L.; MeLiLLo, M. Hyperventilation-induced nystagmus in a large series of vestibular patients Nistagmo evocato dall’iperventilazione in un’ampia popolazione di pazienti vestibolari. ACTA Otorhinolaryngol. Ital. 2011, 31, 17–26. [Google Scholar]
- Møller, M.B. Results of microvascular decompression of the eighth nerve as treatment for disabling positional vertigo. Ann. Otol. Rhinol. Laryngol. 1990, 99, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.; Yamamoto, S.; Sugiyama, K.; Nozue, M. Neurovascular compression syndrome of the eighth cranial nerve. What are the most reliable diagnostic signs? Acta Neurochir. 1998, 140, 1279–1286. [Google Scholar] [CrossRef]
- Markowski, J.; Gierek, T.; Kluczewska, E.; Witkowska, M. Assessment of vestibulocochlear organ function in patients meeting radiologic criteria of vascular compression syndrome of vestibulocochlear nerve-diagnosis of disabling positional vertigo. Med. Sci. Monit. 2011, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Hüfner, K.; Barresi, D.; Glaser, M.; Linn, J.; Adrion, C.; Mansmann, U.; Brandt, T.; Strupp, M. Vestibular paroxysmia: Diagnostic features and medical treatment. Neurology 2008, 71, 1006–1014. [Google Scholar] [CrossRef]
- Elaini, S.; Magnan, J.; Deveze, A.; Girard, N. Magnetic resonance imaging criteria in vascular compression syndrome. Egypt J. Otolaryngol. 2013, 29, 10–1510. [Google Scholar] [CrossRef]
- Muhammad, S.; Tanikawa, R.; Niemelä, M. Surgical Treatment of Pediatric Unilateral Tinnitus Due to Cochleovestibular Nerve Compression by Intrameatal Anterior Inferior Cerebellar Artery Loop. World Neurosurg. 2019, 124, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thai-Van, H.; Fraysse, B.; Sevely, A.; DeGuine, O.; Berges, C. Does cochlear nerve aplasia always occur in the presence of a narrow internal auditory canal. Ann. Otol. Rhinol. Laryngol. 2001, 110, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Na, D.G.; Jung, J.Y.; Hong, S.H. Narrow internal auditory canal syndrome: Parasaggital reconstruction. J. Laryngol. Otol. 2000, 114, 392–394. [Google Scholar] [CrossRef] [PubMed]
- Shelton, C.; Luxford, W.M.; Tonokawa, L.L.; Lo, W.W.M.; House, W.F. The narrow internal auditory canal in children: A contraindication to cochlear implants. Otolaryngol. Neck Surg. 1989, 100, 227–231. [Google Scholar] [CrossRef]
- Fatterpekar, G.M.; Mukherji, S.K.; Lin, Y.; Alley, J.G.; Stone, J.A.; Castillo, M. Normal canals at the fundus of the internal auditory canal: CT evaluation. J. Comput. Assist. Tomogr. 1999, 23, 776–780. [Google Scholar] [CrossRef]
- Junior, I.M.; Dell’Aringa, A.R.; Nardi, J.C.; Kobari, K.; Brandão, L.A.F.; Beatriz Vieira Fernandes, L. Internal Auditory Meatus Stenosis-Case Report. Braz. J. Otorhinolaryngol. 2008, 74, 318. [Google Scholar] [CrossRef] [Green Version]
- Reynard, P.; Ionescu, E.; Ltaief-Boudrigua, A.; Thai-Van, H. A message from a narrowed internal auditory canal in a patient with a hyperpneumatized petrous bone. J. Int. Adv. Otol. 2020, 16, 485–488. [Google Scholar] [CrossRef]
- Reynard, P.; Ionescu, E.; Karkas, A.; Ltaeif-Boudrigua, A.; Thai-Van, H. Unilateral cochleovestibular nerve compression syndrome in a patient with bilateral IAC osteoma. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 213–216. [Google Scholar] [CrossRef]
- Goodarzi, A.; Toussi, A.; Garza, N.; Lechpammer, M.; Brodie, H.; Diaz, R.C.; Shahlaie, K. Internal Acoustic Canal Stenosis Due to Hyperostosis. J. Neurol. Surg. Part B Skull Base 2020, 81, 216–222. [Google Scholar] [CrossRef]
- Levens, S.L. Electronystagmography in normal children. Br. J. Audiol. 1988, 22, 51–56. [Google Scholar] [CrossRef]
- Ionescu, E.; Reynard, P.; Gouleme, N.; Becaud, C.; Spruyt, K.; Ortega-Solis, J.; Thai-Van, H. How sacculo-collic function assessed by cervical vestibular evoked myogenic Potentials correlates with the quality of postural control in hearing impaired children? Int. J. Pediatr. Otorhinolaryngol. 2020, 130, 109840. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, S.M.; Colebatch, J.G.; Young, A.S.; Govender, S.; Welgampola, M.S. Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications. Clin. Neurophysiol. Pract. 2019, 4, 47–68. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, C.; Suzuki, S.; Kinoshita, M.; Egami, N.; Sugasawa, K.; Iwasaki, S. Clinical features of otolith organ-specific vestibular dysfunction. Clin. Neurophysiol. 2018, 129, 238–245. [Google Scholar] [CrossRef]
- Shinjo, Y.; Jin, Y.; Kaga, K. Assessment of vestibular function of infants and children with congenital and acquired deafness using the ice-water caloric test, rotational chair test and vestibular-evoked myogenic potential recording. Acta Otolaryngol. 2007, 127, 736–747. [Google Scholar] [CrossRef]
- Valente, M. Maturational effects of the vestibular system: A study of rotary chair, computerized dynamic posturography, and vestibular evoked myogenic potentials with children. J. Am. Acad. Audiol. 2007, 18, 461–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casselbrant, M.L.; Mandel, E.M.; Sparto, P.J.; Perera, S.; Redfern, M.S.; Fall, P.A.; Furman, M. Years of age: Normative data. Head Neck 2011, 142, 708–714. [Google Scholar] [CrossRef]
- Staller, S.J.; Goin, D.W.; Hildebrandt, M. Pediatric vestibular evaluation with harmonic acceleration. Otolaryngol. Neck Surg. 1986, 95, 471–474. [Google Scholar] [CrossRef]
- Alhabib, S.F.; Saliba, I. Video head impulse test: A review of the literature. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1215–1222. [Google Scholar] [CrossRef]
- Rabbitt, R.D. Directional coding of three-dimensional movements by the vestibular semicircular canals. Biol. Cybern. 1999, 80, 417–431. [Google Scholar] [CrossRef]
- Wiener-Vacher, S.R.; Wiener, S.I. Video head impulse tests with a remote camera system: Normative values of semicircular canal vestibulo-ocular reflex gain in infants and children. Front. Neurol. 2017, 8, 434. [Google Scholar] [CrossRef] [Green Version]
- Alizadeh, S.; Rahbar, N.; Ahadi, M.; Sameni, S.J. Normative vestibulo-ocular reflex data in 6–12 year-old children using video head-impulse test. Audit. Vestib. Res. 2017, 26, 145–150. [Google Scholar]
- Bonaldi, L.V.; do Lago, A.; Crema, L.C.; Fukuda, Y.; Smith, R.L. Internal auditory canal: Pre- and postnatal growth. J. Otolaryngol. 2004, 33, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.R.; Ajzen, S.; D’Ippolito, G.; Alonso, L.; Isotani, S.; Lederman, H. Morphometric Analysis of the Internal Auditory Canal by Computed Tomography Imaging. Iran. J. Radiol. 2012, 9, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Sadik, A.O.; Shaaban, M.H. The relationship between the dimensions of the internal auditory canal and the anomalies of the vestibulocochlear nerve. Folia Morphol. 2017, 76, 178–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janky, K.L.; Rodriguez, A.I. Quantitative Vestibular Function Testing in the Pediatric Population. Semin. Hear. 2018, 39, 257–274. [Google Scholar] [CrossRef]
- Lescanne, E.; Velut, S.; Lefrancq, T.; Destrieux, C. The internal acoustic meatus and its meningeal layers: A microanatomical study. J. Neurosurg. 2002, 97, 1191–1197. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, A.; Sharma, S. Vestibular Paroxysmia with Trigeminal Neuralgia: Simultaneous Occurrence of Two Compression Syndromes: A Rare Case Report. Ann. Otol. Neurotol. 2020, 3, 90–92. [Google Scholar] [CrossRef] [Green Version]
- Verbiest, H. Stenosis of the lumbar vertebral canal and sciatica. Neurosurg. Rev. 1980, 3, 75–89. [Google Scholar] [CrossRef]
- Schmid, A.B.; Fundaun, J.; Tampin, B. Entrapment neuropathies: A contemporary approach to pathophysiology, clinical assessment, and management. Pain Rep. 2020, 5, e829. [Google Scholar] [CrossRef]
- Baek, S.K.; Chae, S.W.; Hung, H.H. Congenital Internal Auditory Canal Stenosis With Facial Palsy. J. Laryngol. Otol. 2003, 117, 784–787. [Google Scholar] [CrossRef]
- Sakina, M.S.; Goh, B.S.; Abdullah, A.; Zulfiqar, M.A.; Saim, L. Internal auditory canal stenosis in congenital sensorineural hearing loss. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 2093–2097. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Koda, J.; Koike, Y. Stenosis of the internal auditory canal with VIIth and VIIIth cranial nerve dysfunctions. ORL 1999, 61, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Best, C.; Gawehn, J.; Krämer, H.H.; Thömke, F.; Ibis, T.; Müller-Forell, W.; Dieterich, M. MRI and neurophysiology in vestibular paroxysmia: Contradiction and correlation. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1349–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, M. Cranio-cervical growth collision: Another explanation of the Arnold-Chiari malformation and of basilar impression. Neuroradiology 1986, 28, 187–194. [Google Scholar] [CrossRef]
- Sakashita, T.; Sando, I. Postnatal development of the internal auditory canal studied by computer-aided three-dimensional reconstruction and measurement. Ann. Otol. Rhinol. Laryngol. 1995, 194, 469–476. [Google Scholar] [CrossRef]
- Roth, M. Reciprocity of the neural growth in the Arnold-Chiari malformation. Acta Radiol. Suppl. 1986, 369, 26061. [Google Scholar]
- Zidan, M.A.; Almansor, N. Presence of vascular loop in patients with audio-vestibular symptoms: Is it a significant finding? Evaluation with 3-tesla MRI 3D constructive interference steady state (CISS) sequence. Egypt J. Radiol. Nucl. Med. 2020, 51, 114. [Google Scholar] [CrossRef]
- Yoo, H.S.; Lee, D.W.; Min, H.J.; Lee, S.H.; Park, C.W. The association of anterior inferior cerebellar artery in internal auditory canal with tinnitus and hearing loss. Korean J. Audiol. 2011, 15, 67–71. [Google Scholar]
- Kim, M.; Chu, H.; Song, M.Y.; Lee, S.D.; Kim, H.N. Relationship between Vestibulocochlear Symptoms and Types of the Anterior Inferior Cerebellar Artery (AICA) Pathway in Cerebellopontine Angle. J. Clin. Otolaryngol. Head Neck Surg. 2012, 23, 74–78. [Google Scholar] [CrossRef]
- Gorrie, A.; Warren, F.M.; De La Garza, A.N.; Shelton, C.; Wiggins, R.H. Is there a correlation between vascular loops in the cerebellopontine angle and unexplained unilateral hearing loss? Otol. Neurotol. 2010, 31, 48–52. [Google Scholar] [CrossRef]
- Reka, D.; Anand, A.; Kulasekaran, N.; Balachandran, G.; Elamparidhi, P.; Sibhithran, R. Vascular Loops at the Cerebellopontine Angle and their Correlation with Otological Symptoms. Int. J. Anat. Radiol. Surg. 2019, 8, 11–14. [Google Scholar] [CrossRef]
- McDermott, A.L.; Dutt, S.N.; Irving, R.M.; Pahor, A.L.; Chavda, S.V. Anterior inferior cerebellar artery syndrome: Factor or fiction. Clin. Otolaryngol. Allied Sci. 2003, 28, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Telano, L.N.; Baker, S. Physiology, Cerebral Spinal Fluid. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519007/ (accessed on 22 May 2022).
- Schizas, C.; Theumann, N.; Burn, A.; Tansey, R.; Wardlaw, D.; Smith, F.W.; Kulik, G. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine 2010, 35, 1919–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preuss, C.V.; Randhawa, G.; Wy, T.J.P.; Saadabadi, A. Oxcarbazepine. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482313/ (accessed on 23 May 2022).
- Nordang, L.; Oestreicher, E.; Arnold, W.; Anniko, M. Glutamate is the afferent neurotransmitter in the human cochlea. Acta Otolaryngol. 2000, 120, 359–362. [Google Scholar] [CrossRef]
- Hamed, S.A. The auditory and vestibular toxicities induced by antiepileptic drugs. Expert Opin. Drug Saf. 2017, 16, 1281–1294. [Google Scholar] [CrossRef]
- Hamed, S.A.; Oseily, A.M. Peripheral and central auditory function in adults with epilepsy and treated with carbamazepine. Hear. Balanc. Commun. 2019, 17, 257–265. [Google Scholar] [CrossRef]
- Boylu, E.; Domaç, F.M.; Misirli, H.; Senol, M.G.; Saraçòlu, M. Effects of the antiepileptic drugs on peripheral nerve function. Acta Neurol. Scand. 2010, 121, 7–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | Vestibular Symptoms (Other than VP) | Auditory Symptoms | Pure Tone Audiogram | Spontaneous Nystagmus | Hyperventilation Maneuver | |
|---|---|---|---|---|---|---|---|
| Group 1 | |||||||
| 1 | M | 8 | None | Absent | N | Absent | Absent |
| 2 | F | 12 | None | Absent | N | (L) horizontal | Absent |
| 3 | F | 15 | None | (R) Hypoacusis | (R) SNHL | (R) horizontal | Absent |
| 4 | M | 15 | Effort-induced vertigo | Absent | N | (R) superior | (R) inferior |
| 5 | F | 16 | Positional vertigo Effort-induced vertigo (L) Retro auricular pain | Absent | N | Absent | Absent |
| 6 | F | 16 | None | Absent | N | Absent | Absent |
| 7 | F | 17 | None | Absent | (x2) moderate HL | (R) horizontal | (L) Nystagmus |
| 8 | F | 18 | None | Bilateral tinnitus | N | (L) horizontal | (R) horizontal |
| Group 2 | |||||||
| 1 | M | 5 | Imbalance | Absent | (L) severe HL | Absent | Absent |
| 2 | F | 6 | Imbalance | Absent | N | Absent | Absent |
| 3 | M | 6 | None | Absent | N | Absent | Absent |
| 4 | F | 8 | Imbalance | Bilateral tinnitus | N | (R) horizontal | Absent |
| 5 | F | 12 | (L) Retro auricular pain | Absent | N | (R) horizontal | Accentuation of nystagmus |
| 6 | F | 13 | Imbalance | Absent | N | (R) horizontal | Accentuation of nystagmus |
| 7 | M | 14 | None | Absent | N | Absent | (L) nystagmus |
| 8 | F | 16 | Retro auricular pain | (L) fluctuating | (L) moderate HL | Absent | Absent |
| ABR I–III Interval | VOR | vHIT | VEMPs | ||
|---|---|---|---|---|---|
| (R) | (L) | ||||
| Group 1 | |||||
| 1 | 2.12 | 2.28 | N | Decreased gain (x2) | N |
| 2 | 2.2 | 2.3 | (R) decreased responses | N | N |
| 3 | 2.42 | 2.46 | N | Decreased gain PC (x2) | N |
| 4 | 2.37 | 2.46 | Bilateral decreased responses | N | N |
| 5 | 2.27 | 2.37 | N | N | N |
| 6 | 2.5 | 2.5 | N | N | N |
| 7 | 2.04 | No response | N | Decreased gain LAC & LLC | N |
| 8 | 1.96 | 1.92 | Bilateral decreased responses | N | N |
| Group 2 | |||||
| 1 | 1.83 | 2.25 | N | Decreased gain LPC | Absent (L) |
| 2 | 2.2 | 2.37 | (R) decreased responses | N | Absent (R) |
| 3 | 2.20 | 2.20 | N | N | Absent (R) |
| 4 | 2.50 | 2.10 | N | N | Absent (R) |
| 5 | 2.21 | 2.33 | N | Decreased gain RLC | N |
| 6 | 2.07 | 2.10 | N | N | N |
| 7 | 2.23 | 2.23 | (L) decreased responses | N | N |
| 8 | 2.36 | 2.36 | N | N | N |
| Group 1 | ||||
|---|---|---|---|---|
| MRI | CT Scan of Temporal Bones + IAC Measurements (mm) | Conclusion | ||
| Right | Left | |||
| 1 | The internal auditory canals are small in size bilaterally. |
|
| Bilateral narrowing of the CC caliber of IACs, more marked on the left side. |
| 2 | The internal auditory canals are small in size bilaterally. |
|
| Bilateral narrowing of the CC caliber of IACs, more marked on the right side. |
| 3 | Bifid aspect of the left saccule. The internal auditory canals are small in size bilaterally. |
|
| Right narowing of the CC caliber of the IACs. |
| 4 | The internal auditory canals are small in size bilaterally. |
|
| Bilateral narrowing of the CC caliber of the IACs. |
| 5 | Narrowing of the IAC in their CC caliber more marked on the right. |
|
| Bilateral narrowing of the CC caliber of the IACs, more marked on the right side. |
| 6 | The internal auditory canals are small in size bilaterally. |
|
| Bilateral narrowing of the CC caliber of IACs, more marked on the right side. |
| 7 | Bilateral IAC narrowing |
|
| Bilateral narrowing of the CC caliber of the IACs, more marked on the right side. |
| 8 | The internal auditory canals are small in size bilaterally. |
|
| Bilateral narrowing of the CC caliber of the IACs, more marked on the left side. |
| Group 2 | ||||
| MRI | ||||
| 1 | Left PICA vascular loop in contact with the cisternal emergence of the left acoustic facial bundle. | |||
| 2 | Vascular loop at the level of the left APC; close contact between the left AICA and the acoustic-facial bundle at this level. | |||
| 3 | Vascular loop at the level of the right APC | |||
| 4 | Arterial vascular loop of the right AICA having a double contact with the cisternal path of the right nerve VIII, especially at the porus, in RE Z zone, without deviation of the neural structure. | |||
| 5 | Double contact between an AICA at the emergence of the VIII on the right. | |||
| 6 | Neurovascular compression syndrome on the right-sided bundle of NC VIII with a moderate mass effect on the nerve structure (pathogenic appearance). | |||
| 7 | Intimate contact of the APC between VII and VIII with right PICA. | |||
| 8 | Vascular-nerve contact between the left AICA and the left acoustic-facial bundle at the level of the IAC porus. This contact is orthogonal with the G facial nerve and VIII G. Mass effect on VIII questionable in transitional zone. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idriss, S.A.; Thai-Van, H.; Altaisan, R.; Ltaief-Boudrigua, A.; Reynard, P.; Ionescu, E.C. The Narrowed Internal Auditory Canal: A Distinct Etiology of Pediatric Vestibular Paroxysmia. J. Clin. Med. 2022, 11, 4300. https://doi.org/10.3390/jcm11154300
Idriss SA, Thai-Van H, Altaisan R, Ltaief-Boudrigua A, Reynard P, Ionescu EC. The Narrowed Internal Auditory Canal: A Distinct Etiology of Pediatric Vestibular Paroxysmia. Journal of Clinical Medicine. 2022; 11(15):4300. https://doi.org/10.3390/jcm11154300
Chicago/Turabian StyleIdriss, Samar A., Hung Thai-Van, Riham Altaisan, Aicha Ltaief-Boudrigua, Pierre Reynard, and Eugen Constant Ionescu. 2022. "The Narrowed Internal Auditory Canal: A Distinct Etiology of Pediatric Vestibular Paroxysmia" Journal of Clinical Medicine 11, no. 15: 4300. https://doi.org/10.3390/jcm11154300
APA StyleIdriss, S. A., Thai-Van, H., Altaisan, R., Ltaief-Boudrigua, A., Reynard, P., & Ionescu, E. C. (2022). The Narrowed Internal Auditory Canal: A Distinct Etiology of Pediatric Vestibular Paroxysmia. Journal of Clinical Medicine, 11(15), 4300. https://doi.org/10.3390/jcm11154300