
New Oral Antitumor Drugs and Medication Safety in Uro-Oncology: Implications for Clinical Practice Based on a Subgroup Analysis of the AMBORA Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Design
2.2. Data Collection
2.3. Medication Review
2.4. Typology of Medication Errors
2.5. Medication Safety Table
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Medication Errors
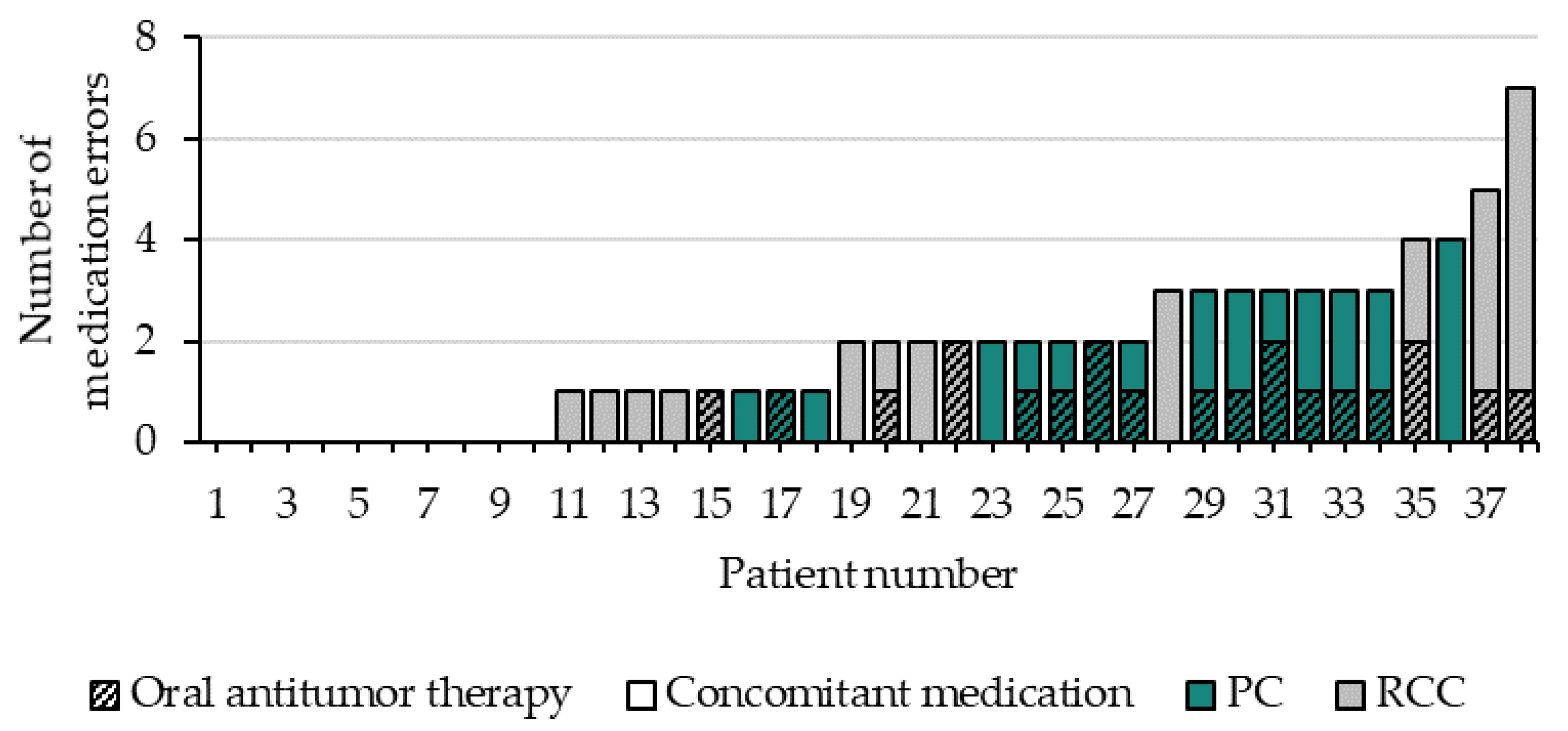
3.2.1. Numbers and Involved Medicines
3.2.2. Typology of Medication Errors
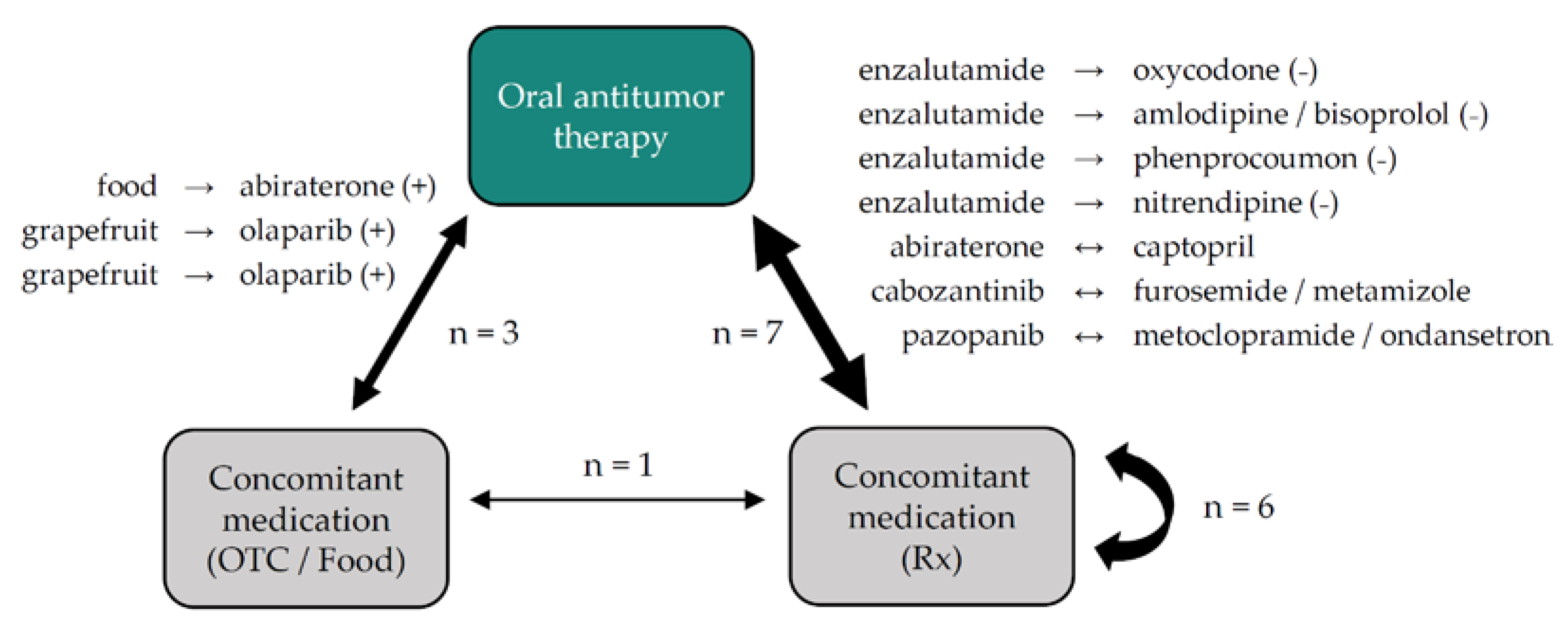
3.2.3. Drug–Drug and Drug–Food Interactions
3.3. Medication Safety Table
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zarrabi, K.; Paroya, A.; Wu, S. Emerging therapeutic agents for genitourinary cancers. J. Hematol. Oncol. 2019, 12, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlichtig, K.; Dürr, P.; Dörje, F.; Fromm, M.F. New oral anti-cancer drugs and medication safety. Dtsch. Arztebl. Int. 2019, 116, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Aisner, J. Overview of the changing paradigm in cancer treatment: Oral chemotherapy. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2007, 64, 4–7. [Google Scholar] [CrossRef]
- Weingart, S.N.; Toro, J.; Spencer, J.; Duncombe, D.; Gross, A.; Bartel, S.; Miransky, J.; Partridge, A.; Shulman, L.N.; Connor, M. Medication errors involving oral chemotherapy. Cancer 2010, 116, 2455–2464. [Google Scholar] [CrossRef] [PubMed]
- Zerillo, J.A.; Goldenberg, B.A.; Kotecha, R.R.; Tewari, A.K.; Jacobson, J.O.; Krzyzanowska, M.K. Interventions to improve oral chemotherapy safety and quality: A systematic review. JAMA Oncol. 2018, 4, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Weingart, S.N.; Zhang, L.; Sweeney, M.; Hassett, M. Chemotherapy medication errors. Lancet Oncol. 2018, 19, e191–e199. [Google Scholar] [CrossRef]
- van Leeuwen, R.W.F.; Brundel, D.H.S.; Neef, C.; van Gelder, T.; Mathijssen, R.H.J.; Burger, D.M.; Jansman, F.G.A. Prevalence of potential drug-drug interactions in cancer patients treated with oral anticancer drugs. Br. J. Cancer 2013, 108, 1071–1078. [Google Scholar] [CrossRef] [Green Version]
- Greer, J.A.; Amoyal, N.; Nisotel, L.; Fishbein, J.N.; MacDonald, J.; Stagl, J.; Lennes, I.; Temel, J.S.; Safren, S.A.; Pirl, W.F. A systematic review of adherence to oral antineoplastic therapies. Oncologist 2016, 21, 354–376. [Google Scholar] [CrossRef] [Green Version]
- Snyder, R.A.; Abarca, J.; Meza, J.L.; Rothschild, J.M.; Rizos, A.; Bates, D.W. Reliability evaluation of the adapted national coordinating council medication error reporting and prevention (NCC MERP) index. Pharmacoepidemiol. Drug Saf. 2007, 16, 1006–1013. [Google Scholar] [CrossRef]
- Spratt, D.E.; Shore, N.; Sartor, O.; Rathkopf, D.; Olivier, K. Treating the patient and not just the cancer: Therapeutic burden in prostate cancer. Prostate Cancer Prostatic Dis. 2021, 24, 647–661. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Zurawski, B.; Oyervides Juárez, V.M.; Hsieh, J.J.; Basso, U.; Shah, A.Y.; et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2021, 384, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Holle, L.M.; Puri, S.; Clement, J.M. Physician-pharmacist collaboration for oral chemotherapy monitoring: Insights from an academic genitourinary oncology practice. J. Oncol. Pharm. Pract. Off. Publ. Int. Soc. Oncol. Pharm. Pract. 2016, 22, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Dürr, P.; Schlichtig, K.; Kelz, C.; Deutsch, B.; Maas, R.; Eckart, M.J.; Wilke, J.; Wagner, H.; Wolff, K.; Preuß, C.; et al. The randomized AMBORA trial: Impact of pharmacological/pharmaceutical care on medication safety and patient-reported outcomes during treatment with new oral anticancer agents. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 1983–1994. [Google Scholar] [CrossRef] [PubMed]
- Schlichtig, K.; Dürr, P.; Dörje, F.; Fromm, M.F. Medication errors during treatment with new oral anticancer agents: Consequences for clinical practice based on the AMBORA study. Clin. Pharmacol Ther. 2021, 110, 1075–1086. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation: The High5s Project—Standard Operating Protocol for Medication Reconciliation Version 3 2014.
- Pharmaceutical Care Network Europe Foundation: PCNE Statement on Medication Review, V3 2013. Available online: https://www.pcne.org/upload/files/150_20160504_PCNE_MedRevtypes.pdf (accessed on 25 January 2022).
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, J.T.; Schmader, K.E.; Samsa, G.P.; Weinberger, M.; Uttech, K.M.; Lewis, I.K.; Cohen, H.J.; Feussner, J.R. A method for assessing drug therapy appropriateness. J. Clin. Epidemiol. 1992, 45, 1045–1051. [Google Scholar] [CrossRef]
- American Geriatrics Society. American geriatrics society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Lexicomp® Drug Interactions. Available online: https://online.lexi.com (accessed on 25 January 2022).
- Preston CL: Stockley’s Interactions Checker. London: Pharmaceutical Press. Available online: http://www.medicinescomplete.com/ (accessed on 25 January 2022).
- Memorial Sloan Kettering Cancer Center: Search about Herbs. Available online: https://www.mskcc.org/cancer-care/diagnosis-treatment/symptom-management/integrative-medicine/herbs/search (accessed on 15 December 2021).
- Pharmaceutical Care Network Europe Foundation. Classification for Drug Related Problems, V8.02 2003–2017. Available online: https://www.pcne.org/upload/files/230_PCNE_classification_V8-02.pdf (accessed on 25 January 2022).
- UpToDate®: Drug Informations. Available online: https://www.uptodate.com/login (accessed on 25 January 2022).
- CredibleMeds® QT Drugs Lists. Available online: https://www.crediblemeds.org (accessed on 25 January 2022).
- Ribed, A.; Romero-Jimenez, R.M.; Escudero-Vilaplana, V.; Iglesias-Peinado, I.; Herranz-Alonso, A.; Codina, C.; Sanjurjo-Saez, M. Pharmaceutical care program for onco-hematologic outpatients: Safety, efficiency and patient satisfaction. Int. J. Clin. Pharm. 2016, 38, 280–288. [Google Scholar] [CrossRef]
- Benoist, G.E.; van Oort, I.M.; Smeenk, S.; Javad, A.; Somford, D.M.; Burger, D.M.; Mehra, N.; van Erp, N.P. Drug-drug interaction potential in men treated with enzalutamide: Mind the gap. Br. J. Clin. Pharmacol. 2018, 84, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Jamani, R.; Lee, E.K.; Berry, S.R.; Saluja, R.; DeAngelis, C.; Giotis, A.; Emmenegger, U. High prevalence of potential drug-drug interactions in patients with castration-resistant prostate cancer treated with abiraterone acetate. Eur. J. Clin. Pharmacol. 2016, 72, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Kruse, V.; Somers, A.; Van Bortel, L.; De Both, A.; Van Belle, S.; Rottey, S. Sunitinib for metastatic renal cell cancer patients: Observational study highlighting the risk of important drug-drug interactions. J. Clin. Pharm. Ther. 2014, 39, 259–265. [Google Scholar] [CrossRef]
- Duran, I.; Carles, J.; Bulat, I.; Hellemans, P.; Mitselos, A.; Ward, P.; Jiao, J.; Armas, D.; Chien, C. Pharmacokinetic drug-drug interaction of apalutamide, part 1: Clinical studies in healthy men and patients with castration-resistant prostate cancer. Clin. Pharm. 2020, 59, 1135–1148. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, C.; Boudou-Rouquette, P.; Azoulay-Rutman, E.; Huillard, O.; Golmard, J.L.; Carton, E.; Noé, G.; Vidal, M.; Orvoen, G.; Chah Wakilian, A.; et al. Potential drug-drug interactions with abiraterone in metastatic castration-resistant prostate cancer patients: A prevalence study in France. Cancer Chemother Pharm. 2017, 79, 1051–1055. [Google Scholar] [CrossRef] [PubMed]
- Mir, O.; Touati, N.; Lia, M.; Litière, S.; Le Cesne, A.; Sleijfer, S.; Blay, J.Y.; Leahy, M.; Young, R.; Mathijssen, R.H.J.; et al. Impact of concomitant administration of gastric acid-suppressive agents and pazopanib on outcomes in soft-tissue sarcoma patients treated within the EORTC 62043/62072 trials. Clin. Cancer Res. 2019, 25, 1479–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, J.; Brar, S.S.; Lesko, L.J. To take or not to take with meals? Unraveling issues related to food effects labeling for oral antineoplastic drugs. Clin. Pharmacol. Drug Dev. 2018, 7, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Spratlin, J.; Kollmannsberger, C.; North, S.; Pankras, C.; Gonzalez, M.; Bernard, A.; Stieltjes, H.; Peng, L.; Jiao, J.; et al. Food effects on abiraterone pharmacokinetics in healthy subjects and patients with metastatic castration-resistant prostate cancer. J. Clin. Pharmacol. 2015, 55, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Fogli, S.; Porta, C.; Del Re, M.; Crucitta, S.; Gianfilippo, G.; Danesi, R.; Rini, B.I.; Schmidinger, M. Optimizing treatment of renal cell carcinoma with VEGFR-TKIs: A comparison of clinical pharmacology and drug-drug interactions of anti-angiogenic drugs. Cancer Treat. Rev. 2020, 84, 101966. [Google Scholar] [CrossRef] [PubMed]
- Gagliano-Jucá, T.; Travison, T.G.; Kantoff, P.W.; Nguyen, P.L.; Taplin, M.E.; Kibel, A.S.; Huang, G.; Bearup, R.; Schram, H.; Manley, R.; et al. Androgen deprivation therapy is associated with prolongation of QTc interval in men with prostate cancer. J. Endocr. Soc. 2018, 2, 485–496. [Google Scholar] [CrossRef] [Green Version]
- Villanueva-Bueno, C.; Escudero-Vilaplana, V.; Collado-Borrell, R.; Giménez-Manzorro, Á.; Ribed, A.; Marzal-Alfaro, B.; Revuelta-Herrero, J.L.; Gonzalez-Haba, E.; Herranz, A.; Sanjurjo, M. Medication guide for the perioperative management of oral antineoplastic agents in cancer patients. Expert Opin. Drug Saf. 2022, 21, 107–119. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. (%) Total (N = 38) |
|---|---|
| Age, years (mean, range) | 69.9 (47–85) |
| Male sex | 36 (94.7) |
| Female sex | 2 (5.3) |
| ECOG status | |
| 0 | 10 (26.3) |
| 1 | 19 (50.0) |
| >1 | 9 (23.7) |
| Cancer type and oral anticancer therapy | |
| Prostate cancer | 20 (52.6) |
| Abiraterone | 13 (34.2) |
| Enzalutamide | 4 (10.5) |
| Olaparib | 3 (7.9) |
| Renal cell carcinoma | 18 (47.4) |
| Cabozantinib | 10 (26.3) |
| Pazopanib | 5 (13.2) |
| Sunitinib | 2 (5.3) |
| Axitinib | 1 (2.6) |
| Anticancer regimen | |
| Monotherapy * (oral) | 37 (97.4) |
| Combination (oral + parenteral) | 1 (2.6) |
| In-label | 35 (92.1) |
| Off-label | 3 (7.9) |
| Number of all drugs# (median, range) | |
| Oral anticancer therapy | 1 (1–1) |
| Concomitant medication | 9 (1–20) |
| Complete medication | 10 (2–21) |
| Use of OTC drugs and habits | |
| Yes | 13 (34.2) |
| No | 25 (65.8) |
| Consumption of grapefruit (-products) | 6 (15.8) |
| Comorbidities (Top 5) | |
| Hypertension | 28 (73.7) |
| Diabetes mellitus | 10 (26.3) |
| Chronic renal failure | 5 (13.2) |
| Dyslipidemia | 5 (13.2) |
| Coronary heart disease | 4 (10.5) |
| Glaucoma | 4 (10.5) |
| Hypothyroidism | 4 (10.5) |
| Atrial fibrillation | 3 (7.9) |
| Cause of Medication Errors | No. (%) | ||||
|---|---|---|---|---|---|
| Complete Medication | Oral Antitumor Therapy | Co- Medication | |||
| Prescribing | Drug selection | Inappropriate drug according to guidelines/formulary | 4 (6.0) | - | 4 (6.0) |
| Inappropriate drug (within guidelines, otherwise contraindicated) | 2 (3.0) | - | 2 (3.0) | ||
| No indication for drug | 2 (3.0) | - | 2 (3.0) | ||
| Inappropriate combination | 11 (16.4) | 7 (10.4) | 4 (6.0) | ||
| Inappropriate duplication | - | - | - | ||
| No drug treatment in spite of existing indication | 4 (6.0) | - | 4 (6.0) | ||
| Too many drugs prescribed for indication | - | - | - | ||
| Drug form | Inappropriate drug form | 4 (6.0) | 1 (1.5) | 3 (4.5) | |
| Dose selection | Drug dose too low | - | - | - | |
| Drug dose too high | 3 (4.5) | - | 3 (4.5) | ||
| Dosage regimen not frequent enough | 2 (3.0) | - | 2 (3.0) | ||
| Dosage regimen too frequent | 4 (6.0) | 1 (1.5) | 3 (4.5) | ||
| Dose timing instructions wrong, unclear or missing | 7 (10.4) | 4 (6.0) + | 3 (4.5) | ||
| Treatment duration | Duration of treatment too short | - | - | - | |
| Duration of treatment too long | 1 (1.5) | 1 (1.5) | - | ||
| Total | 44 (65.7) | 14 (20.9) | 30 (44.8) | ||
| Dispensing | Dispensing | Prescribed drug not available | 1 (1.5) | 1 (1.5) | - |
| Necessary information not provided | - | - | - | ||
| Wrong drug, strength or dosage advised (OTC) | - | - | - | ||
| Wrong drug or strength dispensed | - | - | - | ||
| Total | 1 (1.5) | 1 (1.5) | - | ||
| Use | Drug use process | Not applicable in this trial a | - | - | - |
| Patient related | Patient uses/takes less drug than prescribed or does not take the drug at all | 5 (7.5) | - | 5 (7.5) | |
| Patient uses/takes more drug than prescribed | 1 (1.5) | - | 1 (1.5) | ||
| Patient abuses drug | - | - | - | ||
| Patient uses unnecessary drug | 5 (7.5) | - | 5 (7.5) | ||
| Patient takes food that interacts b | 2 (3.0) | 1 (1.5) | 1 (1.5) | ||
| Patient stores drug inappropriately | - | - | - | ||
| Inappropriate timing or dosing intervals | 3 (4.5) | - | 3 (4.5) | ||
| Patient uses the drug in a wrong way | 2 (3.0) | 2 (3.0) * | - | ||
| Patient unable to use drug/form as directed | - | - | - | ||
| Other | No or inappropriate outcome monitoring (incl. TDM) | 1 (1.5) | 1 (1.5) | - | |
| Other cause | 3 (4.5) | 2 (3.0) # | 1 (1.5) | ||
| No obvious cause | - | - | - | ||
| Total | 22 (32.8) | 6 (9.0) | 16 (23.9) | ||
| Total | 67 (100) | 21 (31.3) | 46 (68.7) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlichtig, K.; Cuba, L.; Dürr, P.; Bellut, L.; Meidenbauer, N.; Kunath, F.; Goebell, P.J.; Mackensen, A.; Dörje, F.; Fromm, M.F.; et al. New Oral Antitumor Drugs and Medication Safety in Uro-Oncology: Implications for Clinical Practice Based on a Subgroup Analysis of the AMBORA Trial. J. Clin. Med. 2022, 11, 4558. https://doi.org/10.3390/jcm11154558
Schlichtig K, Cuba L, Dürr P, Bellut L, Meidenbauer N, Kunath F, Goebell PJ, Mackensen A, Dörje F, Fromm MF, et al. New Oral Antitumor Drugs and Medication Safety in Uro-Oncology: Implications for Clinical Practice Based on a Subgroup Analysis of the AMBORA Trial. Journal of Clinical Medicine. 2022; 11(15):4558. https://doi.org/10.3390/jcm11154558
Chicago/Turabian StyleSchlichtig, Katja, Lisa Cuba, Pauline Dürr, Laura Bellut, Norbert Meidenbauer, Frank Kunath, Peter J. Goebell, Andreas Mackensen, Frank Dörje, Martin F. Fromm, and et al. 2022. "New Oral Antitumor Drugs and Medication Safety in Uro-Oncology: Implications for Clinical Practice Based on a Subgroup Analysis of the AMBORA Trial" Journal of Clinical Medicine 11, no. 15: 4558. https://doi.org/10.3390/jcm11154558
APA StyleSchlichtig, K., Cuba, L., Dürr, P., Bellut, L., Meidenbauer, N., Kunath, F., Goebell, P. J., Mackensen, A., Dörje, F., Fromm, M. F., & Wullich, B. (2022). New Oral Antitumor Drugs and Medication Safety in Uro-Oncology: Implications for Clinical Practice Based on a Subgroup Analysis of the AMBORA Trial. Journal of Clinical Medicine, 11(15), 4558. https://doi.org/10.3390/jcm11154558