
Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview


Abstract
:1. Introduction
2. Methods
3. Results—Overview of Bleeding Patterns of Most Recently Marketed Cyclic OCs

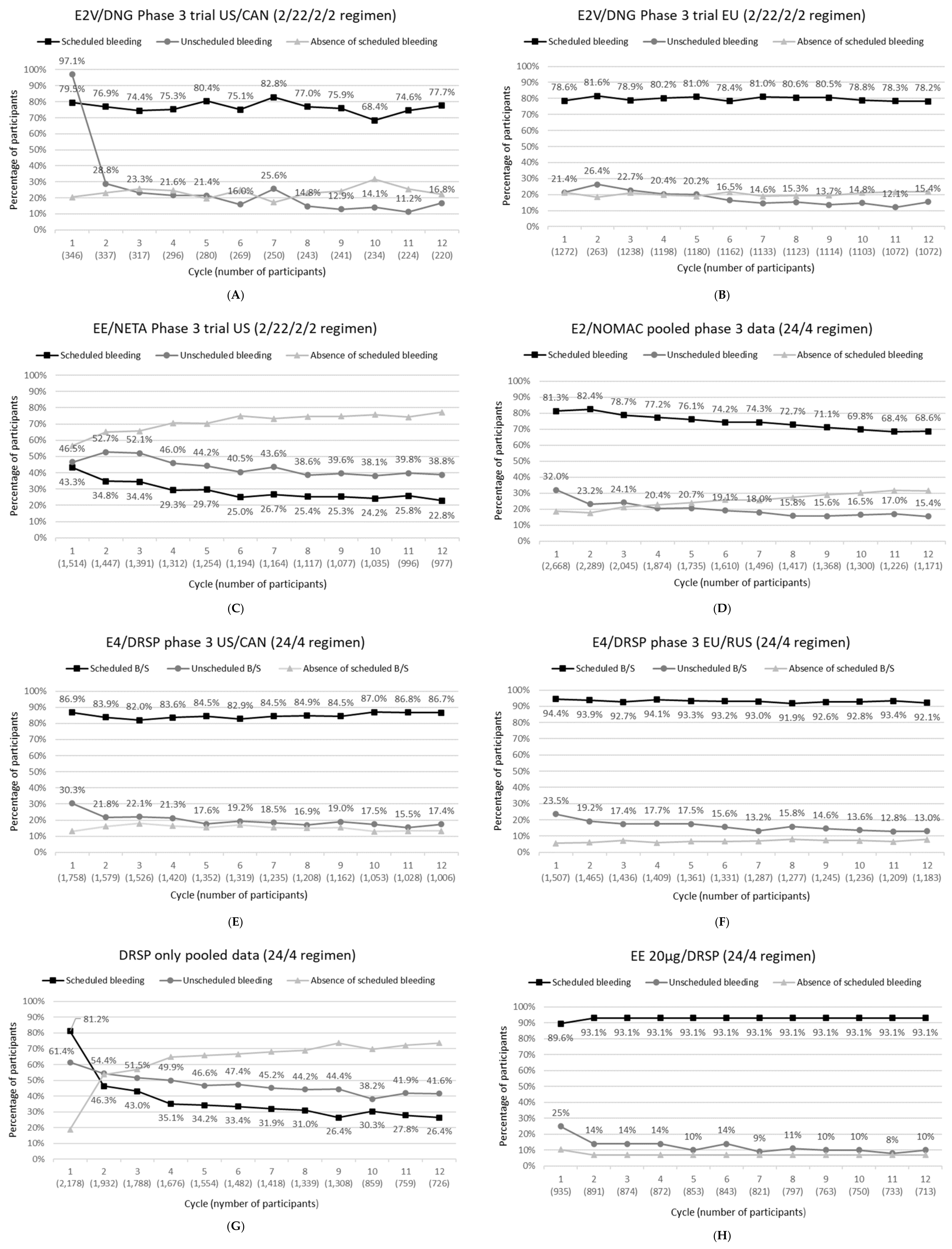
3.1. E2V/DNG
3.2. EE/NETA
3.3. E2/NOMAC
3.4. E4/DRSP
3.5. DRSP-Only
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schrager, S. Abnormal uterine bleeding associated with hormonal contraception. Am. Fam. Physician 2002, 65, 2073–2080. [Google Scholar]
- Villavicencio, J.; Allen, R.H. Unscheduled bleeding and contraceptive choice: Increasing satisfaction and continuation rates. Open Access J. Contracept. 2016, 7, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M.J.; Waugh, M.S. Oral contraceptive discontinuation: A prospective evaluation of frequency and reasons. Am. J. Obstet. Gynecol. 1998, 179, 577–582. [Google Scholar] [CrossRef]
- Rosenberg, M.J.; Long, S.C. Oral contraceptives and cycle control: A critical review of the literature. Adv. Contracept. 1992, 8 (Suppl. S1), 35–45. [Google Scholar] [CrossRef]
- Rosenberg, M.J.; Waugh, M.S.; Stevens, C.M. Smoking and cycle control among oral contraceptive users. Am. J. Obstet. Gynecol. 1996, 174, 628–632. [Google Scholar] [CrossRef]
- Seif, M.W.; Diamond, K.; Nickkho-Amiry, M. Obesity and menstrual disorders. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 516–527. [Google Scholar] [CrossRef]
- Dinger, J.; Do Minh, T.; Heinemann, K. Impact of estrogen type on cardiovascular safety of combined oral contraceptives. Contraception 2016, 94, 328–339. [Google Scholar] [CrossRef]
- Reed, S.; Koro, C.; DiBello, J.; Becker, K.; Bauerfeind, A.; Franke, C.; Heinemann, K. Prospective controlled cohort study on the safety of a monophasic oral contraceptive containing nomegestrol acetate (2.5 mg) and 17beta-oestradiol (1.5 mg) (PRO-E2 study): Risk of venous and arterial thromboembolism. Eur. J. Contracept. Reprod. Health Care 2021, 26, 439–446. [Google Scholar] [CrossRef]
- Douxfils, J.; Klipping, C.; Duijkers, I.; Kinet, V.; Mawet, M.; Maillard, C.; Jost, M.; Rosing, J.; Foidart, J.M. Evaluation of the effect of a new oral contraceptive containing estetrol and drospirenone on hemostasis parameters. Contraception 2020, 102, 396–402. [Google Scholar] [CrossRef]
- Bachmann, G.; Korner, P. Bleeding patterns associated with oral contraceptive use: A review of the literature. Contraception 2007, 76, 182–189. [Google Scholar] [CrossRef]
- Belsey, E.M.; Machin, D.; d’Arcangues, C. The analysis of vaginal bleeding patterns induced by fertility regulating methods. World Health Organization Special Programme of Research, Development and Research Training in Human Reproduction. Contraception 1986, 34, 253–260. [Google Scholar] [CrossRef]
- Mishell, D.R., Jr.; Guillebaud, J.; Westhoff, C.; Nelson, A.L.; Kaunitz, A.M.; Trussell, J.; Davis, A.J. Combined hormonal contraceptive trials: Variable data collection and bleeding assessment methodologies influence study outcomes and physician perception. Contraception 2007, 75, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Mishell, D.R., Jr.; Guillebaud, J.; Westhoff, C.; Nelson, A.L.; Kaunitz, A.M.; Trussell, J.; Davis, A.J. Recommendations for standardization of data collection and analysis of bleeding in combined hormone contraceptive trials. Contraception 2007, 75, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Hodkinson, A.; Dietz, K.C.; Lefebvre, C.; Golder, S.; Jones, M.; Doshi, P.; Heneghan, C.; Jefferson, T.; Boutron, I.; Stewart, L. The use of clinical study reports to enhance the quality of systematic reviews: A survey of systematic review authors. Syst. Rev. 2018, 7, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinicaltrials.gov. Available online: https://www.clinicaltrials.gov (accessed on 21 January 2022).
- Nelson, A.; Parke, S.; Mellinger, U.; Zampaglione, E.; Schmidt, A. Efficacy and safety of a combined oral contraceptive containing estradiol valerate/dienogest: Results from a clinical study conducted in North America. J. Womens Health 2014, 23, 204–210. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research; Food and Drug Administration. Clinical Review Estradiol Valerate/Dienogest (NDA 22-252). 28 April 2010. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/022252_Orig-1_MedR.pdf (accessed on 25 May 2022).
- Palacios, S.; Wildt, L.; Parke, S.; Machlitt, A.; Romer, T.; Bitzer, J. Efficacy and safety of a novel oral contraceptive based on oestradiol (oestradiol valerate/dienogest): A Phase III trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 149, 57–62. [Google Scholar] [CrossRef]
- Apter, D.; Zimmerman, Y.; Beekman, L.; Mawet, M.; Maillard, C.; Foidart, J.M.; Bennink, H.J. Bleeding pattern and cycle control with estetrol-containing combined oral contraceptives: Results from a phase II, randomised, dose-finding study (FIESTA). Contraception 2016, 94, 366–373. [Google Scholar] [CrossRef] [Green Version]
- Archer, D.F.; Nakajima, S.T.; Sawyer, A.T.; Wentworth, J.; Trupin, S.; Koltun, W.D.; Gilbert, R.D.; Ellman, H. Norethindrone acetate 1.0 milligram and ethinyl estradiol 10 micrograms as an ultra low-dose oral contraceptive. Obstet. Gynecol. 2013, 122, 601–607. [Google Scholar] [CrossRef]
- FDA. Medical Review Lo Loestrin (NDA 22-501). 4 October 2010. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/022501Orig1s000MedR.pdf (accessed on 25 May 2022).
- Mansour, D.; Verhoeven, C.; Sommer, W.; Weisberg, E.; Taneepanichskul, S.; Melis, G.B.; Sundstrom-Poromaa, I.; Korver, T. Efficacy and tolerability of a monophasic combined oral contraceptive containing nomegestrol acetate and 17beta-oestradiol in a 24/4 regimen, in comparison to an oral contraceptive containing ethinylestradiol and drospirenone in a 21/7 regimen. Eur. J. Contracept. Reprod. Health Care 2011, 16, 430–443. [Google Scholar] [CrossRef] [Green Version]
- Australian Government, Department of Health and Ageing Therapeutic Goods Administration. Australian Public Assessment Report for Nomegestrol Acetate/Oestradiol. October 2011. Available online: https://www.tga.gov.au/sites/default/files/auspar-zoely.pdf (accessed on 25 May 2022).
- Westhoff, C.; Kaunitz, A.M.; Korver, T.; Sommer, W.; Bahamondes, L.; Darney, P.; Verhoeven, C. Efficacy, safety, and tolerability of a monophasic oral contraceptive containing nomegestrol acetate and 17beta-estradiol: A randomized controlled trial. Obstet. Gynecol. 2012, 119, 989–999. [Google Scholar] [CrossRef]
- Mansour, D.; Westhoff, C.; Kher, U.; Korver, T. Pooled analysis of two randomized, open-label studies comparing the effects of nomegestrol acetate/17beta-estradiol and drospirenone/ethinyl estradiol on bleeding patterns in healthy women. Contraception 2017, 95, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Gemzell-Danielsson, K.; Apter, D.; Zatik, J.; Weyers, S.; Piltonen, T.; Suturina, L.; Apolikhina, I.; Jost, M.; Creinin, M.D.; Foidart, J.M. Estetrol-Drospirenone combination oral contraceptive: A clinical study of contraceptive efficacy, bleeding pattern and safety in Europe and Russia. BJOG 2022, 129, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research; Food and Drug Administration. Multi-Discipline Review of Nextstellis (NDA 214154). 15 April 2021. Available online: https://www.fda.gov/media/149979/download (accessed on 25 May 2022).
- Creinin, M.D.; Westhoff, C.L.; Bouchard, C.; Chen, M.J.; Jensen, J.T.; Kaunitz, A.M.; Achilles, S.L.; Foidart, J.M.; Archer, D.F. Estetrol-drospirenone combination oral contraceptive: North American phase 3 efficacy and safety results. Contraception 2021, 104, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Archer, D.F.; Ahrendt, H.J.; Drouin, D. Drospirenone-only oral contraceptive: Results from a multicenter noncomparative trial of efficacy, safety and tolerability. Contraception 2015, 92, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research; Food and Drug Administration. Multi-Disciplinary Review and Evaluation Slynd (NDA 211367). 24 May 2019. Available online: https://www.fda.gov/media/129539/download (accessed on 25 May 2022).
- Palacios, S.; Colli, E.; Regidor, P.A. Bleeding profile of women using a drospirenone-only pill 4 mg over nine cycles in comparison with desogestrel 0.075 mg. PLoS ONE 2020, 15, e0231856. [Google Scholar] [CrossRef]
- Kimble, T.; Burke, A.E.; Barnhart, K.T.; Archer, D.F.; Colli, E.; Westhoff, C.L. A 1-year prospective, open-label, single-arm, multicenter, phase 3 trial of the contraceptive efficacy and safety of the oral progestin-only pill drospirenone 4 mg using a 24/4-day regimen. Contracept. X 2020, 2, 100020. [Google Scholar] [CrossRef]
- Australian Government, Department of Health and Ageing Therapeutic Goods Administration. Australian Public Assessment Report for Nomegestrol Acetate/Oestradiol (Zoely). October 2011. Available online: https://www.tga.gov.au/sites/default/files/auspar-zoely.pdf (accessed on 25 May 2022).
- Center for Drug Evaluation and Research; Food and Drug Administration. Medical Review Yaz (NDA 21-676). 16 May 2006. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2006/021676s000_MEDR_pt1.pdf (accessed on 25 May 2022).
- Bachmann, G.; Sulak, P.J.; Sampson-Landers, C.; Benda, N.; Marr, J. Efficacy and safety of a low-dose 24-day combined oral contraceptive containing 20 micrograms ethinylestradiol and 3 mg drospirenone. Contraception 2004, 70, 191–198. [Google Scholar] [CrossRef]
- Ahrendt, H.J.; Makalova, D.; Parke, S.; Mellinger, U.; Mansour, D. Bleeding pattern and cycle control with an estradiol-based oral contraceptive: A seven-cycle, randomized comparative trial of estradiol valerate/dienogest and ethinyl estradiol/levonorgestrel. Contraception 2009, 80, 436–444. [Google Scholar] [CrossRef]
- Hagen, A.A.; Barr, M.; Diczfalusy, E. Metabolism of 17-Beta-Oestradiol-4-14-C in Early Infancy. Acta Endocrinol. 1965, 49, 207–220. [Google Scholar] [CrossRef]
- Warmerdam, E.G.; Visser, M.; Coelingh Bennink, H.J.; Groen, M. A new route of synthesis of estetrol. Climacteric 2008, 11 (Suppl. S1), 59–63. [Google Scholar] [CrossRef]
- Gérard, C.; Arnal, J.F.; Jost, M.; Douxfils, J.; Lenfant, F.; Fontaine, C.; Houtman, R.; Archer, D.F.; Reid, R.L.; Lobo, R.A.; et al. Profile of estetrol, a promising native estrogen for oral contraception and the relief of climacteric symptoms of menopause. Expert. Rev. Clin. Pharmacol. 2022, 15, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Fruzzetti, F.; Fidecicchi, T.; Montt Guevara, M.M.; Simoncini, T. Estetrol: A New Choice for Contraception. J. Clin. Med. 2021, 10, 5625. [Google Scholar] [CrossRef]
- Creinin, M.D.; Vieira, C.S.; Westhoff, C.L.; Mansour, D.J.A. Recommendations for standardization of bleeding data analyses in contraceptive studies. Contraception 2022, 112, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Gallo, M.F.; Nanda, K.; Grimes, D.A.; Lopez, L.M.; Schulz, K.F. 20 microg versus >20 microg estrogen combined oral contraceptives for contraception. Cochrane Database Syst. Rev. 2013, 8, CD003989. [Google Scholar] [CrossRef] [Green Version]
- Blode, H.; Kowal, K.; Roth, K.; Reif, S. Pharmacokinetics of drospirenone and ethinylestradiol in Caucasian and Japanese women. Eur. J. Contracept. Reprod. Health Care 2012, 17, 284–297. [Google Scholar] [CrossRef]
- Gerrits, M.G.; Schnabel, P.G.; Post, T.M.; Peeters, P.A. Pharmacokinetic profile of nomegestrol acetate and 17beta-estradiol after multiple and single dosing in healthy women. Contraception 2013, 87, 193–200. [Google Scholar] [CrossRef]
- Polis, C.B.; Hussain, R.; Berry, A. There might be blood: A scoping review on women’s responses to contraceptive-induced menstrual bleeding changes. Reprod. Health 2018, 15, 114. [Google Scholar] [CrossRef] [Green Version]
- Wiegratz, I.; Hommel, H.H.; Zimmermann, T.; Kuhl, H. Attitude of German women and gynecologists towards long-cycle treatment with oral contraceptives. Contraception 2004, 69, 37–42. [Google Scholar] [CrossRef]

{kind=link}
| Bleeding | Evidence of blood loss that requires the use of sanitary protection with a tampon, pad, or pantyliner. |
| Spotting | Evidence of minimal blood loss that does not require new use of any type of sanitary protection, including pantyliners. |
| Episode of bleeding | Bleeding and/or spotting days bounded on either end by 2 days of no bleeding or spotting. |
| Scheduled bleeding and withdrawal bleeding * | Any bleeding or spotting that occurs during hormone-free intervals regardless of the duration of the regimen and may continue into the first 4 days (Days 1–4) of the subsequent cycle of combined hormonal contraceptive (CHC) therapy. |
| Unscheduled bleeding # | Any bleeding that occurs while taking active hormones, regardless of the duration of regimen. Two exceptions:
|
| Unscheduled spotting # | Any spotting that occurs while taking active hormones, regardless of the duration of regimen. Two exceptions:
|
| Amenorrhea | Use of the term amenorrhea should be abandoned in the context of CHC therapy and replaced with absence of all bleeding and spotting. |
| Product/Brand Name | Treatment Regimen | Trial Identifier | Trial/ Countries | Trial Start- Completion | No. Subjects/ Age (Years)/ BMI (kg/m2) * | Data Sources | Discontinuation Rate (%) Overall/Due to AEs/ Due to Bleeding Related AEs |
|---|---|---|---|---|---|---|---|
| E2V/DNG Qlaira ®/Natazia® | 2/22/2/2 | NCT00206583 | Phase 3 US/CAN | March 2005–July 2007 | 490/18–35/≤30 | Nelson 2014 [16] FDA assessment report [17] | 35.1/13.9/5.1 |
| NCT00185289 | Phase 3 EU | April 2004–July 2006 | 1377/18–50/≤30 | Palacios 2010 [18] FDA assessment report [17] | 21.4/10.2/2.5 | ||
| NCT01221831 | Phase 2 Finland (6 cycles) | September 2010–September 2011 | 78/18–35/18–30 | Apter 2016 [19] | 10.3/NR/NR | ||
| EE/NETA 10 µg Lo Loestrin ® | 24/2/2 | NCT00391807 | Phase 3 US | November 2006–September 2008 | 1660/18–45/≤35 | Archer 2013 [20] FDA assessment report [21] | 41.7/10.7/3.8 |
| E2/NOMAC Zoely® | 24/4 | NCT00511199 | Phase 3 EU/Asia/AUS | May 2006–April 2008 | 1591/18–50/17–35 | Mansour 2011 [22] AUSPAR [23] | 28.2/18.2/4.0 |
| NCT00413062 | Phase 3 US/LA/CAN | June 2006–July 2008 | 1666/18–50/17–35 | Westhoff 2012 [24] AUSPAR [23] | 40.7/17.3/3.8 | ||
| NCT00511199 NCT00413062 | Pooled analysis | - | 3233/18–50/17–35 | Mansour 2017 [25] | 34.7/17.9/3.9 | ||
| E4/DRSP Nextstellis®/ Drovelis®/ Lydisilka® | 24/4 | NCT02817828 | Phase 3 EU/RUS | June 2016–April 2018 | 1553/18–50/≤35 | Gemzell Danielsson 2022 [26] FDA assessment report [27] | 21.6//10.1/3.4 |
| NCT02817841 | Phase 3 US/CAN | August 2016–November 2018 | 1864/16–50/≤35 | Creinin 2021 [28] FDA assessment report [27] | 45.5/9.7/2.7 | ||
| NCT01221831 | Phase 2 Finland (6 cycles) | September 2010–September 2011 | 79/18–35/18–30 | Apter 2016 [19] | 8.9/NR/NR | ||
| DRSP-only Slynd®/Slinda® | 24/4 | 2010-021787-15 | Phase 3 Europe | July 2011–March 2013 | 713/18–45/- | Archer 2015 [29] FDA assessment report [30] | 27.8/12.3/4.2 |
| 2011-002396-42 | Phase 3 Europe (9 cycles) | August 2012–January 2014 | 858/18–45/- | Palacios 2020 [31] FDA assessment report [30] | 19.8/9.6/3.3 | ||
| NCT02269241 | Phase 3 US | October 2014–October 2017 | 1006/≥15/- | FDA assessment report [30] Kimble 2020 [32] | 65.0/11.2/NR | ||
| EudraCT 2010-021787-15 EudraCT 2011-002396-42 NCT02269241 EudraCT 2013-002300-13 | Pooled analysis | - | 2598/≥15/- | FDA assessment report [30] | 39.5/10.9/NR | ||
| EE 30 µg/DRSP Yasmin® | 21/7 | NCT00511199 | Phase 3 EU/Asia/AUS | May 2006–April 2008 | 535/18–50/17–35 | Mansour 2011 [22] AUSPAR [33] | 23.4/10.5/0.7 |
| NCT00413062 | Phase 3 US/LA/CAN | June 2006–July 2008 | 554/18–50/17–35 | Westhoff 2012 [24] AUSPAR [33] | 37.9/10.1/1.8 | ||
| NCT00511199 NCT00413062 | Pooled analysis | - | 1084/18–50/17–35 | Mansour 2017 [25] | 30.9/10.3/1.3 | ||
| EE 20 µg/DRSP Yaz® | 24/4 | Protocol 303740 | Phase 3 US/EU/LA | 1027/17–36/≤35 | FDA assessment report [34] Bachman 2004 [35] | 28.9/7.5/NR |
| Product/Brand Name | Trial Identifier(s) | Data Collection | Definition of Spotting | Definition of Bleeding | Definition of Scheduled Bleeding |
|---|---|---|---|---|---|
| E2V/DNG Qlaira®/Natazia® | NCT00206583 NCT00185289 | Paper diary | Vaginal blood in an amount that did not require the use of sanitary protection other than panty liner(s) | Vaginal bleeding the subject categorized as light, normal, or heavy, that, based on her personal experience, required the use of sanitary protection | Start at day 21 and continued without interruption. If no bleeding occurred until Cycle Day 20 of the next cycle, it was assessed as absence of scheduled bleeding in the previous treatment cycle. |
| EE/NETA 10 µg Lo Loestrin® | NCT00391807 | Light bleeding not requiring sanitary protection (other than panty liners) was classified as spotting | Only spotting defined. All vaginal bleeding was recorded, including use of sanitary protection (other than panty liners) | First bleeding episode starting 4 days before the last day of active drug intake during a treatment cycle and 3 days after beginning treatment in the next treatment cycle. | |
| E2/NOMAC Zoely® | NCT00511199 NCT00413062 | Electronic diary | Vaginal bleeding requiring none or at most one pad/tampon per day | Vaginal bleeding requiring more than one pad/tampon per day | Within expected bleeding period (Day 25-Day 3 next cycle) including early and continued bleeding *. |
| E4/DRSP Nextstellis®/ Drovelis®/ Lydisilka® | NCT02817828 NCT02817841 | Paper diary | Minimal vaginal blood loss that did not require the new use of sanitary protection, including panty liners | Vaginal blood loss that required the use of sanitary protection with a tampon, pad or panty liner | Within expected bleeding period (Day 25-Day 3 next cycle) including early and continued bleeding *. |
| DRSP only Slynd®/Slinda® | EudraCT 2010-021787-15 EudraCT 2011-002396-42 NCT02269241 | Electronic diary | Blood loss that did not require new use of any type of sanitary protection | Blood loss that required the use of sanitary protection | Any bleeding or spotting that occurred during hormone-free intervals (defined as days 25–28 ± 1). Up to eight consecutive bleeding days were considered as scheduled bleeding days. |
| EE 30 µg/DRSP Yasmin® | NCT00511199 NCT00413062 | Electronic diary | Vaginal bleeding requiring none or at most one pad/tampon per day | Vaginal bleeding requiring more than one pad/tampon per day | Within expected bleeding period (Day 21-Day 28 next cycle) including early and continued bleeding *. |
| EE 20 µg/DRSP Yaz® 24/4 regimen | Protocol 303740 | Paper diary | No requirement for sanitary protection except panty liners | Need for sanitary protection | First bleeding after hormone withdrawal (i.e., day 25). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Archer, D.F.; Mansour, D.; Foidart, J.-M. Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview. J. Clin. Med. 2022, 11, 4634. https://doi.org/10.3390/jcm11154634
Archer DF, Mansour D, Foidart J-M. Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview. Journal of Clinical Medicine. 2022; 11(15):4634. https://doi.org/10.3390/jcm11154634
Chicago/Turabian StyleArcher, David F., Diana Mansour, and Jean-Michel Foidart. 2022. "Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview" Journal of Clinical Medicine 11, no. 15: 4634. https://doi.org/10.3390/jcm11154634
APA StyleArcher, D. F., Mansour, D., & Foidart, J. -M. (2022). Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview. Journal of Clinical Medicine, 11(15), 4634. https://doi.org/10.3390/jcm11154634