
Influence of Risk Factors on Exercise Tolerance in Patients after Myocardial Infarction—Early Cardiac Rehabilitation in Poland


Abstract
:1. Introduction
- The participation of patients after myocardial infarction in the CSC-Infarct program changes the parameters of exercise tolerance by the cardiovascular system;
- The risk factors determine the obtained parameters of exercise tolerance before commencement and after the completion of the coordinated cardiac rehabilitation program.
2. Materials and Methods
2.1. Participants
2.2. Selection Criteria
2.3. Instruments
2.4. Procedure
2.5. Statistical Analysis
- ns: 0.05 < p <= 1.00;
- *: 0.01 < p <= 0.05;
- **: 0.001 < p <= 0.01;
- ***: 0.0001 < p <= 0.001;
- ****: p <= 0.0001 .
3. Results
3.1. Study Group Characteristics
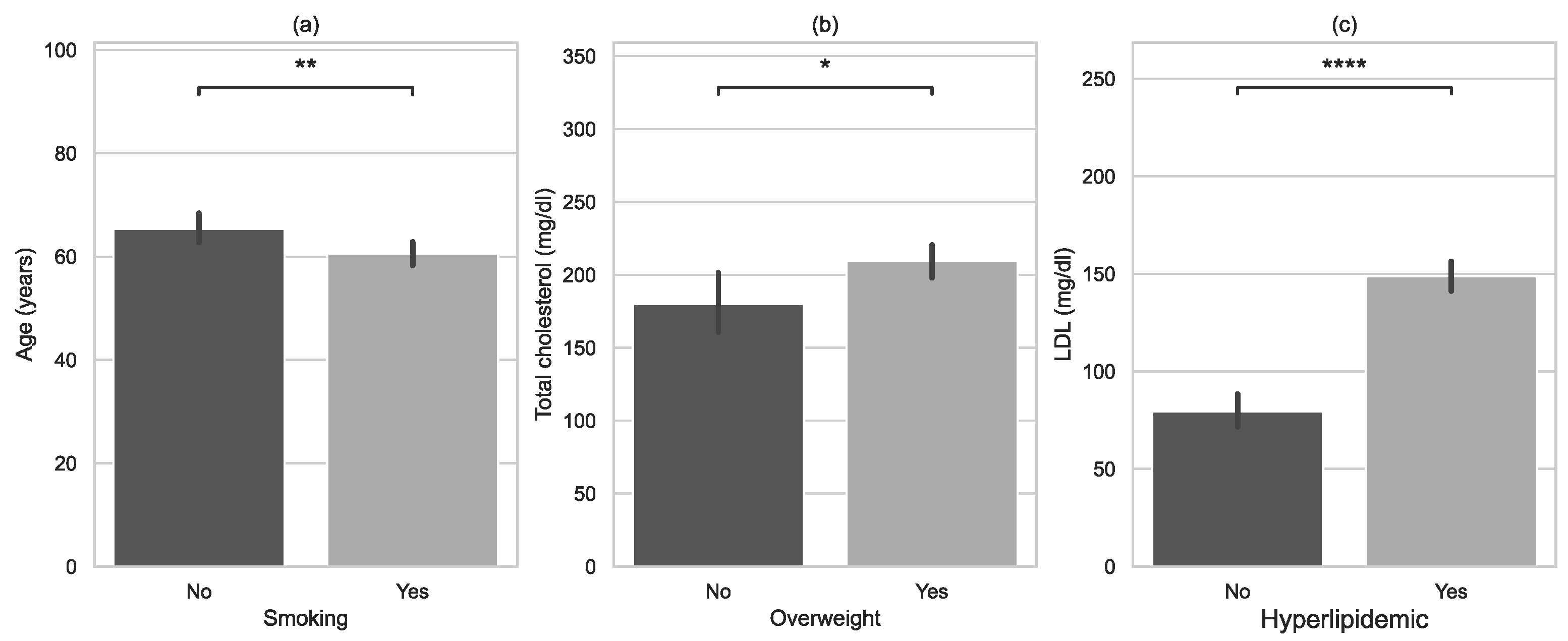
3.2. Risk Factors of Myocardiac Infarction
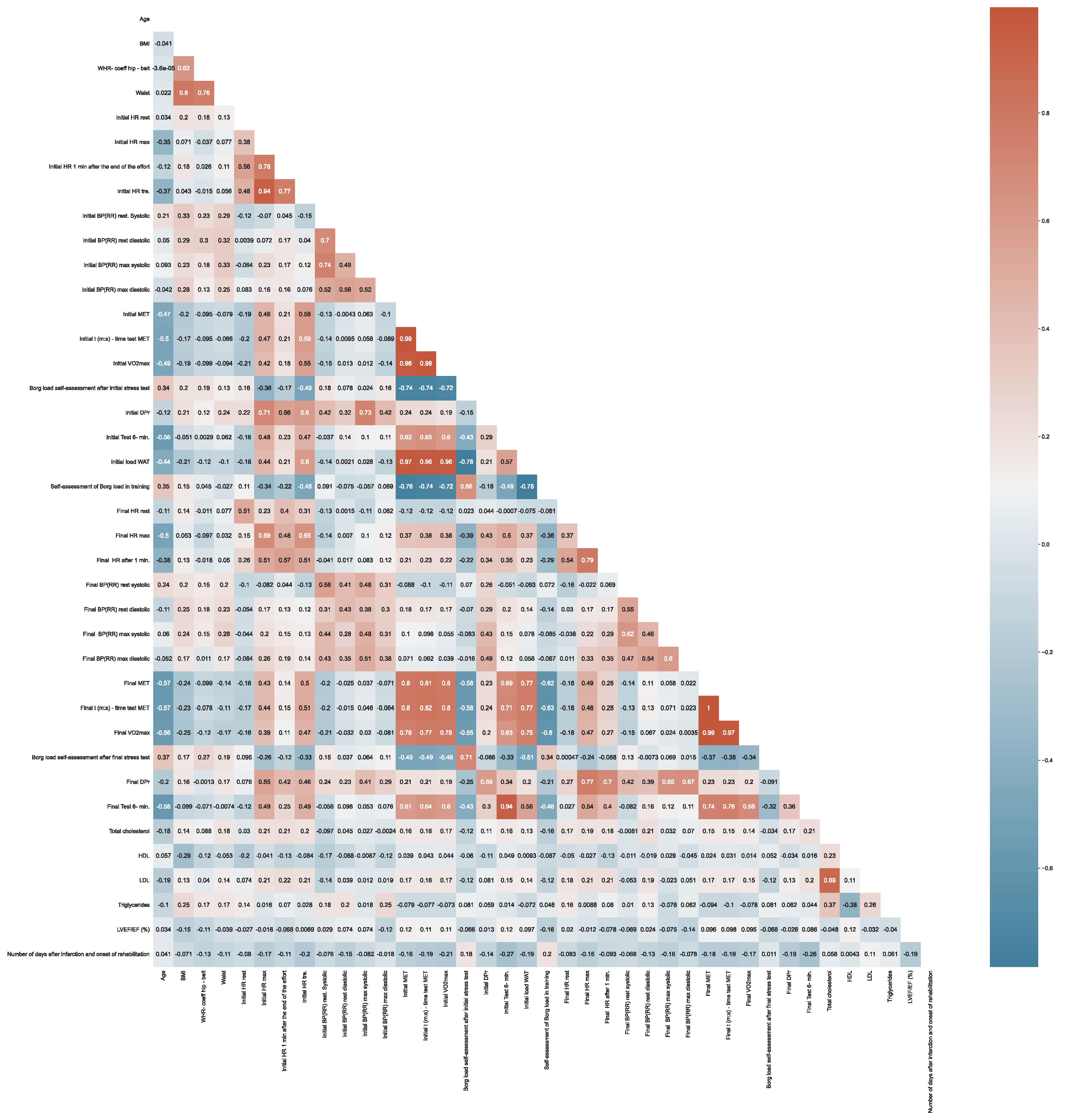
3.3. Correlation between Variables
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Heart Network; European Society of Cardiology. European Cardiovascular Disease Statistics, 2012 ed; European Heart Network: Brussels, Belgium; European Society of Cardiology: Brussels, Belgium, 2012; Available online: https://www.escardio.org/static_file/Escardio/Press-media/press-releases/2013/EU-cardiovascular-disease-statistics-2012.pdf (accessed on 15 February 2020).
- Eurostat Statistics Explained. Cardiovascular Diseases Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/pdfscache/37359.pdf (accessed on 24 September 2019).
- Mącznik-Kubicka, A. Secondary prevention of cardiac patients after myocardial infarction. Chor. Serca Naczyń 2016, 13, 363–366. [Google Scholar]
- Strzelecki, Z.; Szymborski, J. Incidence and Mortality from Cardiovascular Diseases and the Demographic Situation of Poland; Central Statistical Office: Warsaw, Poland, 2015. [Google Scholar]
- Jankowski, P. Principles for the prevention of cardiovascular diseases in 2018. Invasive Cardiol. 2017, 12, 42–48. (In Polish) [Google Scholar]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 6, CD001800. [Google Scholar] [CrossRef]
- Zaczek, R.; Balsam, P.; Peller, M.; Gawałko, M.; Łyżwiński, Ł.; Kiliszek, M.; Baranowski, R.; Opolski, G. Influence of cardiac rehabilitation after myocardial infarction on microvolt alternation in T wave and risk factors for non-negative outcome. Invasive Cardiol. 2017, 12, 48–55. (In Polish) [Google Scholar]
- Jankowski, P.; Czarnecka, D.; Wolfshaut-Wolak, R.; Łysek, R.; Łukaszewska, A.; Bogacki, P.; Grodecki, J.; Mirek-Bryniarska, E.; Nessler, J.; Podolec, P.; et al. Secondary prevention of coronary artery disease in contemporary clinical practice. Cardiol. J. 2015, 22, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Łagoda, I.; Banasik, K.; Sobieszek, G.; Kapka-Skrzypczak, L. Place of physiotherapy in the treatment of myocardial infarction in the context of the Coordinated Specialist Care Program. Gen. Med. Health Sci. 2020, 26, 315–321. (In Polish) [Google Scholar] [CrossRef]
- Hajar, R. Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views 2017, 18, 109–114. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Sia, C.H.; Ko, J.; Zheng, H.; Ho, A.F.-W.; Foo, D.; Foo, L.-L.; Lim, P.Z.-Y.; Liew, B.W.; Chai, P.; Yeo, T.-C.; et al. Association between smoking status and outcomes in myocardial infarction patients undergoing percutaneous coronary intervention. Sci. Rep. 2021, 11, 6466. [Google Scholar] [CrossRef]
- Akil, L.; Ahmad, H.A. Relationships between obesity and cardiovascular diseases in four southern states and Colorado. J. Health Care Poor Underserved 2011, 22, 61–72. [Google Scholar] [CrossRef]
- Cercato, C.; Fonseca, F.A. Cardiovascular risk and obesity. Diabetol. Metab. Syndr. 2019, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Makaryus, A.N.; Picariello, C.; Lazzeri, C.; Attanà, P.; Chiostri, M.; Gensini, G.F.; Valente, S. The Impact of Hypertension on Patients with Acute Coronary Syndromes. Int. J. Hypertens. 2011, 2011, 563657. [Google Scholar] [CrossRef]
- Troughton, R.W.; Lainchbury, J.G.; Elliott, J.; Frampton, C.; Espiner, E.A.; Crozier, I.G.; Yandle, T.G.; Turner, J. Antecedent hypertension and heart failure after myocardial infarction. J. Am. Coll. Cardiol. 2002, 39, 1182–1188. [Google Scholar]
- Miura, K.; Daviglus, M.L.; Dyer, A.R.; Liu, K.; Garside, D.B.; Stamler, J.; Greenland, P. Relationship of Blood Pressure to 25-Year Mortality Due to Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult Men: The Chicago Heart Association Detection Project in Industry. Arch. Intern. Med. 2001, 161, 1501–1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankowski, P.; Niewada, M.; Bochenek, A.; Bochenek-Klimczyk, K.; Bogucki, M.; Drygas, W.; Dudek, D.; Eysymontt, Z.; Grajek, S.; Kozierkiewicz, A.; et al. Optymalny Model Kompleksowej Rehabilitacji i Wtórnej Prewencji [Optimal model of comprehensive rehabilitation and secondary prevention]. Pol. Cardiol. 2013, 71, 995–1003. (In Polish) [Google Scholar] [CrossRef]
- Charakida, M.; Masi, S.; Lüscher, T.F.; Kastelein, J.J.; Deanfield, J.E. Assessment of atherosclerosis: The role of flow-mediated dilatation. Eur. Heart J. 2010, 31, 2854–2861. [Google Scholar] [CrossRef]
- Balsam, P.; Szmit, S. Rehabilitacja kardiologiczna a śmiertelność wśród pacjentów po angioplastyce naczyń wieńcowych. Kardiol. Dypl. 2011, 10, 84–86. (In Polish) [Google Scholar]
- Goel, K.; Lennon, R.J.; Tilbury, R.T.; Squires, R.W.; Thomas, R.J. Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation 2011, 31, 2344–2352. [Google Scholar] [CrossRef]
- WHO. A Healthy Lifestyle—WHO Recommendations. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 9 June 2022).
- Nowak, M.; Grzywa, M. Metabolic obesity in people with normal body weight and cardiovascular diseases. Pol. Merk. Lek. 2011, 31, 118–121. (In Polish) [Google Scholar]
- Van’t Veer, M.; Pijls, N.H.J.; Hennigan, B.; Watkins, S.; Ali, Z.A.; De Bruyne, B.; Zimmermann, F.M.; van Nunen, L.X.; Barbato, E.; Berry, C.; et al. Comparison of Different Diastolic Resting Indexes to iFR: Are They All Equal? J. Am. Coll. Cardiol. 2017, 26, 3088–3096. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Statistica 13.0. Available online: www.statsoft.com (accessed on 21 October 2021).
- Glowinski, S.; Krzyzynski, T. Modelling of the ejection process in a symmetrical flight. J. Theor. Appl. Mech. 2013, 51, 775–785. [Google Scholar]
- Available online: https://www.python.org (accessed on 22 November 2021).
- Grochulska, A.; Glowinski, S.; Bryndal, A. Cardiac Rehabilitation and Physical Performance in Patients after Myocardial Infarction: Preliminary Research. J. Clin. Med. 2021, 10, 2253. [Google Scholar] [CrossRef] [PubMed]
- Bryndal, A.; Majchrzycki, M.; Grochulska, A.; Glowinski, S.; Seremak-Mrozikiewicz, A. Risk Factors Associated with Low Back Pain among A Group of 1510 Pregnant Women. J. Pers. Med. 2020, 10, 51. [Google Scholar] [CrossRef]
- Elshazly, A.; Khorshid, H.; Hanna, H.; Ali, A. Effect of exercise training on heart rate recovery in patients post anterior myocardial infarction. Egypt. Heart J. 2018, 70, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Hai, J.J.; Siu, C.W.; Ho, H.H.; Li, S.W.; Lee, S.; Tse, H.F. Relationship between changes in heart rate recovery after cardiac rehabilitation on cardiovascular mortality in patients with myocardial infarction. Heart Rhythm 2010, 7, 929–936. [Google Scholar] [PubMed]
- Bruning, R.S.; Sturek, M. Benefits of exercise training on coronary blood flow in coronary artery disease patients. Prog. Cardiovasc. Dis. 2015, 57, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Humphrey, R.; Guazzi, M.; Niebauer, J. Cardiac Rehabilitation in Europe. Prog. Cardiovasc. Dis. 2014, 56, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.L.; Holloway, T.M.; Brum, M.; Caruso, V.; Chessex, C.; Grace, S.L. Cardiac rehabilitation wait times: Effect on enrollment. J. Cardiopulm. Rehabil. Prev. 2011, 31, 373–377. [Google Scholar]
- Bierbauer, W.; Scholz, U.; Bermudez, T.; Debeer, D.; Coch, M.; Fleisch-Silvestri, R.; Nacht, C.-A.; Tschanz, H.; Schmid, J.-P.; Hermann, M. Improvements in exercise capacity of older adults during cardiac rehabilitation. Eur. J. Prev. Cardiol. 2020, 27, 1747–1755. [Google Scholar] [CrossRef]
- Rea, T.D.; Heckbert, S.R.; Kaplan, R.C.; Psaty, B.M.; Smith, N.L.; Lemaitre, R.N.; Lin, D. Body mass index and the risk of recurrent coronary events following acute myocardial infarction. Am. J. Cardiol. 2001, 88, 467–472. [Google Scholar] [CrossRef]
- Dharmapriya, M.K.J.K.B.; Silva, M.D.C.; Bandara, D.M.A.K.; Ranasinghe, M.C.R.; Weerathunge, M.P.M.; Wijesinghe, R.A.N.K. The effect of obesity on cardiac rehabilitation in patients who have undergone coronary artery bypass graft surgery at the National Hospital of Sri Lanka. Int. J. Med. Res. Health Sci. 2019, 8, 166–172. [Google Scholar]
- Jayawardena, R.; Sooriyaarachchi, P.; Punchihewa, P.; Lokunarangoda, N.; Pathirana, A.K. Effects of “plate model” as a part of dietary intervention for rehabilitation following myocardial infarction: A randomized controlled trial. Cardiovasc. Diagn. Ther. 2019, 9, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.R.; Buckley, B.S.; McLernon, D.J.; Sheikh, A.; Murphy, A.; Hannaford, P.C. Five-year prognosis in an incident cohort of people presenting with acute myocardial infarction. PLoS ONE 2011, 6, e26573. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, M.; Shabib, G.; Masoumi, G.; Amerizadeh, A.; Shahabi, J.; Heidari, R.; Roohafza, H. A Systematic Review and Meta-analysis on the Prevalence of Smoking Cessation in Cardiovascular Patients After Participating in Cardiac Rehabilitation. Curr. Probl. Cardiol. 2021, 46, 100719. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Unal, B.; Critchley, J.A.; Capewell, S. Mortality reductions in patients receiving exercise-based cardiac rehabilitation: How much can be attributed to cardiovascular risk factor improvements? Eur. J. Prev. Cardiol. 2006, 13, 369–374. [Google Scholar] [CrossRef]
- Laddu, D.R.; Ozemek, C.; Hauer, T.L.; Rouleau, C.R.; Campbell, T.S.; Wilton, S.B.; Aggarwal, S.; Austford, L.; Arena, R. Cardiometabolic responses to cardiac rehabilitation in people with and without diabetes. Int. J. Cardiol. 2020, 301, 156–162. [Google Scholar] [CrossRef]
- Bjarnason-Wehrens, B.; Nebel, R.; Jensen, K.; Hackbusch, M.; Grilli, M.; Gielen, S.; Schwaab, B.; Rauch, B. German Society of Cardiovascular Prevention and Rehabilitation (DGPR). Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: The Cardiac Rehabilitation Outcome Study in Heart Failure (CROS-HF): A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2020, 27, 929–952. [Google Scholar] [CrossRef]
- Tekkeşin, A.İ.; Hayıroğlu, M.İ.; Çinier, G.; Özdemir, Y.S.; İnan, D.; Yüksel, G.; Pay, L.; Parsova, K.E.; Vatanoğlu, E.G.; Şeker, M.; et al. Lifestyle intervention using mobile technology and smart devices in patients with high cardiovascular risk: A pragmatic randomised clinical trial. Atherosclerosis 2021, 319, 21–27. [Google Scholar] [CrossRef]
- Hayıroğlu, M.İ.; Çinier, G.; Yüksel, G.; Pay, L.; Durak, F.; Çınar, T.; İnan, D.; Parsova, K.E.; Vatanoğlu, E.G.; Şeker, M.; et al. Effect of a mobile application and smart devices on heart rate variability in diabetic patients with high cardiovascular risk: A sub-study of the LIGHT randomized clinical trial. Kardiol. Pol. 2021, 79, 1239–1244. [Google Scholar] [CrossRef]
- Hayıroğlu, M.İ.; Çınar, T.; Çinier, G.; Karakaya, A.; Yıldırım, M.; Güney, B.Ç.; Öz, A.; Gündoğmuş, P.D.; Ösken, A.; Özkan, A.; et al. The effect of 1-year mean step count on the change in the atherosclerotic cardiovascular disease risk calculation in patients with high cardiovascular risk: A sub-study of the LIGHT randomized clinical trial. Kardiol. Pol. 2021, 79, 1140–1142. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model A—patients with low risk and good functional capacity (>7 MET) | - Continuous endurance training for 3–5 days/week, 60–90 min/session, intensity 60–80% of heart rate reserve or 50–70% of maximal exertion level - Resistance training 2–3 sessions/week, 2–3 series/session - Exercise to improve general fitness 5 days/week |
| Model A—patients with moderate risk and good or moderate functional capacity (>5 MET) | - Continuous or interval endurance training for 3–5 days/week, 45–60 min/session, intensity 50–60% of heart rate reserve or 50% of maximal exertion level - Resistance training 2–3 days/week, one series/session - Exercise to improve general fitness for 5 days/week |
| Model C—patients with moderate risk and low functional capacity (3–5 MET) or high risk but good functional capacity (>6 MET) | - Moderate risk patients—interval endurance training for 3–5 days/week, 45 min/session, intensity 40–50% of heart rate reserve or 40–50% of maximal exertion level - High-risk patients—a set of exercises to improve general fitness for 5 days/week |
| Model D—patients with moderate risk and very low functional capacity (<3 MET) or high risk and moderate, low, or very low functional capacity (<6 MET) | - Personalized exercise 2–3 sessions/day for 3–5 days/week, 30–45 min/session, intensity under 20% of heart rate reserve or under a 10–15% increase in HR rest |
| Study Group, Total N = 112 | Women n = 34 (30.4%) | Men n = 78 (69.6%) | p-Value | ||
|---|---|---|---|---|---|
| Age | Mean (SD) Range Me 95% CI | 62.8 (10.1) 35.0–87.0 64.0 [60.9;64.7] | 65.5 (9.8) 39.0–80.0 67.0 [62.1;68.9] | 61.6 (10.1) 35.0–87.0 62.5 [59.3;63.9] | 0.0158 1 |
| BMI | Mean (SD) Range Me 95% CI | 28.6 (4.8) 17.3–40.6 28.7 [27.7;29.5] | 26.8 (4.6) 17.3–36.6 27.0 [25.1;28.4] | 29.4 (4.6) 20.0–40.6 29.0 [28.4;29.0] | 0.0054 2 |
| WHR | Mean (SD) Range Me 95% CI | 0.99 (0.13) 0.65–1.4 0.98 [0.97;1.02] | 0.94 (0.10) 0.65–1.2 0.92 [0.90;0.97] | 1.01 (0.13) 0.8–1.4 1.0 [0.99;1.0] | 0.0016 1 |
| Parameter | Total Cholesterol | HDL | LDL | Triglycerides | LVEF/EF |
|---|---|---|---|---|---|
| Mean (SD) Range Me | 201.6 (54.2) 73.0–310.0 206.0 | 48.3 (16.6) 20.2–124.7 44.8 | 125.3 (45.3) 28.0–232.4 128.0 | 167.3 (105.9) 43.0–651.0 140.5 | 50.5 (8.4) 20.0–65.0 50.0 |
| 95% CI | [191.5;211.8] | [45.2;51.4] | [116.8;133.8] | [147.4;187.1] | [49.0;52.1] |
| Rehabilitation | Parameter | HR Rest | HR Max | HR 1 Min | MET |
|---|---|---|---|---|---|
| Before rehabilitation | Mean (SD) Range Me 95% CI | 72.4 (11.8) 47.0–117.0 71.0 [70.2;74.6] | 113.3 (15.3) 73.0–158.0 114.5 [110.4;116.1] | 90.4 (13.5) 55.0–143.0 90.0 [87.9;93.0] | 6.2 (2.0) 3.0–10.1 6.3 [5.8;6.6] |
| After rehabilitation | Mean (SD) Range Me 95% CI | 72.0 (10.8) 52.0–109.0 70.5 [70.0;74.1] | 122.9 (17.0) 80.0–157.0 124.0 [119.7;126.1] | 97.7 (14.1) 64.0–135.0 98.0 [95.1;100.3] | 8.4 (2.6) 3.5–17.2 8.3 [7.9;8.9] |
| p-value | 0.7174 1 | 0.0000 1 | 0.0000 1 | 0.0000 2 | |
| Rehabilitation | Parameter | Borg RPE | DPr | 6MWT | |
| Before rehabilitation | Mean (SD) Range Me 95% CI | 14.5 (0.6) 13.0–15.0 15.0 [14.4;14.6] | 17,213.8 (3751.9) 8600.0–29,900.0 17,230.0 [16,511.3;17,916.4] | 477.5 (106.7) 90.0–690.0 480.0 [457.5;497.5] | |
| After rehabilitation | Mean (SD) Range Me 95% CI | 13.4 (0.7) 12.0–15.0 14.0 [13.3;13.5] | 19,477.7 (4345.5) 10,400.0–31,120.0 19,355.0 [18,664.0;20,291.3] | 531.2 (98.1) 240.0–750.0 540.0 [512.8;549.6] | |
| p-value | 0.0000 2 | 0.0000 2 | 0.0000 2 | ||
| Variables | Overweight (No—Yes) | Smoking (No—Yes) | Diabetes (No—Yes) | Hyperlipidaemia (No—Yes) | Hypertension (No—Yes) |
|---|---|---|---|---|---|
| Initial HR rest | 0.0394 1 | 0.9278 1 | 0.2882 1 | 0.4836 1 | 0.1060 1 |
| Final HR rest | 0.1096 1 | 0.9534 1 | 0.3413 1 | 0.2990 1 | 0.8493 1 |
| Initial HR max | 0.0394 1 | 0.2403 1 | 0.7934 1 | 0.0423 1 | 0.3793 1 |
| Final HR max | 0.0593 1 | 0.2133 1 | 0.8603 2 | 0.1868 2 | 0.1543 2 |
| Initial HR 1 min | 0.0046 1 | 0.8839 1 | 0.2908 1 | 0.0032 1 | 0.3166 1 |
| Final HR 1 min | 0.0415 2 | 0.1332 1 | 0.6578 2 | 0.5187 2 | 0.6113 2 |
| Initial MET | 0.4040 1 | 0.3080 1 | 0.1332 1 | 0.4155 1 | 0.0405 1 |
| Final MET | 0.4698 1 | 0.1088 1 | 0.0272 1 | 0.5677 1 | 0.0154 1 |
| Initial Borg | 0.3894 1 | 0.7949 1 | 0.1807 1 | 0.7423 1 | 0.0579 1 |
| Final Borg | 0.3840 1 | 0.8425 1 | 0.6457 1 | 0.8034 1 | 0.0338 1 |
| Initial DPr | 0.0005 1 | 0.4129 2 | 0.5258 1 | 0.0332 1 | 0.0541 1 |
| Final DPr | 0.0043 2 | 0.1270 3 | 0.7355 2 | 0.0809 2 | 0.7301 2 |
| Initial 6MWT | 0.4362 1 | 0.0029 1 | 0.3154 1 | 0.4836 1 | 0.0462 1 |
| Final 6MWT | 0.4861 1 | 0.0035 1 | 0.3639 1 | 0.3913 1 | 0.0398 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bryndal, A.; Glowinski, S.; Grochulska, A. Influence of Risk Factors on Exercise Tolerance in Patients after Myocardial Infarction—Early Cardiac Rehabilitation in Poland. J. Clin. Med. 2022, 11, 5597. https://doi.org/10.3390/jcm11195597
Bryndal A, Glowinski S, Grochulska A. Influence of Risk Factors on Exercise Tolerance in Patients after Myocardial Infarction—Early Cardiac Rehabilitation in Poland. Journal of Clinical Medicine. 2022; 11(19):5597. https://doi.org/10.3390/jcm11195597
Chicago/Turabian StyleBryndal, Aleksandra, Sebastian Glowinski, and Agnieszka Grochulska. 2022. "Influence of Risk Factors on Exercise Tolerance in Patients after Myocardial Infarction—Early Cardiac Rehabilitation in Poland" Journal of Clinical Medicine 11, no. 19: 5597. https://doi.org/10.3390/jcm11195597
APA StyleBryndal, A., Glowinski, S., & Grochulska, A. (2022). Influence of Risk Factors on Exercise Tolerance in Patients after Myocardial Infarction—Early Cardiac Rehabilitation in Poland. Journal of Clinical Medicine, 11(19), 5597. https://doi.org/10.3390/jcm11195597