
The Link between Stroke Risk and Orodental Status—A Comprehensive Review

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
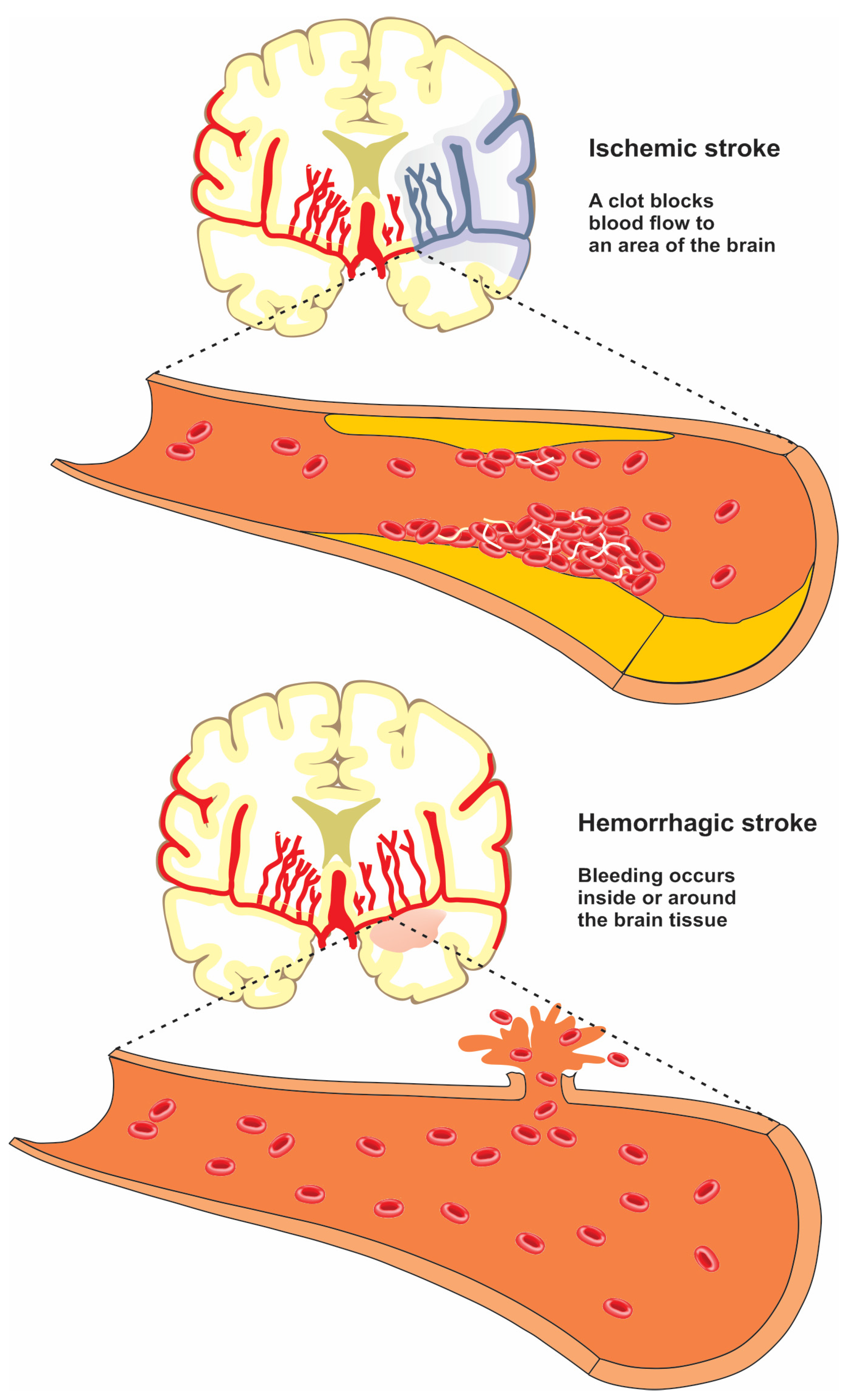
2. Stroke
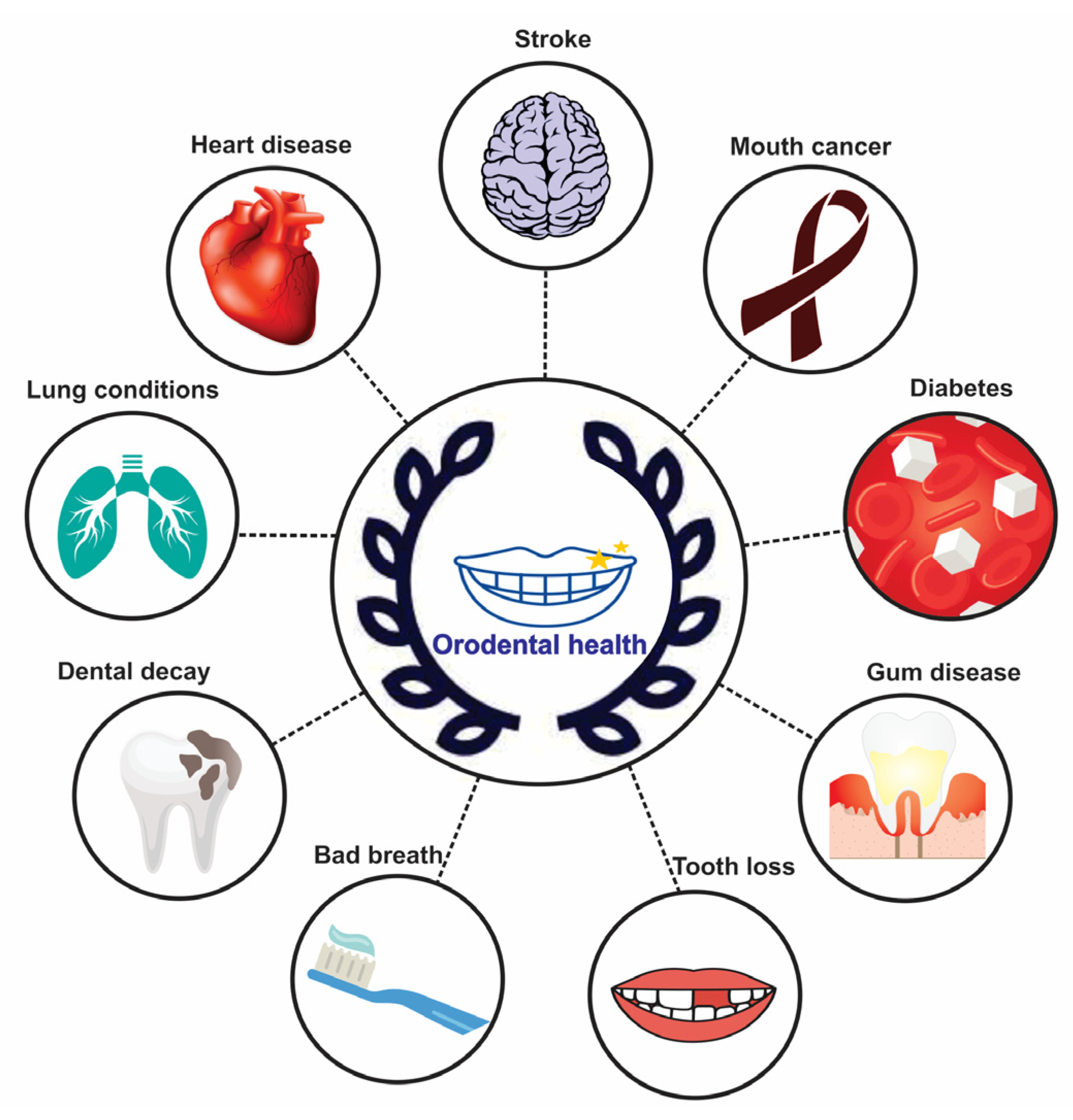
3. Orodental Health
4. Relation between Gum Disease and Stroke
Gingivitis/Periodontitis
5. Relation between Tooth Conditions and Stroke
5.1. Dental Caries
5.2. Tooth Loss
5.3. Endodontic Lesions
6. Effect of Orodental Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yi, X.; Luo, H.; Zhou, J.; Yu, M.; Chen, X.; Tan, L.; Wei, W.; Li, J. Prevalence of stroke and stroke related risk factors: A population based cross sectional survey in southwestern China. BMC Neurol. 2020, 20, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedova, P.; Brown, R.D.; Zvolsky, M.; Belaskova, S.; Volna, M.; Baluchova, J.; Bednarik, J.; Mikulik, R. Incidence of Stroke and Ischemic Stroke Subtypes: A Community-Based Study in Brno, Czech Republic. Cerebrovasc. Dis. 2021, 50, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Sekimoto, Y.; Okamoto, M.; Shibata, S.; Otaka, Y. Association between oral health status and oral food intake level in subacute stroke patients admitted to a convalescent rehabilitation unit. Gerodontology 2022, 39, 67–73. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, L.; Powell, R.; Hulme, S.; Lievesley, M.; Westoby, W.; Zadik, J.; Bowen, A.; Brocklehurst, P.; Smith, C.J. A qualitative exploration of oral health care among stroke survivors living in the community. Health Expect. 2020, 23, 1086–1095. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Ramos-Gomez, F.; Marcus, M.; Maida, C.A.; Wang, Y.; Kinsler, J.J.; Xiong, D.; Lee, S.Y.; Hays, R.D.; Shen, J.; Crall, J.J.; et al. Using a Machine Learning Algorithm to Predict the Likelihood of Presence of Dental Caries among Children Aged 2 to 7. Dent. J. 2021, 9, 141. [Google Scholar] [CrossRef]
- Chung, P.-C.; Chan, T.-C. Association between periodontitis and all-cause and cancer mortality: Retrospective elderly community cohort study. BMC Oral Health 2020, 20, 168. [Google Scholar] [CrossRef]
- Martin-Cabezas, R.; Seelam, N.; Petit, C.; Agossa, K.; Gaertner, S.; Tenenbaum, H.; Davideau, J.-L.; Huck, O. Association between periodontitis and arterial hypertension: A systematic review and meta-analysis. Am. Heart J. 2016, 180, 98–112. [Google Scholar] [CrossRef]
- Rasouli-Ghahroudi, A.A.; Khorsand, A.; Yaghobee, S.; Rokn, A.; Jalali, M.; Masudi, S.; Rahimi, H.; Kabir, A. Oral health status, knowledge, attitude and practice of patients with heart disease. ARYA Atheroscler. 2016, 12, 1–9. [Google Scholar]
- Rawal, I.; Ghosh, S.; Hameed, S.S.; Shivashankar, R.; Ajay, V.S.; Patel, S.A.; Goodman, M.; Ali, M.K.; Narayan, K.; Tandon, N. Association between poor oral health and diabetes among Indian adult population: Potential for integration with NCDs. BMC Oral Health 2019, 19, 191. [Google Scholar] [CrossRef] [PubMed]
- Hamamcilar, O.; Kocahan, T.; AKINOĞLU, B.; Hasanoğlu, A. Effect of poor oral health on respiratory functions and hence sportive performance. Med. J. Islamic World Acad. Sci. 2018, 26, 74–79. [Google Scholar] [CrossRef]
- Beck, J.D.; Offenbacher, S. Systemic effects of periodontitis: Epidemiology of periodontal disease and cardiovascular disease. J. Periodontol. 2005, 76, 2089–2100. [Google Scholar] [CrossRef]
- Sojod, B.; Pidorodeski Nagano, C.; Garcia Lopez, G.M.; Zalcberg, A.; Dridi, S.M.; Anagnostou, F. Systemic lupus erythematosus and periodontal disease: A complex clinical and biological interplay. J. Clin. Med. 2021, 10, 1957. [Google Scholar] [CrossRef]
- Nijakowski, K.; Gruszczyński, D.; Kolasińska, J.; Kopała, D.; Surdacka, A. Periodontal Disease in Patients with Psoriasis: A Systematic Review. Int. J. Environ. Health Res. 2022, 19, 11302. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Tseng, C.-F.; Liu, J.-M.; Chuang, H.-C.; Lei, W.-T.; Liu, L.Y.-M.; Yu, Y.-C.; Hsu, R.-J. Association between periodontal disease and subsequent sjögren’s syndrome: A nationwide population-based cohort study. Int. J. Environ. Health Res. 2019, 16, 771. [Google Scholar] [CrossRef] [Green Version]
- Nijakowski, K.; Lehmann, A.; Rutkowski, R.; Korybalska, K.; Witowski, J.; Surdacka, A. Poor oral hygiene and high levels of inflammatory cytokines in saliva predict the risk of overweight and obesity. Int. J. Environ. Health Res. 2020, 17, 6310. [Google Scholar] [CrossRef]
- Taghat, N.; Lingström, P.; Mossberg, K.; Fändriks, L.; Eliasson, B.; Östberg, A.-L. Oral health by obesity classification in young obese women–a cross-sectional study. Acta Odontol. Scand. 2022; 1–9, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Moazzam, A.A.; Rajagopal, S.M.; Sedghizadeh, P.P.; Zada, G.; Habibian, M. Intracranial bacterial infections of oral origin. J. Clin. Neurosci. 2015, 22, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Takagishi, S.; Arimura, K.; Murata, M.; Iwaki, K.; Okuda, T.; Ido, K.; Nishimura, A.; Narahara, S.; Kawano, T.; Iihara, K. Protein nanoparticles modified with PDGF-B as a novel therapy after acute cerebral infarction. eNeuro 2021, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chioua, M.; Martínez-Alonso, E.; Gonzalo-Gobernado, R.; Ayuso, M.I.; Escobar-Peso, A.; Infantes, L.; Hadjipavlou-Litina, D.; Montoya, J.J.; Montaner, J.; Alcazar, A. New quinolylnitrones for stroke therapy: Antioxidant and neuroprotective (Z)-N-tert-Butyl-1-(2-chloro-6-methoxyquinolin-3-yl) methanimine oxide as a new lead-compound for ischemic stroke treatment. J. Med. Chem. 2019, 62, 2184–2201. [Google Scholar] [CrossRef]
- Mahmoudinezhad, M.; Khalili, M.; Rezaeemanesh, N.; Farhoudi, M.; Eskandarieh, S. Subjective global assessment of malnutrition and dysphagia effect on the clinical and Para-clinical outcomes in elderly ischemic stroke patients: A community-based study. BMC Neurol. 2021, 21, 446. [Google Scholar] [CrossRef] [PubMed]
- Maghsoodi, M.; Rahmani, M.; Ghavimi, H.; Montazam, S.H.; Soltani, S.; Alami, M.; Salatin, S.; Jelvehgari, M. Fast dissolving sublingual films containing sumatriptan alone and combined with methoclopramide: Evaluation in vitro drug release and mucosal permeation. Pharm. Sci. 2016, 22, 153–163. [Google Scholar] [CrossRef]
- Love, C.J.; Selim, M.; Spector, M.; Lo, E.H. Biomaterials for stroke therapy: Key questions in research and clinical translation. Stroke 2019, 50, 2278–2284. [Google Scholar] [CrossRef]
- Wang, H.-K.; Chen, J.-S.; Hsu, C.-Y.; Su, Y.-T.; Sung, T.-C.; Liang, C.-L.; Kwan, A.-L.; Wu, C.-C. A Novel NGF Receptor Agonist B355252 Ameliorates Neuronal Loss and Inflammatory Responses in a Rat Model of Cerebral Ischemia. J. Inflamm. Res. 2021, 14, 2363–2376. [Google Scholar] [CrossRef]
- Farhoudi, M.; Sadigh-Eteghad, S.; Mahmoudi, J.; Farjami, A.; Mahmoudian, M.; Salatin, S. The Therapeutic Benefits of Intravenously Administrated Nanoparticles in Stroke and Age-related Neurodegenerative Diseases. Curr. Pharm. Des. 2022, 28, 1985–2000. [Google Scholar]
- Wood, K.; Stephens, S.E.; Xu, F.; Hazaa, A.; Meek, J.C.; Jensen, H.K.; Jensen, M.O.; Wickramasinghe, R. In Vitro Blood Clot Formation and Dissolution for Testing New Stroke-Treatment Devices. Biomedicines 2022, 10, 1870. [Google Scholar] [CrossRef]
- Zhou, X.B.; Qin, H.; Li, J.; Wang, B.; Wang, C.B.; Liu, Y.M. Platelet-targeted microbubbles inhibit re-occlusion after thrombolysis with transcutaneous ultrasound and microbubbles. Ultrasonics 2011, 51, 270–274. [Google Scholar]
- Bokma, J.P.; Zegstroo, I.; Kuijpers, J.M.; Konings, T.C.; van Kimmenade, R.R.; van Melle, J.P.; Kiès, P.; Mulder, B.J.; Bouma, B.J. Factors associated with coronary artery disease and stroke in adults with congenital heart disease. Heart 2018, 104, 574–580. [Google Scholar] [CrossRef]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Sen, S.; Giamberardino, L.D.; Moss, K.; Morelli, T.; Rosamond, W.D.; Gottesman, R.F.; Beck, J.; Offenbacher, S. Periodontal disease, regular dental care use, and incident ischemic stroke. Stroke 2018, 49, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Alfaddagh, A.; Martin, S.S.; Leucker, T.M.; Michos, E.D.; Blaha, M.J.; Lowenstein, C.J.; Jones, S.R.; Toth, P.P. Inflammation and cardiovascular disease: From mechanisms to therapeutics. Am. J. Prev. Cardiol. 2020, 4, 100130. [Google Scholar] [CrossRef]
- Vidale, S.; Consoli, A.; Arnaboldi, M.; Consoli, D. Postischemic inflammation in acute stroke. J. Clin. Neurol. 2017, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fagundes, N.C.F.; Carvalho, A.P.C.P.S.; Almeida, K.F.B.V.; Magno, M.B.; Maia, L.C.; Lima, R.R. Periodontitis as a risk factor for stroke: A systematic review and meta-analysis. Vasc. Heal. Risk Manag. 2019, 15, 519–532. [Google Scholar] [CrossRef]
- Leão, T.S.S.; Tomasi, G.H.; Conzatti, L.P.; Marrone, L.C.P.; Reynolds, M.A.; Gomes, M.S. Oral Inflammatory Burden and Carotid Atherosclerosis Among Stroke Patients. J. Endod. 2022, 48, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Feng, F.; Zheng, P.; Wang, L.; Wang, Y.; Lv, Y.; Shen, L.; Li, K.; Feng, T.; Chen, Y. Dysregulated lncRNA and mRNA may promote the progression of ischemic stroke via immune and inflammatory pathways: Results from RNA sequencing and bioinformatics analysis. Genes Genom. 2022, 44, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Gu, H.-Q.; Yang, K.-X.; Lin, J.-X.; Jing, J.; Zhao, X.-Q.; Wang, Y.-L.; Liu, L.-P.; Meng, X.; Jiang, Y.; Li, H. Association between high-sensitivity C-reactive protein, functional disability, and stroke recurrence in patients with acute ischaemic stroke: A mediation analysis. EBioMedicine 2022, 80, 104054. [Google Scholar] [CrossRef] [PubMed]
- Dave, R.G.; Geevar, T.; Aaron, S.; Ninan Benjamin, R.; Mammen, J.; Kumar, S.; Vijayan, R.; Gowri, M.; Nair, S.C. Diagnostic utility of flow cytometry based coated-platelets assay as a biomarker to predict thrombotic or hemorrhagic phenotype in acute stroke. Cytom. Part B Clin. Cytom. 2022, 102, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Ge, Y.; Liu, Y.; Zheng, Y.; Hu, R.; Ren, C.; Liu, Q. Identification of the key genes and immune infiltrating cells determined by sex differences in ischaemic stroke through co-expression network module. IET Syst. Biol. 2022, 16, 28–41. [Google Scholar] [CrossRef]
- Coveney, S.; Murphy, S.; Belton, O.; Cassidy, T.; Crowe, M.; Dolan, E.; de Gaetano, M.; Harbison, J.; Horgan, G.; Marnane, M. Inflammatory cytokines, high-sensitivity C-reactive protein, and risk of one-year vascular events, death, and poor functional outcome after stroke and transient ischemic attack. Int. J. Stroke 2022, 17, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Yang, Y.; Yin, N.; Liu, C.; Zhao, Y.; Cheng, H.; Zhou, T.; Zhang, Z.; Zhang, K. Engineering CXCL12 Biomimetic Decoy-Integrated Versatile Immunosuppressive Nanoparticle for Ischemic Stroke Therapy with Management of Overactivated Brain Immune Microenvironment. Small Methods 2022, 6, 2101158. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Z.; Wang, J.; Zhang, X.; Zhao, J.; Bai, N.; Vijayalakshmi, A.; Huo, Q. Scutellarin alleviates cerebral ischemia/reperfusion by suppressing oxidative stress and inflammatory responses via MAPK/NF-κB pathways in rats. Environ. Toxicol. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Alhadidi, Q.; Shah, Z.A. Cofilin mediates LPS-induced microglial cell activation and associated neurotoxicity through activation of NF-κB and JAK–STAT pathway. Mol. Neurobiol. 2018, 55, 1676–1691. [Google Scholar] [CrossRef] [PubMed]
- Jeerakathil, T.; Shuaib, A.; Majumdar, S.R.; Demchuk, A.M.; Butcher, K.S.; Watson, T.J.; Dean, N.; Gordon, D.; Edmond, C.; Coutts, S.B. The A lberta S troke P revention in TIAs and mild strokes (ASPIRE) intervention: Rationale and design for evaluating the implementation of a province-wide TIA T riaging system. Int. J. Stroke 2014, 9, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.A.; Andersen, J.; Kent, T.; Williams, L.S.; Damush, T.M. Using intervention mapping to develop and adapt a secondary stroke prevention program in Veterans Health Administration medical centers. Implement. Sci. 2010, 5, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, M.; Taylor, G.W.; Manz, M.C.; Yoshihara, A.; Sato, M.; Muramatsu, K.; Watanabe, R.; Miyazaki, H. Oral health status: Relationship to nutrient and food intake among 80-year-old Japanese adults. Community Dent. Oral Epidemiol. 2014, 42, 441–450. [Google Scholar] [CrossRef] [Green Version]
- Sabbah, W.; Folayan, M.O.; El Tantawi, M. The Link between Oral and General Health. Int. Dent. J. 2019, 2019, 7862923. [Google Scholar] [CrossRef] [Green Version]
- Bhambri, T. Role of Oral Microbial Flora in Health and Illness. J. Adv. Med. Dent. Sci. 2020, 8, 53–60. [Google Scholar]
- Lee, J.S.; Somerman, M.J. The importance of oral health in comprehensive health care. JAMA 2018, 320, 339–340. [Google Scholar] [CrossRef]
- Kim, H.; Park, J.; Lee, W.; Kim, Y.; Lee, Y. Differences in the oral health status and oral hygiene practices according to the extent of post-stroke sequelae. J. Oral Rehabil. 2018, 45, 476–484. [Google Scholar] [CrossRef]
- Zotti, F.; Dalessandri, D.; Salgarello, S.; Piancino, M.; Bonetti, S.; Visconti, L.; Paganelli, C. Usefulness of an app in improving oral hygiene compliance in adolescent orthodontic patients. Angle Orthod. 2016, 86, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Sharifi, S.; Samani, A.; Ahmadian, E.; Eftekhari, A.; Derakhshankhah, H.; Jafari, S.; Mokhtarpour, M.; Vahed, S.Z.; Salatin, S.; Dizaj, S.M. Oral delivery of proteins and peptides by mucoadhesive nanoparticles. Biointerface Res. Appl. Chem. 2019, 9, 3849–3852. [Google Scholar]
- Sato, H.; Yano, A.; Shimoyama, Y.; Sato, T.; Sugiyama, Y.; Kishi, M. Associations of streptococci and fungi amounts in the oral cavity with nutritional and oral health status in institutionalized elders: A cross sectional study. BMC Oral Health 2021, 21, 590. [Google Scholar] [CrossRef]
- Alghamdi, S. Isolation and identification of the oral bacteria and their characterization for bacteriocin production in the oral cavity. Saudi J. Biol. Sci. 2022, 29, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Lu, N.; Xiao, Y.; Zhang, Y.; Tang, Z.; Zhang, M. Metal-Nanoparticle-Supported Nanozyme-Based Colorimetric Sensor Array for Precise Identification of Proteins and Oral Bacteria. ACS Appl. Mater. Interfaces 2022, 14, 11156–11166. [Google Scholar] [CrossRef]
- Bosma, M.L.; McGuire, J.A.; Sunkara, A.; Sullivan, P.; Yoder, A.; Milleman, J.; Milleman, K. Efficacy of Flossing and Mouthrinsing Regimens on Plaque and Gingivitis: A randomized clinical trial. Am. Dent. Hyg. Assoc. 2022, 96, 8–20. [Google Scholar]
- Milleman, J.; Bosma, M.L.; McGuire, J.A.; Sunkara, A.; McAdoo, K.; DelSasso, A.; Wills, K.; Milleman, K. Comparative Effectiveness of Toothbrushing, Flossing and Mouthrinse Regimens on Plaque and Gingivitis: A 12-week virtually supervised clinical trial. Am. Dent. Hyg. Assoc. 2022, 96, 21–34. [Google Scholar]
- Umeizudike, K.A.; Lähteenmäki, H.; Räisänen, I.T.; Taylor, J.J.; Preshaw, P.M.; Bissett, S.M.; Tervahartiala, T.; Nwhator, S.O.; Pärnänen, P.; Sorsa, T. Ability of matrix metalloproteinase-8 biosensor, IFMA, and ELISA immunoassays to differentiate between periodontal health, gingivitis, and periodontitis. J. Periodontal Res. 2022, 57, 558–567. [Google Scholar] [CrossRef]
- Kurek-Górecka, A.; Walczyńska-Dragon, K.; Felitti, R.; Baron, S.; Olczyk, P. Propolis and Diet Rich in Polyphenols as Cariostatic Agents Reducing Accumulation of Dental Plaque. Molecules 2022, 27, 271. [Google Scholar] [CrossRef]
- Ma, K.S.K.; Lai, J.N.; Veeravalli, J.J.; Chiu, L.T.; Van Dyke, T.E.; Wei, J.C.C. Fibromyalgia and periodontitis: Bidirectional associations in population-based 15-year retrospective cohorts. J. Periodontol. 2022, 93, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the normal bacterial flora of the oral cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [Green Version]
- Periasamy, S.; Kolenbrander, P.E. Central role of the early colonizer Veillonella sp. in establishing multispecies biofilm communities with initial, middle, and late colonizers of enamel. J. Bacteriol. 2010, 192, 2965–2972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, C.P.; Oliveira, F.A.F.; de Barros Silva, P.G.; Alves, A.P.N.N.; Mota, M.R.L.; Montenegro, R.C.; Burbano, R.M.R.; Seabra, A.D.; Lobo Filho, J.G.; Lima, D.L.F. Molecular analysis of oral bacteria in dental biofilm and atherosclerotic plaques of patients with vascular disease. Int. J. Cardiol. 2014, 174, 710–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawato, T.; Tanaka, H.; Tabuchi, M.; Ooshima, K.; Nakai, K.; Yamashita, Y.; Maeno, M. Continual Gram-negative bacterial challenge accelerates stroke onset in stroke-prone spontaneously hypertensive rats. Clin. Exp. Hypertens. 2013, 35, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Hokamura, K.; Taniguchi, N.; Wada, K.; Kudo, C.; Nomura, R.; Kojima, A.; Naka, S.; Muranaka, Y.; Thura, M. The collagen-binding protein of Streptococcus mutans is involved in haemorrhagic stroke. Nat. Commun. 2011, 2, 485. [Google Scholar] [CrossRef] [Green Version]
- Ihara, M.; Yamamoto, Y. Emerging evidence for pathogenesis of sporadic cerebral small vessel disease. Stroke 2016, 47, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Tonomura, S.; Ihara, M.; Kawano, T.; Tanaka, T.; Okuno, Y.; Saito, S.; Friedland, R.P.; Kuriyama, N.; Nomura, R.; Watanabe, Y. Intracerebral hemorrhage and deep microbleeds associated with cnm-positive Streptococcus mutans; a hospital cohort study. Sci. Rep. 2016, 6, 20074. [Google Scholar] [CrossRef] [Green Version]
- Sansores-España, L.D.; Melgar-Rodríguez, S.; Olivares-Sagredo, K.; Cafferata, E.A.; Martínez-Aguilar, V.M.; Vernal, R.; Paula-Lima, A.C.; Díaz-Zúñiga, J. Oral-Gut-Brain Axis in Experimental Models of Periodontitis: Associating Gut Dysbiosis with Neurodegenerative Diseases. Front. Aging 2021, 2, 781582. [Google Scholar] [CrossRef]
- Nijakowski, K.; Gruszczyński, D.; Surdacka, A. Oral Health Status in Patients with Inflammatory Bowel Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11521. [Google Scholar] [CrossRef]
- Ray, K. The oral–gut axis in IBD. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 532. [Google Scholar] [CrossRef]
- Albuquerque-Souza, E.; Sahingur, S.E. Periodontitis, chronic liver diseases, and the emerging oral-gut-liver axis. Periodontol 2000 2022, 89, 125–141. [Google Scholar] [CrossRef]
- Chang, Y.; Woo, H.G.; Lee, J.S.; Song, T.J. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 2021, 92, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; He, T.; Yue, F.; Xu, X.; Wang, L.; Zhu, P.; Teng, F.; Sun, Z.; Liu, X.; Jing, G. Longitudinal multi-omics and microbiome meta-analysis identify an asymptomatic gingival state that links gingivitis, periodontitis, and aging. mBio 2021, 12, e03281-20. [Google Scholar] [CrossRef]
- de Faria, J.B.; de Souza Furtado, T.C.; de Assunção, T.S.F.; Abdalla, D.R.; Andrade, F.M.; Bertoldo, B.B.; de Paula Amaral, E.; Rodrigues, D.B.R.; Júnior, V.R.; de Lima Pereira, S.A. Immunological evaluation of the crevicular fluid in patients with gingivitis, periodontitis, and peri-implantitis: A 1-year cross-sectional study. Res. Soc. Dev. 2021, 10, e41101320756. [Google Scholar] [CrossRef]
- Zuza, E.P.; Garcia, V.G.; Theodoro, L.H.; Ervolino, E.; Favero, L.F.V.; Longo, M.; Ribeiro, F.S.; Martins, A.T.; Spolidorio, L.C.; Zuanon, J.A.S. Influence of obesity on experimental periodontitis in rats: Histopathological, histometric and immunohistochemical study. Clin. Oral Investig. 2018, 22, 1197–1208. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Hung, H.-C.; Rimm, E.B.; Willett, W.C.; Ascherio, A. Periodontal disease, tooth loss, and incidence of ischemic stroke. Stroke 2003, 34, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Abolfazli, N.; Ghoreishizadeh, A.; Ayramlu, H.; Ghavimi, M.; Ghoreishizadeh, M.; Salehsaber, F. Periodontal disease and risk of cerebral ischemic stroke. J. Neurol. Sci. 2011, 28, 307–316. [Google Scholar]
- Mustapha, I.Z.; Debrey, S.; Oladubu, M.; Ugarte, R. Markers of systemic bacterial exposure in periodontal disease and cardiovascular disease risk: A systematic review and meta-analysis. J. Periodontol. 2007, 78, 2289–2302. [Google Scholar]
- Lin, H.W.; Chen, C.M.; Yeh, Y.C.; Chen, Y.Y.; Guo, R.Y.; Lin, Y.P.; Li, Y.C. Dental treatment procedures for periodontal disease and the subsequent risk of ischaemic stroke: A retrospective population-based cohort study. J. Clin. Periodontol. 2019, 46, 642–649. [Google Scholar] [CrossRef]
- Beck, J.; Garcia, R.; Heiss, G.; Vokonas, P.S.; Offenbacher, S. Periodontal disease and cardiovascular disease. J. Periodontol. 1996, 67, 1123–1137. [Google Scholar] [CrossRef]
- Pillai, R.S.; Iyer, K.; Spin-Neto, R.; Kothari, S.F.; Nielsen, J.F.; Kothari, M. Oral health and brain injury: Causal or casual relation? Cerebrovasc. Dis. Extra 2018, 8, 1–15. [Google Scholar] [CrossRef]
- Tribble, G.D.; Lamont, R.J. Bacterial invasion of epithelial cells and spreading in periodontal tissue. Periodontol 2000 2010, 52, 68. [Google Scholar] [CrossRef] [PubMed]
- Pizzo, G.; Guiglia, R.; Russo, L.L.; Campisi, G. Dentistry and internal medicine: From the focal infection theory to the periodontal medicine concept. Eur. J. Intern. Med. 2010, 21, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Cabała, A.; Chomyszyn-Gajewska, M.; Drozdz, W. The impact of periodontal infection on systemic inflammatory process and atherosclerosis. Przegląd Lek. 2006, 63, 681–684. [Google Scholar]
- Sfyroeras, G.S.; Roussas, N.; Saleptsis, V.G.; Argyriou, C.; Giannoukas, A.D. Association between periodontal disease and stroke. J. Vasc. Surg. 2012, 55, 1178–1184. [Google Scholar] [CrossRef] [Green Version]
- Mayr, M.; Metzler, B.; Kiechl, S.; Willeit, J.; Schett, G.; Xu, Q.; Wick, G. Endothelial cytotoxicity mediated by serum antibodies to heat shock proteins of Escherichia coli and Chlamydia pneumoniae: Immune reactions to heat shock proteins as a possible link between infection and atherosclerosis. Circulation 1999, 99, 1560–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, K.; Nabuchi, A.; Ito, R.; Miyachi, K.; Kuramitsu, H.K.; Okuda, K. Correlation between detection rates of periodontopathic bacterial DNA in carotid coronary stenotic artery plaque and in dental plaque samples. J. Clin. Microbiol. 2004, 42, 1313–1315. [Google Scholar] [CrossRef] [Green Version]
- Nakano, K.; Nemoto, H.; Nomura, R.; Inaba, H.; Yoshioka, H.; Taniguchi, K.; Amano, A.; Ooshima, T. Detection of oral bacteria in cardiovascular specimens. Oral Microbiol. Immunol. 2009, 24, 64–68. [Google Scholar] [CrossRef]
- Paraskevas, S.; Huizinga, J.D.; Loos, B.G. A systematic review and meta-analyses on Creactive protein in relation to periodontitis. J. Clin. Periodontol. 2008, 35, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Seoane, J.; Blanco, M.; Rodriguez-Yanez, M.; Takkouche, B.; Blanco, J.; Castillo, J. Association between periodontitis and ischemic stroke: A systematic review and meta-analysis. Eur. J. Epidemiol. 2017, 32, 43–53. [Google Scholar] [CrossRef]
- Hashemipour, M.A.; Afshar, A.J.; Borna, R.; Seddighi, B.; Motamedi, A. Gingivitis and periodontitis as a risk factor for stroke: A case-control study in the Iranian population. Dent. Res. J. 2013, 10, 613–619. [Google Scholar]
- Syrjänen, J.; Valtonen, V.; Livanainen, M.; Hovi, T.; Malkamäki, M.; Mäkelä, P. Association between cerebral infarction and increased serum bacterial antibody levels in young adults. Acta Psychiatr. Scand. 1986, 73, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Lafon, A.; Tala, S.; Ahossi, V.; Perrin, D.; Giroud, M.; Béjot, Y. Association between periodontal disease and non-fatal ischemic stroke: A case-control study. Acta Odontol. Scand. 2014, 72, 687–693. [Google Scholar] [CrossRef]
- Kim, H.D.; Sim, S.J.; Moon, J.Y.; Hong, Y.C.; Han, D.H. Association between periodontitis and hemorrhagic stroke among Koreans: A case-control study. J. Periodontol. 2010, 81, 658–665. [Google Scholar] [CrossRef] [Green Version]
- Sen, S.; Sumner, R.; Hardin, J.; Barros, S.; Moss, K.; Beck, J.; Offenbacher, S. Periodontal disease and recurrent vascular events in stroke/transient ischemic attack patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 1420–1427. [Google Scholar] [CrossRef] [Green Version]
- Howell, T.H.; Ridker, P.M.; Ajani, U.A.; Christen, W.G.; Hennekens, C.H. Periodontal disease and risk of subsequent cardiovascular disease in US male physicians. J. Am. Coll. Cardiol. 2001, 37, 445–450. [Google Scholar] [CrossRef] [Green Version]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; DeRouen, T.A. Periodontal disease and coronary heart disease risk. JAMA 2000, 284, 1406–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabharwal, A.; Stellrecht, E.; Scannapieco, F.A. Associations between dental caries and systemic diseases: A scoping review. BMC Oral Health 2021, 21, 472. [Google Scholar] [CrossRef]
- Kelishadi, R.; Mortazavi, S.; Hossein, T.R.; Poursafa, P. Association of cardiometabolic risk factors and dental caries in a population-based sample of youths. Diabetol. Metab. Syndr. 2010, 2, 22. [Google Scholar] [CrossRef] [Green Version]
- Sen, S.; Curtis, J.; Hicklin, D.; Nichols, C.; Rosamond, W.; Gottesman, R.; Moss, K.; Divaris, K.; Beck, J.; Offenbacher, S. Dental Caries Associated with Incident Ischemic Stroke: Atherosclerosis Risk In Communities Study (4329). Neurology 2021, 96, 4329. [Google Scholar]
- Valm, A.M. The structure of dental plaque microbial communities in the transition from health to dental caries and periodontal disease. J. Mol. Biol. 2019, 431, 2957–2969. [Google Scholar] [CrossRef] [PubMed]
- Grau, A.J.; Becher, H.; Ziegler, C.M.; Lichy, C.; Buggle, F.; Kaiser, C.; Lutz, R.; Bültmann, S.; Preusch, M.; Dörfer, C.E. Periodontal disease as a risk factor for ischemic stroke. Stroke 2004, 35, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Gerreth, P.; Maciejczyk, M.; Zalewska, A.; Gerreth, K.; Hojan, K. Comprehensive evaluation of the oral health status, salivary gland function, and oxidative stress in the saliva of patients with subacute phase of stroke: A case-control study. J. Clin. Med. 2020, 9, 2252. [Google Scholar] [CrossRef]
- Anbarserri, N.M.; Ismail, K.M.; Anbarserri, H.; Alanazi, D.; AlSaffan, A.D.; Baseer, M.A.; Shaheen, R. Impact of severity of tooth loss on oral-health-related quality of life among dental patients. J. Fam. Med. Prim. Care 2020, 9, 187–191. [Google Scholar]
- Burt, B.; Ismail, A.; Morrison, E.; Beltran, E. Risk factors for tooth loss over a 28-year period. J. Dent. Res. 1990, 69, 1126–1130. [Google Scholar] [CrossRef]
- Klock, K.S.; Haugejorden, O. Primary reasons for extraction of permanent teeth in Norway: Changes from 1968 to 1988. Community Dent. Oral Epidemiol. 1991, 19, 336–341. [Google Scholar] [CrossRef]
- Papapanou, P.N. Periodontal diseases: Epidemiology. Ann. Periodontol. 1996, 1, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Oluwagbemigun, K.; Dietrich, T.; Pischon, N.; Bergmann, M.; Boeing, H. Association between number of teeth and chronic systemic diseases: A cohort study followed for 13 years. PLoS ONE 2015, 10, e0123879. [Google Scholar] [CrossRef]
- Del Pinto, R.; Monaco, A.; Ortu, E.; Czesnikiewicz-Guzik, M.; Muñoz Aguilera, E.; Giannoni, M.; D’Aiuto, F.; Guzik, T.J.; Ferri, C.; Pietropaoli, D. Access to dental care and blood pressure profiles in adults with high socioeconomic status. J. Periodontol. 2022, 93, 1060–1071. [Google Scholar] [CrossRef]
- Gong, P.; Tian, Q.; He, Y.; He, P.; Wang, J.; Guo, Y.; Ye, Q.; Li, M. Dental pulp stem cell transplantation facilitates neuronal neuroprotection following cerebral ischemic stroke. Biomed. Pharmacother. 2022, 152, 113234. [Google Scholar] [CrossRef]
- Shimizu, Y.; Takeda-Kawaguchi, T.; Kuroda, I.; Hotta, Y.; Kawasaki, H.; Hariyama, T.; Shibata, T.; Akao, Y.; Kunisada, T.; Tatsumi, J. Exosomes from dental pulp cells attenuate bone loss in mouse experimental periodontitis. J. Periodontal Res. 2022, 57, 162–172. [Google Scholar] [CrossRef]
- Mikami, R.; Mizutani, K.; Matsuyama, Y.; Gohda, T.; Gotoh, H.; Aoyama, N.; Matsuura, T.; Kido, D.; Takeda, K.; Saito, N. Association of type 2 diabetes with periodontitis and tooth loss in patients undergoing hemodialysis. PLoS ONE 2022, 17, e0267494. [Google Scholar] [CrossRef]
- Hua, J.; Lu, J.; Tang, X.; Fang, Q. Association between Geriatric Nutritional Risk Index and Depression after Ischemic Stroke. Nutrients 2022, 14, 2698. [Google Scholar] [CrossRef]
- Han, X.; Cai, J.; Li, Y.; Rong, X.; Li, Y.; He, L.; Li, H.; Liang, Y.; Huang, H.; Xu, Y. Baseline Objective Malnutritional Indices as Immune-Nutritional Predictors of Long-Term Recurrence in Patients with Acute Ischemic Stroke. Nutrients 2022, 14, 1337. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, B.L.; Gamborg, M. Remaining teeth, cardiovascular morbidity and death among adult Danes. Prev. Med. 2008, 47, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Choe, H.; Kim, Y.H.; Park, J.W.; Kim, S.Y.; Lee, S.-Y.; Jee, S.H. Tooth loss, hypertension and risk for stroke in a Korean population. Atherosclerosis 2009, 203, 550–556. [Google Scholar] [CrossRef]
- Abnet, C.C.; Qiao, Y.-L.; Dawsey, S.M.; Dong, Z.-W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K. The relationship between oral conditions and ischemic stroke and peripheral vascular disease. J. Am. Dent. Assoc. 2002, 133, 23S–30S. [Google Scholar] [CrossRef]
- Wu, T.; Trevisan, M.; Genco, R.J.; Dorn, J.P.; Falkner, K.L.; Sempos, C.T. Periodontal disease and risk of cerebrovascular disease: The first national health and nutrition examination survey and its follow-up study. Arch. Intern. Med. 2000, 160, 2749–2755. [Google Scholar] [CrossRef] [Green Version]
- Joshy, G.; Arora, M.; Korda, R.J.; Chalmers, J.; Banks, E. Is poor oral health a risk marker for incident cardiovascular disease hospitalisation and all-cause mortality? Findings from 172 630 participants from the prospective 45 and Up Study. BMJ Open 2016, 6, e012386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, H.I.; Ellison, L.F.; Taylor, G.W. Periodontal disease and risk of fatal coronary heart and cerebrovascular diseases. J. Cardiovasc. Risk 1999, 6, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Patrakka, O.; Mehtonen, H.; Tuomisto, S.; Pienimäki, J.-P.; Ollikainen, J.; Huhtala, H.; Pessi, T.; Oksala, N.; Lehtimäki, T.; Järnstedt, J.; et al. Association between Oral Pathology, Carotid Stenosis, and Oral Bacterial DNA in Cerebral Thrombi of Patients with Stroke. Stroke Res. Treat. 2021, 2021, 5402764. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Redd, K.; Trivedi, T.; Moss, K.; Alonso, A.; Soliman, E.Z.; Magnani, J.W.; Chen, L.Y.; Gottesman, R.F.; Rosamond, W.; et al. Periodontal Disease, Atrial Fibrillation and Stroke. Am. Heart J. 2021, 235, 36–43. [Google Scholar] [CrossRef]
- Cho, H.J.; Shin, M.S.; Song, Y.; Park, S.K.; Park, S.M.; Kim, H.D. Severe Periodontal Disease Increases Acute Myocardial Infarction and Stroke: A 10-Year Retrospective Follow-up Study. J. Dent. Res. 2021, 100, 706–713. [Google Scholar] [CrossRef]
- Lafon, A.; Pereira, B.; Dufour, T.; Rigouby, V.; Giroud, M.; Béjot, Y.; Tubert-Jeannin, S. Periodontal disease and stroke: A meta-analysis of cohort studies. Eur. J. Neurol. 2014, 21, 1155–1161. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Zambrano, M.; Del Brutto, V.J. Severe edentulism is a major risk factor influencing stroke incidence in rural Ecuador (The Atahualpa Project). Int. J. Stroke 2017, 12, 201–204. [Google Scholar] [CrossRef]
- Shin, H.-E.; Park, E.-J.; Jung, E.-K.; Kim, E.-K.; Cho, M.-J. The Relationship between oral health and stroke in adults based on the 6th (2015) Korea National Health and Nutrition Examination Survey. J. Dent. Hyg. Sci. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Cheng, F.; Zhang, M.; Wang, Q.; Xu, H.; Dong, X.; Gao, Z.; Chen, J.; Wei, Y.; Qin, F. Tooth loss and risk of cardiovascular disease and stroke: A dose-response meta analysis of prospective cohort studies. PLoS ONE 2018, 13, e0194563. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, M.; Akagawa, Y. The relationship between tooth loss and cerebral stroke. Jpn. Dent. Sci. Rev. 2011, 47, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Wiener, R.C. Tooth loss and stroke: Results from the behavioral risk factor surveillance system, 2010. Am. Dent. Hyg. Assoc. 2014, 88, 285–291. [Google Scholar]
- You, Z.; Cushman, M.; Jenny, N.S.; Howard, G. Tooth loss, systemic inflammation, and prevalent stroke among participants in the reasons for geographic and racial difference in stroke (REGARDS) study. Atherosclerosis 2009, 203, 615–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernawati, S. The Relationship Between Oral Cavity Infections and the Occurance of Stroke. In Proceedings of the 7th International Meeting and the 4th Joint Scientific Meeting in Dentistry, Surabaya, Indonesia, 5–7 October 2017; pp. 259–262. [Google Scholar]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Arena, C.; Caponio, V.C.A.; Caloro, G.A.; Zhurakivska, K.; Adipietro, I.; Troiano, G.; Lo Muzio, L. Inspection of the microbiota in endodontic lesions. Dent. J. 2019, 7, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portelli, M.; Militi, A.; Lo Giudice, A.; Lo Giudice, R.; Rustico, L.; Fastuca, R.; Nucera, R. 3D assessment of endodontic lesions with a low-dose CBCT protocol. Dent. J. 2020, 8, 51. [Google Scholar] [CrossRef] [PubMed]
- Aloutaibi, Y.A.; Alkarim, A.S.; Qumri, E.M.; Almansour, L.A.; Alghamdi, F.T. Chronic Endodontic Infections and Cardiovascular Diseases: Does the Evidence Support an Independent Association? Cureus 2021, 13, e19864. [Google Scholar] [CrossRef]
- Segura-Sampedro, J.J.; Jiménez-Giménez, C.; Jane-Salas, E.; Cabanillas-Balsera, D.; Martín-González, J.; Segura-Egea, J.J.; López-López, J. Periapical and endodontic status of patients with inflammatory bowel disease: Age-and sex-matched case–control study. Int. Endod. J. 2022, 55, 748–757. [Google Scholar] [CrossRef]
- Dizaj, S.M.; Rad, A.A.; Safaei, N.; Salatin, S.; Ahmadian, E.; Sharifi, S.; Vahed, S.Z.; Lotfipour, F.; Shahi, S. The application of nanomaterials in cardiovascular diseases: A review on drugs and devices. J. Pharm. Pharm. Sci. 2019, 22, 501–515. [Google Scholar] [CrossRef] [Green Version]
- Bergandi, L.; Giuggia, B.; Alovisi, M.; Comba, A.; Silvagno, F.; Maule, M.; Aldieri, E.; Scotti, N.; Scacciatella, P.; Conrotto, F. Endothelial dysfunction marker variation in young adults with chronic apical periodontitis before and after endodontic treatment. J. Endod. 2019, 45, 500–506. [Google Scholar] [CrossRef]
- Rôças, I.; Siqueira Jr, J. Root canal microbiota of teeth with chronic apical periodontitis. J. Clin. Microbiol. 2008, 46, 3599–3606. [Google Scholar] [CrossRef] [Green Version]
- Dorn, B.; Harris, L.; Wujick, C.; Vertucci, F.; Progulske-Fox, A. Invasion of vascular cells in vitro by Porphyromonas endodontalis. Int. Endod. J. 2002, 35, 366–371. [Google Scholar] [CrossRef]
- Gomes, M.S.; Blattner, T.C.; Sant’Ana Filho, M.; Grecca, F.S.; Hugo, F.N.; Fouad, A.F.; Reynolds, M.A. Can apical periodontitis modify systemic levels of inflammatory markers? A systematic review and meta-analysis. J. Endod. 2013, 39, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Sebring, D.; Buhlin, K.; Norhammar, A.; Rydén, L.; Jonasson, P.; EndoReCo; Lund, H.; Kvist, T.; Bjørndal, L.; Dawson, V. Endodontic inflammatory disease: A risk indicator for a first myocardial infarction. Int. Endod. J. 2022, 55, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Caplan, D.J.; Pankow, J.S.; Cai, J.; Offenbacher, S.; Beck, J.D. The relationship between self-reported history of endodontic therapy and coronary heart disease in the Atherosclerosis Risk in Communities Study. J. Am. Dent. Assoc. 2009, 140, 1004–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pussinen, P.J.; Alfthan, G.; Jousilahti, P.; Paju, S.; Tuomilehto, J. Systemic exposure to Porphyromonas gingivalis predicts incident stroke. Atherosclerosis 2007, 193, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Bugueno, I.M.; Zobairi El-Ghazouani, F.; Batool, F.; El Itawi, H.; Anglès-Cano, E.; Benkirane-Jessel, N.; Toti, F.; Huck, O. Porphyromonas gingivalis triggers the shedding of inflammatory endothelial microvesicles that act as autocrine effectors of endothelial dysfunction. Sci. Rep. 2020, 10, 1778. [Google Scholar] [CrossRef] [Green Version]
- Goldfeld, S.; Francis, K.L.; O’Connor, E.; Ludvigsson, J.; Faresjö, T.; Nikiema, B.; Gauvin, L.; Yang-Huang, J.; Abu Awad, Y.; McGrath, J.J. Comparative inequalities in child dental caries across four countries: Examination of international birth cohorts and implications for oral health policy. PLoS ONE 2022, 17, e0268899. [Google Scholar] [CrossRef]
- D’Souza, R.N.; Collins, F.S.; Murthy, V.H. Oral health for all—realizing the promise of science. N. Engl. J. Med. 2022, 386, 809–811. [Google Scholar] [CrossRef]
- Choi, S.E.; Sima, C.; Pandya, A. Impact of treating oral disease on preventing vascular diseases: A model-based cost-effectiveness analysis of periodontal treatment among patients with type 2 diabetes. Diabetes Care 2020, 43, 563–571. [Google Scholar] [CrossRef]
- Orlandi, M.; Graziani, F.; D’Aiuto, F. Periodontal therapy and cardiovascular risk. Periodontol 2000 2020, 83, 107–124. [Google Scholar] [CrossRef]
- Minassian, C.; D’Aiuto, F.; Hingorani, A.D.; Smeeth, L. Invasive dental treatment and risk for vascular events: A self-controlled case series. Ann. Intern. Med. 2010, 153, 499–506. [Google Scholar] [CrossRef]
- Baba, N.D. Cancer of the oral cavity in three brothers of the whole blood in Mauritania. Pan Afr. Med. J. 2016, 25, 156. [Google Scholar]
- Singhvi, H.R.; Malik, A.; Chaturvedi, P. The role of chronic mucosal trauma in oral cancer: A review of literature. Indian J. Med. Paediatr. Oncol. 2017, 38, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behnoud, F.; Torabian, S.; Zargaran, M. Relationship between oral poor hygiene and broken teeth with oral tongue squamous cell carcinoma. Acta Med. Iran. 2011, 49, 159–162. [Google Scholar] [PubMed]
- Deng, Q.; Yan, L.; Lin, J.; Zhuang, Z.; Hong, Y.; Hu, C.; Lin, L.; Pan, L.; Shi, B.; Wang, J. A composite oral hygiene score and the risk of oral cancer and its subtypes: A large-scale propensity score-based study. Clin. Oral Investig. 2022, 26, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Nath, S.; Ferreira, J.; McVicar, A.; Oshilaja, T.; Swann, B. Rise in oral cancer risk factors associated with the COVID-19 pandemic mandates a more diligent approach to oral cancer screening and treatment. J. Am. Dent. Assoc. 2022, 153, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Narayan, T.; Revanna, G.; Hallikeri, U.; Kuriakose, M.A. Dental caries and periodontal disease status in patients with oral squamous cell carcinoma: A screening study in urban and semiurban population of Karnataka. J. Oral Maxillofac. Surg. 2014, 13, 435–443. [Google Scholar] [CrossRef]
- Wu, Y.T.; Chen, C.Y.; Lai, W.T.; Kuo, C.C.; Huang, Y.B. Increasing risks of ischemic stroke in oral cancer patients treated with radiotherapy or chemotherapy: A nationwide cohort study. Int. J. Neurosci. 2015, 125, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Kanai, K.; Mandai, T.; Shibata, A.; Takahashi, Y.; Hirata, Y.; Furuki, Y. Perioperative stroke in a patient undergoing surgery for oral cancer: A case report. Oncol. Lett. 2016, 12, 2660–2663. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.F.; Kuo, Y.L.; Pu, C.; Chou, Y.J. Neck dissection and stroke in patients with oral cavity cancer: A population-based cohort study. Head Neck 2017, 39, 63–70. [Google Scholar] [CrossRef]
- Gerreth, P.; Gerreth, K.; Maciejczyk, M.; Zalewska, A.; Hojan, K. Is an oral health status a predictor of functional improvement in ischemic stroke patients undergoing comprehensive rehabilitation treatment? Brain Sci. 2021, 11, 338. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Design | Oral Health Factor | Sample Size | Follow Up | Country | Stroke Subtype | Remarks | Reference |
|---|---|---|---|---|---|---|---|
| A cohort study | Periodontal disease | 71 adults | 4 years | Finland | Ischemic stroke | An association between poor oral health and acute ischemic stroke. Most patients had poor oral health and had 19.0 teeth left on median | [123] |
| A cohort study | Periodontal disease | 5958 adults | 17 years | US | Ischemic stroke | An independent association between severe periodontal disease and stroke | [124] |
| A retrospective cohort study | Periodontal disease | 298,128 adults | 10 years | Korea | - | Severe periodontal disease increased total stroke by 1.4% | [125] |
| A cohort study | Periodontal disease | 15,792 adults with the age of 45–64 | 15 years | US | Cardioembolic and thrombotic stroke | Periodontal disease was significantly associated with cardioembolic and thrombotic stroke subtypes | [30] |
| A meta-analysis of cohort studies | Periodontitis, gingivitis, and tooth loss | - | - | - | Fatal or non-fatal, ischemic or hemorrhagic | Both periodontitis (relative risk 1.63) and tooth loss (relative risk 1.39) were associated with the stroke risk | [126] |
| A case-control study | Periodontitis and gingivitis | 771 adults | - | Germany | Cerebral ischemia | Periodontitis was found to be an independent risk factor only in younger patients and men | [102] |
| A prospective cohort study | Severe periodontal disease | 807 adults aged ≥40 years | 4 years | Latin America | - | A direct but modest association between periodontal disease and stroke | [127] |
| A cohort study | Periodontal disease and tooth loss | 3389 adults over 40 years of age | - | Korea | - | Loss of tooth due to periodontal disease is a risk factor for stroke. The stroke risk was 2.17 times higher in the group with less than 19 remaining teeth | [128] |
| A cohort study | Periodontal disease and tooth loss | 41, 380 adults | 4 years | US | Ischemic stroke | A modest association was found between baseline periodontal disease history and stroke. Men with ≤24 teeth at baseline were at a higher risk of stroke compared to men with ≥25 teeth | [75] |
| A cohort study | Number of dental caries and tooth loss | 206,602 adults | 10.4 years | Korea | Cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage | Regular oral hygiene behavior was negatively and number of dental caries was positively associated with stroke occurrence | [71] |
| A dose-response meta-analysis study | Tooth loss | - | Updated to April 2017 | - | - | A significant dose-response association between tooth loss and stroke risk | [129] |
| A review study | Tooth loss | - | 10 years | - | - | A relationship between early tooth loss and the stroke occurrence | [130] |
| A cross-sectional study | Tooth loss | 410,939 adults | 4 years | US | Cerebral vascular accidents, cerebral infarctions, and cerebrovascular ischemia | Tooth loss had a potential association as an independent factor in the stroke incidence | [131] |
| A national, population-based, longitudinal study | Tooth loss | 24,393 black and white adults aged 45 years and over | 10 years | US | Stroke mortality | Tooth loss was positively associated with C-reactive protein, white blood cell count, and stroke/TIA | [132] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shahi, S.; Farhoudi, M.; Dizaj, S.M.; Sharifi, S.; Sadigh-Eteghad, S.; Goh, K.W.; Ming, L.C.; Dhaliwal, J.S.; Salatin, S. The Link between Stroke Risk and Orodental Status—A Comprehensive Review. J. Clin. Med. 2022, 11, 5854. https://doi.org/10.3390/jcm11195854
Shahi S, Farhoudi M, Dizaj SM, Sharifi S, Sadigh-Eteghad S, Goh KW, Ming LC, Dhaliwal JS, Salatin S. The Link between Stroke Risk and Orodental Status—A Comprehensive Review. Journal of Clinical Medicine. 2022; 11(19):5854. https://doi.org/10.3390/jcm11195854
Chicago/Turabian StyleShahi, Shahriar, Mehdi Farhoudi, Solmaz Maleki Dizaj, Simin Sharifi, Saeed Sadigh-Eteghad, Khang Wen Goh, Long Chiau Ming, Jagjit Singh Dhaliwal, and Sara Salatin. 2022. "The Link between Stroke Risk and Orodental Status—A Comprehensive Review" Journal of Clinical Medicine 11, no. 19: 5854. https://doi.org/10.3390/jcm11195854
APA StyleShahi, S., Farhoudi, M., Dizaj, S. M., Sharifi, S., Sadigh-Eteghad, S., Goh, K. W., Ming, L. C., Dhaliwal, J. S., & Salatin, S. (2022). The Link between Stroke Risk and Orodental Status—A Comprehensive Review. Journal of Clinical Medicine, 11(19), 5854. https://doi.org/10.3390/jcm11195854