
Troponin in COVID-19: To Measure or Not to Measure? Insights from a Prospective Cohort Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Design
2.2. Outcomes
2.3. Statistical Analysis
3. Results
3.1. Primary Outcome—In-Hospital Mortality
3.2. Secondary Outcomes
3.3. Multivariate Analysis Results
3.4. Predictive Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Majure, D.T.; Gruberg, L.; Saba, S.G.; Kvasnovsky, C.; Hirsch, J.S.; Jauhar, R.; Northwell Health COVID-19 Research Consortium. Usefulness of elevated troponin to predict death in patients with COVID-19 and myocardial injury. Am. J. Cardiol. 2021, 138, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Aikawa, T.; Takagi, H.; Ishikawa, K.; Kuno, T. Myocardial injury characterized by elevated cardiac troponin and in-hospital mortality of COVID-19: An insight from a meta-analysis. J. Med. Virol. 2021, 93, 51. [Google Scholar] [CrossRef]
- Metkus, T.S.; Sokoll, L.J.; Barth, A.S.; Czarny, M.J.; Hays, A.G.; Lowenstein, C.J.; Michos, E.D.; Nolley, E.P.; Post, W.S.; Resar, J.R. Myocardial injury in severe COVID-19 compared with non-COVID-19 acute respiratory distress syndrome. Circulation 2021, 143, 553–565. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Moll-Bernardes, R.; De Sousa, A.S.; Macedo, A.V.S.; Lopes, R.D.; Vera, N.; Maia, L.C.R.; Feldman, A.; Arruda, G.; Castro, M.J.C.; Pimentel-Coelho, P.M. IL-10 and IL-12 (P70) levels predict the risk of COVID-19 progression in hypertensive patients: Insights from the BRACE-CORONA trial. Front. Cardiovasc. Med. 2021, 8, 702507. [Google Scholar] [CrossRef]
- Moll-Bernardes, R.; Fortier, S.C.; Sousa, A.S.; Lopes, R.D.; Vera, N.; Conde, L.; Feldman, A.; Arruda, G.; Cabral-Castro, M.; Albuquerque, D.C.; et al. NKG2A expression among CD8 cells is associated with COVID-19 progression in hypertensive patients: Insights from the BRACE CORONA randomized trial. J. Clin. Med. 2022, 11, 3713. [Google Scholar] [CrossRef]
- Mancia, G.; Rea, F.; Ludergnani, M.; Apolone, G.; Corrao, G. Renin–angiotensin–aldosterone system blockers and the risk of COVID-19. N. Engl. J. Med. 2020, 382, 2431–2440. [Google Scholar] [CrossRef]
- Lopes, R.D.; Macedo, A.V.S.; de Barros, E.S.P.G.M.; Moll-Bernardes, R.J.; Dos Santos, T.M.; Mazza, L.; Feldman, A.; D’Andrea Saba Arruda, G.; de Albuquerque, D.C.; Camiletti, A.S.; et al. Effect of discontinuing vs continuing angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on days alive and out of the hospital in patients admitted with COVID-19: A randomized clinical trial. JAMA 2021, 325, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Gagno, G.; Sinagra, G.; Beltrami, A.P.; Janjusevic, M.; Ippolito, G.; Zumla, A.; Fluca, A.L.; Ferro, F. Effects of SARS-CoV-2 on cardiovascular system: The dual role of angiotensin-converting enzyme 2 (ACE2) as the virus receptor and homeostasis regulator-review. Int. J. Mol. Sci. 2021, 22, 4526. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhu, L.; Cai, J.; Lei, F.; Qin, J.-J.; Xie, J.; Liu, Y.-M.; Zhao, Y.-C.; Huang, X.; Lin, L. Association of inpatient use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ. Res. 2020, 126, 1671–1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, R.D.; Macedo, A.V.S.; de Barros, E.S.P.G.M.; Moll-Bernardes, R.J.; Feldman, A.; D’Andrea Saba Arruda, G.; de Souza, A.S.; de Albuquerque, D.C.; Mazza, L.; Santos, M.F.; et al. Continuing versus suspending angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: Impact on adverse outcomes in hospitalized patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)—The BRACE CORONA trial. Am. Heart J. 2020, 226, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Omland, T.; Prebensen, C.; Roysland, R.; Sovik, S.; Sorensen, V.; Rosjo, H.; Svensson, M.; Berdal, J.E.; Myhre, P.L. Established cardiovascular biomarkers provide limited prognostic information in unselected patients hospitalized with COVID-19. Circulation 2020, 142, 1878–1880. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Montalto, C.; Pagnesi, M.; Lupi, L.; Cappelletti, A.; Baldetti, L.; Baldi, E.; Lombardi, C.; Metra, M.; Perlini, S.; et al. High troponin levels in patients hospitalized for coronavirus disease 2019: A maker or a marker of prognosis? J. Cardiovasc. Med. 2021, 22, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J. Troponin and BNP use in COVID-19. Cardiol. Mag. 2020, 18. Available online: https://www.acc.org/latest-in-cardiology/articles/2020/03/18/15/25/troponin-and-bnp-use-in-covid19 (accessed on 21 August 2022).
- Baigent, C.; Windecker, S.; Andreini, D.; Arbelo, E.; Barbato, E.; Bartorelli, A.L.; Baumbach, A.; Behr, E.R.; Berti, S.; Bueno, H. ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 2—Care pathways, treatment, and follow-up. Cardiovasc. Res. 2022, 43, 1059–1103. [Google Scholar]
- Zwaenepoel, B.; Dhont, S.; Schaubroeck, H.; Gevaert, S. The use of cardiac troponins and B-type natriuretic peptide in COVID-19. Acta Cardiol. 2021; 1–6, online ahead of print. [Google Scholar] [CrossRef]
- Akhvlediani, T.; Ali, S.M.; Angus, D.C.; Arabi, Y.M.; Ashraf, S.; Baillie, J.K.; Bakamutumaho, B.; Beane, A.; Bozza, F.; Brett, S.J. Global outbreak research: Harmony not hegemony. Lancet Infect. Dis. 2020, 20, 770–772. [Google Scholar] [CrossRef]
- Chapman, A.R.; Bularga, A.; Mills, N.L. High-sensitivity cardiac troponin can be an ally in the fight against COVID-19. Circulation 2020, 141, 1733–1735. [Google Scholar] [CrossRef]
- Sandoval, Y.; Januzzi, J.L., Jr.; Jaffe, A.S. Cardiac troponin for assessment of myocardial injury in COVID-19: JACC review topic of the week. J. Am. Coll. Cardiol. 2020, 76, 1244–1258. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.G.; Cooper, L.T., Jr. What we (don’t) know about myocardial injury after COVID-19. Eur. Heart J. 2021, 42, 1879–1882. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Measured Troponin | χ2 Test p-Value | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| n | (%) | n | (%) | n | (%) | ||
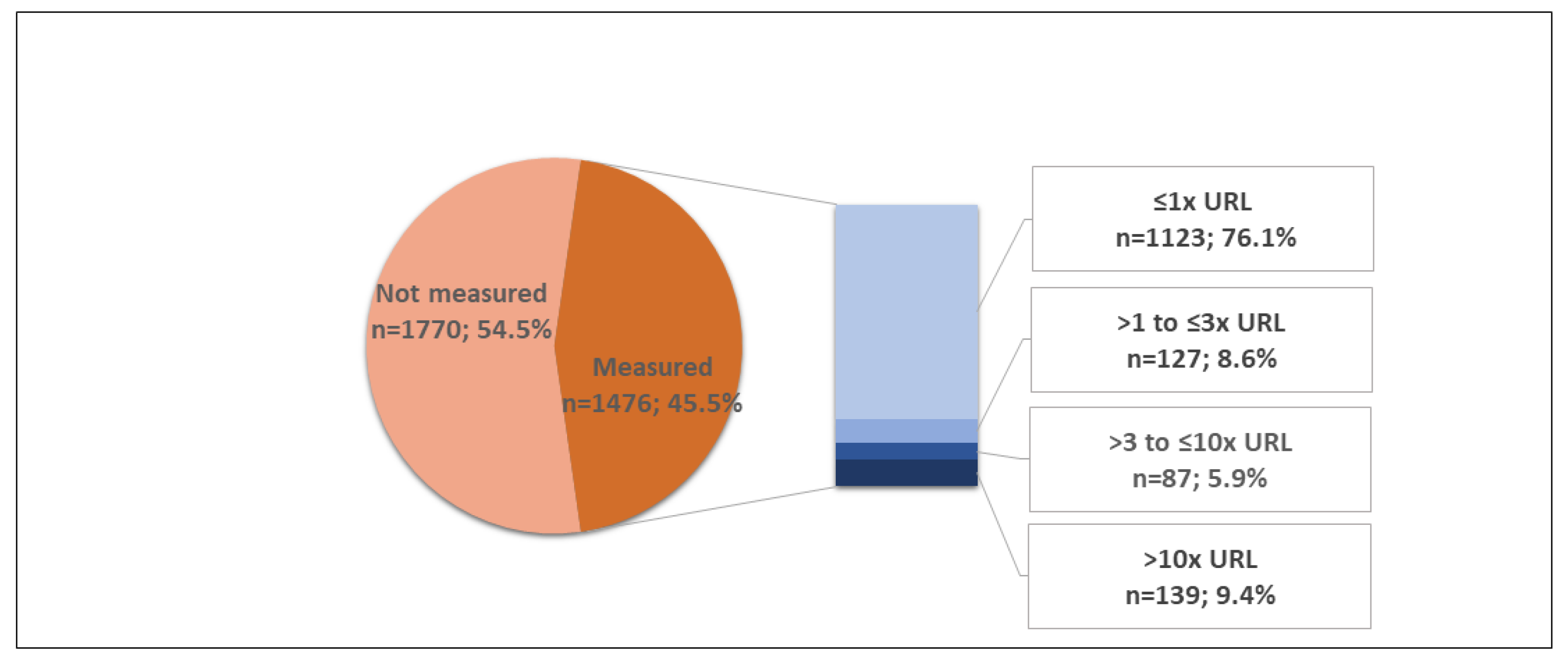
| All patients | 3246 | (100.0) | 1770 | (54.5) | 1476 | (45.5) | |
| Sex | |||||||
| Male | 1935 | (59.6) | 1040 | (53.7) | 895 | (46.3) | 0.277 |
| Female | 1311 | (40.4) | 730 | (55.7) | 581 | (44.3) | |
| Age (years) | |||||||
| <40 | 603 | (18.6) | 349 | (57.9) | 254 | (42.1) | 0.140 |
| 40–59 | 1357 | (41.8) | 748 | (55.1) | 609 | (44.9) | |
| 60–69 | 541 | (16.7) | 281 | (51.9) | 260 | (48.1) | |
| ≥70 | 745 | (23.0) | 392 | (52.6) | 353 | (47.4) | |
| O2 saturation | |||||||
| >93% | 2327 | (71.7) | 1272 | (54.7) | 1055 | (45.3) | 0.807 |
| ≤93% | 919 | (28.3) | 498 | (54.2) | 421 | (45.8) | |
| Diabetes | |||||||
| No | 2434 | (75.0) | 1331 | (54.7) | 1103 | (45.3) | 0.759 |
| Yes | 812 | (25.0) | 439 | (54.1) | 373 | (45.9) | |
| Hypertension | |||||||
| No | 1403 | (43.2) | 789 | (56.2) | 614 | (43.8) | 0.088 |
| Yes | 1843 | (56.8) | 981 | (53.2) | 862 | (46.8) | |
| Heart failure | |||||||
| No | 3145 | (96.9) | 1717 | (54.6) | 1428 | (45.4) | 0.674 |
| Yes | 101 | (3.1) | 53 | (52.5) | 48 | (47.5) | |
| Coronary disease | |||||||
| No | 3029 | (93.3) | 1666 | (55.0) | 1363 | (45.0) | 0.043 |
| Yes | 217 | (6.7) | 104 | (47.9) | 113 | (52.1) | |
| Chronic heart disease | |||||||
| No | 3079 | (94.9) | 1695 | (55.1) | 1384 | (44.9) | 0.010 |
| Yes | 167 | (5.1) | 75 | (44.9) | 92 | (55.1) | |
| Chronic Kidney disease | |||||||
| No | 3094 | (95.3) | 1676 | (54.2) | 1418 | (45.8) | 0.064 |
| Yes | 152 | (4.7) | 94 | (61.8) | 58 | (38.2) | |
| Thromboembolic phenomena * | |||||||
| No | 3126 | (96.3) | 1693 | (54.2) | 1433 | (45.8) | 0.031 |
| Yes | 120 | (3.7) | 77 | (64.2) | 43 | (35.8) | |
| Stroke or TIA | |||||||
| No | 3154 | (97.2) | 1723 | (54.6) | 1431 | (45.4) | 0.501 |
| Yes | 92 | (2.8) | 47 | (51.1) | 45 | (48.9) | |
| Myopericarditis | |||||||
| No | 3201 | (98.6) | 1755 | (54.8) | 1446 | (45.2) | 0.004 |
| Yes | 45 | (1.4) | 15 | (33.3) | 30 | (66.7) | |
| Myocardial ischemia ** | |||||||
| No | 3174 | (97) | 1746 | (55.0) | 1428 | (45.0) | <0.001 |
| Yes | 72 | (3.0) | 24 | (33.3) | 48 | (66.7) | |
| Acute renal failure | |||||||
| No | 2866 | (88.3) | 1550 | (54.1) | 1316 | (45.9) | 0.161 |
| Yes | 380 | (11.7) | 220 | (57.9) | 160 | (42.1) | |
| Sepsis or septic shock | |||||||
| No | 2907 | (89.6) | 1605 | (55.2) | 1302 | (44.8) | 0.022 |
| Yes | 339 | (10.4) | 165 | (48.7) | 174 | (51.3) | |
| Invasive ventilation | |||||||
| No | 2625 | (80.9) | 1399 | (53.3) | 1226 | (46.7) | 0.004 |
| Yes | 621 | (19.1) | 371 | (59.7) | 250 | (40.3) | |
| Death | |||||||
| No | 2893 | (89.1) | 1559 | (53.9) | 1334 | (46.1) | 0.036 |
| Yes | 353 | (10.9) | 211 | (59.8) | 142 | (40.2) | |
| Characteristics | Frequencies n (%) | Prevalence of Myocardial Injury * | Prevalence Ratio (95% CI) | χ2 Test p-Value |
|---|---|---|---|---|
| Patients with measured troponin | 1476 (100) | 23.9% | ||
| Sex | ||||
| Male | 895 (60.6) | 25.5% | 1.2 (0.97, 1.43) | 0.081 |
| Female | 581 (39.4) | 21.5% | 1 | |
| Age | ||||
| <40 years | 254 (17.2) | 7.5% | 1 | <0.001 |
| 40 to 59 years | 609 (41.3) | 14.0% | 1.9 (1.16, 3.00) | |
| 60 to 69 years | 260 (17.6) | 33.1% | 4.4 (2.77, 7.04) | |
| ≥70 years | 353 (23.9) | 46.2% | 6.2 (3.95, 9.65) | |
| Oxygen saturation | ||||
| ≥94% | 1055 (71.5) | 21.1% | 1 | <0.001 |
| ≤93% | 421 (28.5) | 30.9% | 1.5 (1.21, 1.76) | |
| Diabetes | ||||
| No | 1103 (74.7) | 21.2% | 1 | <0.001 |
| Yes | 373 (25.3) | 31.9% | 1.5 (1.25, 1.81) | |
| Hypertension | ||||
| No | 614 (41.6) | 14.3% | 1 | <0.001 |
| Yes | 862 (58.4) | 30.7% | 2.1(1.72, 2.66) | |
| Heart failure | ||||
| No | 1428 (96.7) | 22.8% | 1 | <0.001 |
| Yes | 48 (3.3) | 58.3% | 2.6 (1.97, 3.30) | |
| Coronary artery disease | ||||
| No | 1363 (92.3) | 22.2% | 1 | <0.001 |
| Yes | 113 (7.7) | 44.2% | 2.0 (1.58, 2.50) | |
| Chronic heart disease | ||||
| No | 1384 (93.8) | 22.3% | 1 | <0.001 |
| Yes | 92 (6.2) | 47.8% | 2.1 (1.69, 2.71) | |
| Chronic kidney disease | ||||
| No | 1418 (96.1) | 22.8% | 1 | <0.001 |
| Yes | 58 (3.9) | 50.0% | 2.2 (1.67, 2.89) |
| Characteristics | In-Hospital Mortality | Relative Risk (RR) (95% CI) | χ2 Test p-Value |
|---|---|---|---|
| Troponin (×URL) | |||
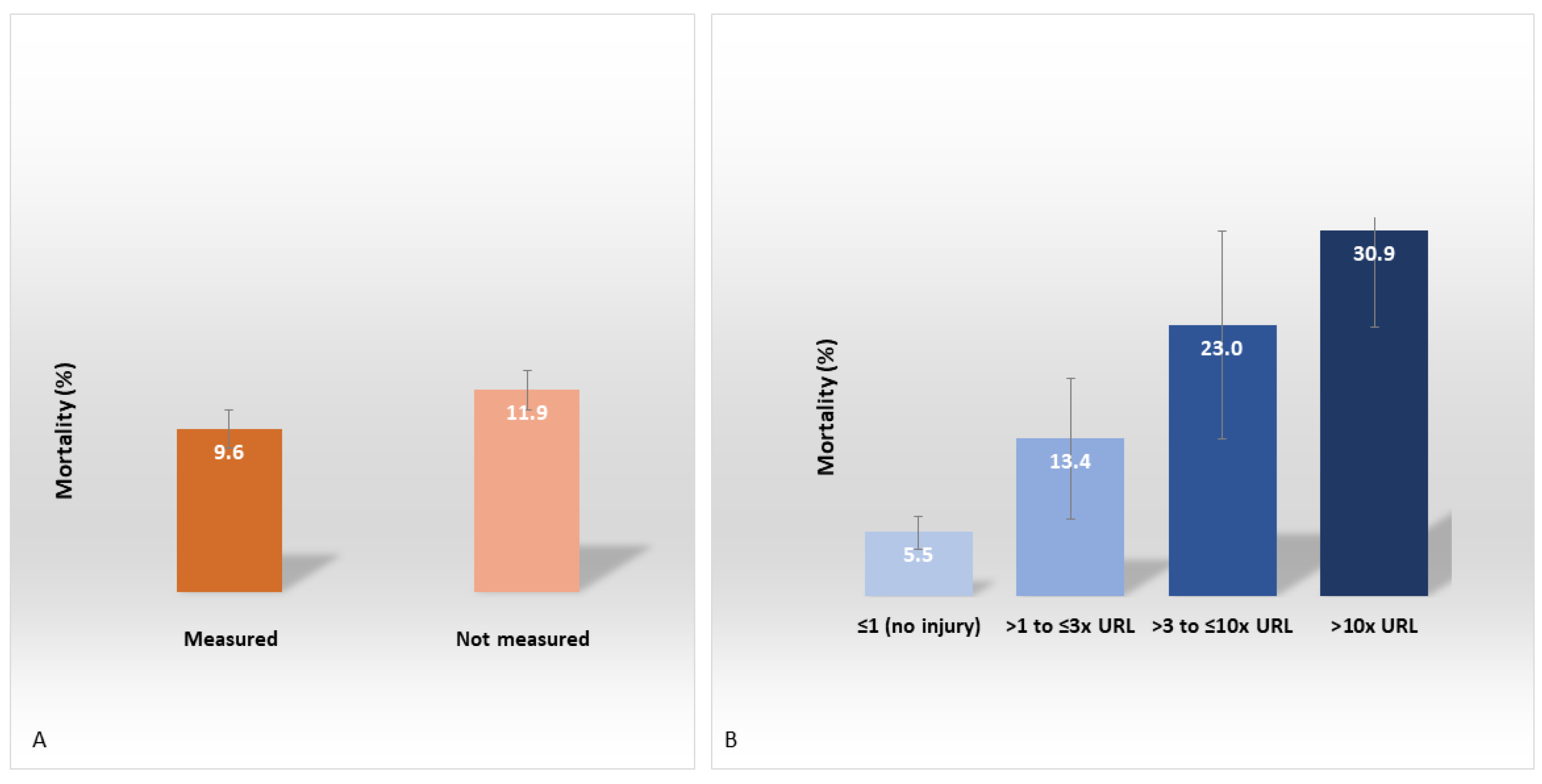
| ≤1 (negative) | 5.5% | 1 | <0.001 |
| >1 (myocardial injury) | 22.7% | 4.1 (3.01, 5.59) | |
| Not measured | 11.9% | 2.2 (1.64, 2.84) | |
| Sex | |||
| Male | 11.2% | 1.1 (0.87, 1.30) | 0.522 |
| Female | 10.5% | 1 | |
| Age | |||
| <40 years | 2.5% | 1 | <0.001 |
| 40–59 years | 6.3% | 2.5 (1.47, 4.32) | |
| 60–69 years | 12.6% | 5.0 (2.92, 8.73) | |
| ≥70 years | 24.8% | 9.9 (5.96, 16.71) | |
| Oxygen saturation | |||
| >93% | 7.9% | 1 | <0.001 |
| ≤93% | 18.5% | 2.3 (1.94, 2.86) | |
| Diabetes | |||
| No | 8.8% | 1 | <0.001 |
| Yes | 17.1% | 1.9 (1.59, 2.37) | |
| Hypertension | |||
| No | 7.8% | 1 | <0.001 |
| Yes | 13.2% | 1.7 (1.37, 2.11) | |
| Heart failure | |||
| No | 10.4% | 1 | <0.001 |
| Yes | 24.8% | 2.4 (1.66, 3.38) | |
| Coronary artery disease | |||
| No | 10.4% | 1 | 0.001 |
| Yes | 17.5% | 1.7 (1.24, 2.29) | |
| Chronic heart disease | |||
| No | 10.4% | 1 | <0.001 |
| Yes | 20.4% | 2.0 (1.43, 2.70) | |
| Chronic kidney disease | |||
| No | 10.2% | 1 | <0.001 |
| Yes | 25.0% | 2.5 (1.83, 3.30) | |
| Total | 10.9% |
| Characteristics | Multiple Logistic Model | Final Logistic Model | |||
|---|---|---|---|---|---|
| aOR | p-Value | aOR | 95% CI | p-Value | |
| Troponin (×URL) | <0.001 | <0.001 | |||
| ≤1 (negative) | 1 | 1 | |||
| >1 (myocardial injury) | 2.95 | <0.001 | 2.99 | 2.06–4.36 | <0.001 |
| Not measured | 2.17 | <0.001 | 2.20 | 1.62–2.97 | <0.001 |
| Sex | |||||
| Male | 1.20 | 0.149 | |||
| Female | 1 | ||||
| Age (years) | <0.001 | <0.001 | |||
| <40 | 1 | 1 | |||
| 40–59 | 2.40 | 0.003 | 2.32 | 1.3 –4.07 | 0.003 |
| 60–69 | 4.36 | <0.001 | 4.12 | 2.29–7.39 | <0.001 |
| ≥70 | 9.64 | <0.001 | 9.07 | 5.22–15.75 | <0.001 |
| Oxygen saturation (%) | |||||
| >93 | 1 | 1 | |||
| ≤93 | 2.17 | <0.001 | 2.17 | 1.71–2.75 | < 0.001 |
| Diabetes | |||||
| No | 1 | 1 | |||
| Yes | 1.37 | 0.018 | 1.35 | 1.05–1.73 | 0.018 |
| Hypertension | |||||
| No | 1 | ||||
| Yes | 0.85 | 0.260 | |||
| Heart failure | |||||
| No | 1 | ||||
| Yes | 1.18 | 0.557 | |||
| Coronary disease | |||||
| No | 1 | ||||
| Yes | 0.80 | 0.296 | |||
| Chronic heart disease | |||||
| No | 1 | ||||
| Yes | 1.19 | 0.467 | |||
| Kidney disease | |||||
| No | 1 | ||||
| Yes | 1.39 | 0.128 | |||
| Age (Years) | Diabetes | O2 Sat | Troponin | ||
|---|---|---|---|---|---|
| ≤1 × URL (No Injury) | >1 × URL (Injury *) | Not Measured | |||
| <40 | No | >93% | 1.2% | 3.4% | 2.5% |
| ≤93% | 2.5% | 7.1% | 5.3% | ||
| Yes | >93% | 1.6% | 4.3% | 3.4% | |
| ≤93% | 3.3% | 9.3% | 7.0% | ||
| 40–59 | No | >93% | 2.6% | 7.5% | 5.6% |
| ≤93% | 5.6% | 15.0% | 11.5% | ||
| Yes | >93% | 3.5% | 9.9% | 7.4% | |
| ≤93% | 7.4% | 19.2% | 14.9% | ||
| 60–69 | No | >93% | 4.6% | 12.6% | 9.6% |
| ≤93% | 9.5% | 23.8% | 18.7% | ||
| Yes | >93% | 6.1% | 16.3% | 12.5% | |
| ≤93% | 12.4% | 29.7% | 23.7% | ||
| ≥70 | No | >93% | 9.6% | 24.1% | 18.9% |
| ≤93% | 18.7% | 40.8% | 33.6% | ||
| Yes | >93% | 12.5% | 30.0% | 23.9% | |
| ≤93% | 23.7% | 48.2% | 40.6% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moll-Bernardes, R.; Mattos, J.D.; Schaustz, E.B.; Sousa, A.S.; Ferreira, J.R.; Tortelly, M.B.; Pimentel, A.M.L.; Figueiredo, A.C.B.S.; Noya-Rabelo, M.M.; Sales, A.R.K.; et al. Troponin in COVID-19: To Measure or Not to Measure? Insights from a Prospective Cohort Study. J. Clin. Med. 2022, 11, 5951. https://doi.org/10.3390/jcm11195951
Moll-Bernardes R, Mattos JD, Schaustz EB, Sousa AS, Ferreira JR, Tortelly MB, Pimentel AML, Figueiredo ACBS, Noya-Rabelo MM, Sales ARK, et al. Troponin in COVID-19: To Measure or Not to Measure? Insights from a Prospective Cohort Study. Journal of Clinical Medicine. 2022; 11(19):5951. https://doi.org/10.3390/jcm11195951
Chicago/Turabian StyleMoll-Bernardes, Renata, João D. Mattos, Eduardo B. Schaustz, Andréa S. Sousa, Juliana R. Ferreira, Mariana B. Tortelly, Adriana M. L. Pimentel, Ana Cristina B. S. Figueiredo, Marcia M. Noya-Rabelo, Allan R. K. Sales, and et al. 2022. "Troponin in COVID-19: To Measure or Not to Measure? Insights from a Prospective Cohort Study" Journal of Clinical Medicine 11, no. 19: 5951. https://doi.org/10.3390/jcm11195951
APA StyleMoll-Bernardes, R., Mattos, J. D., Schaustz, E. B., Sousa, A. S., Ferreira, J. R., Tortelly, M. B., Pimentel, A. M. L., Figueiredo, A. C. B. S., Noya-Rabelo, M. M., Sales, A. R. K., Albuquerque, D. C., Rosado-de-Castro, P. H., Camargo, G. C., Souza, O. F., Bozza, F. A., Medei, E., & Luiz, R. R. (2022). Troponin in COVID-19: To Measure or Not to Measure? Insights from a Prospective Cohort Study. Journal of Clinical Medicine, 11(19), 5951. https://doi.org/10.3390/jcm11195951