

Challenges in the Management of the Patient with a Failing Kidney Graft: A Narrative Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Management of the Failing Allograft
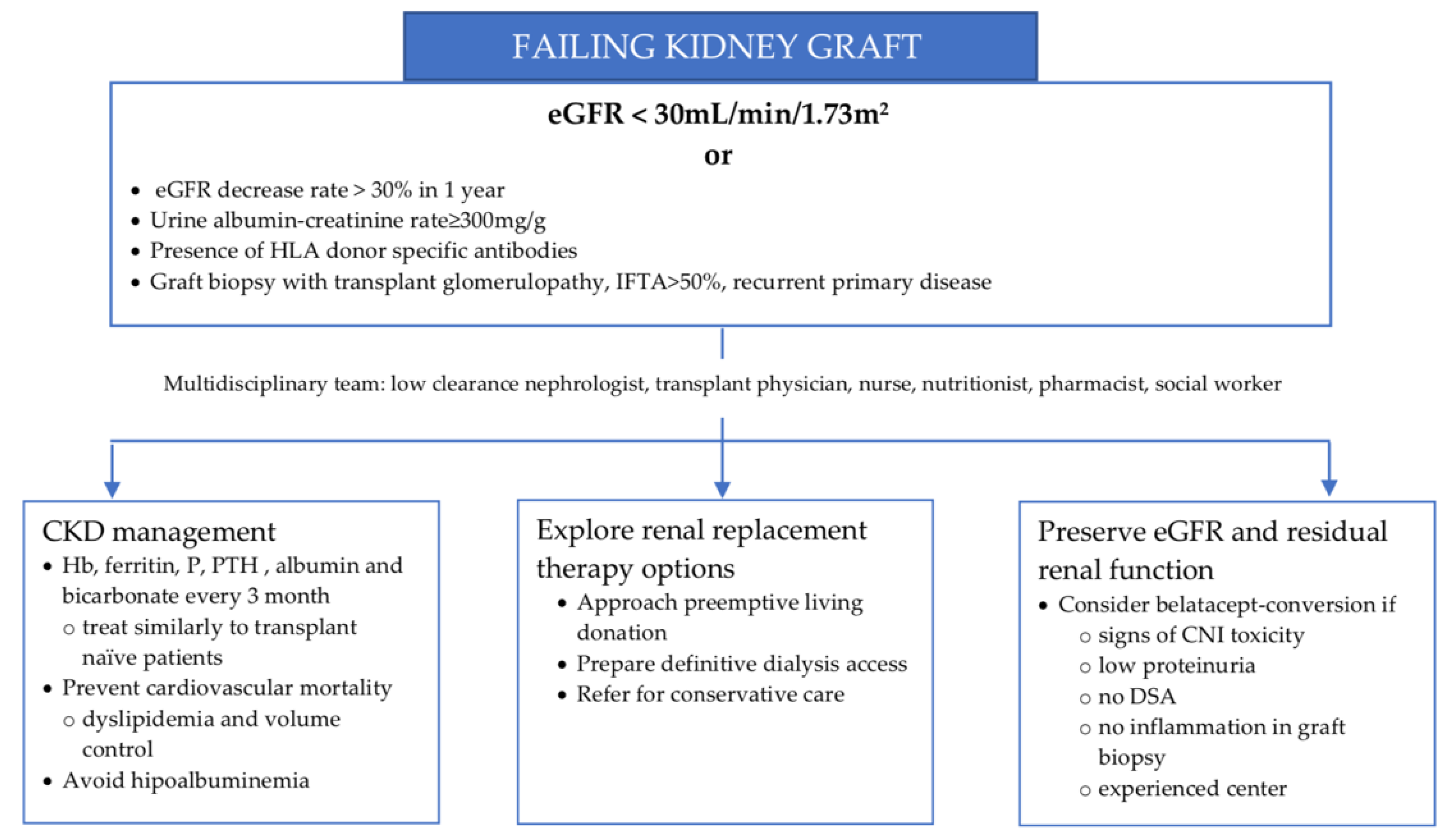
3.1. Definition of a Failing Allograft
3.2. Chronic Kidney Disease Management
3.3. Individualized Care to a Patient with a Failing Allograft and Strategies to Defer Dialysis
3.4. Dialysis Timing, Modality and Conservative Care
3.5. Immunosuppression Withdrawal
3.6. Graft Nephrectomy
3.7. Relisting for a Subsequent Kidney Transplant
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| CKD | chronic kidney disease |
| CKD-MBD | chronic kidney disease associated mineral bone disorder |
| CNI | calcineurin inhibitor |
| cPRA | calculated panel reactive antibody |
| DSA | donor specific antibody |
| ESA | erythropoiesis stimulating agents |
| GFR | glomerular filtration rate |
| GIS | graft intolerance syndrome |
| HD | hemodialysis |
| IS | immunosuppression |
| KDIGO | kidney disease improving global outcomes |
| KT | kidney transplant |
| KRAFT | the kidney recipient with allograft failure transition of care |
| PD | peritoneal dialysis |
| PRA | panel reactive antibody |
| RCT | randomized clinical trial |
References
- Coemans, M.; Süsal, C.; Döhler, B.; Anglicheau, D.; Giral, M.; Bestard, O.; Legendre, C.; Emonds, M.-P.; Kuypers, D.; Molenberghs, G.; et al. Analyses of the short- and long-term graft survival after kidney transplantation in Europe between 1986 and 2015. Kidney Int. 2018, 94, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Boenink, R.; Astley, M.E.; Huijben, J.A.; Stel, V.S.; Kerschbaum, J.; Ots-Rosenberg, M.; Åsberg, A.A.; Lopot, F.; Golan, E.; De la Nuez, P.C.; et al. The ERA Registry Annual Report 2019: Summary and age comparisons. Clin. Kidney J. 2022, 15, 452–472. [Google Scholar] [CrossRef]
- Lentine, K.L.; Smith, J.M.; Hart, A.; Miller, J.; Skeans, M.A.; Larkin, L.; Robinson, A.; Gauntt, K.; Israni, A.K.; Hirose, R.; et al. OPTN/SRTR 2020 Annual Data Report: Kidney. Am. J. Transplant. 2022, 22 (Suppl. 2), 21–136. [Google Scholar] [CrossRef] [PubMed]
- Brar, A.; Markell, M.; Stefanov, D.G.; Timpo, E.; Jindal, R.M.; Nee, R.; Sumrani, N.; John, D.; Tedla, F.; Salifu, M.O. Mortality after Renal Allograft Failure and Return to Dialysis. Am. J. Nephrol. 2017, 45, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Perl, J.; Hasan, O.; Bargman, J.M.; Jiang, D.; Na, Y.; Gill, J.S.; Jassal, S.V. Impact of Dialysis Modality on Survival after Kidney Transplant Failure. Clin. J. Am. Soc. Nephrol. 2011, 6, 582–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Management of the Failing Kidney Transplant British Transplantation Society Guidelines. 2014. Available online: https://bts.org.uk/wp-content/uploads/2016/09/13_BTS_Failing_Graft-1.pdf (accessed on 1 May 2022).
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO clinical practice guideline for the care of kidney transplant recipients Chapter 6: Treatment of Acute Rejection. Am. J. Transplant. 2009, 9 (Suppl. 3), S21–S22. [Google Scholar]
- Pottel, H.; Delay, A.; Maillard, N.; Mariat, C.; Delanaye, P. 20-year longitudinal follow-up of measured and estimated glomerular filtration rate in kidney transplant patients. Clin. Kidney J. 2021, 14, 909–916. [Google Scholar] [CrossRef]
- Clayton, P.A.; Lim, W.H.; Wong, G.; Chadban, S.J. Relationship between eGFR Decline and Hard Outcomes after Kidney Transplants. J. Am. Soc. Nephrol. 2016, 27, 3440–3446. [Google Scholar] [CrossRef] [Green Version]
- McCaughan, J.A.; Courtney, A.E.; Maxwell, A.P. Estimated Glomerular Filtration Rate Decline as a Predictor of Dialysis in Kidney Transplant Recipients. Am. J. Nephrol. 2014, 39, 297–305. [Google Scholar] [CrossRef]
- Lima, S.L.; Miranda, D.M.; Rinne, A.G.; Mena, N.N.; Tamajón, L.P.; Rodríguez, A.; González, A.A.; Delgado, A.G.; Moure, C.F.; Rinne, F.G.; et al. Estimated GFR Slope in Kidney Transplant Patients: When the Error Is Random. Transplantation 2022, 106, 391–400. [Google Scholar] [CrossRef]
- Diena, D.; Messina, M.; De Biase, C.; Fop, F.; Scardino, E.; Rossetti, M.M.; Barreca, A.; Verri, A.; Biancone, L. Relationship between early proteinuria and long term outcome of kidney transplanted patients from different decades of donor age. BMC Nephrol. 2019, 20, 443. [Google Scholar] [CrossRef]
- Molnar, M.Z.; Ojo, A.O.; Bunnapradist, S.; Kovesdy, C.P.; Kalantar-Zadeh, K. Timing of dialysis initiation in transplant-naive and failed transplant patients. Nat. Rev. Nephrol. 2012, 8, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Tangri, N.; Ferguson, T.W.; Wiebe, C.; Eng, F.; Nash, M.; Astor, B.C.; Lam, N.; Ye, F.; Shin, J.-I.; Whitlock, R.; et al. Validation of the Kidney Failure Risk Equation in Kidney Transplant Recipients. Can. J. Kidney Health Dis. 2020, 25, 7. [Google Scholar] [CrossRef]
- Akbari, S.; Knoll, G.; White, C.; Kumar, T.; Fairhead, T.; Akbari, A. Accuracy of Kidney Failure Risk Equation in Transplant Recipients. Kidney Int. Rep. 2019, 4, 1334–1337. [Google Scholar] [CrossRef] [Green Version]
- Mayrdorfer, M.; Liefeldt, L.; Wu, K.; Rudolph, B.; Zhang, Q.; Friedersdorff, F.; Lachmann, N.; Schmidt, D.; Osmanodja, B.; Naik, M.G.; et al. Exploring the Complexity of Death-Censored Kidney Allograft Failure. J. Am. Soc. Nephrol. 2021, 32, 1513–1526. [Google Scholar] [CrossRef]
- Sellarés, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef]
- Van Loon, E.; Bernards, J.; Van Craenenbroeck, A.H.; Naesens, M. The causes of kidney allograft failure: More than alloimmunity. A viewpoint article. Transplantation 2020, 104, E46–E56. [Google Scholar] [CrossRef]
- Lubetzky, M.; Tantisattamo, E.; Molnar, M.Z.; Lentine, K.L.; Basu, A.; Parsons, R.F.; Woodside, K.J.; Pavlakis, M.; Blosser, C.D.; Singh, N.; et al. The failing kidney allograft: A review and recommendations for the care and management of a complex group of patients. Am. J. Transplant. 2021, 21, 2937–2949. [Google Scholar] [CrossRef]
- Woo, Y.M.; Pereira, B.J.G.; Gill, J.S. Chronic kidney disease progression in native and transplant kidneys. Curr. Opin. Nephrol. Hypertens. 2004, 13, 607–611. [Google Scholar] [CrossRef]
- Ansell, D.; Udayaraj, U.P.; Steenkamp, R.; Dudley, C.R.K. Chronic Renal Failure in Kidney Transplant Recipients. Do They Receive Optimum Care?: Data from the UK Renal Registry. Am. J. Transplant. 2007, 7, 1167–1176. [Google Scholar] [CrossRef]
- Akbari, A.; Hussain, N.; Karpinski, J.; Knoll, G.A. Chronic Kidney Disease Management: Comparison between Renal Transplant Recipients and Nontransplant Patients with Chronic Kidney Disease. Nephron. Clin. Pract. 2007, 107, c7–c13. [Google Scholar] [CrossRef] [PubMed]
- Tsujita, M.; Kosugi, T.; Goto, N.; Futamura, K.; Nishihira, M.; Okada, M.; Hiramitsu, T.; Narumi, S.; Uchida, K.; Takeda, A.; et al. The effect of maintaining high hemoglobin levels on long-term kidney function in kidney transplant recipients: A randomized controlled trial. Nephrol. Dial. Transplant. 2019, 34, 1409–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obi, Y.; Ichimaru, N.; Sakaguchi, Y.; Iwadoh, K.; Ishii, D.; Sakai, K.; Iwami, D.; Harada, H.; Sumida, K.; Sekine, A.; et al. Correcting anemia and native vitamin D supplementation in kidney transplant recipients: A multicenter, 2 × 2 factorial, open-label, randomized clinical trial. Transpl. Int. 2021, 34, 1212–1225. [Google Scholar] [CrossRef] [PubMed]
- Molinari, P.; Alfieri, C.M.; Mattinzoli, D.; Campise, M.; Cervesato, A.; Malvica, S.; Favi, E.; Messa, P.; Castellano, G. Bone and Mineral Disorder in Renal Transplant Patients: Overview of Pathology, Clinical, and Therapeutic Aspects. Front. Med. 2022, 9, 821884. [Google Scholar] [CrossRef]
- Iseri, K.; Carrero, J.J.; Evans, M.; Felländer-Tsai, L.; Berg, H.E.; Runesson, B.; Stenvinkel, P.; Lindholm, B.; Qureshi, A.R. Fractures after kidney transplantation: Incidence, predictors, and association with mortality. Bone 2020, 140, 115554. [Google Scholar] [CrossRef]
- Ferreira, A.C.; Mendes, M.; Silva, C.; Cotovio, P.; Aires, I.; Navarro, D.; Caeiro, F.; Ramos, R.; Salvador, R.; Correia, B.; et al. Improvement of Mineral and Bone Disorders After Renal Transplantation. Transplantation 2022, 106, e251–e261. [Google Scholar] [CrossRef]
- Lehmann, G.; Ott, U.; Stein, G.; Steiner, T.; Wolf, G. Renal Osteodystrophy After Successful Renal Transplantation: A Histomorphometric Analysis in 57 Patients. Transplant. Proc. 2007, 39, 3153–3158. [Google Scholar] [CrossRef]
- Evenepoel, P.; Claes, K.; Meijers, B.; Laurent, M.; Bammens, B.; Naesens, M.; Sprangers, B.; Cavalier, E.; Kuypers, D. Natural history of mineral metabolism, bone turnover and bone mineral density in de novo renal transplant recipients treated with a steroid minimization immunosuppressive protocol. Nephrol. Dial. Transplant. 2020, 35, 697–705. [Google Scholar] [CrossRef]
- Indd, K. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- Dawoud, D.; Harms, J.; Williams, T.; Kumar, V.; Allon, M. Predialysis Vascular Access Surgery in Patients with Failing Kidney Transplants. Am. J. Kidney Dis. 2013, 62, 398–400. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.R.; Oza-Gajera, B.; Chapla, K.; Djamali, A.X.; Muth, B.L.; Turk, J.; Wakeen, M.; Yevzlin, A.S.; Astor, B.C. Initial Vascular Access Type in Patients with a Failed Renal Transplant. Clin. J. Am. Soc. Nephrol. 2014, 9, 1225–1231. [Google Scholar] [CrossRef]
- Johnston, O.; Zalunardo, N.; Rose, C.; Gill, J.S. Prevention of Sepsis during the Transition to Dialysis May Improve the Survival of Transplant Failure Patients. J. Am. Soc. Nephrol. 2007, 18, 1331–1337. [Google Scholar] [CrossRef] [Green Version]
- Solid, C.; Foley, R.; Gill, J.; Gilbertson, D.; Collins, A. Epoetin use and Kidney Disease Outcomes Quality Initiative hemoglobin targets in patients returning to dialysis with failed renal transplants. Kidney Int. 2007, 71, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Huml, A.M.; Sehgal, A.R. Hemodialysis Quality Metrics in the First Year Following a Failed Kidney Transplant. Am. J. Nephrol. 2019, 50, 161–167. [Google Scholar] [CrossRef]
- Evans, R.D.; Bekele, S.; Campbell, S.M.; Clark, S.G.; Harris, L.; Thomas, A.; Jones, G.L.; Thuraisingham, R. Assessment of a Dedicated Transplant Low Clearance Clinic and Patient Outcomes on Dialysis After Renal Allograft Loss at 2 UK Transplant Centers. Transplant. Direct 2018, 4, e352. [Google Scholar] [CrossRef]
- Arshad, A.; Jackson-Spence, F.; Sharif, A. Development and evaluation of dedicated low clearance transplant clinics for patients with failing kidney transplants. J. Ren. Care 2019, 45, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Tantisattamo, E.; Hanna, R.M.; Reddy, U.G.; Ichii, H.; Dafoe, D.C.; Danovitch, G.M.; Kalantar-Zadeh, K. Novel options for failing allograft in kidney transplanted patients to avoid or defer dialysis therapy. Curr. Opin. Nephrol. Hypertens. 2020, 29, 80–91. [Google Scholar] [CrossRef]
- Karpe, K.M.; Talaulikar, G.S.; Walters, G.D. Calcineurin inhibitor withdrawal or tapering for kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 2017, CD006750. [Google Scholar] [CrossRef]
- Leal, R.; Tsapepas, D.; Crew, R.J.; Dube, G.K.; Ratner, L.; Batal, I. Pathology of Calcineurin and Mammalian Target of Rapamycin Inhibitors in Kidney Transplantation. Kidney Int. Rep. 2018, 3, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Sawinski, D.; Trofe-Clark, J.; Leas, B.; Uhl, S.; Tuteja, S.; Kaczmarek, J.L.; French, B.; Umscheid, C.A. Calcineurin Inhibitor Minimization, Conversion, Withdrawal, and Avoidance Strategies in Renal Transplantation: A Systematic Review and Meta-Analysis. Am. J. Transplant. 2016, 16, 2117–2138. [Google Scholar] [CrossRef]
- Ponticelli, C. Can mTOR inhibitors reduce the risk of late kidney allograft failure? Transpl. Int. 2008, 21, 2–10. [Google Scholar] [CrossRef]
- Vincenti, F.; Rostaing, L.; Grinyo, J.; Rice, K.; Steinberg, S.; Gaite, L.; Moal, M.C.; Mondragon-Ramirez, G.A.; Kothari, J.; Polinsky, M.S.; et al. Belatacept and Long-Term Outcomes in Kidney Transplantation. N. Engl. J. Med. 2016, 374, 333–343. [Google Scholar] [CrossRef]
- Durrbach, A.; Pestana, J.M.; Florman, S.; Rial, M.D.C.; Rostaing, L.; Kuypers, D.; Matas, A.; Wekerle, T.; Polinsky, M.; Meier-Kriesche, H.U.; et al. Long-Term Outcomes in Belatacept- Versus Cyclosporine-Treated Recipients of Extended Criteria Donor Kidneys: Final Results From BENEFIT-EXT, a Phase III Randomized Study. Am J Transplant. 2016, 16, 3192–3201. [Google Scholar] [CrossRef] [Green Version]
- Schulte, K.; Vollmer, C.; Klasen, V.; Bräsen, J.H.; Püchel, J.; Borzikowsky, C.; Kunzendorf, U.; Feldkamp, T. Late conversion from tacrolimus to a belatacept-based immuno-suppression regime in kidney transplant recipients improves renal function, acid-base derangement and mineral-bone metabolism. J. Nephrol. 2017, 30, 607–615. [Google Scholar] [CrossRef]
- Dürr, M.; Lachmann, N.; Zukunft, B.; Schmidt, D.; Budde, K.; Brakemeier, S. Late Conversion to Belatacept After Kidney Transplantation: Outcome and Prognostic Factors. Transplant. Proc. 2017, 49, 1747–1756.e1. [Google Scholar] [CrossRef]
- Choi, M.; Bachmann, F.; Wu, K.; Lachmann, N.; Schmidt, D.; Brakemeier, S.; Duerr, M.; Kahl, A.; Eckardt, K.-U.; Budde, K.; et al. Microvascular inflammation is a risk factor in kidney transplant recipients with very late conversion from calcineurin inhibitor-based regimens to belatacept. BMC Nephrol. 2020, 21, 354. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, M.; Li, H.; Yu, P.; Yuan, L.; Hao, C.; Chen, J.; Kalantar-Zadeh, K. Association of Initial Twice-Weekly Hemodialysis Treatment with Preservation of Residual Kidney Function in ESRD Patients. Am. J. Nephrol. 2014, 40, 140–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, J.S.; Abichandani, R.; Kausz, A.T.; Pereira, B.J. Mortality after kidney transplant failure: The impact of non-immunologic factors. Kidney Int. 2002, 62, 1875–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molnar, M.Z.; Streja, E.; Kovesdy, C.P.; Hoshino, J.; Hatamizadeh, P.; Glassock, R.J.; Ojo, A.O.; Kalantar-Zadeh, K. Estimated glomerular filtration rate at reinitiation of dialysis and mortality in failed kidney transplant recipients. Nephrol. Dial. Transplant. 2012, 27, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Johnson, D.W.; Kesselhut, J.; Li, J.J.; et al. A Randomized, Controlled Trial of Early versus Late Initiation of Dialysis. N. Engl. J. Med. 2010, 363, 609–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, S.; Kadatz, M.; Gill, J.; Gill, J.S. Access to kidney transplantation after a failed first kidney transplant and associations with patient and allograft survival: An analysis of national data to inform allocation policy. Clin. J. Am. Soc. Nephrol. 2019, 14, 1228–1237. [Google Scholar] [CrossRef]
- Perl, J.; Bargman, J.M.; Davies, S.J.; Jassal, S.V. Clinical outcomes after failed renal transplantation—Does dialysis modality matter? Semin Dial. 2008, 21, 239–244. [Google Scholar] [CrossRef]
- Benomar, M.; Vachey, C.; Lobbedez, T.; Henriques, J.; Ducloux, D.; Vernerey, D.; Courivaud, C. Peritoneal dialysis after kidney transplant failure: A nationwide matched cohort study from the French Language Peritoneal Dialysis Registry (RDPLF). Nephrol. Dial. Transplant. 2019, 34, 858–863. [Google Scholar] [CrossRef] [Green Version]
- Chaudhri, S.; Thomas, A.A.; Samad, N.; Fan, S.L. Peritoneal dialysis in patients with failed kidney transplant: Single centre experience. Nephrology 2018, 23, 162–168. [Google Scholar] [CrossRef]
- Melo, A.G.J.T.; Barbosa, G.S.B.; Cortes, D.D.P.V.R.; Ribeiro, R.G.; Araujo, L.K.; Pereira, B.J.; Abensur, H.; Moysés, R.M.A.; Elias, R.M. Returning to PD after kidney transplant failure is a valuable option. Int. Urol. Nephrol. 2022, 54, 1123–1126. [Google Scholar] [CrossRef]
- Murakami, N.; Gelfand, S.L.; Sciacca, K.R.; Killeen, K.; Leiter, R.E.; Adler, J.T.; Chandraker, A.K.; Lakin, J.R. Inpatient Kidney Palliative Care for Kidney Transplant Recipients with Failing Allografts. Kidney Med. 2022, 4, 100398. [Google Scholar] [CrossRef]
- Alhamad, T.; Lubetzky, M.; Lentine, K.L.; Edusei, E.; Parsons, R.; Pavlakis, M.; Woodside, K.J.; Adey, D.; Blosser, C.D.; Concepcion, B.P.; et al. Kidney recipients with allograft failure, transition of kidney care (KRAFT): A survey of contemporary practices of transplant providers. Am. J. Transplant. 2021, 21, 3034–3042. [Google Scholar] [CrossRef]
- Augustine, J.J.; Woodside, K.J.; Padiyar, A.; Sanchez, E.Q.; Hricik, D.E.; Schulak, J.A. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation 2012, 94, 738–743. [Google Scholar] [CrossRef]
- Casey, M.J.; Wen, X.; Kayler, L.K.; Aiyer, R.; Scornik, J.C.; Meier-Kriesche, H.-U. Prolonged Immunosuppression Preserves Nonsensitization Status After Kidney Transplant Failure. Transplantation 2014, 98, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Lucisano, G.; Brookes, P.; Santos-Nunez, E.; Firmin, N.; Gunby, N.; Hassan, S.; Gueret-Wardle, A.; Herbert, P.; Papalois, V.; Willicombe, M.; et al. Allosensitization after transplant failure: The role of graft nephrectomy and immunosuppression—A retrospective study. Transpl. Int. 2019, 32, 949–959. [Google Scholar] [CrossRef]
- Smak Gregoor, P.J.; Zietse, R.; Van Saase, J.L.; Op De Hoek, C.T.; Ijzermans, J.N.; Lavrijssen, A.T.; De Jong, G.; Kramer, P.; Weimar, W. Immunosuppression should be stopped in patients with renal allograft failure. Clin. Transplant. 2001, 15, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, A.M.S.A.; McIntyre, S.; Turner, D.M.; Henderson, L.K.; Battle, R.K. The Impact of Withdrawal of Maintenance Immunosuppression and Graft Nephrectomy on HLA Sensitization and Calculated Chance of Future Transplant. Transplant. Direct 2018, 4, e409. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.; Kim, Y.C.; Moon, J.J.; Song, E.Y.; Min, S.-I.; Ha, J.; Joo, K.W.; Kim, Y.S.; Ahn, C.; Lee, H. Weaning Immunosuppressant in Patients with Failing Kidney Grafts and The Outcomes: A Single-Center Retrospective Cohort Study. Sci. Rep. 2020, 10, 6425–6429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmoliaptsis, V.; Gjorgjimajkoska, O.; Sharples, L.D.; Chaudhry, A.N.; Chatzizacharias, N.; Peacock, S.; Torpey, N.; Bolton, E.M.; Taylor, C.J.; Bradley, J.A. Impact of donor mismatches at individual HLA-A, -B, -C, -DR, and -DQ loci on the development of HLA-specific antibodies in patients listed for repeat renal transplantation. Kidney Int. 2014, 86, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Martin, K.; Cantwell, L.; Barraclough, K.A.; Lian, M.; Masterson, R.; Hughes, P.D.; Chow, K.V. Prolonged immunosuppression does not improve risk of sensitization or likelihood of retransplantation after kidney transplant graft failure. Transpl. Int. 2021, 34, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Knoll, G.; Campbell, P.; Chassé, M.; Fergusson, D.; Ramsay, T.; Karnabi, P.; Perl, J.; House, A.A.; Kim, J.; Johnston, O.; et al. Immunosuppressant Medication Use in Patients with Kidney Allograft Failure: A Prospective Multicenter Canadian Cohort Study. J. Am. Soc. Nephrol. 2022, 33, 1182–1192. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.; Mohan, S. Managing Patients with Failing Kidney Allograft: Many Questions Remain. Clin. J. Am. Soc. Nephrol. 2022, 17, 444–451. [Google Scholar] [CrossRef]
- Kidney Transplantation in Adults: Management of the Patient with a Failed Kidney Transplant—UpToDate [Internet]. Available online: https://www.uptodate.com/contents/kidney-transplantation-in-adults-management-of-the-patient-with-a-failed-kidney-transplant?search=kidney-graft-failure&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H2595807251 (accessed on 20 June 2022).
- Fiorentino, M.; Gallo, P.; Giliberti, M.; Colucci, V.; Schena, A.; Stallone, G.; Gesualdo, L.; Castellano, G. Management of patients with a failed kidney transplant: What should we do? Clin. Kidney J. 2020, 14, 98–106. [Google Scholar] [CrossRef]
- Kassakian, C.T.; Ajmal, S.; Gohh, R.Y.; Morrissey, P.E.; Bayliss, G.P. Immunosuppression in the failing and failed transplant kidney: Optimizing outcomes: Table 1. Nephrol. Dial. Transplant. 2016, 31, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Pham, P.-T.; Everly, M.; Faravardeh, A.; Pham, P.-C. Management of patients with a failed kidney transplant: Dialysis reinitiation, immunosuppression weaning, and transplantectomy World Journal of Nephrology. World J. Nephrol. 2015, 4, 148–159. [Google Scholar] [CrossRef]
- Badell, I.R.; Bray, R.A.; Elbein, R.; Chami, A.S.; Easley, K.A.; Pastan, S.O.; Guasch, A.; Gebel, H.M.; Adams, A.B.; Larsen, C.P. Belatacept in Kidney Transplant Recipients With Failed Allografts for the Prevention of Humoral Sensitization: A Pilot Randomized Controlled Trial. Transplantation 2021, 105, e395–e396. [Google Scholar] [CrossRef]
- Bunthof, K.L.; Hazzan, M.; Hilbrands, L.B. Review: Management of patients with kidney allograft failure. Transplant. Rev. 2018, 32, 178–186. [Google Scholar] [CrossRef]
- Ghyselen, L.; Naesens, M. Indications, risks and impact of failed allograft nephrectomy. Transplant. Rev. 2019, 33, 48–54. [Google Scholar] [CrossRef]
- Johnston, O.; Rose, C.; Landsberg, D.; Gourlay, W.A.; Gill, J.S. Nephrectomy after transplant failure: Current practice and outcomes. Am J Transplant. 2007, 7, 1961–1967. [Google Scholar] [CrossRef]
- Milongo, D.; Kamar, N.; Del Bello, A.; Guilbeau-Frugier, C.; Sallusto, F.; Esposito, L.; Dörr, G.; Blancher, A.; Congy-Jolivet, N. Allelic and epitopic characterization of intra-kidney-allograft anti-HLA antibodies at allograft nephrectomy. Am. J. Transplant. 2017, 17, 420–431. [Google Scholar] [CrossRef] [Green Version]
- Del Bello, A.; Congy-Jolivet, N.; Sallusto, F.; Guilbeau-Frugier, C.; Cardeau-Desangles, I.; Fort, M.; Esposito, L.; Guitard, J.; Cointault, O.; Lavayssiere, L.; et al. Donor-specific antibodies after ceasing immunosuppressive therapy, with or without an allograft nephrectomy. Clin. J. Am. Soc. Nephrol. 2012, 7, 1310–1319. [Google Scholar] [CrossRef] [Green Version]
- Gavriilidis, P.; Callaghan, J.M.O.; Hunter, J.; Fernando, T.; Imray, C.; Roy, D. Allograft nephrectomy versus nonallograft nephrectomy after failed renal transplantation: A systematic review by updated meta-analysis. Transpl. Int. 2021, 34, 1374–1385. [Google Scholar] [CrossRef]
- Ayus, J.C.; Achinger, S.G.; Lee, S.; Sayegh, M.H.; Go, A.S. Transplant nephrectomy improves survival following a failed renal allograft. J. Am. Soc. Nephrol. 2010, 21, 374–380. [Google Scholar] [CrossRef] [Green Version]
- Systematic Transplantectomy Versus Conventional Care after Kidney Graft Failure. 2022. Available online: https://clinicaltrials.gov/ct2/show/NCT01817504 (accessed on 25 September 2022).
- Takase, H.M.; Contti, M.M.; Nga, H.S.; Bravin, A.M.; Valiatti, M.F.; El-Dib, R.P.; De Andrade, L.G.M. Nephrectomy Versus Embolization of Non-Functioning Renal Graft: A Systematic Review with a Proportional Meta-Analysis. Ann. Transplant. 2018, 23, 207–217. [Google Scholar] [CrossRef]
- Delgado, P.; Diaz, F.; Gonzalez, A.; Sanchez, E.; Gutierrez, P.; Hernandez, D.; Torres, A.; Lorenzo, V. Intolerance syndrome in failed renal allografts: Incidence and efficacy of percutaneous embolization. Am. J. Kidney Dis. 2005, 46, 339–344. [Google Scholar] [CrossRef]
- Ojo, A.O.; Wolfe, R.A.; Agodoa, L.Y.; Held, P.J.; Port, F.K.; Leavey, S.F.; Callard, S.E.; Dickinson, D.M.; Schmouder, R.L.; Leichtman, A.B. Prognosis after primary renal transplant failure and the beneficial effects of repeat transplantation: Multivariate analyses from the United States Renal Data System. Transplantation 1998, 66, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.S.; Schaubel, D.E.; Wei, G.; Fenton, S.S.A. Evaluating the Survival Benefit of Kidney Retransplantation. Transplantation 2006, 82, 669–674. [Google Scholar] [CrossRef] [PubMed]
- McCaughan, J.A.; Patterson, C.C.; Maxwell, A.P.; Courtney, A.E. Factors influencing survival after kidney transplant failure. Transplant. Res. 2014, 3, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manook, M.; Koeser, L.; Ahmed, Z.; Robb, M.; Johnson, R.; Shaw, O.; Kessaris, N.; Dorling, A.; Mamode, N. Post-listing survival for highly sensitised patients on the UK kidney transplant waiting list: A matched cohort analysis. Lancet 2017, 389, 727–734. [Google Scholar] [CrossRef]
- Leal, R.; Pardinhas, C.; Martinho, A.; Sá, H.O.; Figueiredo, A.; Alves, R. Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss. J. Clin. Med. 2022, 11, 5753. [Google Scholar] [CrossRef]


{kind=link}
| Candidate for Retransplant | Not a Candidate for Retransplant | Other Notes | |
|---|---|---|---|
| Lubetzky et al. (KRAFT) AST 2022 [19] |
|
|
|
| Davis et al. CJASN 2022 [68] |
|
|
|
| Miller; Brennan UptoDate [69] | If retransplantation planned within 1 year:
|
|
|
| Fiorentino et al. CKJ 2021 [70] |
|
|
|
| Kassakian et al. NDT 2016 [71] |
|
|
|
| Pham et al. World J Nephrol 2015 [72] |
|
|
|
| British Transplantation Society 2014 [6] |
|
|
|
| Established Indications for Graft Nephrectomy |
|---|
| Primary dysfunction |
| Severe acute rejection resistant to immunosuppression |
| Severe graft pyelonephritis/urosepsis |
| Post-transplant lymphoproliferative disease in the graft |
| Refractory graft intolerance syndrome |
| Graft hemorrhage or thrombosis |
| To create space for subsequent retransplant |
| Relative Indications for Graft Nephrectomy |
| Early graft loss (<6–12 months) |
| Resistant BK virus nephropathy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leal, R.; Pardinhas, C.; Martinho, A.; Sá, H.O.; Figueiredo, A.; Alves, R. Challenges in the Management of the Patient with a Failing Kidney Graft: A Narrative Review. J. Clin. Med. 2022, 11, 6108. https://doi.org/10.3390/jcm11206108
Leal R, Pardinhas C, Martinho A, Sá HO, Figueiredo A, Alves R. Challenges in the Management of the Patient with a Failing Kidney Graft: A Narrative Review. Journal of Clinical Medicine. 2022; 11(20):6108. https://doi.org/10.3390/jcm11206108
Chicago/Turabian StyleLeal, Rita, Clara Pardinhas, António Martinho, Helena Oliveira Sá, Arnaldo Figueiredo, and Rui Alves. 2022. "Challenges in the Management of the Patient with a Failing Kidney Graft: A Narrative Review" Journal of Clinical Medicine 11, no. 20: 6108. https://doi.org/10.3390/jcm11206108
APA StyleLeal, R., Pardinhas, C., Martinho, A., Sá, H. O., Figueiredo, A., & Alves, R. (2022). Challenges in the Management of the Patient with a Failing Kidney Graft: A Narrative Review. Journal of Clinical Medicine, 11(20), 6108. https://doi.org/10.3390/jcm11206108