1. Introduction
According to the 2012 revision of the Atlanta classification for acute pancreatitis (AP), organ failure including the cardiovascular system, lungs or kidneys is the main determinant of AP severity [
1]. About one-third of patients with AP develop transient or persistent single or multiple organ failure, with renal failure being diagnosed in about 20% [
2]. Moreover, the markers associated with renal function: serum creatinine [
3] and blood urea nitrogen [
4] are recognized predictors of severity of AP. Either serum creatinine or urea nitrogen is included in most prognostic scores currently used or proposed to evaluate AP severity such as Acute Physiology and Chronic Health Examination II (APACHE II), Bedside Index for Severity in AP (BISAP), Glasgow criteria, Ranson score, Harmless AP Score (HAPS), Japanese Severity Score (JSS) or Pancreatitis Outcome Prediction (POP) [
5]. This reflects the fact that both underlying chronic kidney disease [
6,
7,
8] and acute kidney injury (AKI) developing in the course of AP [
9] are adversely associated with AP severity and mortality.
The most widely accepted way of describing kidney function is through glomerular filtration rate (GFR), which use is supported by the clinical practice guidelines [
10]. The assessment of GFR is based on measuring the renal clearance of exogenous (e.g., inulin, iohexol, iothalamate, or radiopharmaceuticals
51Cr-ethylenediaminetetraacetic acid and
99mTc-diethylenetriaminepentaacetic acid) or endogenous substances (most commonly creatinine) [
11,
12]. Since such measurements are either invasive or cumbersome for patients (e.g., the assessment of creatinine clearance requires 24 h urine collection), routine clinical practice has widely adopted an estimation of GFR. Several formulas have been validated for this purpose, including those introduced by Chronic Kidney Disease–Epidemiology Collaboration (CKD-EPI), based on serum creatinine or cystatin C concentrations, age, sex and race [
13,
14]. The CKD-EPI formulas produce sufficiently adequate estimated GFR (eGFR) values in most cases when serum creatinine or cystatin C concentrations are stable over time, supporting clinical decisions in patients with chronic kidney disease [
10]. However, these formulas do not work well when renal function is changing acutely, mainly because the changes in serum creatinine or cystatin C concentrations are slower (or appear with a lag time) compared to the changes in GFR [
15,
16]. Moreover, in patients with acute conditions, many non-renal factors (abnormalities in water balance, inflammation, altered metabolism and diet, or treatment including fluid resuscitation) influence the serum/plasma concentrations of creatinine and cystatin C [
16]. In such patients, the measurement of GFR may be contraindicated (clearance of exogenous markers) or unreliable (creatinine clearance). Therefore, current diagnostic criteria for AKI are based on changes in serum creatinine over time, and not on measured GFR or eGFR [
17].
To solve this problem, several authors [
15,
18,
19,
20] introduced the formulas enabling GFR estimation in a non-steady state, based on a general concept of creatinine clearance and incorporating the dynamically changing serum creatinine concentrations. Of those, the mathematically simplest formula of Chen [
20] has been verified in several clinical studies involving patients of intensive care unit (ICU) [
21] and renal transplant recipients [
22,
23]. In general, the clinical observational studies [
21,
22,
23,
24,
25,
26] supported the usefulness of KeGFR in the assessment of patients with acutely changing serum creatinine and suggested that KeGFR may improve drug dosing in such patients [
27]. It has been postulated that evaluating GFR in patients with AKI would improve the assessment of patients in addition to laboratory markers of kidney tubular injury such as neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), or so-called cell cycle arrest biomarkers: tissue inhibitor of matrix metalloproteinase-2 (TIMP-2) and insulin growth factor binding protein-7 (IGFBP-7) [
28]. On the contrary, there are limited data showing a lack of agreement between KeGFR and measured GFR in patients with acutely changing kidney function [
29,
30].
We were not able to identify any studies using the kinetic eGFR (KeGFR) in patients or experimental animals with AP. Therefore, our aim was to estimate GFR in patients with AP using the KeGFR formula and to evaluate the diagnostic utility of KeGFR in the early stage of AP (first three days of hospital stay) to assess renal function and to predict the severity of AP. In the early phase of AP, hemodynamic changes are common and acute kidney injury may develop, resulting in dynamic changes in serum creatinine concentrations observed in clinical practice.
2. Materials and Methods
2.1. Patients and Definitions
The study was based on a retrospective analysis of data from two cohorts of adult patients with AP, recruited at the Surgery Department, District Hospital in Sucha Beskidzka, Poland, between January and December 2014 [
31] and in the Department of Surgery, Complex of Health Care Centers in Wadowice, Poland, between March 2014 and December 2015 [
32]. Both centers are secondary care regional hospitals. Both cohorts were recruited following the agreement of the appropriate bioethical commissions, and the present study protocol for the retrospective analysis of formerly obtained data was accepted by the Bioethical Committee of Jagiellonian University, Kraków, Poland (approval no 122.6120.241.2015 issued on 22 October 2015). The present study included patients for whom data were available to calculate KeGFR (i.e., serum creatinine was measured on each day of the study in known 24 h intervals).
The two cohorts included patients who were prospectively recruited based on consistent inclusion and exclusion criteria, namely, patients were included if they were admitted to hospital within the first 24 h following the onset of AP symptoms, they were diagnosed with AP based on the 2012 revised Atlanta classification (i.e., fulfilled at least two of three diagnostic criteria based on clinical, laboratory and imaging signs and symptoms) [
1], they were adults (≥18 years old) and signed an informed consent for the study upon recruitment [
31,
32].
Patients with chronic pancreatitis, active cancer and chronic liver disease (viral hepatitis or liver cirrhosis) were excluded. Moreover, patients with a medical record of chronic kidney disease in whom baseline serum creatinine exceeded 170 µmol/L were excluded from the present study.
The final severity of AP was classified as mild (MAP), moderately severe (MSAP) or severe (SAP) according to the revised Atlanta classification [
1] taking into account the persistent or transient cardiovascular, pulmonary, or renal failure as defined by modified Marshall scoring system (MMSS) [
1], the systemic complications (exacerbation of comorbidities), and the local complications occurring during the entire hospital stay. Renal failure was defined according to MMSS [
1] as serum creatinine exceeding 170 µmol/L.
The demographic and clinical data were collected including age, sex, preexisting comorbidities, BMI > 30 kg/m
2, AP etiology, AP course and complications (presence of systemic inflammatory response syndrome—SIRS, pleural effusions, local complications, transient persistent organ failure as defined in revised 2012 Atlanta classification [
1], mortality), and AP treatment (endoscopic retrograde cholangiopancreatography—ERCP, surgery, parenteral nutrition, length of hospital stay).
2.2. Laboratory Tests
In both cohorts, blood and urine samples were collected using the same timing, i.e., on admission (i.e., day 1) and then daily for two consecutive days of hospital stay (day 2 and day 3). Routine laboratory tests including complete blood count, biochemistry (serum albumin, glucose, urea, creatinine) and immunochemistry tests (serum C-reactive protein and plasma D-dimer) were performed on the day of blood collection in the laboratories associated with study centers. In both study centers, serum creatinine was assayed with the kinetic Jaffe method traceable to the isotope dilution mass spectrometry (IDMS) reference measurement procedure. Cobas 4000 analyzers (Roche Diagnostics, Mannheim, Germany) were used for the measurements. The reference intervals for serum creatinine were 44.0–80.0 µmol/L for adult women and 62.0–106.0 µmol/L for adult men, respectively. The serum urea/creatinine ratio (a unitless number) was calculated as serum urea expressed in mmol/L multiplied by 1000 (to unify the units) divided by serum creatinine in µmol/L.
Moreover, serum and urine samples were stored for additional laboratory tests that were performed in series following the collection of all samples. Briefly, blood and urine samples were centrifuged, and the supernatant was aliquoted, frozen and kept at −80 °C until analysis. The additional laboratory tests included serum cystatin C, β-trace protein (BTP), uromodulin, angiopoietin-2, soluble fms-like tyrosine kinase-1 (sFlt-1), neutrophil gelatinase-associated lipocalin (NGAL) and urine NGAL. The additional tests were not done on a part of the patients due to limited volume of samples. The numbers of patients with available results of the additional tests are presented in
Appendix A (
Table A1).
Serum cystatin C and BTP were measured using immunonephelometric method and Nephelometer II analyzer (Siemens Healthcare, Erlangen, Germany). The laboratory reference interval for cystatin C was 0.59–1.04 mg/L; the reference interval for serum BTP was <0.70 mg/L. The concentrations of sFlt-1 in serum were measured by electrochemiluminescence on Cobas 8000 analyzer (Roche Diagnostics, Mannheim, Germany). The concentrations of sFlt-1 in healthy subjects were 63–108 ng/mL. Urine NGAL was assessed with chemiluminescence microparticle immunoassay (Architect urine NGAL) on Abbott Architect analyzer (Abbott Laboratories, Chicago, IL, USA). The measurements were performed in the Diagnostic Department, University Hospital in Kraków, Poland.
Angiopoietin-2, uromodulin and NGAL in serum were measured with commercially available enzyme-linked immunosorbent assays (ELISA): Quantikine ELISA Human Angiopoietin-2 Immunoassay (R&D Systems, McKinley Place, MN, USA), Human Uromodulin ELISA and Human Lipocalin-2/NGAL ELISA (BioVendor, Brno, Czech Republic). The readings were performed with Automatic Micro ELISA Reader ELX 808 (BIO-TEK® Instruments Inc., Winooski, VT, USA). According to the manufacturers of the kits, reference values in healthy adults were 1.065–8.907 ng/mL for angiopoietin-2, and 37.0–501.0 ng/mL for uromodulin, respectively. Serum NGAL concentrations in unselected adult donors were 14.4–169.2 ng/mL for men and 21.6–276.0 for women. The measurements were performed in the Department of Diagnostics, Chair of Clinical Biochemistry, Jagiellonian University Medical College, Kraków, Poland.
2.3. Equation Used to Estimate Kinetic GFR
KeGFR was estimated based on the formula presented by Chen [
20], using eGFR based on serum creatinine calculated from 2021 CKD-EPI formula [
13] as the substitute for creatinine clearance. Precisely, we used the following Formula (1):
where min
SCr is minimum serum creatinine during the study, eGFR is the respective GFR calculated using 2021 CKD-EPI equation, and
mean SCr is the arithmetic mean of two consecutive serum creatinine results obtained during the study (e.g., on day 1 and day 2), Δ
SCr is a difference between the two consecutive serum creatinine results (e.g., day 2 creatinine–day 1 creatinine), Δ
t is time in h between the two consecutive serum creatinine results (this equaled 24 h in our study), and maxΔ
SCr is a maximum possible rise in serum creatinine per day (such as may be observed in an anuric patient during AKI). For maxΔ
SCr, we used a value of 132.6 µmol/L (equal to 1.5 mg/dL as suggested by Chen [
20] for adult patients). Since serum creatinine values are represented both in numerators and denominators in Equation (1), the equation works well irrespective of the unit used to express serum creatinine concentrations, and we used the values in µmol/L as reported by the study centers’ laboratories. Because the estimation of KeGFR requires two consecutive serum creatinine results, and we did not record pre-hospitalization serum creatinine values (these were unavailable in many patients), we were able to estimate two KeGFR values during the study: on day 2 (based on serum creatinine measured on admission, i.e., day 1 and on day 2), and day 3 (based on day 2 and day 3 serum creatinine results).
2.4. Statistical Analysis
Categorical data were summarized using number and percentage of the respective group and compared between groups using Pearson chi-squared test. Quantitative variables were summarized using mean and standard deviations if normally distributed and median and lower (Q1), upper quartile (Q3) if non-normally distributed. Since the vast majority of variables were non-normally distributed, Mann–Whitney test or Kruskal–Wallis test were used to compare the values between two or three groups, respectively. Spearman rank correlation coefficient was calculated to assess correlations between variables. Multiple linear and logistic regression was used to verify if the association between KeGFR and age is independent of the study center. The diagnostic accuracy was evaluated using receiver operating characteristic (ROC) curves. The cut-off values were selected at maximum Youden index. Multiple logistic regression served to assess KeGFR as a predictor of renal failure and SAP with adjustment for clinically significant confounders (age, sex, preexisting comorbidities, study center). Two-tailed statistical tests were used; the results were considered significant at p < 0.05. Statistica 13.3 (Tibco Software Inc., Tulsa, OK, USA) and associated Plus Bundle ver. 5.0.96 (StatSoft Polska, Kraków, Poland) were used for computations.
4. Discussion
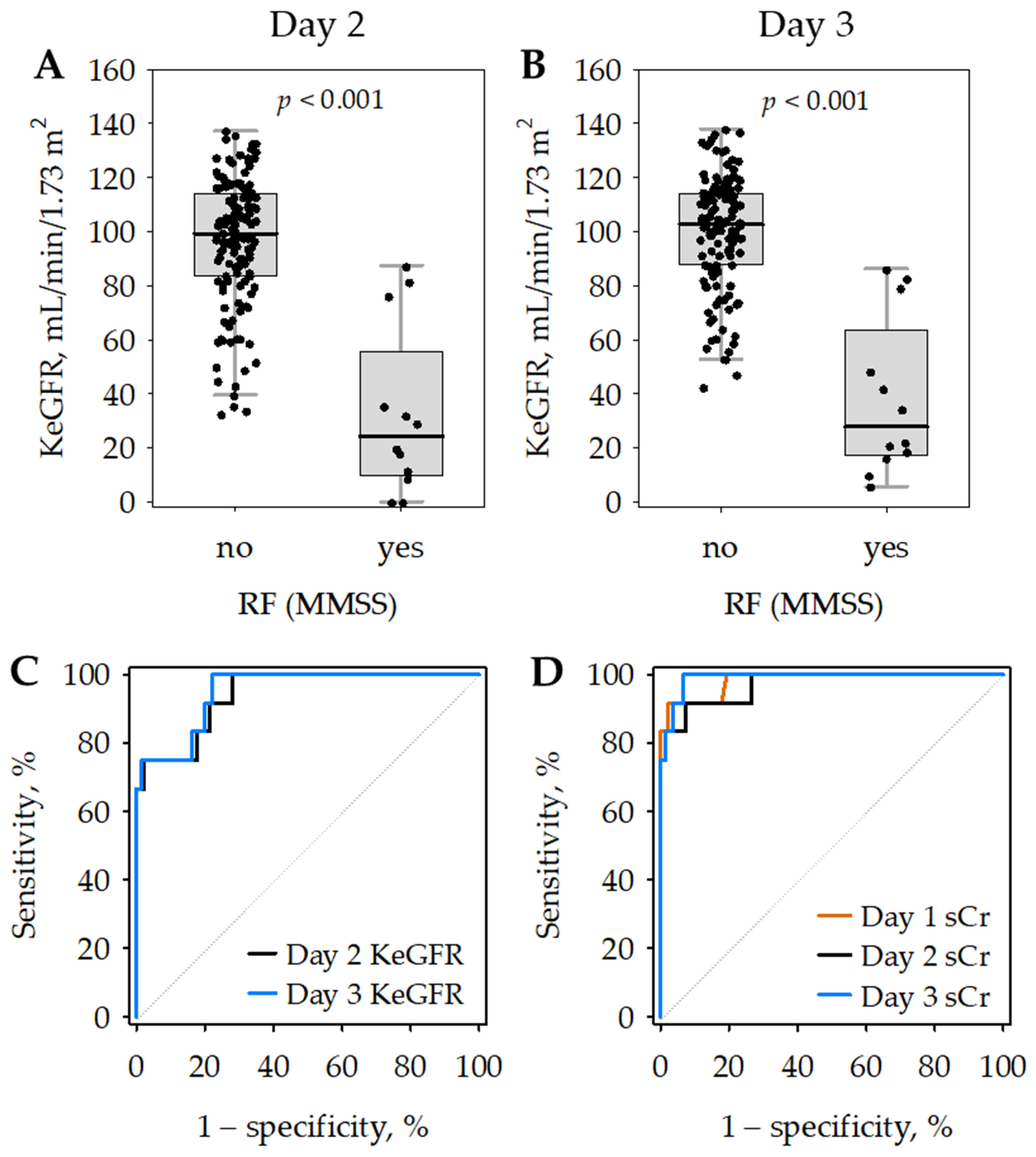
In our study, significant acute changes in serum creatinine were observed in nearly one-fourth of patients with AP during the first three days from admission. KeGFR was an accurate marker of renal failure defined according to MMSS in the early phase of AP. Although the diagnostic accuracy for renal failure was similar for KeGFR and single serum creatinine measurements on days 2 and 3 of the hospital stay, the changes in KeGFR associated with the dynamic changes in kidney function were more pronounced than the respective changes in serum creatinine. Moreover, KeGFR values assessed in patients with AP during the initial days of the hospital stay significantly predicted a severe course of the disease and mortality.
To the best of our knowledge, KeGFR has not been studied before in patients with AP, either in the context of kidney injury or as a marker of severity. In the initial phase of AP, dynamic changes in serum creatinine, indicating the dynamic changes in glomerular filtration, are common. Therefore, steady state eGFR would not adequately reflect kidney function in many patients with early stage of AP. In 23% of our patients, the difference in two serum creatinine concentrations obtained within the first three days of hospital stay (i.e., within 48 h) exceeded 26.5 µmol/L. Such a difference has been recognized by KDIGO guidelines [
17] as indicative of AKI, and AKI diagnosed with the KDIGO definition is associated with increased mortality [
33,
34]. In the present study, KeGFR correlated negatively with the markers of endothelial injury (angiopoietin 2 and sFlt-1), in line with our previous observations showing the association between these endothelial markers and early kidney injury in AP [
31,
35]. This supports the pathophysiological role of endothelial dysfunction in early AP, associated with increased vascular leakage and hemodynamic changes that also influence glomerular filtration.
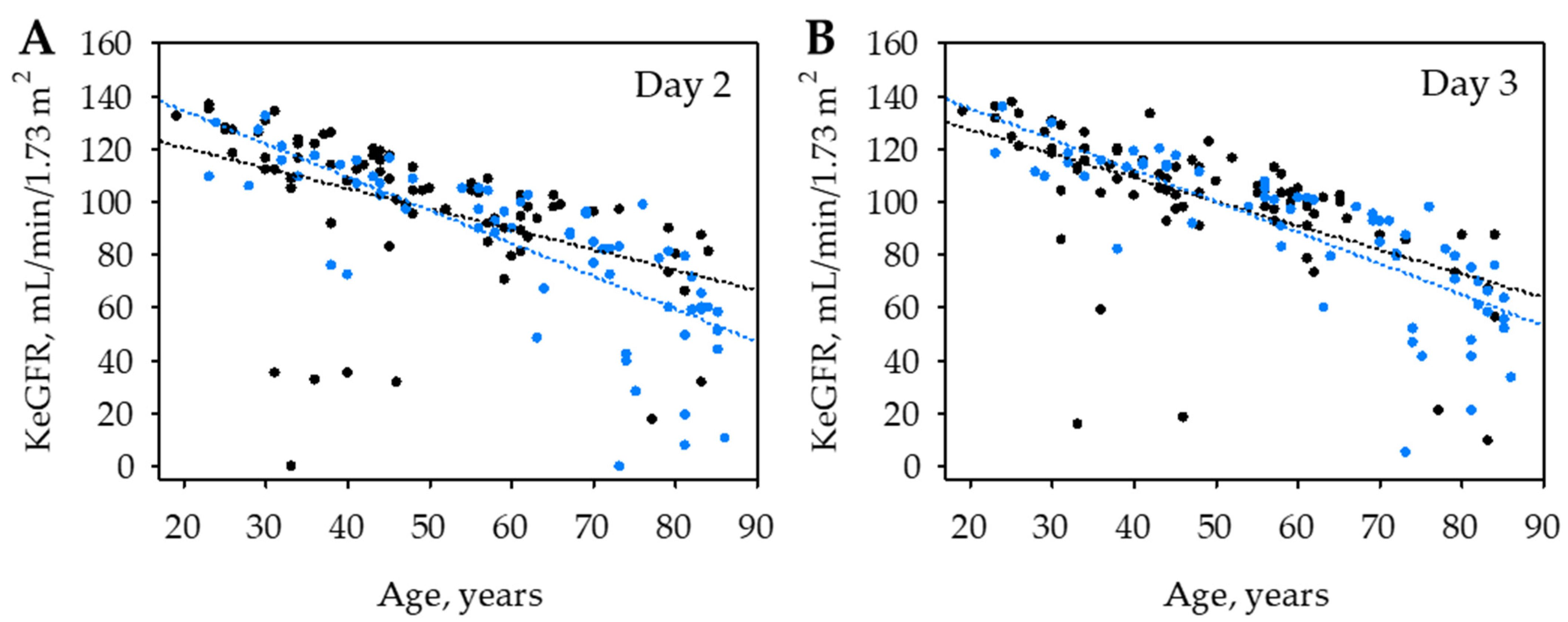
In the studied group, KeGFR was strongly negatively correlated with age, which may reflect both the well-known decrease in baseline GFR observed in elderly patients [
10] and the more pronounced hemodynamic changes in older patients or the higher risk for AKI in older patients with AP [
2]. Moreover, although we calculated KeGFR based on body surface area-standardized eGFR values, women were characterized with lower KeGFR than men. Both the baseline patients’ characteristics were therefore included as confounders in the multiple regression analyses.
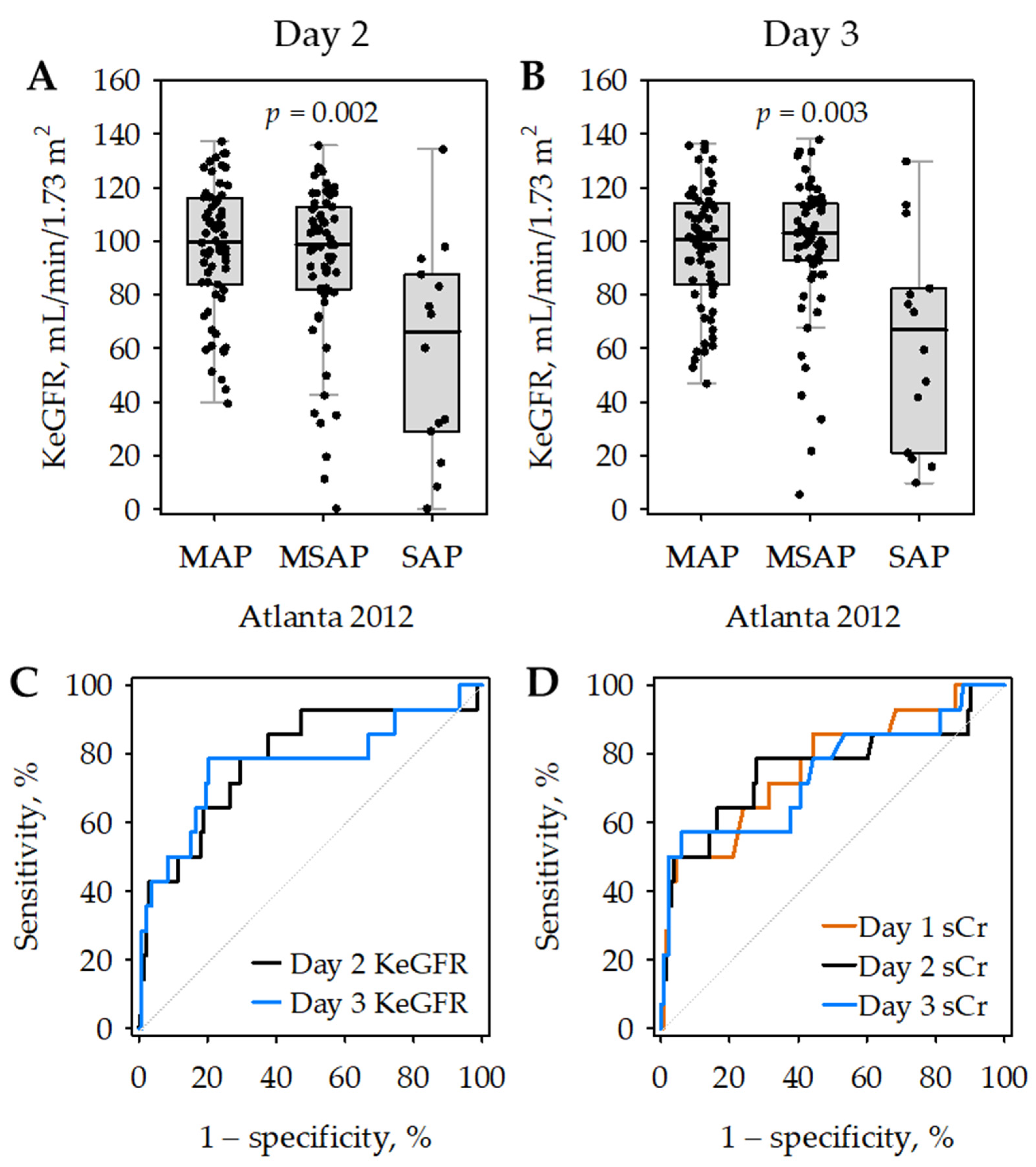
We observed significant changes in serum creatinine mainly in patients with MSAP and SAP. Moreover, renal failure diagnosed in line with MMSS was most prevalent in SAP. Consequently, lower KeGFR was significantly associated with the diagnosis of SAP and mortality. In 2021, Tod et al. [
36] published an analysis of data from a Hungarian AP registry. They reported a significant association between lower steady-state eGFR within 24 h from admission and the diagnosis of SAP, increased length of hospital stay, and mortality [
36]. We did not observe a significant correlation between KeGFR and length of hospital stay; nonetheless, we observed lower KeGFR values in patients with SAP (even after excluding those diagnosed with renal failure) and a significant association between low KeGFR and mortality. We must, however, underlie several doubts regarding the report of Tod et al. [
36]: first, their method of eGFR calculation is unclear (although they stated that they used the 2009 CKD-EPI equation based on serum creatinine, the equation shown in their report differs significantly from the 2009 CKD-EPI equation); further, the number of patients included in the analysis is also unclear (they claimed to include data of 1224 patients; however, they apparently excluded 511 patients with eGFR > 90 mL/min/1.73 m
2).
In addition to serum creatinine, we measured other markers of glomerular filtration (cystatin C, BTP) in available serum samples of our patients. Since these results were not available in the whole studied group, we did not calculate KeGFR based on serum cystatin C or BTP. It is, however, possible to use Chen’s equation with non-creatinine filtration markers; for example, the study of Pianta et al. [
23] showed the clinical utility of KeGFR based on plasma cystatin C in renal transplant recipients. We have previously evaluated serum cystatin C and BTP as markers of AKI in the early phase of AP, showing the moderate diagnostic utility of both markers [
37]. Now, we observed strong negative correlations between creatinine-based KeGFR and serum concentrations of cystatin C and BTP. In contrast, the correlations between KeGFR and serum NGAL were weak and there were no significant correlations between KeGFR and urine NGAL in our present study. Since our previous results suggest that urine NGAL is a good diagnostic marker of AKI in the early phase of AP [
37], we may hypothesize that the simultaneous use of KeGFR with urine NGAL (or alternatively, other tubular markers) could be a sensitive diagnostic strategy for renal injury and dysfunction.
Although the idea of GFR estimation in a non-steady state is not new, KeGFR has regained interest in recent years, following the work of Sheldon Chen [
20], who proposed a relatively simple equation allowing for the estimation of GFR from the results of repeated serum creatinine measurements performed in patients with acutely changing kidney function. The idea behind the equation proposed by Chen was clearly described in his article [
20] and the calculations were easy to adopt in clinical research. This equation was used to calculate KeGFR in observational clinical studies including patients treated in ICU [
21,
24,
25], general hospital patients [
26] and renal transplant recipients [
22,
23]; the same equation was used in our study. There are, however, some discrepancies in the use of the equation between the studies. Namely, the maximum daily change in serum creatinine has either been estimated based on a chosen creatinine concentration, respective eGFR and the volume of distribution for serum creatinine (e.g., by Pianta et al. [
23] and O’Sullivan and Doyle [
24]), or substituted by a constant number (133 µmol/day) as originally suggested by Chen [
20] (e.g., in studies [
21,
22] and ours). Moreover, the previous studies used either the Modification of Diet in Renal Diseases (MDRD) [
24] or the 2009 CKD-EPI equation [
21,
22,
23] as the basic estimation of GFR, whereas we decided on the 2021 race-independent CKD-EPI equation [
13]. The 2009 CKD-EPI equation has been shown to better estimate measured GFR than MDRD and has been recommended by KDIGO guidelines to evaluate patients with chronic kidney disease [
10,
38]. Nonetheless, the two (2009 and 2021) CKD-EPI equations give similar numbers in Caucasian adults and the 2021 equation has been shown to be slightly more consistent with measured GFR in this population [
39]. Further discrepancies between the studies regard serum creatinine measurements. Pianta et al. [
23] measured serum creatinine with the enzymatic method while O’Sullivan and Doyle [
24] and Dash et al. [
22] used the kinetic Jaffe method, similar to our study.
Irrespective of the differences, the results of clinical observational studies [
21,
22,
23,
24,
25,
26] support the clinical utility of KeGFR in various patient populations with acutely changing serum creatinine and are in general agreement with our results. In 2015, Dewitte et al. [
21] published an analysis of 57 patients who developed AKI within 24 h of admission to ICU. They calculated KeGFR on the day following admission and measured urine NGAL, TIMP-2 and IGFBP-7 on admission and on the following day. They assessed the diagnostic accuracy of the studied markers for two distinct outcomes: renal recovery after 48 h in response to fluid resuscitation, and major adverse kidney events (death, renal replacement therapy or doubled serum creatinine at 30 days from admission). KeGFR was an accurate predictor of early recovery from AKI, with an AUROC of 0.87. Both the product of TIMP-2 and IGFBP-7 concentrations and KeGFR showed similarly high diagnostic accuracy for major adverse kidney events (AUROC of 0.80) [
21]. The study [
21] included only two patients with AP (3.5% of the studied group); however, the primary end-point of early (within 48 h) recovery from AKI following fluid resuscitation corresponds well to the definition of transient organ failure in AP, i.e., resolving within 48 h (in contrast to persistent organ failure in SAP). In 2017, O’Sullivan and Doyle [
24] retrospectively compared KeGFR and MDRD-based eGFR as predictors of AKI, renal replacement therapy and the mortality of 107 patients admitted to high dependency and intensive care units of a district hospital. AP was not mentioned among the patients’ diagnoses. KeGFR calculated using two initial serum creatinine concentrations measured after admission predicted AKI and renal replacement therapy with better diagnostic accuracy than eGFR calculated with the MDRD equation at admission. However, neither KeGFR nor eGFR (MDRD) predicted 30-day mortality [
24]. De Oliveira Marques et al. [
25] retrospectively analyzed data from a large cohort (over 13,000) of patients during the first week in ICU. The lowest KeGFR recorded during the first week of stay in the ICU was shown to be associated with the outcome variables (need for renal replacement therapy, hospital mortality and 1-year mortality) in addition to the maximum AKI stage as defined by KDIGO guidelines [
17]. There was moderate concordance between the renal function assessed by KeGFR and AKI diagnosis and stages as defined by the KDIGO guidelines. Christiadi et al. [
26] evaluated KeGFR in 140 hospital patients with positive electronic AKI alert (i.e., serum creatinine results fulfilling the KDIGO [
17] definition of AKI) and 242 control patients without AKI. The decrease in KeGFR of 8–10% or more was identified as an accurate marker of AKI. The authors [
26] observed that decreasing KeGFR may allow for 24 h earlier identification of patients with AKI compared with a creatinine increase fulfilling KDIGO criteria. All these results are consistent regarding the clinical utility of KeGFR in the detection of acute decrease in renal function and related increase in adverse clinical outcomes in patients admitted to hospital, high dependency or intensive care units. Given the lack of previous studies on KeGFR in patients with AP, these patients’ populations are most comparable to ours.
Clinically, KeGFR enables the translation of changes in serum creatinine in individual patients into more meaningful numbers [
24,
27]. GFR may better guide therapeutic decisions than serum creatinine alone. Calculating KeGFR allows widely accepted GFR thresholds to be used to initiate renal replacement therapy or to adjust doses of therapeutic drugs in patients with changing renal function where steady-state eGFR equations are inappropriate. As shown by Kwong et al. [
27], in critically ill patients, the use of KeGFR instead of eGFR would result in significant changes in drug dosing in about 25% of patients.
Scarce data are available on KeGFR validation against measured GFR in patients with dynamically changing kidney function; we were able to identify two such studies, published in 2020 and 2021. Both studies used iohexol clearance as the reference standard of measured GFR. Sangla et al. [
29] included 66 adult patients admitted to general ICU. They compared Chen’s KeGFR and CKD-EPI eGFR based on serum creatinine and cystatin C with measured GFR. All studied equations overestimated GFR. The estimations based on serum creatinine led to worse results over time, which appeared to be associated with the development of sarcopenia leading to lower production of creatinine [
29]. Desgrouas et al. [
30] compared eleven eGFR equations with measured GFR in 57 intensive care patients with shock. Measured GFR on day 1 of the study was significantly lower in most patients when compared to baseline steady-state eGFR, reflecting quickly decreasing renal function. All studied equations resulted in a significant positive bias (between 12 and 46 mL/min/1.73 m
2) versus measured GFR. In fact, Chen’s KeGFR was shown to be less consistent with measured GFR than several other formulas (e.g., Yashiro [
19] or Moran and Myers [
18]) [
30]. Moreover, in both studies [
29,
30], all formulas used to estimate GFR resulted in unacceptable imprecision.
In the present study, we chose the simplest KeGFR formula proposed by Chen. However, his further works suggested more complicated formulas allowing for theoretical improvements in KeGFR estimation [
40,
41]. Although these formulas offer better estimates of KeGFR based on the dynamic modeling of creatinine distribution and elimination, their clinical use is hindered by the difficulties in mathematical calculations. The uptake of these formulas would possibly require a wide access to software designed to calculate KeGFR, verified in clinical studies. Optimally, KeGFR calculated using various proposed formulas should be verified against measured GFR in patients with acutely changing (decreasing or increasing) kidney function.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}



