
The Role of Interventional Radiology in the Diagnosis and Treatment of Pulmonary Arteriovenous Malformations
 , and
, and 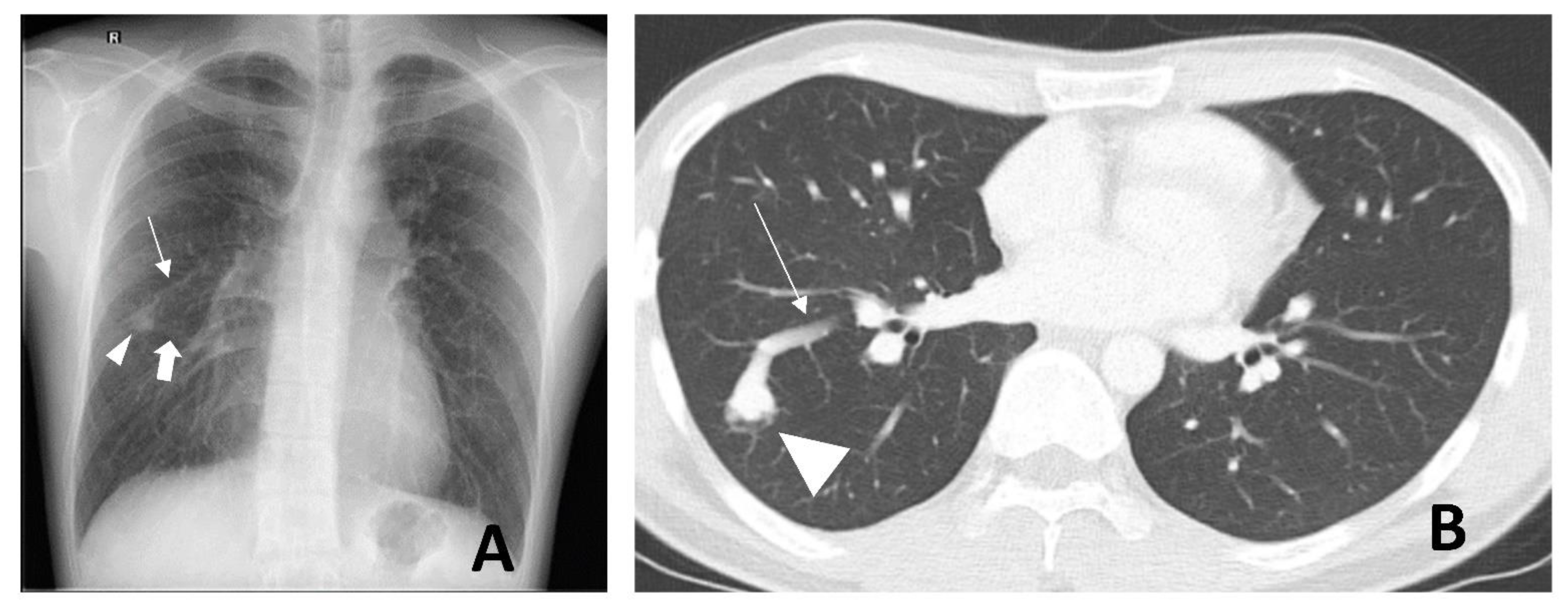{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- (1)
- Simple type: commonest, up to 80%, with a single segmental artery feeding the malformation;
- (2)
- Complex type: with multiple segmental feeding arteries;
- (3)
- Diffuse type: rare, with hundreds of malformations [10].
2. Radiological Diagnosis
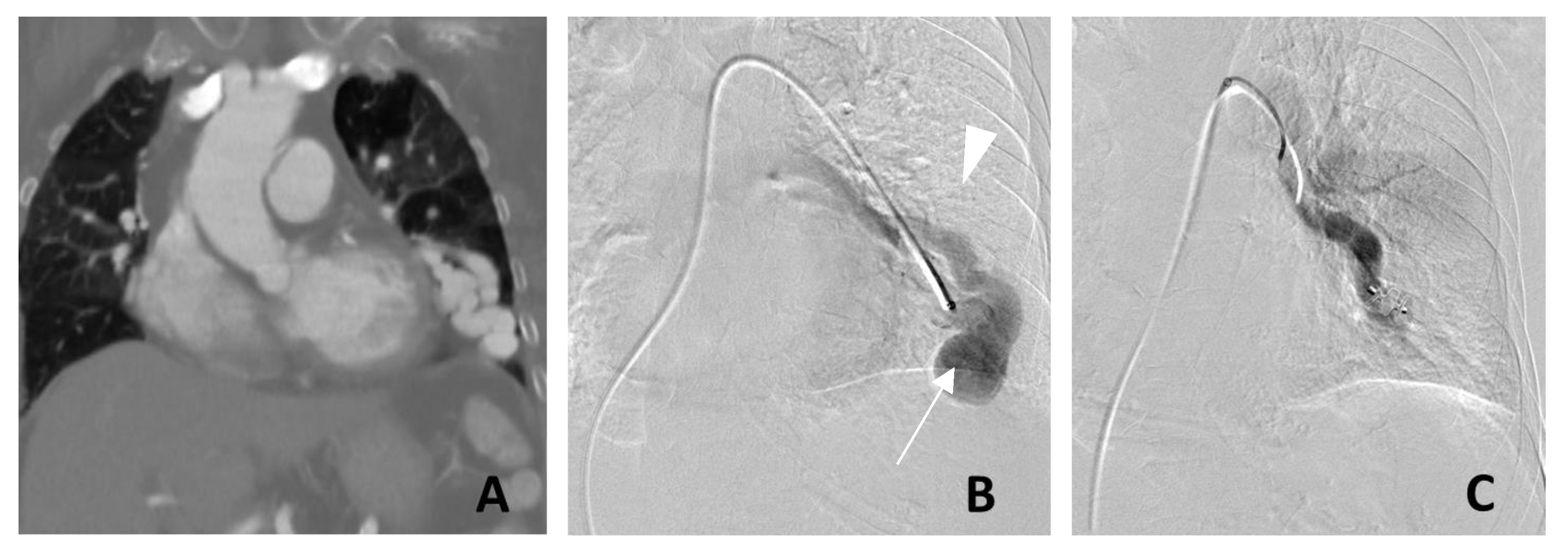
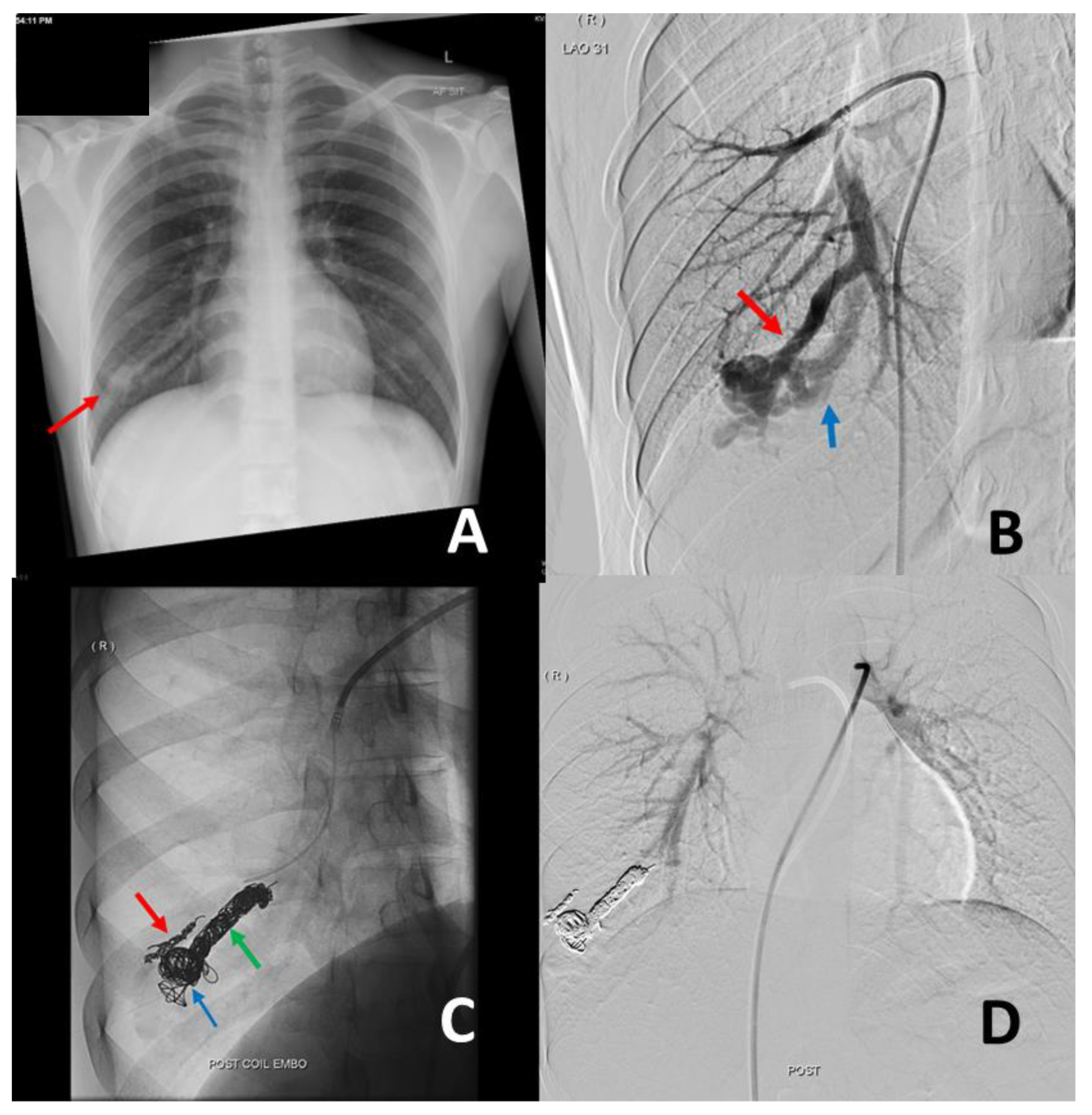
3. Management of PAVM
- (1)
- Any PAVM (solitary or multiple) with a feeding artery that is 2 mm or larger;
- (2)
- Measurable increase in the size of the PAVM;
- (3)
- Paradoxical emboli or symptomatic hypoxemia.
- (1)
- Diffuse lobar or segmental PAVMs;
- (2)
- Complex PAVMs not amenable to embolization;
- (3)
- PAVMs with large feeding arteries not amenable to embolization;
- (4)
- Practices or regions that lack an interventional radiology service;
- (5)
- Patients with contraindication to iodinated contrast medium.
- (1)
- Electrical detachments, such as AZUR HydroCoil Detachable (Terumo Interventional Systems, Somerset, NJ, USA),
- (2)
- Mechanical latch and hook mechanisms, such as Interlock and IDC detachable embolization coils (Boston Scientific, Marlborough, MA, USA)
- (3)
- Ball and socket mechanical detachment mechanisms, such as Ruby Coils (Penumbra, Alameda, CA, USA) and Concerto coils (Medtronic, Santa Rosa, CA, USA).
4. Complications of Endovascular Treatment
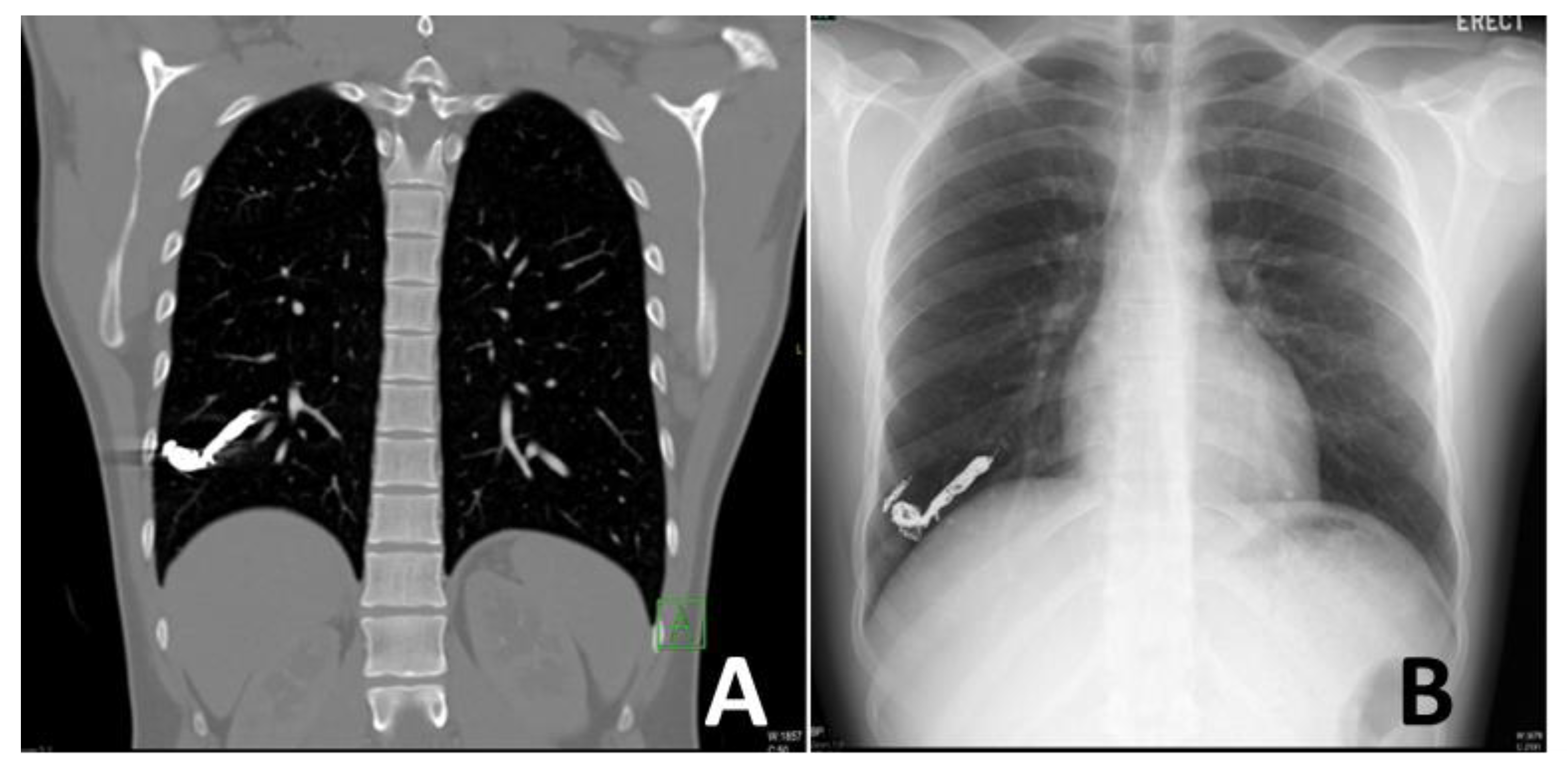
5. Post-Embolization Follow-Up
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gossage, J.R.; Kanj, G. Pulmonary arteriovenous malformations. A state of the art review. Am. J. Respir. Crit. Care Med. 1998, 158, 643–661. [Google Scholar] [CrossRef] [PubMed]
- Saboo, S.S.; Chamarthy, M.; Bhalla, S.; Park, H.; Sutphin, P.; Kay, F.; Battaile, J.; Kalva, S.P. Pulmonary arteriovenous malformations: Diagnosis. Cardiovasc. Diagn. Ther. 2018, 8, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Shovlin, C.L.; Condliffe, R.; Donaldson, J.W.; Kiely, D.G.; Wort, S.J.; British Thoracic Society. British Thoracic Society Clinical Statement on Pulmonary Arteriovenous Malformations. Thorax 2017, 72, 1154–1163. [Google Scholar] [CrossRef] [Green Version]
- Hundt, W.; Kalinowski, M.; Kiessling, A.; Heverhagen, J.T.; Eivazi, B.; Werner, J.; Steinbach, S.; Klose, K.J.; Burbelko, M. Novel approach to complex pulmonary arteriovenous malformation embolization using detachable coils and Amplatzer vascular plugs. Eur. J. Radiol. 2012, 81, e732–e738. [Google Scholar] [CrossRef] [PubMed]
- Kuczyńska, M.; Pyra, K.; Światłowski, Ł.; Sobstyl, J.; Kuklik, E.; Jargiełło, T. Endovascular embolisation strategies for pulmonary arteriovenous malformations. Pol. J. Radiol. 2018, 83, e189–e196. [Google Scholar] [CrossRef]
- Cottin, V.; Chinet, T.; Lavolé, A.; Corre, R.; Marchand, E.; Reynaud-Gaubert, M.; Plauchu, H.; Cordier, J.F.; Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: A series of 126 patients. Medicine 2007, 86, 1–17. [Google Scholar] [CrossRef]
- Suchin, C.R.; Whitman, G.J.; Chew, F.S. Pulmonary arteriovenous malformation. AJR Am. J. Roentgenol. 1996, 167, 648. [Google Scholar] [CrossRef] [Green Version]
- Khurshid, I.; Downie, G.H. Pulmonary arteriovenous malformation. Postgrad. Med. J. 2002, 78, 191–197. [Google Scholar] [CrossRef] [Green Version]
- White, R.I., Jr.; Mitchell, S.E.; Barth, K.H.; Kaufman, S.L.; Kadir, S.; Chang, R.; Terry, P.B. Angioarchitecture of pulmonary arteriovenous malformations: An important consideration before embolotherapy. AJR Am. J. Roentgenol. 1983, 140, 681–686. [Google Scholar] [CrossRef] [Green Version]
- Meek, M.E.; Meek, J.C.; Beheshti, M.V. Management of pulmonary arteriovenous malformations. Semin. Intervent. Radiol. 2011, 28, 24–31. [Google Scholar] [CrossRef]
- Raptis, D.A.; Short, R.; Robb, C.; Marlow, J.; Naeem, M.; McWilliams, S.; White, A.J.; Chakinala, M.; Picus, D.; Bhalla, S. CT Appearance of Pulmonary Arteriovenous Malformations and Mimics. Radiographics 2022, 42, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Faughnan, M.E.; Mager, J.J.; Hetts, S.W.; Palda, V.A.; Lang-Robertson, K.; Buscarini, E.; Deslandres, E.; Kasthuri, R.S.; Lausman, A.; Poetker, D.; et al. Second International Guidelines for the Diagnosis and Management of Hereditary Hemorrhagic Telangiectasia. Ann. Intern. Med. 2020, 173, 989–1001. [Google Scholar] [CrossRef] [PubMed]
- Montrief, T.; Alerhand, S.; Denault, A.; Scott, J. Point-of-care echocardiography for the evaluation of right-to-left cardiopulmonary shunts: A narrative review. Can. J. Anaesth. 2020, 67, 1824–1838. [Google Scholar] [CrossRef]
- Kijima, Y.; Gevorgyan, R.; McWilliams, J.P.; Miller, N.; Noureddin, N.; Tobis, J.M. Usefulness of Transcranial Doppler for Detecting Pulmonary Arteriovenous Malformations in Hereditary Hemorrhagic Telangiectasia. Am. J. Cardiol. 2016, 117, 1180–1184. [Google Scholar] [CrossRef]
- Müller-Hülsbeck, S.; Marques, L.; Maleux, G.; Osuga, K.; Pelage, J.P.; Wohlgemuth, W.A.; Andersen, P.E. CIRSE Standards of Practice on Diagnosis and Treatment of Pulmonary Arteriovenous Malformations. Cardiovasc. Intervent. Radiol. 2020, 43, 353–361. [Google Scholar] [CrossRef]
- Nagano, M.; Ichinose, J.; Sasabuchi, Y.; Nakajima, J.; Yasunaga, H. Surgery versus percutaneous transcatheter embolization for pulmonary arteriovenous malformation: Analysis of a national inpatient database in Japan. J. Thorac. Cardiovasc. Surg. 2017, 154, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Milic, A.; Chan, R.P.; Cohen, J.H.; Faughnan, M.E. Reperfusion of pulmonary arteriovenous malformations after embolotherapy. J. Vasc. Interv. Radiol. 2005, 16, 1675–1683. [Google Scholar] [CrossRef]
- Muhammad, A.; Rauf, Z.; Shahid, J.; Iqbal, J.; Haq, T.U.; Zafar, U. Endovascular Embolisation of Pulmonary Arteriovenous Malformation Using Amplatzer Vascular Plugs. Cureus 2022, 14, e24214. [Google Scholar] [CrossRef]
- Shovlin, C.L.; Tighe, H.C.; Davies, R.J.; Gibbs, J.S.; Jackson, J.E. Embolisation of pulmonary arteriovenous malformations: No consistent effect on pulmonary artery pressure. Eur. Respir. J. 2008, 32, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Lee, S.Y.; Cha, J.G.; Lim, J.K.; Park, J.; Lee, J.; Cha, S.I.; Kim, C.H.; Seo, H. Pulmonary arteriovenous malformation (PAVM) embolization: Prediction of angiographically-confirmed recanalization according to PAVM Diameter changes on CT. CVIR Endovasc. 2021, 4, 16. [Google Scholar] [CrossRef]
- Hong, J.; Lee, S.Y.; Lim, J.K.; Lee, J.; Park, J.; Cha, J.G.; Lee, H.J.; Kim, D. Feasibility of Single-Shot Whole Thoracic Time-Resolved MR Angiography to Evaluate Patients with Multiple Pulmonary Arteriovenous Malformations. Korean J. Radiol. 2022, 23, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Hamamoto, K.; Matsuura, K.; Chiba, E.; Okochi, T.; Tanno, K.; Tanaka, O. Feasibility of Non-contrast-enhanced MR Angiography Using the Time-SLIP Technique for the Assessment of Pulmonary Arteriovenous Malformation. Magn. Reson. Med. Sci. 2016, 15, 253–265. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yap, C.W.; Wee, B.B.K.; Yee, S.Y.; Tiong, V.; Chua, Y.X.; Teo, L.; Lohan, R.; Tan, A.; Singh, P.; Rajendran, P.C.; et al. The Role of Interventional Radiology in the Diagnosis and Treatment of Pulmonary Arteriovenous Malformations. J. Clin. Med. 2022, 11, 6282. https://doi.org/10.3390/jcm11216282
Yap CW, Wee BBK, Yee SY, Tiong V, Chua YX, Teo L, Lohan R, Tan A, Singh P, Rajendran PC, et al. The Role of Interventional Radiology in the Diagnosis and Treatment of Pulmonary Arteriovenous Malformations. Journal of Clinical Medicine. 2022; 11(21):6282. https://doi.org/10.3390/jcm11216282
Chicago/Turabian StyleYap, Chee Woei, Bernard B. K. Wee, Sze Ying Yee, Vincent Tiong, Yi Xiu Chua, Lycia Teo, Rahul Lohan, Amos Tan, Pavel Singh, Prapul Chander Rajendran, and et al. 2022. "The Role of Interventional Radiology in the Diagnosis and Treatment of Pulmonary Arteriovenous Malformations" Journal of Clinical Medicine 11, no. 21: 6282. https://doi.org/10.3390/jcm11216282
APA StyleYap, C. W., Wee, B. B. K., Yee, S. Y., Tiong, V., Chua, Y. X., Teo, L., Lohan, R., Tan, A., Singh, P., Rajendran, P. C., Yang, C., Yee, Y. C., Anil, G., & Ong, S. J. (2022). The Role of Interventional Radiology in the Diagnosis and Treatment of Pulmonary Arteriovenous Malformations. Journal of Clinical Medicine, 11(21), 6282. https://doi.org/10.3390/jcm11216282