


Lipid Profile and Small Dense Low-Density Lipoprotein in Acute Coronary Syndrome Patients: Relationships to Demographic, Clinical, Angiographic, and Therapeutic Variables
 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Study Procedure
2.3. Study Definitions
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Demographics of Study Patients
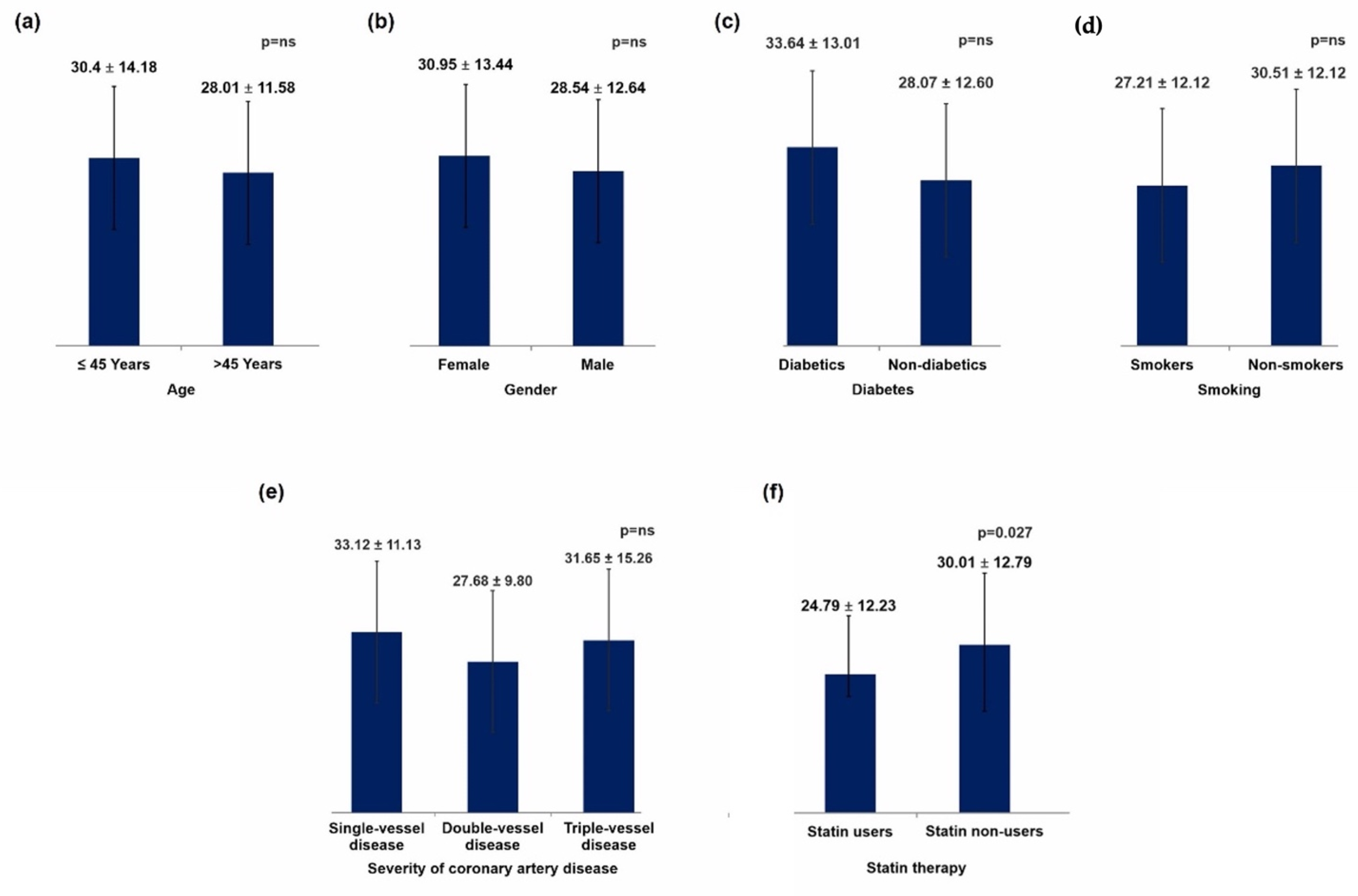
3.2. Lipid Profile According to Patient Age and Gender
3.3. Lipid Profile Comparison between Diabetics versus Non-Diabetics and Smokers versus Non-Smokers
3.4. Lipid Profile Comparison According to Patient’s Statin Therapy
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ishii, J.; Kashiwabara, K.; Ozaki, Y.; Takahashi, H.; Kitagawa, F.; Nishimura, H.; Ishii, H.; Iimuro, S.; Kawai, H.; Muramatsu, T. Small dense low-density lipoprotein cholesterol and cardiovascular risk in statin-treated patients with coronary artery disease. J Atheroscler. Thromb. 2022, 29, 1458–1474. [Google Scholar] [CrossRef] [PubMed]
- Hoogeveen, R.C.; Gaubatz, J.W.; Sun, W.; Dodge, R.C.; Crosby, J.R.; Jiang, J.; Couper, D.; Virani, S.S.; Kathiresan, S.; Boerwinkle, E.; et al. Small dense low-density lipoprotein-cholesterol concentrations predict risk for coronary heart disease: The Atherosclerosis Risk in Communities (ARIC) study. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1069–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikezaki, H.; Lim, E.; Cupples, L.A.; Liu, C.T.; Asztalos, B.F.; Schaefer, E.J. Small dense low-density lipoprotein cholesterol is the most atherogenic lipoprotein parameter in the prospective Framingham Offspring Study. J Am Heart Assoc. 2021, 10, e019140. [Google Scholar] [CrossRef]
- Singh, A.; Puhan, R.; Pradhan, A.; Ali, W.; Sethi, R. Small dense low-density lipoprotein for risk prediction of acute coronary syndrome. Cardiol. Res. 2021, 12, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; He, L. Relationship between small dense low density lipoprotein and cardiovascular events in patients with acute coronary syndrome undergoing percutaneous coronary intervention. BMC Cardiovasc. Disord. 2021, 21, 169. [Google Scholar] [CrossRef]
- Arai, H.; Kokubo, Y.; Watanabe, M.; Sawamura, T.; Ito, Y.; Minagawa, A.; Okamura, T.; Miyamato, Y. Small dense low-density lipoproteins cholesterol can predict incident cardiovascular disease in an urban Japanese cohort: The Suita study. J. Atheroscler. Thromb. 2013, 20, 195–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balling, M.; Nordestgaard, B.G.; Langsted, A.; Varbo, A.; Kamstrup, P.R.; Afzal, S. Small dense low-density lipoprotein cholesterol predicts atherosclerotic cardiovascular disease in the Copenhagen General Population Study. J. Am. Coll. Cardiol. 2020, 75, 2873–2875. [Google Scholar] [CrossRef]
- Hirano, T.; Ito, Y.; Saegusa, H.; Yoshino, G. A novel and simple method for quantification of small, dense LDL. J. Lipid Res. 2003, 44, 2193–2201. [Google Scholar] [CrossRef] [Green Version]
- Ito, Y.; Fujimura, M.; Ohta, M.; Hirano, T. Development of a homogeneous assay for measurement of small dense LDL cholesterol. Clin Chem. 2011, 57, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Albers, J.J.; Kennedy, H.; Marcovina, S.M. Evaluation of a new homogenous method for detection of small dense LDL cholesterol: Comparison with the LDL cholesterol profile obtained by density gradient ultracentrifugation. Clin Chim. Acta 2011, 412, 556–561. [Google Scholar] [CrossRef]
- Renjith, R.S.; Jayakumari, N. A simple economical method for assay of atherogenic small dense low-density lipoprotein-cholesterol (sdLDL-C). Indian J. Clin Biochem. 2011, 26, 385–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srisawasdi, P.; Chaloeysup, S.; Teerajetgul, Y.; Pocathikorn, A.; Sukasem, C.; Vanavanan, S.; Kroll, M.H. Estimation of plasma small dense LDL cholesterol from classic lipid measures. Am. J. Clin Pathol. 2011, 136, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samanta, B. Can calculated SdLDL serve as a substitute for estimated SdLDL? Asian J. Med. Sci. 2021, 12, 14–19. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction; Katus, H.A.; Lindahl, B.; Morrow, D.A. Third universal definition of myocardial infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [Green Version]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Evangelista, A.; Griffin, B.P.; Iung, B.; Otto, C.M.; Pellikka, P.A.; Quiñones, M.; et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J. Am. Soc. Echocardiogr. 2009, 22, 1–23. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Yogesh Kumar, Y.S.; Sud, S.; Bhardwaj, S.; Pareek, T.K. Acute coronary syndrome in young males after a prolonged stay at high altitude. Med. J. Armed Forces India. 2021, 77, 490–493. [Google Scholar] [CrossRef]
- Tsai, W.C.; Wu, K.Y.; Lin, G.M.; Chen, S.J.; Lin, W.S.; Yang, S.P.; Cheng, S.M.; Lin, C.S. Clinical characteristics of patients less than forty years old with coronary artery disease in Taiwan: A cross-sectional study. Acta Cardiol. Sin. 2017, 33, 233–240. [Google Scholar]
- Reda, A.A.; Mina, M.B.; Taha Hussein, A.N. Pattern of risk factors and management strategies in patients with acute coronary syndrome. Menoufia Med. J. 2018, 31, 378–386. [Google Scholar]
- Goel, P.K.; Ashfaq, F.; Khanna, R.; Ramesh, V.; Pandey, C.M. The association between small dense low density lipoprotein and coronary artery disease in North Indian patients. Indian J. Clin Biochem. 2017, 32, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Gohari, L.H.; Ghassab, R.K.; Firoozray, M.; Zavarehee, A.; Basiri, H.A. The association between small dense low density lipoprotein, apolipoprotein B, apolipoprotein B/apolipoprotein A1 ratio and coronary and coronary artery stenosis. Med. J. Islam. Repub. Iran 2009, 23, 8–13. [Google Scholar]
- Taskinen, M.R. Diabetic dyslipidaemia: From basic research to clinical practice. Diabetologia 2003, 46, 733–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ban, Y.; Koba, S.; Tsunoda, F.; Yokota, Y.; Ezumi, H.; Kondo, T.; Suzuki, H.; Katagiri, T. Predominance of small dense low-density lipoproteins and abnormal glucose regulation in patients with acute coronary syndrome. Circ. J. 2006, 70, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.L.; Zhang, H.W.; Cao, Y.X.; Liu, H.H.; Hua, Q.; Li, Y.F.; Zhang, Y.; Wu, N.Q.; Zhu, C.G.; Xu, R.X.; et al. Association of small dense low-density lipoprotein with cardiovascular outcome in patients with coronary artery disease and diabetes: A prospective, observational cohort study. Cardiovasc. Diabetol. 2020, 19, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, V.; Deepa, R.; Velmurugan, K.; Gokulakrishnan, K. Association of small dense LDL with coronary artery disease and diabetes in urban Asian Indians—The Chennai urban rural epidemiology study (CURES-8). J. Assoc. Physicians India 2005, 53, 95–100. [Google Scholar]
- Wilson, P.W.F.; Jacobson, T.A.; Martin, S.S.; Jackson, E.J.; Le, N.A.; Davidson, M.H.; Vesper, H.W.; Frikke-Schmidt, R.; Ballantyne, C.M.; Remaley, A.T. Lipid measurements in the management of cardiovascular diseases: Practical recommendations a scientific statement from the national lipid association writing group. J. Clin. Lipidol. 2021, 15, 629–648. [Google Scholar] [CrossRef]
- Blaha, M.J.; Blumenthal, R.S.; Brinton, E.A.; Jacobson, T.A. National Lipid Association Taskforce on Non-HDL Cholesterol. The importance of non-HDL cholesterol reporting in lipid management. J. Clin. Lipidol. 2008, 2, 267–273. [Google Scholar] [CrossRef]
- Brunner, F.J.; Waldeyer, C.; Ojeda, F.; Salomaa, V.; Kee, F.; Sans, S.; Thorand, B.; Giampaoli, S.; Brambilla, P.; Tunstall-Pedoe, H.; et al. Application of non-HDL cholesterol for population-based cardiovascular risk stratification: Results from the Multinational Cardiovascular Risk Consortium. Lancet 2019, 14, 2173–2183. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Ali, W.; Mishra, S.; Pradhan, A.; Sethi, R.; Kushwaha, R.; Singh, U.S.; Perrone, M.A. Circulating soluble lectin-like oxidized low-density lipoprotein receptor-1 (sLOX-1): A diagnostic indicator across the spectrum of acute coronary syndrome. J. Clin Med. 2021, 10, 5567. [Google Scholar] [CrossRef]
- Wang, X.; Wang, L.; Cao, R.; Yang, X.; Xiao, W.; Zhang, Y.; Ye, P. Correlation between small and dense low-density lipoprotein cholesterol and cardiovascular events in Beijing community population. J. Clin. Hypertens 2021, 23, 345–351. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Patients (n = 200) |
|---|---|
| Males | 156 (78.0%) |
| Females | 44 (22.0%) |
| Diabetic | 36 (18.0%) |
| Non-diabetic | 164 (82.0%) |
| Smoker | 87 (43.5%) |
| Non-smoker | 113 (56.5%) |
| Single-vessel disease * | 43/88 (48.9%) |
| Double-vessel disease * | 20/88 (22.7%) |
| Triple-vessel disease * | 25/88 (28.4%) |
| Anterior wall myocardial infarction | 78 (39.0%) |
| Inferior wall myocardial infarction | 91 (45.5%) |
| Non-ST-segment myocardial infarction | 31 (15.5%) |
| Variable | ≤45 Years (n = 89) | >45 Years (n = 111) | p Value |
|---|---|---|---|
| Males | 75 (84.3%) | 81 (73.0%) | 0.055 |
| Females | 14 (15.7%) | 30 (27.0%) | |
| Diabetic | 13 (14.6%) | 23 (20.7%) | 0.263 |
| Non-diabetic | 76 (85.5%) | 88 (79.3%) | |
| Smoker | 36 (40.4%) | 51 (46.0%) | 0.436 |
| Non-smoker | 53 (59.6%) | 60 (54.1%) | |
| Single-vessel disease | 22/34 (64.7%) | 21/54 (38.9%) | 0.005 |
| Double-vessel disease | 9/34 (26.5%) | 11/54 (20.4%) | |
| Triple-vessel disease | 3/34 (8.8%) | 22/54 (40.7%) | |
| Anterior wall myocardial infarction | 32 (36.0%) | 46 (41.4%) | 0.715 |
| Inferior wall myocardial infarction | 42 (47.2%) | 49 (44.1%) | |
| Non-ST-segment myocardial infarction | 15 (16.9%) | 16 (14.4%) |
| Variable | ≤45 Years (n = 89) | >45 Years (n = 111) | p Value | Females (n = 44) | Males (n = 156) | p Value |
|---|---|---|---|---|---|---|
| TC, mg/dL | 170.58 ± 46.28 | 163.73 ± 36.53 | 0.244 | 169.69 ± 38.00 | 165.96 ± 42.13 | 0.597 |
| HDL, mg/dL | 40.44 ± 10.57 | 39.98 ± 8.47 | 0.728 | 41.75 ± 10.78 | 39.74 ± 9.02 | 0.214 |
| cLDLc, mg/dL | 104.58 ± 36.76 | 98.88 ± 30.66 | 0.328 | 100.54 ± 30.86 | 102.39 ± 34.32 | 0.750 |
| TG, mg/dL | 118.22 ± 49.96 | 114.84 ± 51.95 | 0.643 | 126.59 ± 65.07 | 113.46 ± 46.07 | 0.131 |
| Non-HDL, mg/dL | 130.13 ± 40.81 | 122.70 ± 33.03 | 0.157 | 127.02 ± 33.99 | 125.72 ± 37.64 | 0.836 |
| dLDLc, mg/dL | 103.79 ± 34.96 | 99.42 ± 28.69 | 0.333 | 102.29 ± 27.96 | 101.10 ± 32.66 | 0.826 |
| sd-LDL-C, mg/dL | 30.40 ± 14.18 | 28.01 ± 11.58 | 0.190 | 30.95 ± 13.44 | 28.54 ± 12.64 | 0.273 |
| lbLDL-C, mg/dL | 73.43 ± 25.41 | 71.46 ± 20.33 | 0.542 | 71.45 ± 20.98 | 72.59 ± 23.21 | 0.769 |
| sd-LDL-C: lbLDL-C ratio | 0.42 ± 0.11 | 0.40 ± 0.18 | 0.433 | 0.45 ± 0.23 | 0.40 ± 0.18 | 0.089 |
| Variable | Diabetics (n = 164) | Non-Diabetics (n = 36) | p Value | Smoker (n = 80) | Non-Smoker (n = 106) | p Value |
|---|---|---|---|---|---|---|
| TC, mg/dL | 168.19 ± 35.63 | 166.47 ± 42.41 | 0.597 | 161.82 ± 41.37 | 170.59 ± 40.82 | 0.136 |
| HDL, mg/dL | 37.98 ± 10.47 | 40.67 ± 9.17 | 0.214 | 40.44 ± 8.83 | 39.99 ± 9.93 | 0.739 |
| cLDL-C, mg/dL | 102.68 ± 27.37 | 101.84 ± 34.78 | 0.894 | 100.00 ± 33.95 | 103.49 ± 33.28 | 0.469 |
| TG, mg/dL | 136.49 ± 59.43 | 111.92 ± 48.00 | 0.131 | 109.59 ± 48.50 | 121.55 ± 52.41 | 0.100 |
| Non-HDL, mg/dL | 131.31 ± 30.30 | 124.84 ± 38.04 | 0.836 | 121.84 ± 37.39 | 129.22 ± 36.15 | 0.160 |
| dLDL-C, mg/dL | 106.58 ± 27.78 | 100.22 ± 32.37 | 0.826 | 98.78 ± 31.20 | 103.35 ± 31.94 | 0.312 |
| sd-LDL-C, mg/dL | 33.64 ± 13.01 | 28.07 ± 12.60 | 0.273 | 27.21 ± 12.12 | 30.51 ± 13.21 | 0.071 |
| lbLDL-C, mg/dL | 72.93 ± 1.100 | 72.21 ± 23.20 | 0.769 | 71.52 ± 22.14 | 72.97 ± 23.19 | 0.655 |
| sd-LDL-C: lbLDL-C ratio | 0.48 ± 0.21 | 0.39 ± 0.19 | 0.023 | 0.38 ± 0.18 | 0.43 ± 0.21 | 0.103 |
| Variable | SVD (n = 37) | DVD (n = 17) | TVD (n = 25) | p Value |
|---|---|---|---|---|
| TC, mg/dL | 177.82 ± 31.17 | 169.65 ± 33.19 | 164.61 ± 50.03 | 0.364 |
| HDL, mg/dL | 40.00 ± 10.10 | 42.77 ± 9.06 | 39.24 ± 8.06 | 0.422 |
| cLDL-C, mg/dL | 109.05 ± 28.35 | 104.05 ± 24.03 | 97.02 ± 40.19 | 0.322 |
| TG, mg/dL | 126.65 ± 55.41 | 121.21 ± 46.81 | 132.04 ± 55.22 | 0.796 |
| Non-HDL, mg/dL | 135.00 ± 29.69 | 126.90 ± 29.18 | 125.46 ± 45.23 | 0.484 |
| dLDL-C, mg/dL | 110.03 ± 26.96 | 98.16 ± 22.32 | 100.08 ± 36.69 | 0.222 |
| sd-LDL-C, mg/dL | 33.12 ± 11.13 | 27.68 ± 9.80 | 31.65 ± 15.26 | 0.262 |
| lbLDL-C, mg/dL | 76.81 ± 20.23 | 70.48 ± 14.89 | 68.41 ± 25.74 | 0.239 |
| sd-LDL-C: lbLDL-C ratio | 0.45 ± 0.21 | 0.38 ± 0.14 | 0.47 ± 0.21 | 0.241 |
| Variable | Statin Users (n = 36) | Statin Non-Users (n = 164) | p Value |
|---|---|---|---|
| TC, mg/dL | 149.32 ± 36.66 | 170.61 ± 41.24 | 0.005 |
| HDL, mg/dL | 38.71 ± 10.30 | 40.51 ± 9.25 | 0.301 |
| cLDL-C, mg/dL | 90.92 ± 25.47 | 104.45 ± 34.66 | 0.028 |
| TG, mg/dL, mg/dL | 104.25 ± 40.27 | 119.00 ± 52.77 | 0.116 |
| Non-HDL, mg/dL | 112.83 ± 31.09 | 128.90 ± 37.39 | 0.017 |
| dLDL-C, mg/dL | 90.43 ± 26.77 | 103.76 ± 32.17 | 0.022 |
| sd-LDL-C, mg/dL | 24.79 ± 12.23 | 30.01 ± 12.79 | 0.027 |
| lbLDL-C, mg/dL | 65.63 ± 18.03 | 73.81 ± 23.38 | 0.778 |
| Sd-LDL-C: lbLDL-C ratio | 0.37 ± 0.19 | 0.41 ± 0.20 | 0.970 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradhan, A.; Kuka, R.; Vishwakarma, P.; Ali, W.; Perrone, M.A.; Iellamo, F.; Chaudhary, G.; Chandra, S.; Sethi, R.; Dwivedi, S.; et al. Lipid Profile and Small Dense Low-Density Lipoprotein in Acute Coronary Syndrome Patients: Relationships to Demographic, Clinical, Angiographic, and Therapeutic Variables. J. Clin. Med. 2022, 11, 6846. https://doi.org/10.3390/jcm11226846
Pradhan A, Kuka R, Vishwakarma P, Ali W, Perrone MA, Iellamo F, Chaudhary G, Chandra S, Sethi R, Dwivedi S, et al. Lipid Profile and Small Dense Low-Density Lipoprotein in Acute Coronary Syndrome Patients: Relationships to Demographic, Clinical, Angiographic, and Therapeutic Variables. Journal of Clinical Medicine. 2022; 11(22):6846. https://doi.org/10.3390/jcm11226846
Chicago/Turabian StylePradhan, Akshyaya, Ravninder Kuka, Pravesh Vishwakarma, Wahid Ali, Marco Alfonso Perrone, Ferdinando Iellamo, Gaurav Chaudhary, Sharad Chandra, Rishi Sethi, Sudhanshu Dwivedi, and et al. 2022. "Lipid Profile and Small Dense Low-Density Lipoprotein in Acute Coronary Syndrome Patients: Relationships to Demographic, Clinical, Angiographic, and Therapeutic Variables" Journal of Clinical Medicine 11, no. 22: 6846. https://doi.org/10.3390/jcm11226846
APA StylePradhan, A., Kuka, R., Vishwakarma, P., Ali, W., Perrone, M. A., Iellamo, F., Chaudhary, G., Chandra, S., Sethi, R., Dwivedi, S., Narain, V., & Saran, R. K. (2022). Lipid Profile and Small Dense Low-Density Lipoprotein in Acute Coronary Syndrome Patients: Relationships to Demographic, Clinical, Angiographic, and Therapeutic Variables. Journal of Clinical Medicine, 11(22), 6846. https://doi.org/10.3390/jcm11226846