
Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior–Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Cataract Surgical Procedures
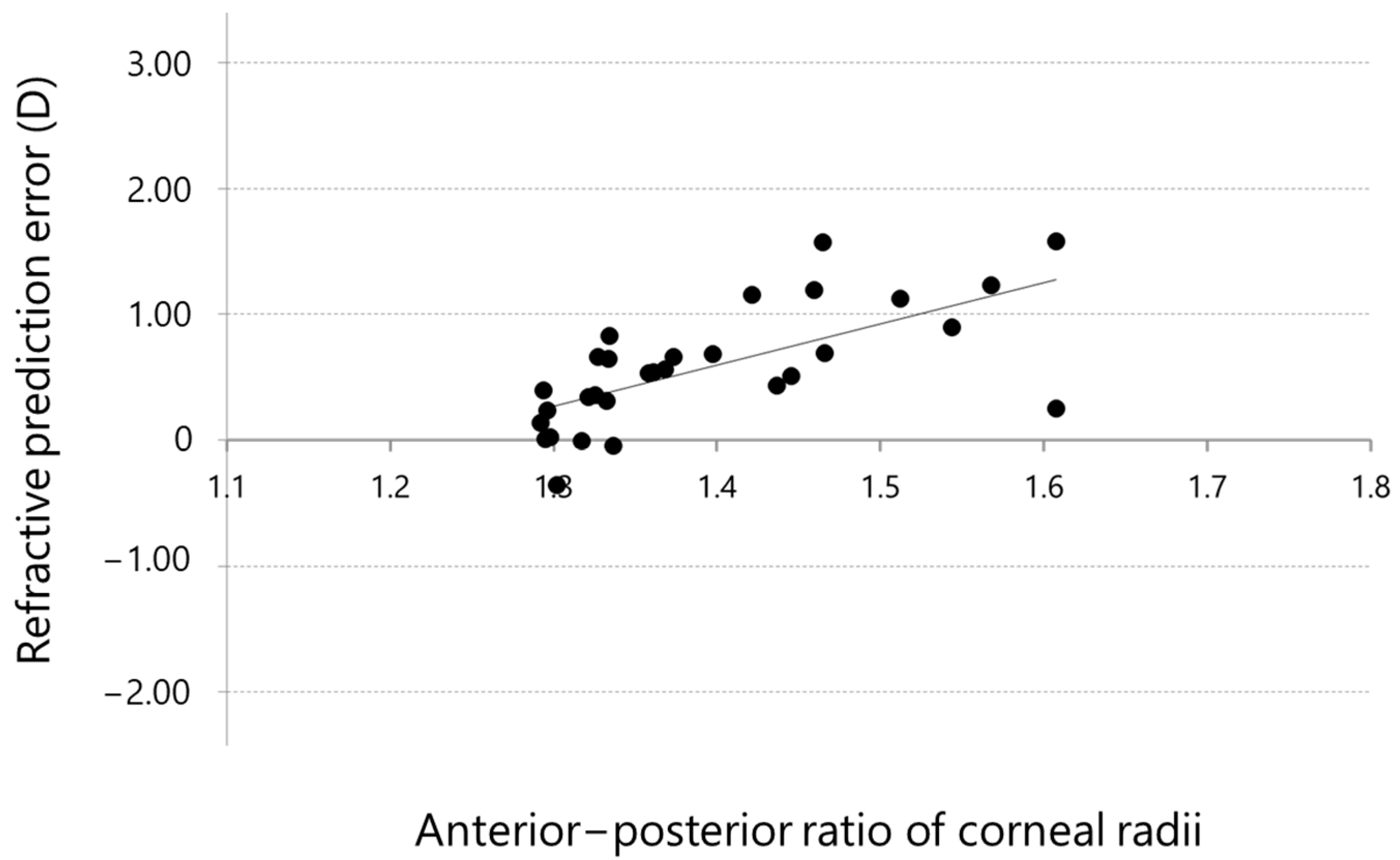
2.3. Estimation of Refractive Error in the Double-K Method Induced by the Anterior–Posterior Ratio of the Corneal Radii
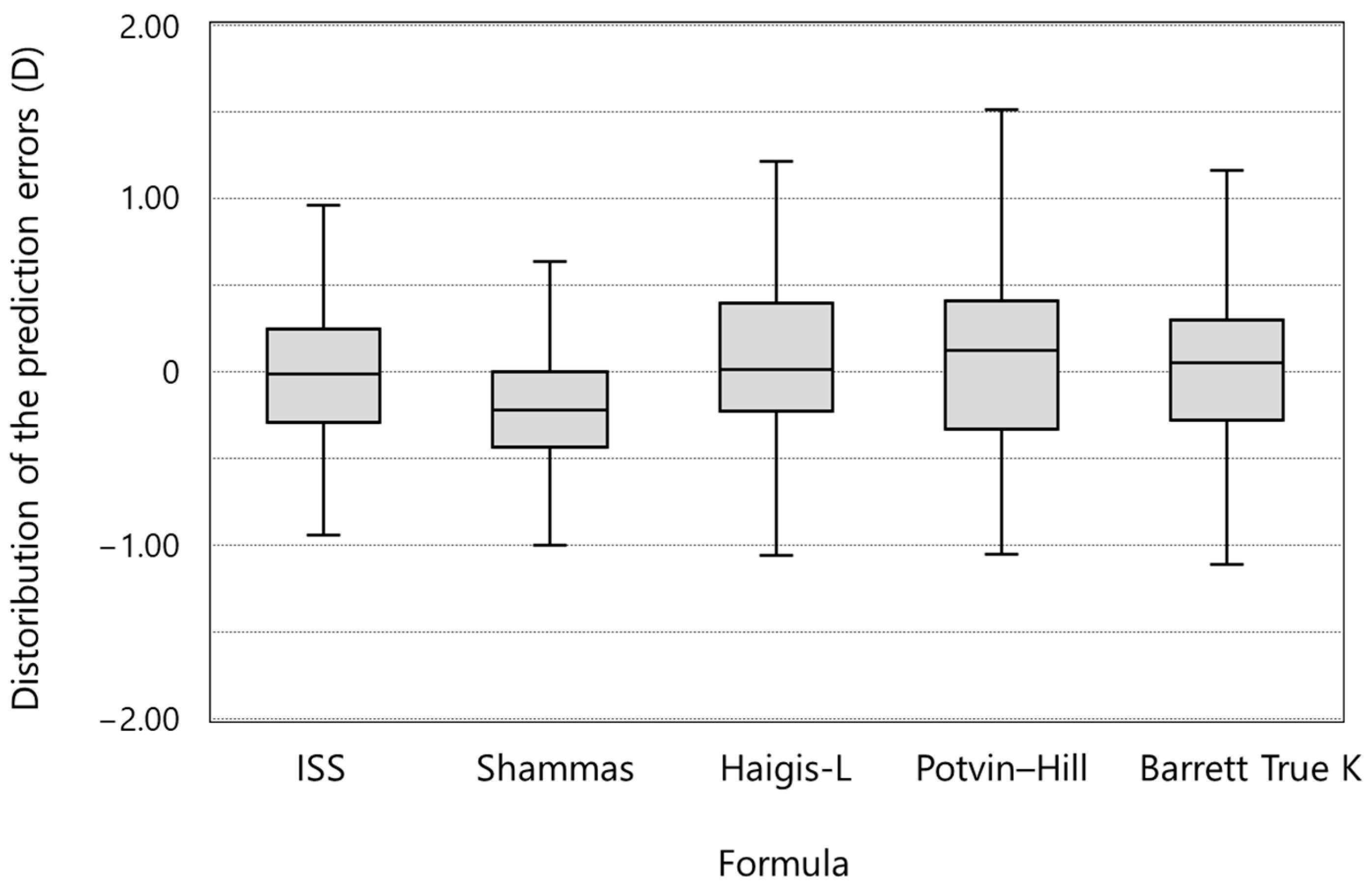
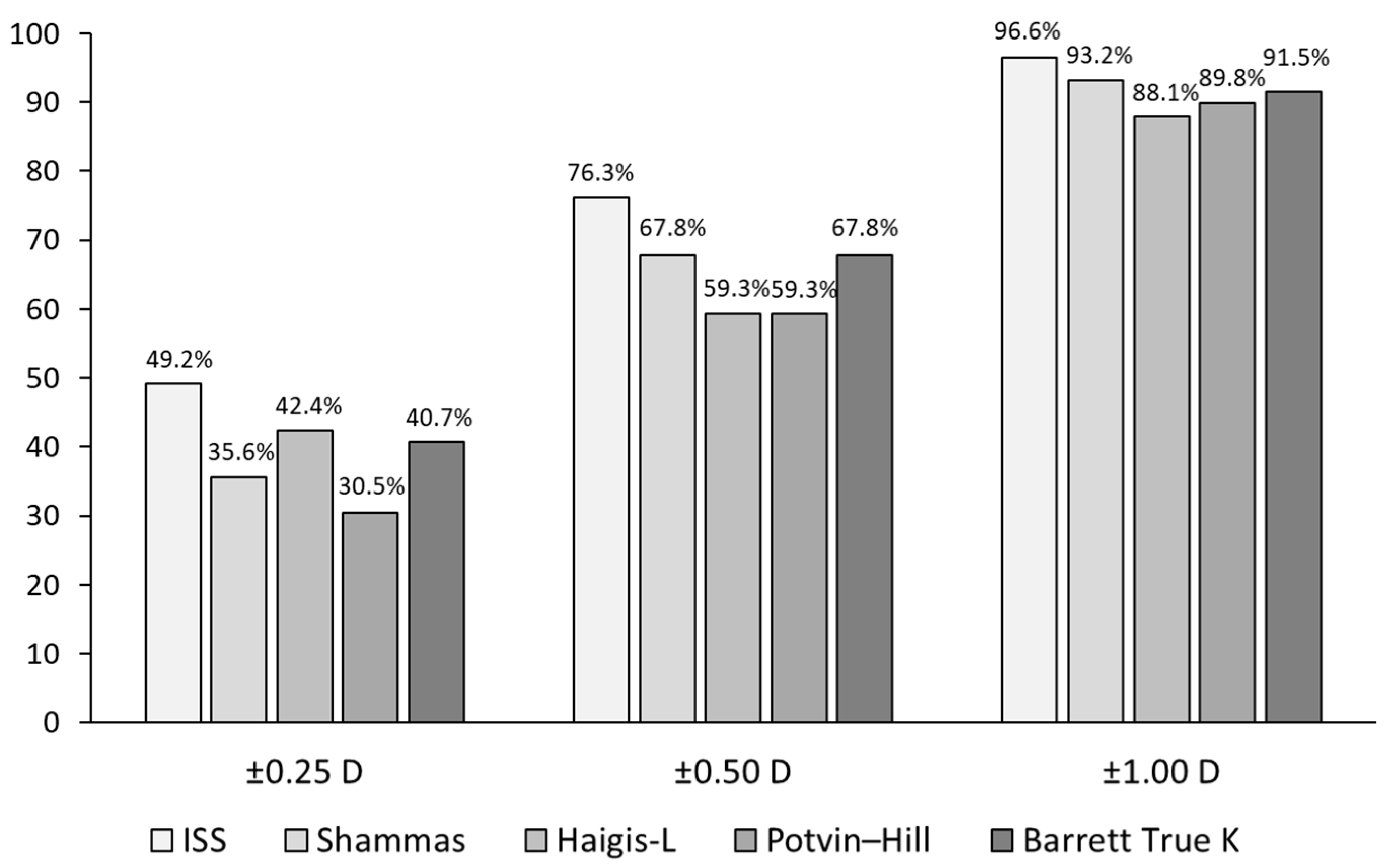
2.4. Intraocular Lens Power Calculations Using the ISS Method and Comparison of the Predictability of the ISS Method with That of Other Formulas or Methods
2.5. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoffer, K.J. Intraocular lens power calculation for eyes after refractive keratotomy. J. Refract. Surg. 1995, 11, 490–493. [Google Scholar] [CrossRef]
- Seitz, B.; Langenbucher, A.; Nguyen, N.X.; Kus, M.M.; Küchle, M. Underestimation of intraocular lens power for cataract surgery after myopic photorefractive keratectomy. Ophthalmology 1999, 106, 693–702. [Google Scholar] [CrossRef]
- Gimbel, H.V.; Sun, R.; Kaye, G.B. Refractive error in cataract surgery after previous refractive surgery. J. Cataract Refract. Surg. 2000, 26, 142–144. [Google Scholar] [CrossRef]
- Gimbel, H.V.; Sun, R.; Furlong, M.T.; van Westenbrugge, J.A.; Kassab, J. Accuracy and predictability of intraocular lens power calculation after photorefractive keratectomy. J. Cataract Refract. Surg. 2000, 26, 1147–1151. [Google Scholar] [CrossRef]
- Gimbel, H.V.; Sun, R. Accuracy and predictability of intraocular lens power calculation after laser in situ keratomileusis. J. Cataract Refract. Surg. 2001, 27, 571–576. [Google Scholar] [CrossRef]
- Retzlaff, J.A.; Sanders, D.R.; Kraff, M.C. Development of the SRK/T intraocular lens implant power calculation formula. J. Cataract Refract. Surg. 1990, 16, 333–340. [Google Scholar] [CrossRef]
- Aramberri, J. Intraocular lens power calculation after corneal refractive surgery, double-K method. J. Cataract Refract. Surg. 2003, 29, 2063–2068. [Google Scholar] [CrossRef]
- Holladay, J.T. Cataract Surgery in patients with previous keratorefractive surgery (RK, PRK and LASIK). Ophthalmic Pract. 1997, 15, 238–244. [Google Scholar]
- Hugger, P.; Kohnen, T.; LaRosa, F.A.; Holladay, J.T.; Koch, D.D. Comparison of changes in manifest refraction and corneal power after photorefractive keratectomy. Am. J. Ophthalmol. 2000, 129, 68–75. [Google Scholar] [CrossRef]
- Feiz, V.; Mannis, M.J.; Garcia-Ferrer, F.; Kandavel, G.; Darlington, J.K.; Kim, E.; Caspar, J.; Wang, J.-L.; Wang, W. Intraocular lens power calculation after laser in situ keratomileusis for myopia and hyperopia; a standardized approach. Cornea 2001, 20, 792–797. [Google Scholar] [CrossRef]
- Hamed, A.M.; Wang, L.; Misra, M.; Koch, D.D. A comparative analysis of five methods of determining corneal refractive power in eyes that have undergone myopic laser in situ keratomileusis. Ophthalmology 2002, 109, 651–658. [Google Scholar] [CrossRef]
- Keller, P.R.; McGhee, C.N.J.; Weed, K.H. Fourier analysis of corneal topography data after photorefractive keratectomy. J. Cataract Refract. Surg. 1998, 24, 1447–1455. [Google Scholar] [CrossRef]
- Celikkol, L.; Pavlopoulos, G.; Weinstein, B.; Celikkol, G.; Feldman, S.T. Calculation of intraocular lens power after radial keratotomy with computerized videokeratography. Am. J. Ophthalmol. 1995, 120, 739–750. [Google Scholar] [CrossRef]
- Rosa, N.; Capasso, L.; Romano, A. A new method of calculating intraocular lens power after photorefractive keratectomy. J. Refract. Surg. 2002, 18, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Shammas, H.J.; Shammas, M.C.; Garabet, A.; Kim, J.H.; Shammas, A.; LaBree, L. Correcting the corneal power measurements for intraocular lens power calculations after myopic laser in situ keratomileusis. Am. J. Ophthalmol. 2003, 36, 426–432. [Google Scholar] [CrossRef]
- Wang, L.; Booth, M.A.; Koch, D.D. Comparison of intraocular lens power calculation methods in eyes that have undergone LASIK. Ophthalmology 2004, 111, 1825–1831. [Google Scholar] [CrossRef]
- Camellin, M.; Calossi, A. A new formula for intraocular lens power calculation after refractive corneal surgery. J. Refract. Surg. 2006, 22, 187–199. [Google Scholar] [CrossRef]
- Masket, S.; Masket, S.E. Simple regression formula for intraocular lens power adjustment in eyes requiring cataract surgery after excimer laser photoablation. J. Cataract Refract. Surg. 2006, 32, 430–434. [Google Scholar] [CrossRef]
- Walter, K.A.; Gagnon, M.R.; Hoopes, P.C., Jr.; Dickinson, P.J. Accurate intraocular lens power calculation after myopic laser in situ keratomileusis, bypassing corneal power. J. Cataract Refract. Surg. 2006, 32, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Borasio, E.; Stevens, J.; Smith, G.T. Estimation of true corneal power after keratorefractive surgery in eyes requiring cataract surgery: BESSt formula. J. Cataract Refract. Surg. 2006, 32, 2004–2014. [Google Scholar] [CrossRef]
- Rabsilber, T.M.; Reuland, A.J.; Holzer, M.P.; Auffarth, G.U. Intraocular lens power calculation using ray tracing following excimer laser surgery. Eye 2007, 21, 697–701. [Google Scholar] [CrossRef] [Green Version]
- Shammas, H.J.; Shammas, M.C. No-history method of intraocular lens power calculation for cataract surgery after myopic laser in situ keratomileusis. J. Cataract Refract. Surg. 2007, 33, 31–36. [Google Scholar] [CrossRef]
- Einighammer, J.; Oltrup, T.; Bende, T.; Jean, B. Calculating intraocular lens geometry by real ray tracing. J. Refract. Surg. 2007, 23, 393–404. [Google Scholar] [CrossRef]
- Haigis, W. Intraocular lens calculation after refractive surgery for myopia: Haigis-L formula. J. Cataract Refract. Surg. 2008, 34, 1658–1663. [Google Scholar] [CrossRef]
- Potvin, R.; Hill, W. New algorithm for intraocular lens power calculations after myopic laser in situ keratomileusis based on rotating Scheimpflug camera data. J. Cataract Refract. Surg. 2015, 41, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Saiki, M.; Negishi, K.; Kato, N.; Arai, H.; Toda, I.; Torii, H.; Dogru, M.; Tsubota, K. A new central-peripheral corneal curvature method for intraocular lens power calculation after excimer laser refractive surgery. Acta Ophthalmol. 2013, 91, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Saiki, M.; Negishi, K.; Kato, N.; Ogino, R.; Arai, H.; Toda, I.; Dogru, M.; Tsubota, K. Modified double-K method for intraocular lens power calculation after excimer laser corneal refractive surgery. J. Cataract Refract. Surg. 2013, 39, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Barrett, G.D. An improved universal theoretical formula for intraocular lens power prediction. J. Cataract Refract. Surg. 1993, 19, 713–720. [Google Scholar] [CrossRef]
- Abulafia, A.; Hill, W.E.; Koch, D.D.; Wang, L.; Barrett, G.D. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J. Cataract Refract. Surg. 2016, 42, 363–369. [Google Scholar] [CrossRef]
- Wang, L.; Hill, W.E.; Koch, D.D. Evaluation of intraocular lens power prediction methods using the American Society of Cataract and Refractive Surgeons Post-Keratorefractive Intraocular Lens Power Calculator. J. Cataract Refract. Surg. 2010, 36, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tang, M.; Huang, D.; Weikert, M.P.; Koch, D.D. Comparison of Newer Intraocular Lens Power Calculation Methods for Eyes after Corneal Refractive Surgery. Ophthalmology 2015, 122, 2443–2449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ianchulev, T.; Hoffer, K.J.; Yoo, S.H.; Chang, D.F.; Breen, M.; Padrick, T.; Tran, D.B. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology 2014, 121, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K.; Kamiya, K.; Iida, Y.; Shoji, N. Comparison of Predictability Using Barrett Universal II and SRK/T Formulas according to Keratometry. J. Ophthalmol. 2020, 2020, 7625725. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Post-LASIK (n = 30) |
|---|---|
| Mean ± SD (Range) | |
| Age (years) | 55.4 ± 10.3 (22–71) |
| Axial length (mm) | 26.75 ± 1.67 (24.81–29.63) |
| Mean K by IOL master (D) Mean corneal radius of curvature by IOL master (mm) (keratometric index = 1.3375) | 38.90 ± 2.35 (33.08–41.88) 8.68 ± 0.56 (8.06–10.20) |
| Mean anterior corneal radius of curvature by Pentacam (mm) | 8.73 ± 0.58 (7.97–10.45) |
| Mean posterior corneal radius of curvature by Pentacam (mm) | 6.33 ± 0.26 (5.71–6.88) |
| Mean ± SD (Range) | |
|---|---|
| Age (years) | 59.0 ± 9.3 (36–77) |
| Axial length (mm) | 27.01 ± 1.94 (23.99–32.76) |
| Mean K by IOL master (D) Mean corneal radius of curvature by IOL master (mm)(keratometric index = 1.3375) | 38.95 ± 2.54 (33.84–43.25) 8.66 ± 0.57 (7.80–9.97) |
| Mean anterior corneal radius of curvature by Pentacam (mm) | 8.68 ± 0.55 (7.81–9.86) |
| Mean posterior corneal radius of curvature by Pentacam (mm) | 6.36 ± 0.29 (5.70–7.31) |
| TNP (4.0 mm) by Pentacam (D) | 37.30 ± 2.55 (31.60–41.80) |
| Formula/Method | Refractive Prediction Error (D) | ||||
|---|---|---|---|---|---|
| Numerical | Absolute | ||||
| Mean ± SD (Range) | p-Value | Mean ± SD (Range) | Median | p-Value vs. ISS | |
| ISS | −0.02 ± 0.45 | 0.770 | 0.35 ± 0.27 | 0.29 | N/A |
| (−1.11–0.96) | (0.01–1.11) | ||||
| Shammas | −0.20 ± 0.54 | 0.005 * | 0.45 ± 0.36 | 0.29 | 0.028 * |
| (−1.42–1.36) | (0.00–1.42) | ||||
| Haigis-L | 0.07 ± 0.59 | 0.361 | 0.45 ± 0.38 | 0.37 | 0.199 |
| (−1.26–1.59) | (0.00–1.59) | ||||
| Potvin–Hill | 0.13 ± 0.65 | 0.124 | 0.50 ± 0.43 | 0.38 | 0.025 * |
| (−1.05–2.34) | (0.02–2.34) | ||||
| Barrett True K | 0.02 ± 0.58 | 0.754 | 0.43 ± 0.39 | 0.28 | 0.581 |
| (−1.16–1.61) | (0.03–1.61) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iida, Y.; Shimizu, K.; Shoji, N. Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior–Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method. J. Clin. Med. 2022, 11, 522. https://doi.org/10.3390/jcm11030522
Iida Y, Shimizu K, Shoji N. Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior–Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method. Journal of Clinical Medicine. 2022; 11(3):522. https://doi.org/10.3390/jcm11030522
Chicago/Turabian StyleIida, Yoshihiko, Kimiya Shimizu, and Nobuyuki Shoji. 2022. "Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior–Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method" Journal of Clinical Medicine 11, no. 3: 522. https://doi.org/10.3390/jcm11030522
APA StyleIida, Y., Shimizu, K., & Shoji, N. (2022). Development of a New Method for Calculating Intraocular Lens Power after Myopic Laser In Situ Keratomileusis by Combining the Anterior–Posterior Ratio of the Corneal Radius of the Curvature with the Double-K Method. Journal of Clinical Medicine, 11(3), 522. https://doi.org/10.3390/jcm11030522