
Diet/Nutrition: Ready to Transition from a Cancer Recurrence/Prevention Strategy to a Chronic Pain Management Modality for Cancer Survivors?

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
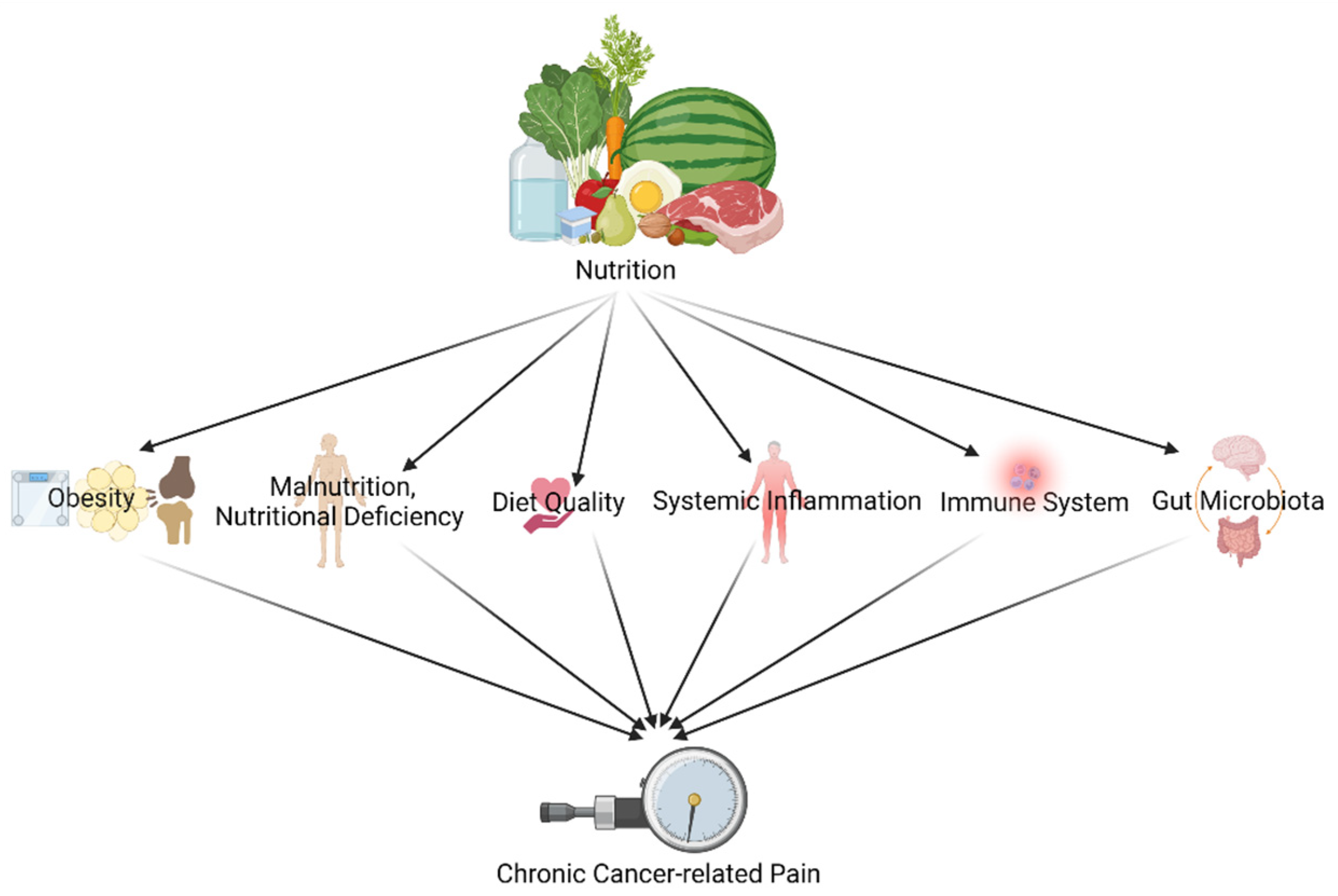
3. Pain and Nutrition in Cancer Survivors: An Update from Cancer and Chronic Pain Literature
3.1. Impact of Diet and Nutrition on Pain in Cancer Survivors through Obesity
3.2. Impact of Diet and Nutrition on Pain in Cancer Survivors through Malnutrition, Nutritional Deficiency, and Diet Quality
3.3. Impact of Diet and Nutrition on Pain in Cancer Survivors through the Immune System and Systemic Inflammation
3.4. Impact of Diet and Nutrition on Pain in Cancer Survivors through Gut Microbiota
4. How Can We Implement This Knowledge in Clinical Practice?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Brown, M.; Farquhar-Smith, P. Pain in cancer survivors; filling in the gaps. Br. J. Anaesth. 2017, 119, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, W.; Rosenthal, D.S. Oncology Acupuncture for Chronic Pain in Cancer Survivors: A Reflection on the American Society of Clinical Oncology Chronic Pain Guideline. Hematol. Oncol. Clin. N. Am. 2018, 32, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Mailis, A.; Tepperman, P.S.; Hapidou, E.G. Chronic pain: Evolution of clinical definitions and implications for practice. Psychol. Inj. Law 2020, 13, 412–426. [Google Scholar] [CrossRef]
- Leysen, L.; Beckwée, D.; Nijs, J.; Pas, R.; Bilterys, T.; Vermeir, S.; Adriaenssens, N. Risk factors of pain in breast cancer survivors: A systematic review and meta-analysis. Support. Care Cancer 2017, 25, 3607–3643. [Google Scholar] [CrossRef]
- Van Den Beuken-Van, M.H.; Hochstenbach, L.M.; Joosten, E.A.; Tjan-Heijnen, V.C.; Janssen, D.J. Update on Prevalence of Pain in Patients With Cancer: Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef] [Green Version]
- Glare, P.A.; Davies, P.S.; Finlay, E.; Gulati, A.; Lemanne, D.; Moryl, N.; Oeffinger, K.C.; Paice, J.; Stubblefield, M.D.; Syrjala, K.L. Pain in Cancer Survivors. J. Clin. Oncol. 2014, 32, 1739–1747. [Google Scholar] [CrossRef] [Green Version]
- Burton, A.W.; Fanciullo, G.J.; Beasley, R.D.; Fisch, M.J. Chronic Pain in the Cancer Survivor: A New Frontier. Pain Med. 2007, 8, 189–198. [Google Scholar] [CrossRef]
- Azizoddin, D.R.; Schreiber, K.; Beck, M.R.; Enzinger, A.C.; Hruschak, V.; Darnall, B.D.; Edwards, R.R.; Allsop, M.J.; Tulsky, J.A.; Boyer, E.; et al. Chronic pain severity, impact, and opioid use among patients with cancer: An analysis of biopsychosocial factors using the CHOIR learning health care system. Cancer 2021, 127, 3254–3263. [Google Scholar] [CrossRef]
- Habib, A.S.; Kertai, M.; Cooter, M.; Greenup, A.R.; Hwang, S. Risk factors for severe acute pain and persistent pain after surgery for breast cancer: A prospective observational study. Reg. Anesth. Pain Med. 2019, 44, 192–199. [Google Scholar] [CrossRef]
- Virizuela, J.A.; Camblor-Álvarez, M.; Luengo-Pérez, L.M.; Grande, E.; Álvarez-Hernández, J.; Sendrós-Madroño, M.J.; Jiménez-Fonseca, P.; Peris, M.C.; Ocón-Bretón, M.J. Nutritional support and parenteral nutrition in cancer patients: An expert consensus report. Clin. Transl. Oncol. 2018, 20, 619–629. [Google Scholar] [CrossRef]
- Inglis, J.E.; Lin, P.-J.; Kerns, S.L.; Kleckner, I.R.; Kleckner, A.S.; Castillo, A.D.; Mustian, K.M.; Peppone, L.J. Nutritional Interventions for Treating Cancer-Related Fatigue: A Qualitative Review. Nutr. Cancer 2019, 71, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Braakhuis, A.; Campion, P.; Bishop, K. The Effects of Dietary Nutrition Education on Weight and Health Biomarkers in Breast Cancer Survivors. Med. Sci. 2017, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, C.L.; Flatt, S.W.; Byers, T.E.; Colditz, G.A.; Demark-Wahnefried, W.; Ganz, P.A.; Wolin, K.Y.; Elias, A.; Krontiras, H.; Liu, J.; et al. Results of the Exercise and Nutrition to Enhance Recovery and Good Health for You (ENERGY) trial: A behavioral weight loss intervention in overweight or obese breast cancer survivors. J. Clin. Oncol. 2015, 33, 3169. [Google Scholar] [CrossRef]
- Doyle, C.; Kushi, L.H.; Byers, T.; Courneya, K.S.; Demark-Wahnefried, W.; Grant, B.; McTiernan, A.; Rock, C.L.; Thompson, C.; Gansler, T.; et al. Nutrition and physical activity during and after cancer treatment: An American Cancer Society guide for informed choices. CA Cancer J. Clin. 2006, 56, 323–353. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Pinilla, F.; Gomez, A.G. The influence of dietary factors in central nervous system plasticity and injury recovery. PM&R 2011, 3 (Suppl. S1), S111–S116. [Google Scholar]
- Fernandez-Lao, C.; Cantarero-Villanueva, I.; Fernández-de-Las-Peñas, C.; Del-Moral-Avila, R.; Arendt-Nielsen, L.; Arroyo-Morales, M. Myofascial trigger points in neck and shoulder muscles and widespread pressure pain hypersensitivtiy in patients with postmastectomy pain: Evidence of peripheral and central sensitization. Clin. J. Pain 2010, 26, 798–806. [Google Scholar] [CrossRef]
- Sánchez-Jiménez, A.; Cantarero-Villanueva, I.; Molina-Barea, R.; Fernández-Lao, C.; Galiano-Castillo, N.; Arroyo-Morales, M. Widespread Pressure Pain Hypersensitivity and Ultrasound Imaging Evaluation of Abdominal Area after Colon Cancer Treatment. Pain Med. 2014, 15, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Comino, L.; Fernández-Lao, C.; Castro-Martín, E.; Lozano-Lozano, M.; Cantarero-Villanueva, I.; Arroyo-Morales, M.; Martín-Martín, L. Myofascial pain, widespread pressure hypersensitivity, and hyperalgesia in the face, neck, and shoulder regions, in survivors of head and neck cancer. Support. Care Cancer 2019, 28, 2891–2898. [Google Scholar] [CrossRef]
- Leysen, L.; Adriaenssens, N.; Nijs, J.; Pas, R.; Bilterys, T.; Vermeir, S.; Lahousse, A.; Beckwée, D. Chronic Pain in Breast Cancer Survivors: Nociceptive, Neuropathic, or Central Sensitization Pain? Pain Pract. 2018, 19, 183–195. [Google Scholar] [CrossRef]
- Chao, C.; Bhatia, S.; Xu, L.; Cannavale, K.L.; Wong, F.L.; Huang, P.S.; Cooper, R.; Armenian, S.H. Chronic Comorbidities Among Survivors of Adolescent and Young Adult Cancer. J. Clin. Oncol. 2020, 38, 3161. [Google Scholar] [CrossRef]
- Paice, J.A.; Portenoy, R.; Lacchetti, C.; Campbell, T.; Cheville, A.; Citron, M.; Constine, L.S.; Cooper, A.; Glare, P.; Keefe, F.; et al. Management of chronic pain in survivors of adult cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 3325–3345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, C.R.; Hart-Johnson, T.; Loeffler, D.R. Cancer-related chronic pain: Examining quality of life in diverse cancer survivors. Cancer 2011, 117, 1994–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Groef, A.; Penen, F.; Dams, L.; Van der Gucht, E.; Nijs, J.; Meeus, M. Best-Evidence Rehabilitation for Chronic Pain Part 2: Pain during and after Cancer Treatment. J. Clin. Med. 2019, 8, 979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjørklund, G.; Aaseth, J.; Doşa, M.D.; Pivina, L.; Dadar, M.; Pen, J.J.; Chirumbolo, S. Does diet play a role in reducing nociception related to inflammation and chronic pain? Nutrition 2019, 66, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Audette, J.F.; Bailey, A. Integrative Pain Medicine: The Science and Practice of Complementary and Alternative Medicine in Pain Management; Springer Science & Business Media: Totowa, NJ, USA, 2008. [Google Scholar]
- Hendrix, J.; Nijs, J.; Ickmans, K.; Godderis, L.; Ghosh, M.; Polli, A. The Interplay between Oxidative Stress, Exercise, and Pain in Health and Disease: Potential Role of Autonomic Regulation and Epigenetic Mechanisms. Antioxidants 2020, 9, 1166. [Google Scholar] [CrossRef]
- Yilmaz, S.T.; Elma, Ö.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Nutrition/Dietary Supplements and Chronic Pain in Patients with Cancer and Survivors of Cancer: A Systematic Review and Research Agenda. Pain Physician 2021, 24, 335–344. [Google Scholar]
- Tapsell, L.C. Dietary behaviour changes to improve nutritional quality and health outcomes. Chronic Dis. Transl. Med. 2017, 3, 154–158. [Google Scholar] [CrossRef]
- Ren, K.; Dubner, R. Interactions between the immune and nervous systems in pain. Nat. Med. 2010, 16, 1267–1276. [Google Scholar] [CrossRef]
- Malafoglia, V.; Ilari, S.; Vitiello, L.; Tenti, M.; Balzani, E.; Muscoli, C.; Raffaeli, W.; Bonci, A. The Interplay between Chronic Pain, Opioids, and the Immune System. Neuroscientist 2021, 10738584211030493. [Google Scholar] [CrossRef]
- Parekh, N.; Chandran, U.; Bandera, E.V. Obesity in Cancer Survival. Annu. Rev. Nutr. 2012, 32, 311–342. [Google Scholar] [CrossRef] [Green Version]
- Buch, K.; Gunmalm, V.; Andersson, M.; Schwarz, P.; Brøns, C. Effect of chemotherapy and aromatase inhibitors in the adjuvant treatment of breast cancer on glucose and insulin metabolism-A systematic review. Cancer Med. 2019, 8, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Cox-Martin, E.; Trahan, L.H.; Cox, M.G.; Dougherty, P.M.; Lai, E.A.; Novy, D.M. Disease burden and pain in obese cancer patients with chemotherapy-induced peripheral neuropathy. Support. Care Cancer 2017, 25, 1873–1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morelhão, P.K.; Tufik, S.; Andersen, M.L. The Interactions Between Obesity, Sleep Quality, and Chronic Pain. J. Clin. Sleep Med. 2018, 14, 1965–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mínguez-Olaondo, A.; Martínez-Valbuena, I.; Romero, S.; Frühbeck, G.; Luquin, M.R.; Martínez-Vila, E.; Irimia, P. Excess abdominal fat is associated with cutaneous allodynia in individuals with migraine: A prospective cohort study. J. Headache Pain 2020, 21, 9. [Google Scholar] [CrossRef]
- Emery, C.F.; Olson, K.L.; Bodine, A.; Lee, V.; Habash, D.L. Dietary intake mediates the relationship of body fat to pain. Pain 2017, 158, 273–277. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ippolito, M.; Monge, T.; Violi, R.; Cappello, P.; Ferrocino, I.; Cocolin, L.S.; De Francesco, A.; Bo, S.; Finocchiaro, C. Gut microbiota composition after diet and probiotics in overweight breast cancer survivors: A randomized open-label pilot intervention trial. Nutrition 2020, 74, 110749. [Google Scholar] [CrossRef]
- Minerbi, A.; Gonzalez, E.; Brereton, N.J.; Anjarkouchian, A.; Dewar, K.; Fitzcharles, M.-A.; Chevalier, S.; Shir, Y. Altered microbiome composition in individuals with fibromyalgia. Pain 2019, 160, 2589–2602. [Google Scholar] [CrossRef] [Green Version]
- Timmins, H.C.; Mizrahi, D.; Li, T.; Kiernan, M.C.; Goldstein, D.; Park, S.B. Metabolic and lifestyle risk factors for chemotherapy-induced peripheral neuropathy in taxane and platinum-treated patients: A systematic review. J. Cancer Surviv. 2021, 1–15. [Google Scholar] [CrossRef]
- Forsythe, L.P.; Alfano, C.M.; George, S.M.; McTiernan, A.; Baumgartner, K.B.; Bernstein, L.; Ballard-Barbash, R. Pain in long-term breast cancer survivors: The role of body mass index, physical activity, and sedentary behavior. Breast Cancer Res. Treat. 2013, 137, 617–630. [Google Scholar] [CrossRef] [Green Version]
- Mosher, C.E.; Sloane, R.; Morey, M.C.; Snyder, D.C.; Cohen, H.J.; Miller, P.E.; Demark-Wahnefried, W. Associations between lifestyle factors and quality of life among older long-term breast, prostate, and colorectal cancer survivors. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2009, 115, 4001–4009. [Google Scholar] [CrossRef]
- Petrovchich, I.; Kober, K.M.; Wagner, L.; Paul, S.M.; Abrams, G.; Chesney, M.A.; Topp, K.; Smoot, B.; Schumacher, M.; Conley, Y.P. Deleterious effects of higher body mass index on subjective and objective measures of chemotherapy-induced peripheral neuropathy in cancer survivors. J. Pain Symptom Manag. 2019, 58, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Sheng, J.Y.; Santa-Maria, C.A.; Blackford, A.L.; Lim, D.; Carpenter, A.; Smith, K.L.; Cohen, G.I.; Coughlin, J.; Appel, L.J.; Stearns, V. The impact of weight loss on physical function and symptoms in overweight or obese breast cancer survivors: Results from POWER-remote. J. Cancer Surviv. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L. To create a consensus on malnutrition diagnostic criteria: A report from the Global Leadership Initiative on Malnutrition (GLIM) meeting at the ESPEN Congress 2016. J. Parenter. Enter. Nutr. 2017, 41, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Prevost, V.; Joubert, C.; Heutte, N.; Babin, E. Assessment of nutritional status and quality of life in patients treated for head and neck cancer. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Argiles, J.M. Cancer-associated malnutrition. Eur. J. Oncol. Nurs. 2005, 9 (Suppl. S2), S39–S50. [Google Scholar] [CrossRef]
- Field, R.; Pourkazemi, F.; Turton, J.; Rooney, K. Dietary Interventions Are Beneficial for Patients with Chronic Pain: A Systematic Review with Meta-Analysis. Pain Med. 2021, 22, 694–714. [Google Scholar] [CrossRef]
- Mohammadi, S.; Sulaiman, S.; Koon, P.B.; Amani, R.; Hosseini, S.M. Association of Nutritional Status with Quality of Life in Breast Cancer Survivors. Asian Pac. J. Cancer Prev. 2013, 14, 7749–7755. [Google Scholar] [CrossRef] [Green Version]
- Capra, S.; Ferguson, M.; Ried, K. Cancer: Impact of nutrition intervention outcome—Nutrition issues for patients. Nutrition 2001, 17, 769–772. [Google Scholar] [CrossRef]
- De Vries, Y.; Van Den Berg, M.; De Vries, J.; Boesveldt, S.; de Kruif, J.T.C.; Buist, N.; Haringhuizen, A.; Los, M.; Sommeijer, D.; Timmer-Bonte, J. Differences in dietary intake during chemotherapy in breast cancer patients compared to women without cancer. Supportive Care Cancer 2017, 25, 2581–2591. [Google Scholar] [CrossRef] [Green Version]
- Petzel, M.Q.B.; Hoffman, L. Nutrition Implications for Long-Term Survivors of Pancreatic Cancer Surgery. Nutr. Clin. Pract. 2017, 32, 588–598. [Google Scholar] [CrossRef]
- Hu, Y.; Kim, H.-I.; Hyung, W.J.; Song, K.J.; Lee, J.H.; Kim, Y.M.; Noh, S.H. Vitamin B12 deficiency after gastrectomy for gastric cancer: An analysis of clinical patterns and risk factors. Ann. Surg. 2013, 258, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Philpot, U.; Johnson, M. Diet therapy in the management of chronic pain: Better diet less pain? Pain Manag. 2019, 9, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-H.; Kang, J.W.; Lee, T.H. Therapeutic options for aromatase inhibitor-associated arthralgia in breast cancer survivors: A systematic review of systematic reviews, evidence mapping, and network meta-analysis. Maturitas 2018, 118, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Dragan, S.; Șerban, M.-C.; Damian, G.; Buleu, F.; Valcovici, M.; Christodorescu, R. Dietary Patterns and Interventions to Alleviate Chronic Pain. Nutrients 2020, 12, 2510. [Google Scholar] [CrossRef]
- Niravath, P.; Chen, B.; Chapman, J.-A.W.; Agarwal, S.K.; Welschhans, R.L.; Bongartz, T.; Kalari, K.R.; Shepherd, L.E.; Bartlett, J.; Pritchard, K. Vitamin D levels, vitamin D receptor polymorphisms, and inflammatory cytokines in aromatase inhibitor-induced Arthralgias: An analysis of CCTG MA. 27. Clin. Breast Cancer 2018, 18, 78–87. [Google Scholar] [CrossRef]
- Martin, K.R.; Reid, D.M. Is there a role for vitamin D in the treatment of chronic pain? Ther. Adv. Musculoskelet. Dis. 2017, 9, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; McCall, C. The role of vitamin C in the treatment of pain: New insights. J. Transl. Med. 2017, 15, 77. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Vissers, M.C.M.; Cook, J.S. The Effect of Intravenous Vitamin C on Cancer- and Chemotherapy-Related Fatigue and Quality of Life. Front. Oncol. 2014, 4, 283. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahman, K.; Hackshaw, K. Nutritional Supplements for the Treatment of Neuropathic Pain. Biomedicines 2021, 9, 674. [Google Scholar] [CrossRef]
- Schlesinger, S.; Walter, J.; Hampe, J.; von Schönfels, W.; Hinz, S.; Küchler, T.; Jacobs, G.; Schafmayer, C.; Nöthlings, U. Lifestyle factors and health-related quality of life in colorectal cancer survivors. Cancer Causes Control. 2014, 25, 99–110. [Google Scholar] [CrossRef]
- Porciello, G.; Montagnese, C.; Crispo, A.; Grimaldi, M.; Libra, M.; Vitale, S.; Palumbo, E.; Pica, R.; Calabrese, I.; Cubisino, S. Mediterranean diet and quality of life in women treated for breast cancer: A baseline analysis of DEDiCa multicentre trial. PLoS ONE 2020, 15, e0239803. [Google Scholar] [CrossRef] [PubMed]
- Wayne, S.J.; Baumgartner, K.; Baumgartner, R.N.; Bernstein, L.; Bowen, D.J.; Ballard-Barbash, R. Diet quality is directly associated with quality of life in breast cancer survivors. Breast Cancer Res. Treat. 2006, 96, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Song, S.; Moon, S.-E.; Jung, S.-Y.; Lee, E.S.; Kim, Z.; Youn, H.J.; Cho, J.; Yoo, Y.B.; Lee, S.K. Adherence to the American Cancer Society guidelines for cancer survivors and health-related quality of life among breast cancer survivors. Nutrients 2019, 11, 2924. [Google Scholar] [CrossRef] [Green Version]
- Lei, Y.-Y.; Ho, S.C.; Cheng, A.; Kwok, C.; Lee, C.-K.I.; Cheung, K.L.; Lee, R.; Loong, H.H.; He, Y.-Q.; Yeo, W. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Guideline is associated with better health-related quality of life among Chinese patients with breast cancer. J. Natl. Compr. Cancer Netw. 2018, 16, 275–285. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K. American Cancer Society guideline for diet and physical activity for cancer prevention. CA Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective; Continuous Update Project Expert Report; World Cancer Research Fund: London, UK, 2018. [Google Scholar]
- Christensen, M.A.; Smoak, P.; Lisano, J.K.; Hayward, R.; Coronado, C.; Kage, K.; Shackelford, D.; Stewart, L.K. Cardiorespiratory fitness, visceral fat, and body fat, but not dietary inflammatory index, are related to C-reactive protein in cancer survivors. Nutr. Health 2019, 25, 195–202. [Google Scholar] [CrossRef]
- Alfano, C.M.; Imayama, I.; Neuhouser, M.L.; Kiecolt-Glaser, J.K.; Smith, A.W.; Meeske, K.; McTiernan, A.; Bernstein, L.; Baumgartner, K.B.; Ulrich, C.M. Fatigue, inflammation, and ω-3 and ω-6 fatty acid intake among breast cancer survivors. J. Clin. Oncol. 2012, 30, 1280. [Google Scholar] [CrossRef]
- Kurtys, E.; Eisel, U.; Verkuyl, J.; Broersen, L.; Dierckx, R.; de Vries, E. The combination of vitamins and omega-3 fatty acids has an enhanced anti-inflammatory effect on microglia. Neurochem. Int. 2016, 99, 206–214. [Google Scholar] [CrossRef]
- Guest, D.D.; Evans, E.M.; Rogers, L.Q. Diet components associated with perceived fatigue in breast cancer survivors. Eur. J. Cancer Care 2013, 22, 51–59. [Google Scholar] [CrossRef]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef]
- Zuniga, K.E.; Parma, D.L.; Muñoz, E.; Spaniol, M.; Wargovich, M.; Ramirez, A.G. Dietary intervention among breast cancer survivors increased adherence to a Mediterranean-style, anti-inflammatory dietary pattern: The Rx for Better Breast Health Randomized Controlled Trial. Breast Cancer Res. Treat. 2019, 173, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. JAMA 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, S.M.; Neuhouser, M.L.; Mayne, S.T.; Irwin, M.L.; Albanes, D.; Gail, M.H.; Alfano, C.M.; Bernstein, L.; McTiernan, A.; Reedy, J. Postdiagnosis diet quality is inversely related to a biomarker of inflammation among breast cancer survivors. Cancer Epidemiol. Prev. Biomark. 2010, 19, 2220–2228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orchard, T.S.; Andridge, R.R.; Yee, L.D.; Lustberg, M.B. Diet quality, inflammation, and quality of life in breast cancer survivors: A cross-sectional analysis of pilot study data. J. Acad. Nutr. Diet. 2018, 118, 578–588.e1. [Google Scholar] [CrossRef]
- Nashed, M.G.; Balenko, M.D.; Singh, G. Cancer-induced oxidative stress and pain. Current Pain Headache Reports 2014, 18, 384. [Google Scholar] [CrossRef]
- Shim, H.S.; Bae, C.; Wang, J.; Lee, K.-H.; Hankerd, K.M.; Kim, H.K.; Chung, J.M.; La, J.-H. Peripheral and central oxidative stress in chemotherapy-induced neuropathic pain. Mol. Pain 2019, 15, 1744806919840098. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Ma, J.; Lu, W. The Significance of Mitochondrial Dysfunction in Cancer. Int. J. Mol. Sci. 2020, 21, 5598. [Google Scholar] [CrossRef]
- Sui, B.-D.; Xu, T.-Q.; Liu, J.-W.; Wei, W.; Zheng, C.-X.; Guo, B.-L.; Wang, Y.-Y.; Yang, Y.-L. Understanding the role of mitochondria in the pathogenesis of chronic pain. Postgrad. Med. J. 2013, 89, 709–714. [Google Scholar] [CrossRef]
- Doyle, T.M.; Salvemini, D. Mini-Review: Mitochondrial dysfunction and chemotherapy-induced neuropathic pain. Neurosci. Lett. 2021, 760, 136087. [Google Scholar] [CrossRef]
- Totsch, S.K.; Waite, M.E.; Sorge, R.E. Dietary influence on pain via the immune system. Prog. Mol. Biol. Transl. Sci. 2015, 131, 435–469. [Google Scholar]
- Skouroliakou, M.; Grosomanidis, D.; Massara, P.; Kostara, C.; Papandreou, P.; Ntountaniotis, D.; Xepapadakis, G. Serum antioxidant capacity, biochemical profile and body composition of breast cancer survivors in a randomized Mediterranean dietary intervention study. Eur. J. Nutr. 2018, 57, 2133–2145. [Google Scholar] [CrossRef] [PubMed]
- Butalla, A.C.; Crane, T.E.; Patil, B.; Wertheim, B.C.; Thompson, P.; Thomson, C.A. Effects of a Carrot Juice Intervention on Plasma Carotenoids, Oxidative Stress, and Inflammation in Overweight Breast Cancer Survivors. Nutr. Cancer 2012, 64, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Schatz, A.A.; Oliver, T.K.; Swarm, R.A.; Paice, J.A.; Darbari, D.S.; Dowell, D.; Meghani, S.H.; Winckworth-Prejsnar, K.; Bruera, E.; Plovnick, R.M.; et al. Bridging the Gap Among Clinical Practice Guidelines for Pain Management in Cancer and Sickle Cell Disease. J. Natl. Compr. Cancer Netw. 2020, 18, 392–399. [Google Scholar] [CrossRef] [Green Version]
- Hartung, J.E.; Eskew, O.; Wong, T.; Tchivileva, I.E.; Oladosu, F.A.; O’Buckley, S.C.; Nackley, A.G. Nuclear factor-kappa B regulates pain and COMT expression in a rodent model of inflammation. Brain Behav. Immun. 2015, 50, 196–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolberg, M.; Pedersen, S.; Bastani, N.E.; Carlsen, H.; Blomhoff, R.; Paur, I. Tomato paste alters NF-κB and cancer-related mRNA expression in prostate cancer cells, xenografts, and xenograft microenvironment. Nutr. Cancer 2015, 67, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Deleemans, J.M.; Chleilat, F.; Reimer, R.A.; Henning, J.-W.; Baydoun, M.; Piedalue, K.-A.; McLennan, A.; Carlson, L.E. The chemo-gut study: Investigating the long-term effects of chemotherapy on gut microbiota, metabolic, immune, psychological and cognitive parameters in young adult Cancer survivors; study protocol. BMC Cancer 2019, 19, 1243. [Google Scholar] [CrossRef] [Green Version]
- Song, B.C.; Bai, J. Microbiome-gut-brain axis in cancer treatment-related psychoneurological toxicities and symptoms: A systematic review. Supportive Care Cancer 2021, 29, 605–617. [Google Scholar] [CrossRef]
- Kelly, D.L.; Lyon, D.E.; Yoon, S.L.; Horgas, A.L. The microbiome and cancer: Implications for oncology nursing science. Cancer Nurs. 2016, 39, E56–E62. [Google Scholar] [CrossRef]
- Guo, R.; Chen, L.-H.; Xing, C.; Liu, T. Pain regulation by gut microbiota: Molecular mechanisms and therapeutic potential. Br. J. Anaesth. 2019, 123, 637–654. [Google Scholar] [CrossRef] [Green Version]
- Santoni, M.; Miccini, F.; Battelli, N. Gutmicrobiota, immunity and pain. Immunol. Lett. 2021, 229, 44–47. [Google Scholar] [CrossRef]
- Nijs, J.; Yilmaz, S.T.; Elma, O.; Tatta, J.; Mullie, P.; Vanderweeen, L.; Clarys, P.; Deliens, T.; Coppieters, I.; Weltens, N.; et al. Nutritional intervention in chronic pain: An innovative way of targeting central nervous system sensitization? Expert Opin. Ther. Targets 2020, 24, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Elma, Ö.; Yilmaz, S.T.; Mullie, P.; Vanderweeën, L.; Clarys, P.; Deliens, T.; Coppieters, I.; Weltens, N.; Van Oudenhove, L. Nutritional neurobiology and central nervous system sensitisation: Missing link in a comprehensive treatment for chronic pain? Br. J. Anaesth. 2019, 123, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Forsythe, P.; Kunze, W.A.; Bienenstock, J. On communication between gut microbes and the brain. Curr. Opin. Gastroenterol. 2012, 28, 557–562. [Google Scholar] [CrossRef]
- Dworsky-Fried, Z.; Kerr, B.J.; Taylor, A.M. Microbes, microglia, and pain. Neurobiol. Pain 2020, 7, 100045. [Google Scholar] [CrossRef] [PubMed]
- Croisier, E.; Brown, T.; Bauer, J. The Efficacy of Dietary Fiber in Managing Gastrointestinal Toxicity Symptoms in Patients with Gynecologic Cancers undergoing Pelvic Radiotherapy: A Systematic Review. J. Acad. Nutr. Diet. 2021, 121, 261–277.e2. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- Guida, F.; Boccella, S.; Belardo, C.; Iannotta, M.; Piscitelli, F.; De Filippis, F.; Paino, S.; Ricciardi, F.; Siniscalco, D.; Marabese, I. Altered gut microbiota and endocannabinoid system tone in vitamin D deficiency-mediated chronic pain. Brain Behav. Immun. 2020, 85, 128–141. [Google Scholar] [CrossRef]
- Dalile, B.; Van Oudenhove, L.; Vervliet, B.; Verbeke, K. The role of short-chain fatty acids in microbiota–gut–brain communication. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 461–478. [Google Scholar] [CrossRef]
- Sheflin, A.M.; Borresen, E.C.; Kirkwood, J.S.; Boot, C.M.; Whitney, A.K.; Lu, S.; Brown, R.J.; Broeckling, C.D.; Ryan, E.P.; Weir, T.L. Dietary supplementation with rice bran or navy bean alters gut bacterial metabolism in colorectal cancer survivors. Mol. Nutr. Food Res. 2017, 61, 1500905. [Google Scholar] [CrossRef] [Green Version]
- Horigome, A.; Okubo, R.; Hamazaki, K.; Kinoshita, T.; Katsumata, N.; Uezono, Y.; Xiao, J.; Matsuoka, Y. Association between blood omega-3 polyunsaturated fatty acids and the gut microbiota among breast cancer survivors. Benef. Microbes 2019, 10, 751–758. [Google Scholar] [CrossRef]
- Fassier, P.; Zelek, L.; Lécuyer, L.; Bachmann, P.; Touillaud, M.; Druesne-Pecollo, N.; Galan, P.; Cohen, P.; Hoarau, H.; Latino-Martel, P. Modifications in dietary and alcohol intakes between before and after cancer diagnosis: Results from the prospective population-based NutriNet-Santé cohort. Int. J. Cancer 2017, 141, 457–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.; Lee, J.; Kim, J. Imbalanced nutrient intake in cancer survivors from the examination from the nationwide health examination center-based cohort. Nutrients 2018, 10, 212. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.F.; Liu, S.; John, E.M.; Must, A.; Demark-Wahnefried, W. Diet quality of cancer survivors and noncancer individuals: Results from a national survey. Cancer 2015, 121, 4212–4221. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.F.; Ojha, R.P.; Krull, K.R.; Gibson, T.M.; Lu, L.; Lanctot, J.; Chemaitilly, W.; Robison, L.L.; Hudson, M.M. Adult Survivors of Childhood Cancer Have Poor Adherence to Dietary Guidelines. J. Nutr. 2016, 146, 2497–2505. [Google Scholar] [CrossRef] [Green Version]
- Tollosa, D.N.; Holliday, E.; Hure, A.; Tavener, M.; James, E.L. A 15-year follow-up study on long-term adherence to health behaviour recommendations in women diagnosed with breast cancer. Breast Cancer Res. Treat. 2020, 182, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Polak, R.; Dacey, M.; Phillips, E.M. Time for food—Training physiatrists in nutritional prescription. J. Rehabil. Med. 2017, 49, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Youn, J.; Lee, Y.J.; Kang, M.; Hyun, T.; Song, Y.; Lee, J.E. Dietary supplement use among cancer survivors and the general population: A nation-wide cross-sectional study. BMC Cancer 2017, 17, 891. [Google Scholar] [CrossRef] [Green Version]
- Du, M.; Luo, H.; Blumberg, J.B.; Rogers, G.; Chen, F.; Ruan, M.; Shan, Z.; Biever, E.; Zhang, F.F. Dietary supplement use among adult cancer survivors in the United States. J. Nutr. 2020, 150, 1499–1508. [Google Scholar] [CrossRef]
- Boland, E.; Ahmedzai, S. Persistent pain in cancer survivors. Curr. Opin. Support. Palliat. Care 2017, 11, 181–190. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 275–276. [Google Scholar] [CrossRef] [Green Version]
- Pouchieu, C.; Fassier, P.; Druesne-Pecollo, N.; Zelek, L.; Bachmann, P.; Touillaud, M.; Bairati, I.; Hercberg, S.; Galan, P.; Cohen, P. Dietary supplement use among cancer survivors of the NutriNet-Sante cohort study. Br. J. Nutr. 2015, 113, 1319–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burden, S.; Jones, D.J.; Sremanakova, J.; Sowerbutts, A.M.; Lal, S.; Pilling, M.; Todd, C. Dietary interventions for adult cancer survivors. Cochrane Database Syst. Rev. 2019, 2019, CD011287. [Google Scholar] [CrossRef] [PubMed]
- Befort, C.A.; Klemp, J.R.; Austin, H.L.; Perri, M.G.; Schmitz, K.H.; Sullivan, D.K.; Fabian, C.J. Outcomes of a weight loss intervention among rural breast cancer survivors. Breast Cancer Res. Treat. 2012, 132, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Tjon-A-Joe, S.; Pannekoek, S.; Kampman, E.; Hoedjes, M. Adherence to diet and body weight recommendations among cancer survivors after completion of initial cancer treatment: A systematic review of the literature. Nutr. Cancer 2019, 71, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Barlow, K.H.; van der Pols, J.C.; Ekberg, S.; Johnston, E.A. Cancer survivors’ perspectives of dietary information provision after cancer treatment: A scoping review of the Australian context. Health Promot. J. Aust. 2021, 33, 232–244. [Google Scholar] [CrossRef]
- Vijayvergia, N.; Denlinger, C.S. Lifestyle factors in cancer survivorship: Where we are and where we are headed. J. Pers. Med. 2015, 5, 243–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Reference | The Dietary Recommendations |
|---|---|
| 2020 American Cancer Society (ACS) Guideline on Diet and Physical Activity for Cancer Prevention [66] |
|
| World Cancer Research Fund (WCRF)/American Institute for Cancer Research (AICR) Diet, Nutrition, Physical Activity and Cancer: a Global Perspective (2018) [67] |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tümkaya Yılmaz, S.; Malfliet, A.; Elma, Ö.; Deliens, T.; Nijs, J.; Clarys, P.; De Groef, A.; Coppieters, I. Diet/Nutrition: Ready to Transition from a Cancer Recurrence/Prevention Strategy to a Chronic Pain Management Modality for Cancer Survivors? J. Clin. Med. 2022, 11, 653. https://doi.org/10.3390/jcm11030653
Tümkaya Yılmaz S, Malfliet A, Elma Ö, Deliens T, Nijs J, Clarys P, De Groef A, Coppieters I. Diet/Nutrition: Ready to Transition from a Cancer Recurrence/Prevention Strategy to a Chronic Pain Management Modality for Cancer Survivors? Journal of Clinical Medicine. 2022; 11(3):653. https://doi.org/10.3390/jcm11030653
Chicago/Turabian StyleTümkaya Yılmaz, Sevilay, Anneleen Malfliet, Ömer Elma, Tom Deliens, Jo Nijs, Peter Clarys, An De Groef, and Iris Coppieters. 2022. "Diet/Nutrition: Ready to Transition from a Cancer Recurrence/Prevention Strategy to a Chronic Pain Management Modality for Cancer Survivors?" Journal of Clinical Medicine 11, no. 3: 653. https://doi.org/10.3390/jcm11030653
APA StyleTümkaya Yılmaz, S., Malfliet, A., Elma, Ö., Deliens, T., Nijs, J., Clarys, P., De Groef, A., & Coppieters, I. (2022). Diet/Nutrition: Ready to Transition from a Cancer Recurrence/Prevention Strategy to a Chronic Pain Management Modality for Cancer Survivors? Journal of Clinical Medicine, 11(3), 653. https://doi.org/10.3390/jcm11030653