
The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Refractive and Visual Outcomes
3.2. Visual Quality—Spectacle Independence, Dysphotopsia, and Adverse Events
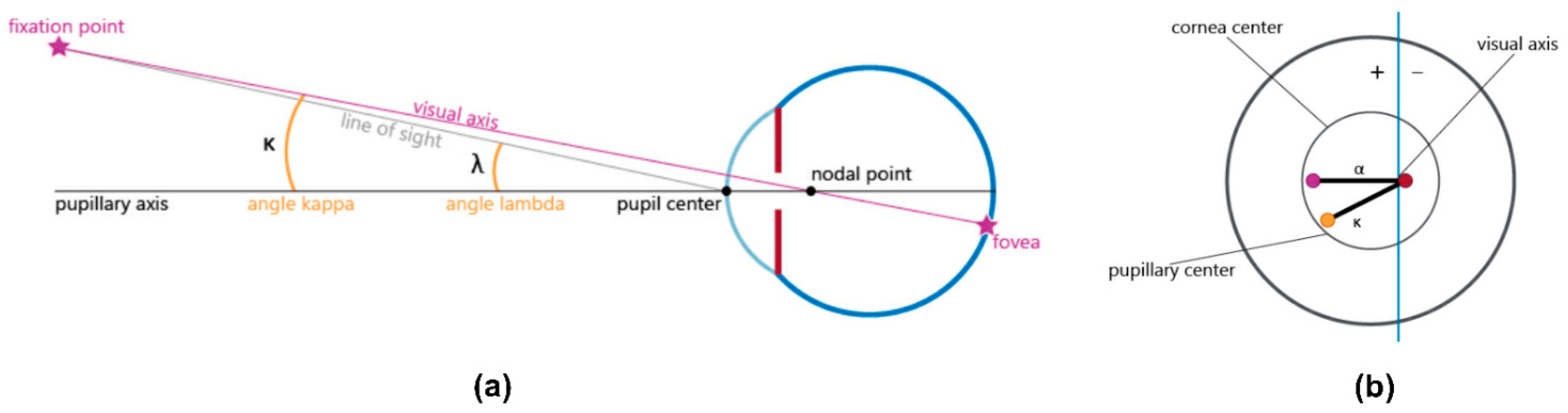
3.3. Refractive Aberrations and Notable Angles (Kappa and Alpha)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qi, Y.; Lin, J.; Leng, L.; Zhao, G.; Wang, Q.; Li, C.; Hu, L. Role of angle κ in visual quality in patients with a trifocal diffractive intraocular lens. J. Cataract. Refract. Surg. 2018, 8, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Barona, C.; Corredor-Ortega, C.; Avendaño-Domínguez, A.; Cervantes-Coste, G.; Cantú-Treviño, M.P.; Gonzalez-Salinas, R. Impact of correlation of angle α with ocular biometry variables. J. Cataract. Refract. Surg. 2021, 10, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Grzybowski, A.; Eppig, T. Angle alpha as predictor for improving patient satisfaction with multifocal intraocular lenses? Graefes Arch. Clin. Exp. Ophthalmol. 2021, 3, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Braga-Mele, R.; Chang, D.; Dewey, S.; Foster, G.; Henderson, B.A.; Hill, W.; Hoffman, R.; Little, B.; Mamalis, N.; Oetting, T.; et al. ASCRS Cataract. Clinical Committee. Multifocal intraocular lenses: Relative indications and contraindications for implantation. J. Cataract. Refract. Surg. 2014, 2, 313–322. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.E.; Webers, C.A.; Touwslager, W.R.; Bauer, N.J.; de Brabander, J.; Berendschot, T.T.; Nuijts, R.M. Dissatisfaction after implantation of multifocal intraocular lenses. J. Cataract. Refract. Surg. 2011, 5, 859–865. [Google Scholar] [CrossRef]
- Woodward, M.A.; Randleman, J.B.; Stulting, R.D. Dissatisfaction after multifocal intraocular lens implantation. J. Cataract. Refract. Surg. 2009, 6, 992–997. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Huang, J.Y.; Sun, C.C.; Yang, S.F.; Chen, H.C.; Lin, H.Y. Correlation and predictability of ocular aberrations and the visual outcome after quadrifocal intraocular lens implantation: A retrospective longitudinal study. BMC Ophthalmol. 2019, 1, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santhiago, M.R.; Netto, M.V.; Barreto, J., Jr.; Gomes, B.A.F.; Schaefer, A.; Kara-Junior, N. A contralateral eye study comparing apodized diffrative and full diffrative lenses: Wavefront analysis and distance and near uncorrected visual acuity. Clinics 2009, 10, 953–960. [Google Scholar] [CrossRef] [Green Version]
- Miháltz, K.; Vécsei-Marlovits, P.V. The impact of visual axis position on the optical quality after implantation of multifocal intraocular lenses with different asphericity values. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 3, 673–683. [Google Scholar] [CrossRef]
- Lee, H.; Lee, K.; Ahn, J.M.; Kim, E.K.; Sgrignoli, B.; Kim, T.I. Evaluation of optical quality parameters and ocular aberrations in multifocal intraocular lens implanted eyes. Yonsei Med. J. 2014, 5, 1413–1420. [Google Scholar] [CrossRef] [Green Version]
- Park, C.Y.; Oh, S.Y.; Chuck, R.S. Measurement of angle kappa and centration in refractive surgery. Curr. Opin. Ophthalmol. 2012, 4, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Harrer, A.; Hirnschall, N.; Tabernero, J.; Artal, P.; Draschl, P.; Maedel, S.; Findl, O. Variability in angle κ and its influence on higher-order aberrations in pseudophakic eyes. J. Cataract. Refract. Surg. 2017, 8, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Prakash, G.; Agarwal, A.; Prakash, D.R.; Kumar, D.A.; Agarwal, A.; Jacob, S. Role of angle kappa in patient dissatisfaction with refractive-design multifocal intraocular lenses. J. Cataract. Refract. Surg. 2011, 9, 1739–1740. [Google Scholar] [CrossRef] [PubMed]
- Ashena, Z.; Maqsood, S.; Ahmed, S.N.; Nanavaty, M.A. Effect of Intraocular Lens Tilt and Decentration on Visual Acuity, Dysphotopsia and Wavefront Aberrations. Vision 2020, 3, 41. [Google Scholar] [CrossRef]
- Hayashi, K.; Hayashi, H.; Nakao, F.; Hayashi, F. Correlation between pupillary size and intraocular lens decentration and visual acuity of a zonal-progressive multifocal lens and a monofocal lens. Ophthalmology 2001, 11, 2011–2017. [Google Scholar] [CrossRef]
- Madrid-Costa, D.; Pérez-Vives, C.; Ruiz-Alcocer, J.; Albarrán-Diego, C.; Montés-Micó, R. Visual simulation through different intraocular lenses in patients with previous myopic corneal ablation using adaptive optics: Effect of tilt and decentration. J. Cataract. Refract. Surg. 2012, 5, 774–786. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. Biometric factors associated with the visual performance of a high addition multifocal intraocular lens. Curr. Eye Res. 2018, 8, 998–1005. [Google Scholar] [CrossRef] [Green Version]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. Patient selection to optimize near vision performance with a low-addition trifocal lens. J. Optom. 2020, 1, 50–58. [Google Scholar] [CrossRef]
- Tchah, H.; Nam, K.; Yoo, A. Predictive factors for photic phenomena after refractive, rotationally asymmetric, multifocal intraocular lens implantation. Int. J. Ophthalmol. 2017, 10, 241–245. [Google Scholar] [CrossRef]
- Karhanová, M.; Marešová, K.; Pluháček, F.; Mlčák, P.; Vláčil, O.; Sín, M. Význam úhlu kappa pro centraci multifokálních nitroočních čoček [The importance of angle kappa for centration of multifocal intraocular lenses. Ces. Slov. Oftalmol. 2013, 2, 64–68. (In Czech) [Google Scholar]
- Soda, M.; Yaguchi, S. Effect of decentration on the optical performance in multifocal intraocular lenses. Ophthalmologica 2012, 4, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Pazo, E.E.; Richoz, O.; McNeely, R.; Millar, Z.A.; Moore, T.C.; Moore, J.E. Optimized visual outcome after asymmetrical multifocal IOL rotation. J. Refract. Surg. 2016, 7, 494–496. [Google Scholar] [CrossRef] [PubMed]
- Bonaque-González, S.; Jaskulski, M.T.; Carmona-Ballester, D.; Pareja-Ríos, A.; Trujillo-Sevilla, J.M. Influence of angle Kappa on the optimal intraocular orientation of asymmetric multifocal intraocular lenses. J. Optom. 2021, 1, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Kou, J.; Chen, D.; Wang, D.; Zhao, Y.; Hu, M.; Lin, X.; Dai, Q.; Li, J.; Zhao, Y.E. Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J. Cataract. Refract. Surg. 2019, 9, 1258–1264. [Google Scholar] [CrossRef]
- Chang, D.H.; Waring, G.O., IV. The subject-fixated coaxially sighted corneal light reflex: A clinical marker for centration of refractive treatments and devices. Am. J. Ophthalmol. 2014, 5, 863–874. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 20, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Vallejo, M.; Llorens-Quintana, C.; Furlan, W.D.; Monsoriu, J.A. Visual acuity and contrast sensitivity screening with a new iPad application. Displays 2016, 44, 15–20. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Tauste, A.; Albarrán, C.; Basterra, I.; Piñero, D. Fast measure of visual acuity and contrast sensitivity defocus curves with an iPad application. Open Ophthalmol. J. 2019, 1, 15–22. [Google Scholar] [CrossRef]
- Cervantes-Coste, G. The influence of angle alpha, angle kappa and optical aberra-tions on the visual outcomes after implantation of a high-addition trifocal IOL_2021. Mendeley Data 2021. [Google Scholar] [CrossRef]
- Holzer, M.P.; Rabsilber, T.M.; Auffarth, G.U. Presbyopiekorrektur mittels Intraokularlinsen. (Presbyopia correction using intraocular lenses). Ophthalmologe 2006, 8, 661–666. (In German) [Google Scholar] [CrossRef] [PubMed]
- Modesti, M.; Pasqualitto, G.; Appolloni, R.; Pecorella, I.; Sourdille, P. Preoperative and postoperative size and movements of the lens capsular bag: Ultrasound biomicroscopy analysis. J. Cataract. Refract. Surg. 2011, 10, 1775–1784. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lin, D.; Wang, Y.; Chen, W.; Xiao, W.; Xiang, Y.; Zhu, Y.; Chen, C.; Dong, X.; Liu, Y.; et al. Comparison of Visual Neuroadaptations after Multifocal and Monofocal Intraocular Lens Implantation. Front. Neurosci. 2021, 15, 719. [Google Scholar] [CrossRef]
- García-Bella, J.; Ventura-Abreu, N.; Morales-Fernández, L.; Talavero-González, P.; Carballo-Álvarez, J.; Sanz-Fernández, J.C.; Vázquez-Moliní, J.M.; Martínez-de-la-Casa, J.M. Visual outcomes after progressive apodized diffractive intraocular lens implantation. Eur. J. Ophthalmol. 2018, 3, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Vallejo, M.; Remón, L.; Monsoriu, J.A.; Furlan, W.D. Designing a new test for contrast sensitivity function measurement with iPad. J. Optom. 2015, 2, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Fernández, J.; García-Montesinos, J.; Martínez, J.; Piñero, D.P.; Rodríguez-Vallejo, M. Posterior capsular opacification evaluation through contrast sensitivity defocus curves with two multifocal intraocular lenses of similar material. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 10, 2995–3002. [Google Scholar] [CrossRef]
- Nochez, Y.; Majzoub, S.; Pisella, P.J. Effect of interaction of macroaberrations and scattered light on objective quality of vision in pseudophakic eyes with aspheric monofocal intraocular lenses. J. Cataract. Refract. Surg. 2012, 4, 633–640. [Google Scholar] [CrossRef]
- Nio, Y.K.; Jansonius, N.M.; Fidler, V.; Geraghty, E.; Norrby, S.; Kooijman, A.C. Spherical and irregular aberrations are important for the optimal performance of the human eye. Ophthalmic Physiol. Opt. 2002, 2, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Ravalico, G.; Parentin, F.; Baccara, F. Effect of astigmatism on multifocal intraocular lenses. J. Cataract. Refract. Surg. 1999, 6, 804–807. [Google Scholar] [CrossRef]
- Pérez-Merino, P.; Marcos, S. Effect of intraocular lens decentration on image quality tested in a custom model eye. J. Cataract. Refract. Surg. 2018, 7, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Nanavaty, M.A.; Spalton, D.J.; Gala, K.B. Fellow-eye comparison of 2 aspheric microincision intraocular lenses and effect of asphericity on visual performance. J. Cataract. Refract. Surg. 2012, 4, 625–632. [Google Scholar] [CrossRef]
- Rocha, K.M.; Soriano, E.S.; Chalita, M.R.; Yamada, A.C.; Bottós, K.; Bottós, J.; Morimoto, L.; Nosé, W. Wavefront analysis and contrast sensitivity of aspheric and spherical intraocular lenses: A randomized prospective study. Am. J. Ophthalmol. 2006, 5, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N. Assessment of corneal optical quality for premium IOLs with Pentacam. Highlights Ophthalmol. 2011, 4, 16–20. [Google Scholar] [CrossRef]
- Alió, J.L.; Pikkel, J. Multifocal Intraocular Lenses: The Art and the Practice; Springer Nature: Basingstoke, UK, 2019; p. 23. [Google Scholar]
- Artal, P.; Berrio, E.; Guirao, A.; Piers, P. Contribution of the cornea and internal surfaces to the change of ocular aberrations with age. J. Opt. Soc. Am. A 2002, 1, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Long, T.; Gu, X.; Ma, T. Changes in angle kappa and angle alpha before and after Cataract. surgery. J. Cataract. Refract. Surg. 2020, 3, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Day, A.C.; Dhariwal, M.; Keith, M.S.; Ender, F.; Perez Vives, C.; Miglio, C.; Zou, L.; Anderson, D.F. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing Cataract. surgery in the UK. Br. J. Ophthalmol. 2019, 7, 993–1000. [Google Scholar] [CrossRef] [Green Version]
- Michelitsch, M.; Ardjomand, N.; Vidic, B.; Wedrich, A.; Steinwender, G. Prävalenz und Altersabhängigkeit von kornealem Astigmatismus bei Patienten vor. (Prevalence and age-related changes of corneal astigmatism in patients before cataract surgery). Ophthalmologe 2017, 3, 247–251. (In German) [Google Scholar] [CrossRef] [PubMed]
- Pang, Y.L.; Yuan, L.; Cao, X.G.; Hou, X.R.; Bao, Y.Z. Characteristics and analysis of corneal astigmatism in age-related Cataract. patients over 50 years old. Chin. J. Ophthalmol. 2020, 5, 349–355. (In Chinese) [Google Scholar] [CrossRef]
- Artal, P.; Chen, L.; Fernández, E.J.; Singer, B.; Manzanera, S.; Williams, D.R. Neural compensation for the eye’s optical aberrations. J. Vis. 2004, 4, 281–287. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Preoperative Parameters | Mean ± SD | Minimum | Maximum |
|---|---|---|---|
| Age | 66.89 ± 10.1 | 45 | 82 |
| K1 total keratometry (D) | 43.21 ± 1.17 | 40.5 | 45.1 |
| K1 anterior (D) | 43.09 ± 1.18 | 39.75 | 45.2 |
| K2 total keratometry (D) | 43.78 ± 1.19 | 40.75 | 45.67 |
| K2 anterior (D) | 43.77 ± 1.25 | 40.75 | 45.75 |
| AXL (mm) | 23.68 ± 0.87 | 21.67 | 25.8 |
| IOL power (D) | 20.69 ± 2.71 | 13 | 26 |
| Pupil photopic (mm) | 3.03 ± 0.59 | 1.97 | 4.5 |
| Pupil mesopic (mm) | 4.96 ± 1.43 | 2.99 | 8.56 |
| Clinical Outcomes | Preoperative | Postoperative Month 1 | Postoperative Month 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Min | Max | Mean ± SD | Min | Max | Mean ± SD | Min | Max | |
| SPH (D) | 0.52 ± 2.58 | −10.0 | 3.25 | 0.02 ± 0.46 | −1.00 | 1.25 | −0.01 ± 0.48 | −1.25 | 1.25 |
| CYL (D) | −0.54 ± 0.56 | −2.00 | 0.25 | −0.49 ± 0.44 | −1.50 | 1.00 | −0.27 ± 0.44 | −1.25 | 1.00 |
| SEQ (D) | 0.25 ± 2.62 | −10.0 | 3.13 | −0.23 ± 0.47 | −1.50 | 1.00 | −0.15 ± 0.54 | −1.25 | 1.50 |
| Axis (degrees) | 88.4 ± 49.4 | 5.00 | 180 | 79.6 ± 51.6 | 0.00 | 180 | 84.4 ± 54.2 | 0.00 | 180 |
| UDVA (logMAR) | 0.68 ± 0.53 | 0.18 | 2.4 | 0.12 ± 0.11 | 0.00 | 0.70 | 0.09 ± 0.09 | 0.00 | 0.40 |
| CDVA (logMAR) | 0.27 ± 0.41 | 0.00 | 2.4 | 0.04 ± 0.08 | 0.00 | 0.54 | 0.02 ± 0.05 | 0.00 | 0.18 |
| UIVA (logMAR) | 0.65 ± 0.16 | 0.30 | 0.88 | 0.17 ± 0.12 | 0.00 | 0.60 | 0.18 ± 0.14 | 0.00 | 0.40 |
| UNVA (logMAR) | 0.69 ± 0.16 | 0.30 | 0.88 | 0.12 ± 0.11 | 0.00 | 0.48 | 0.10 ± 0.09 | 0.00 | 0.30 |
| Visual Acuity Area under Curve (AUC) | Mean ± SD | Minimum | Maximum | p-Value 1 |
|---|---|---|---|---|
| Month 1 (n = 51) | ||||
| Total (+1.0 D to −3.5 D) | 1.81 ± 0.98 | 0.00 | 4.35 | 0.0324 |
| Far (+1.0 D to −0.5 D) | 0.52 ± 0.20 | 0.00 | 0.90 | 0.0554 |
| Intermediate (−0.5 D to −2.0 D) | 0.53 ± 0.33 | 0.00 | 1.50 | 0.1987 |
| Near (−2.0 D to −3.5 D) | 0.65 ± 0.47 | 0.00 | 2.00 | 0.0435 |
| Month 3 (n = 41) | ||||
| Total (+1.0 D to −3.5 D) | 2.28 ± 0.91 | 0.23 | 3.92 | |
| Far (+1.0 D to −0.5 D) | 0.61 ± 0.20 | 0.09 | 0.92 | |
| Intermediate (−0.5 D to −2.0 D) | 0.64 ± 0.29 | 0.02 | 1.15 | |
| Near (−2.0 D to −3.5 D) | 0.87 ± 0.44 | 0.00 | 1.65 |
| Contrast Sensitivity Threshold Area under Curve (AUC) | Mean ± SD | Minimum | Maximum | p-Value 1 |
|---|---|---|---|---|
| Month 1 (n = 54) | ||||
| Total (+1.0 D to −3.5 D) | 2.11 ± 1.64 | 0.00 | 6.35 | 0.0060 |
| Far (+1.0 D to −0.5 D) | 0.75 ± 0.44 | 0.00 | 1.73 | 0.0027 |
| Intermediate (−0.5 D to −2.0 D) | 0.57 ± 0.56 | 0.00 | 2.04 | 0.0635 |
| Near (−2.0 D to −3.5 D) | 0.63 ± 0.66 | 0.00 | 2.40 | 0.0725 |
| Month 3 (n = 40) | ||||
| Total (+1.0 D to −3.5 D) | 2.84 ± 1.76 | 0.12 | 7.19 | |
| Far (+1.0 D to −0.5 D) | 0.96 ± 0.43 | 0.12 | 1.78 | |
| Intermediate (−0.5 D to −2.0 D) | 0.74 ± 0.60 | 0.00 | 2.32 | |
| Near (−2.0 D to −3.5 D) | 0.89 ± 0.69 | 0.00 | 2.59 |
| Optical Aberrations | Preoperative | Postoperative Month 1 | p-Value 1 |
|---|---|---|---|
| AST total (D) | −0.06 ± 0.78 | −0.12 ± 0.77 | 0.6574 |
| AST corneal (D) | −0.18 ± 0.85 | −0.46 ± 0.81 | 0.5323 |
| AST internal (D) | −0.31 ± 1.42 | −0.15 ± 1.08 | 0.5683 |
| Coma total (RMS) | 0.32 ± 0.29 | 0.16 ± 0.34 | 0.0259 |
| Coma corneal (RMS) | 0.33 ± 0.45 | 0.16 ± 0.13 | 0.2766 |
| Coma internal (RMS) | 0.38 ± 0.52 | 0.25 ± 0.42 | 0.4661 |
| HOA total (RMS) | 0.97 ± 1.16 | 0.84 ± 3.25 | 0.0815 |
| HOA corneal (RMS) | 0.55 ± 0.69 | 0.40 ± 0.32 | 0.7493 |
| HOA internal (RMS) | 1.03 ± 1.32 | 0.91 ± 3.37 | 0.0129 |
| Angle kappa photopic | 0.35 ± 0.18 | 0.24 ± 0.11 | 0.0007 |
| Angle kappa mesopic | 0.40 ± 0.18 | 0.32 ± 0.12 | <0.0001 |
| Angle alfa photopic | 0.56 ± 0.19 | 0.61 ± 0.29 | 0.5158 |
| Angle alfa mesopic | 0.63 ± 0.30 | 0.63 ± 0.36 | 0.4775 |
| Angle Kappa | R | 95% C.I. | R2 | p-Value 1 |
|---|---|---|---|---|
| Preoperative | ||||
| HOA total (RMS) | −0.133 | −0.50; 0.27 | 0.044 | 0.5172 |
| HOA corneal (RMS) | 0.036 | −0.37; 0.42 | 0.000 | 0.8602 |
| HOA internal (RMS) | 0.082 | −0.33; 0.47 | 0.002 | 0.6971 |
| UDVA (logMAR) | −0.053 | −0.41; 0.32 | 0.019 | 0.7758 |
| CDVA (logMAR) | −0.128 | −0.47; 0.24 | 0.029 | 0.4917 |
| UIVA (logMAR) | −0.155 | −0.49; 0.22 | 0.057 | 0.4043 |
| UNVA (logMAR) | 0.012 | −0.35; 0.37 | 0.006 | 0.9475 |
| Postoperative Month 1 | ||||
| HOA total (RMS) | 0.082 | −0.21; 0.37 | 0.000 | 0.5857 |
| HOA corneal (RMS) | 0.204 | −0.09; 0.47 | 0.014 | 0.1693 |
| HOA internal (RMS) | 0.206 | −0.09; 0.48 | 0.068 | 0.1692 |
| UDVA (logMAR) | −0.248 | −0.51; 0.05 | 0.071 | 0.0925 |
| CDVA (logMAR) | −0.187 | −0.46; 0.12 | 0.045 | 0.2094 |
| UIVA (logMAR) | −0.334 | −0.57; −0.04 | 0.151 | 0.0219 |
| UNVA (logMAR) | −0.269 | −0.52; 0.03 | 0.098 | 0.0671 |
| Angle Alpha | R | 95% C.I. | R2 | p-Value 1 |
|---|---|---|---|---|
| Preoperative | ||||
| HOA total (RMS) | −0.376 | −0.69; 0.06 | 0.128 | 0.0770 |
| HOA corneal (RMS) | −0.392 | −0.70; 0.04 | 0.040 | 0.0643 |
| HOA internal (RMS) | −0.204 | −0.58; 0.25 | 0.025 | 0.3633 |
| UDVA (logMAR) | 0.150 | −0.24; 0.50 | 0.031 | 0.4466 |
| CDVA (logMAR) | 0.112 | −0.28; 0.47 | 0.010 | 0.5713 |
| UIVA (logMAR) | −0.053 | −0.43; 0.34 | 0.015 | 0.7893 |
| UNVA (logMAR) | 0.037 | −0.35; 0.41 | 0.002 | 0.8526 |
| Postoperative Month 1 | ||||
| HOA total (RMS) | −0.290 | −0.56; 0.04 | 0.076 | 0.0779 |
| HOA corneal (RMS) | −0.517 | −0.72; −0.23 | 0.206 | 0.0009 |
| HOA internal (RMS) | −0.359 | −0.62; −0.03 | 0.049 | 0.0291 |
| UDVA (logMAR) | 0.004 | −0.32; 0.33 | 0.017 | 0.9795 |
| CDVA (logMAR) | −0.305 | −0.58; 0.03 | 0.070 | 0.0622 |
| UIVA (logMAR) | −0.280 | −0.56; 0.05 | 0.110 | 0.0881 |
| UNVA (logMAR) | −0.315 | −0.58; 0.02 | 0.113 | 0.0543 |
| R | 95% C.I. | R2 | p-Value 1 | |
|---|---|---|---|---|
| HOA total preop | ||||
| UDVA (logMAR) | −0.015 | −0.37; 0.34 | <0.001 | 0.9326 |
| CDVA (logMAR) | 0.226 | −0.14; 0.54 | 0.002 | 0.2064 |
| UIVA (logMAR) | −0.283 | −0.58; 0.08 | 0.004 | 0.1101 |
| UNVA (logMAR) | −0.245 | −0.55; 0.12 | 0.097 | 0.1703 |
| HOA corneal preop | ||||
| UDVA (logMAR) | 0.083 | −0.27; 0.41 | 0.026 | 0.6347 |
| CDVA (logMAR) | 0.417 | 0.09; 0.66 | 0.264 | 0.0126 |
| UIVA (logMAR) | −0.459 | −0.69; −0.14 | 0.217 | 0.0056 |
| UNVA (logMAR) | −0.039 | −0.38; 0.31 | <0.001 | 0.8262 |
| Coma total preop | ||||
| UDVA (logMAR) | −0.199 | −0.52; 0.16 | 0.017 | 0.2653 |
| CDVA (logMAR) | 0.125 | −0.24; 0.46 | 0.003 | 0.4898 |
| UIVA (logMAR) | −0.379 | −0.65; −0.03 | 0.042 | 0.0296 |
| UNVA (logMAR) | −0.433 | −0.68; −0.09 | 0.104 | 0.0118 |
| Coma corneal preop | ||||
| UDVA (logMAR) | −0.030 | −0.37; 0.32 | 0.001 | 0.8668 |
| CDVA (logMAR) | 0.352 | 0.01; 0.62 | 0.210 | 0.0411 |
| UIVA (logMAR) | −0.536 | −0.74; −0.23 | 0.255 | 0.0011 |
| UNVA (logMAR) | −0.282 | −0.57; 0.07 | 0.012 | 0.1063 |
| R | 95% C.I. | R2 | p-Value 1 | |
|---|---|---|---|---|
| Residual Corneal Astigmatism | ||||
| UDVA (logMAR) | 0.134 | −0.16; 0.40 | 0.054 | 0.3524 |
| CDVA (logMAR) | −0.085 | −0.36; 0.21 | <0.001 | 0.5558 |
| UIVA (logMAR) | 0.365 | 0.09; 0.59 | 0.173 | 0.0091 |
| UNVA (logMAR) | 0.255 | −0.03; 0.50 | 0.068 | 0.0741 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cervantes-Coste, G.; Tapia, A.; Corredor-Ortega, C.; Osorio, M.; Valdez, R.; Massaro, M.; Velasco-Barona, C.; Gonzalez-Salinas, R. The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL. J. Clin. Med. 2022, 11, 896. https://doi.org/10.3390/jcm11030896
Cervantes-Coste G, Tapia A, Corredor-Ortega C, Osorio M, Valdez R, Massaro M, Velasco-Barona C, Gonzalez-Salinas R. The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL. Journal of Clinical Medicine. 2022; 11(3):896. https://doi.org/10.3390/jcm11030896
Chicago/Turabian StyleCervantes-Coste, Guadalupe, André Tapia, Claudia Corredor-Ortega, Mariana Osorio, Rafael Valdez, Martha Massaro, Cecilio Velasco-Barona, and Roberto Gonzalez-Salinas. 2022. "The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL" Journal of Clinical Medicine 11, no. 3: 896. https://doi.org/10.3390/jcm11030896
APA StyleCervantes-Coste, G., Tapia, A., Corredor-Ortega, C., Osorio, M., Valdez, R., Massaro, M., Velasco-Barona, C., & Gonzalez-Salinas, R. (2022). The Influence of Angle Alpha, Angle Kappa, and Optical Aberrations on Visual Outcomes after the Implantation of a High-Addition Trifocal IOL. Journal of Clinical Medicine, 11(3), 896. https://doi.org/10.3390/jcm11030896