
Comparison of Clinical Outcomes, Visual Quality and Visual Function of Two Presbyopia-Correcting Intraocular Lenses Made from the Same Material, but with Different Design and Optics

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
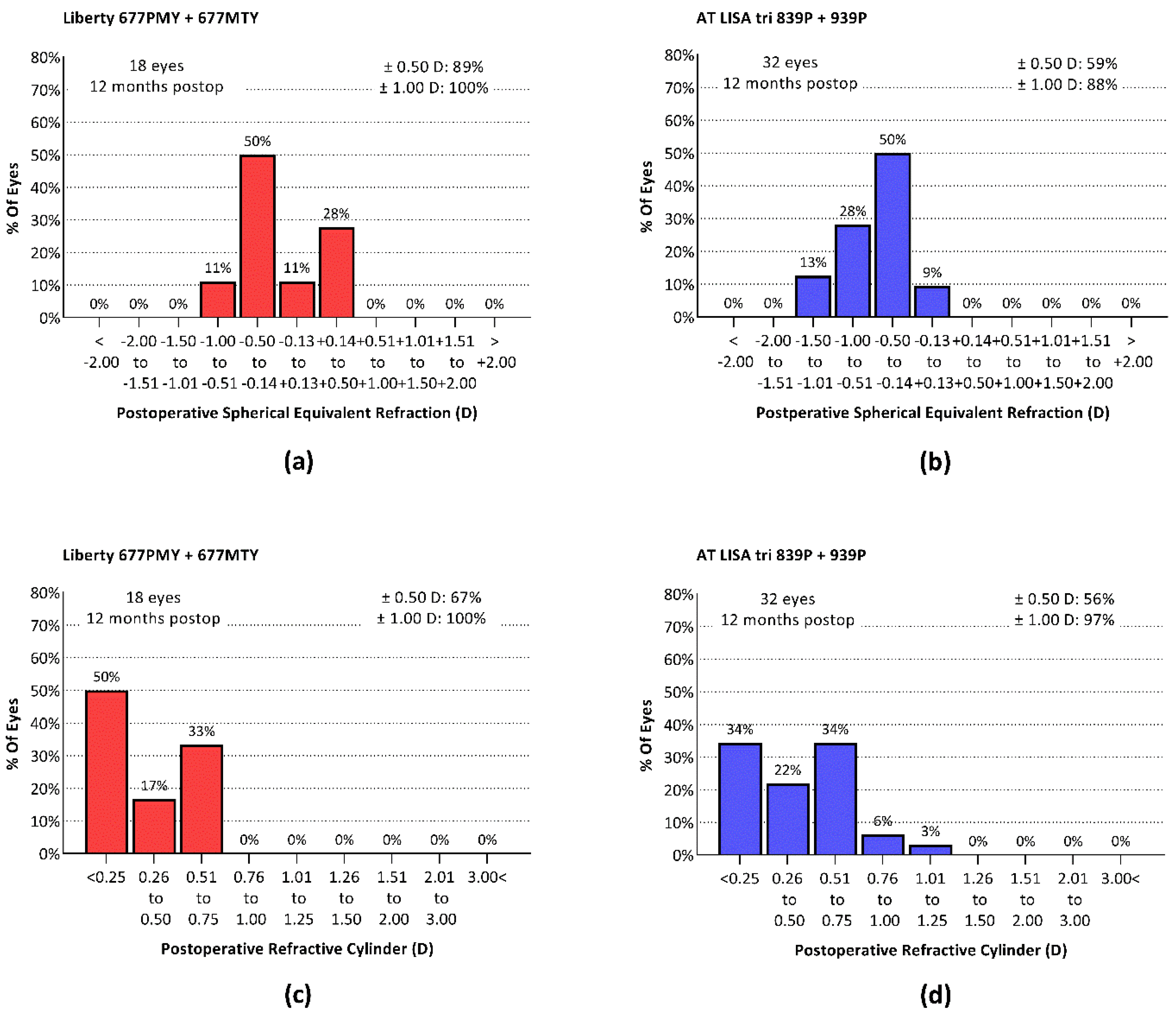
3.1. Refractive Correction
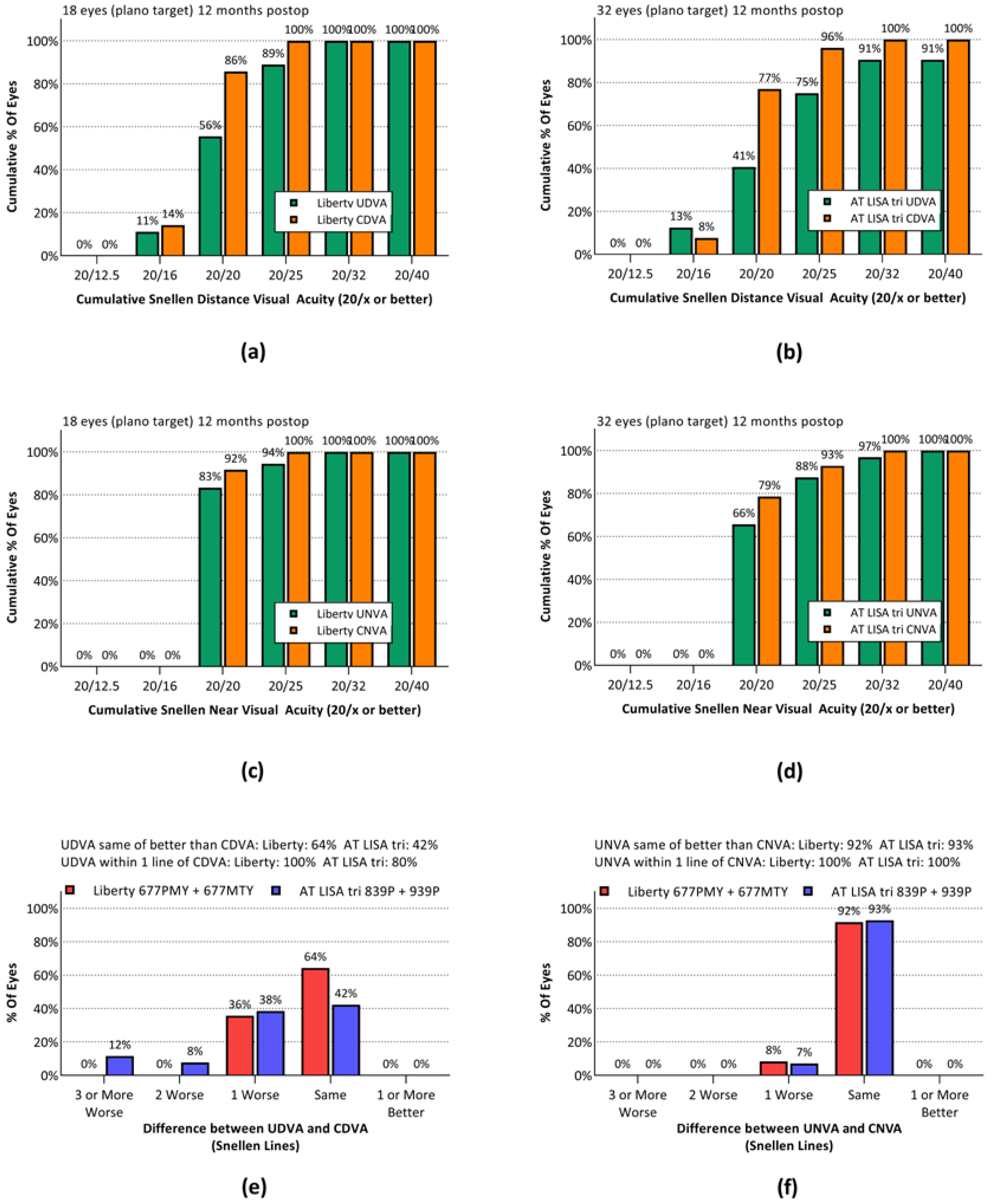
3.2. Visual Outcomes
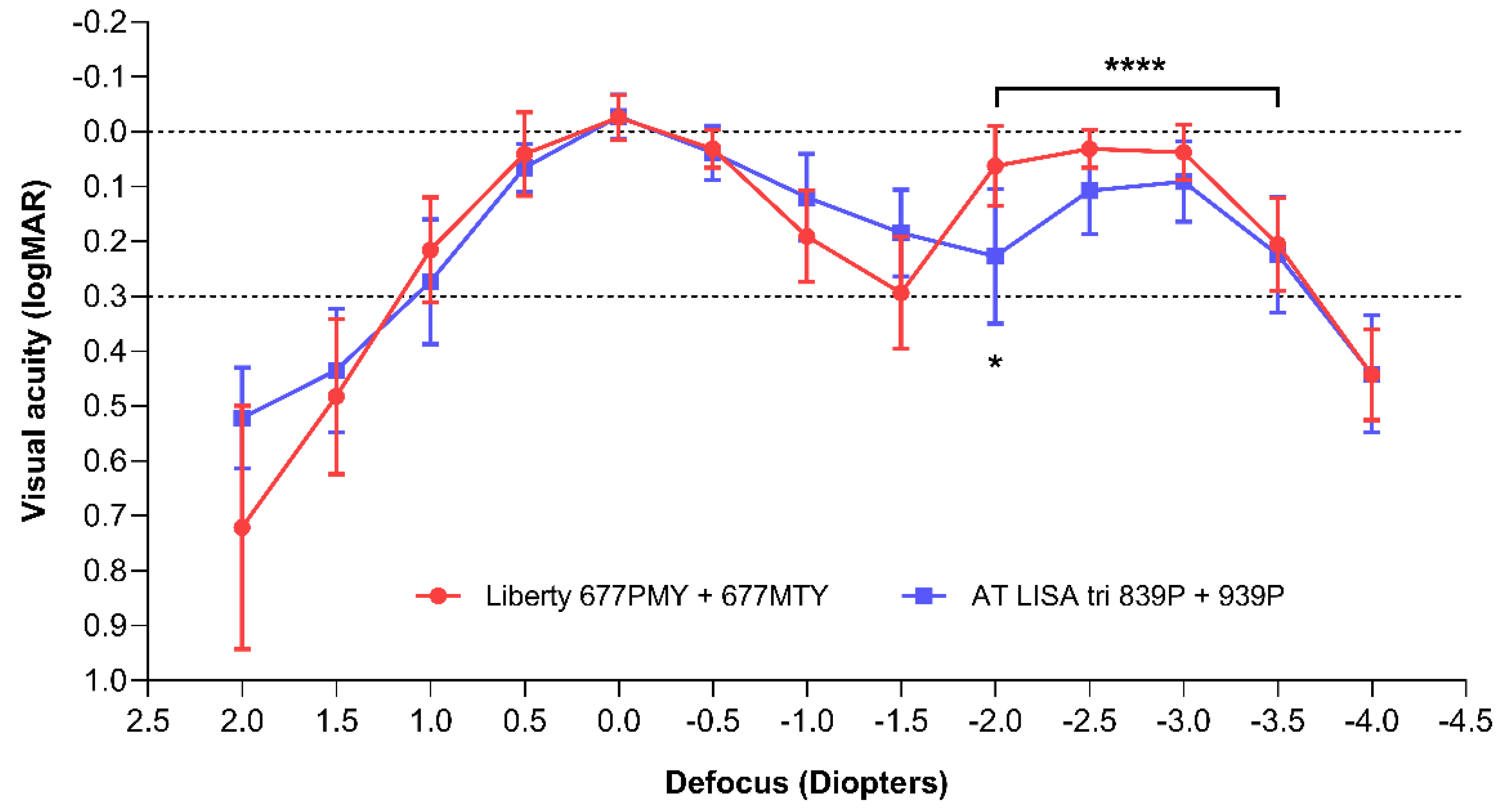
3.3. Defocus Curves and Area under Curve
3.4. Visual Quality
3.4.1. Optical Quality
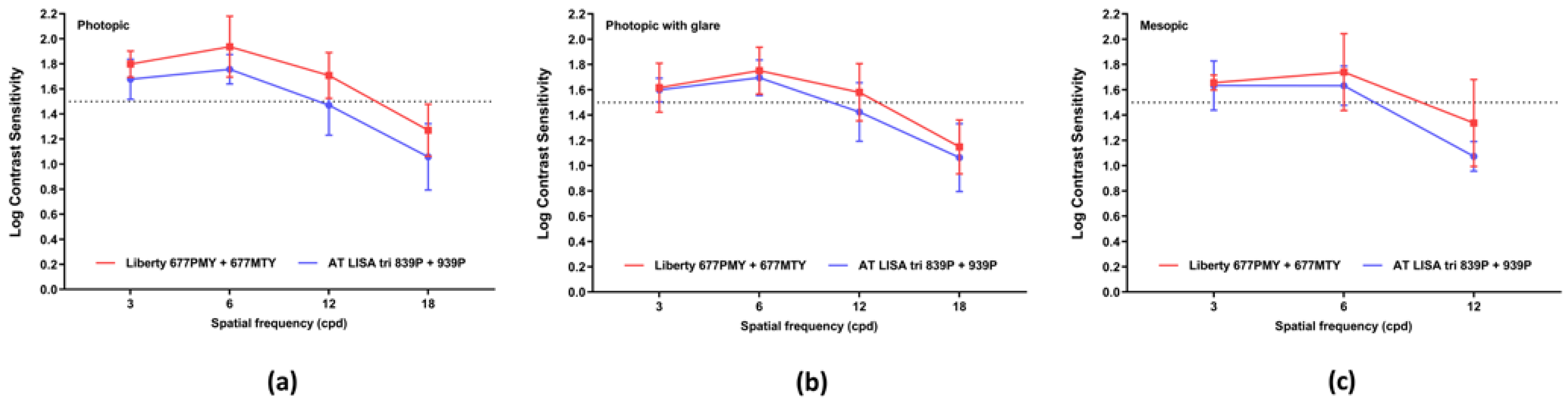
3.4.2. Contrast Sensitivity
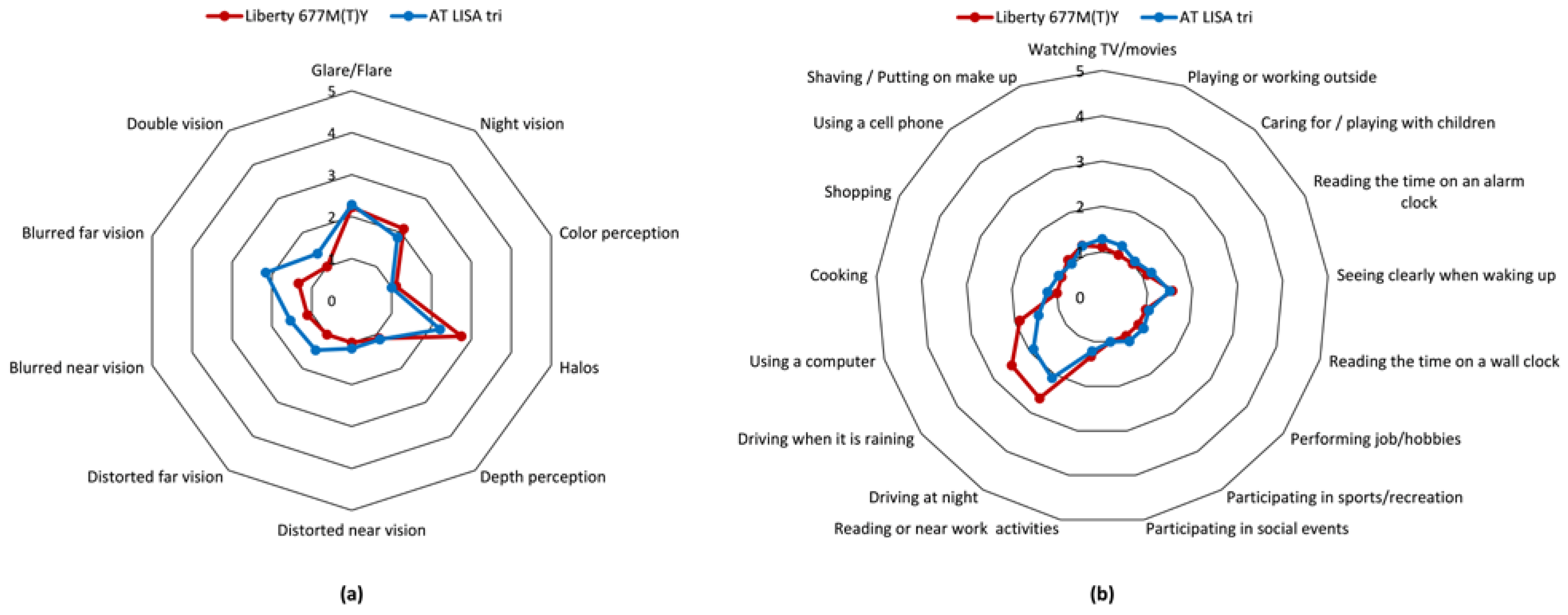
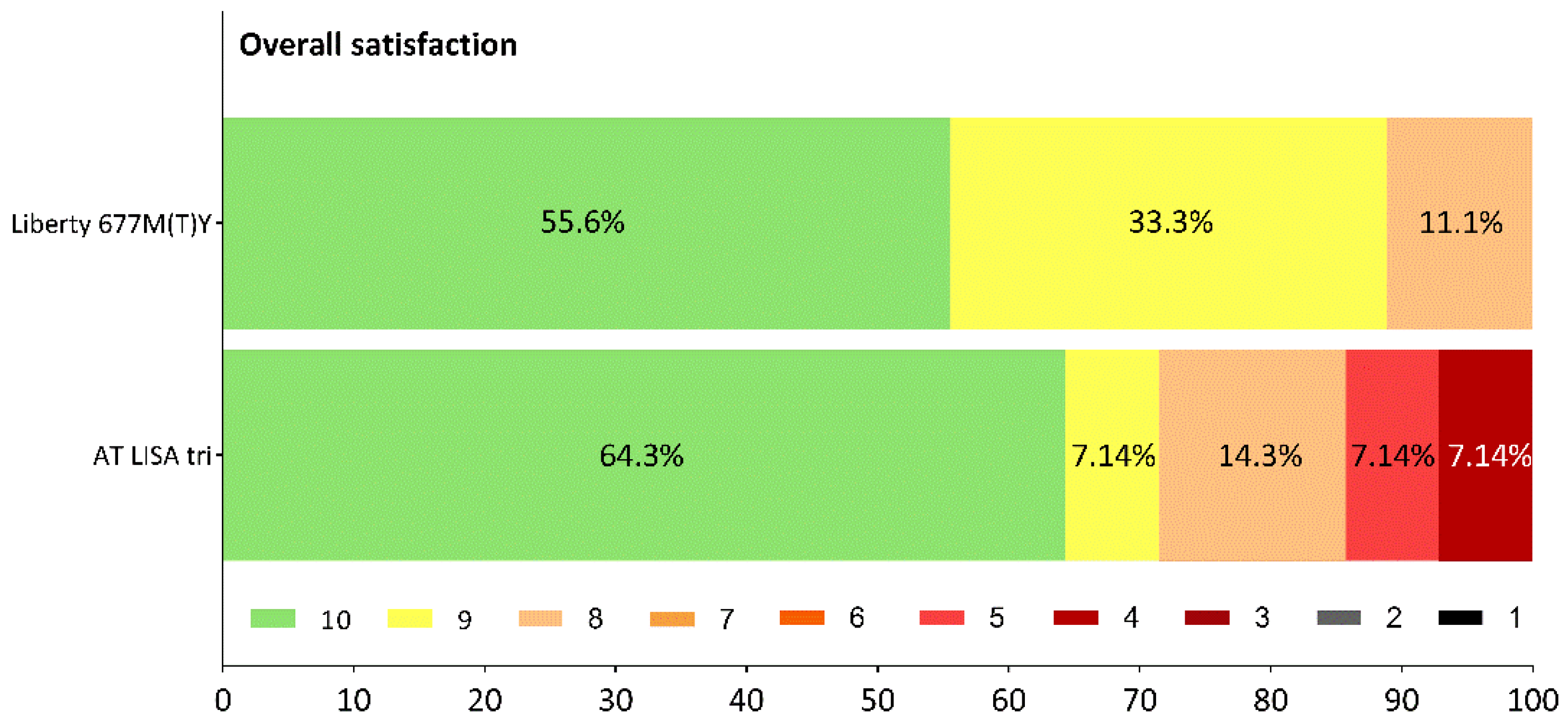
3.4.3. Visual Function, Dysphotopsia, Patient Satisfaction
3.5. Posterior Capsule Opacification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ESCRS 2019 Clinical Trends Survey Results. EuroTimes. 2020. Available online: https://www.eurotimes.org/wp-content/uploads/2020/11/Clinical-Survey-Results-2019-Supplement_PQ.pdf (accessed on 5 November 2020).
- Logothetis, H.D.; Feder, R.S. Which intraocular lens would ophthalmologists choose for themselves? Eye 2019, 33, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Buckhurst, P.J.; Naroo, S.A.; Davies, L.N.; Shah, S.; Drew, T.; Wolffsohn, J.S. Assessment of dysphotopsia in pseudophakic subjects with multifocal intraocular lenses. BMJ Open Ophthalmol. 2017, 1, e000064. [Google Scholar] [CrossRef] [Green Version]
- Masket, S.; Fram, N.R. Pseudophakic Dysphotopsia: Review of Incidence, Cause, and Treatment of Positive and Negative Dysphotopsia. Ophthalmology 2020, 30787–30789. [Google Scholar] [CrossRef]
- Schartmüller, D.; Schriefl, S.; Schwarzenbacher, L.; Leydolt, C.; Kundi, M.; Pieh, S.; Menapace, R.; Kriechbaum, K. Posterior capsule opacification and Nd:YAG laser rates with two hydrophobic acrylic single-piece IOLs. Eye 2020, 5, 857–863. [Google Scholar] [CrossRef]
- Yagci, R.; Uzun, F.; Acer, S.; Hepsen, I.F. Comparison of visual quality between aspheric and spherical IOLs. Eur. J. Ophthalmol. 2014, 5, 688–692. [Google Scholar] [CrossRef]
- Tang, Y.; Song, H.; Chen, J.; Tang, X. Comparison of pseudophakic retinal straylight in spherical/aspherical and hydrophobic/hydrophilic intraocular lens. Int. J. Ophthalmol. 2015, 6, 1146–1150. [Google Scholar] [CrossRef]
- Savini, G.; Barboni, P.; Ducoli, P.; Borrelli, E.; Hoffer, K.J. Influence of intraocular lens haptic design on refractive error. J. Cataract Refract. Surg. 2014, 9, 1473–1478. [Google Scholar] [CrossRef]
- Zhu, X.; Meng, J.; He, W.; Rong, X.; Lu, Y. Comparison of the rotational stability between plate-haptic toric and C-loop haptic toric IOLs in myopic eyes. J. Cataract Refract. Surg. 2020, 10, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Alió, J.L.; Dick, H.B.; Dell, S.; Slade, S. Efficacy and safety of multifocal intraocular lenses following cataract and refractive lens exchange: Metaanalysis of peer-reviewed publications. J. Cataract Refract. Surg. 2016, 2, 310–328. [Google Scholar] [CrossRef]
- Pérez-Vives, C. Biomaterial influence on intraocular lens performance: An overview. J. Ophthalmol. 2018, 2018, 2687385. [Google Scholar] [CrossRef] [Green Version]
- Masket, S.; Rupnick, Z.; Fram, N.R.; Kwong, S.; McLachlan, J. Surgical management of positive dysphotopsia: U.S. perspective. J. Cataract Refract. Surg. 2020, 1474–1479. [Google Scholar] [CrossRef]
- Miyata, K.; Kataoka, Y.; Matsunaga, J.; Honbo, M.; Minami, K. Prospective Comparison of One-Piece and Three-Piece Tecnis Aspheric Intraocular Lenses: 1-year Stability and its Effect on Visual Function. Curr. Eye Res. 2015, 9, 930–935. [Google Scholar] [CrossRef]
- Poyales, F.; Pérez, R.; López-Brea, I.; Zhou, Y.; Rico, L.; Garzón, N. Comparison of Visual Performance and Patient Satisfaction Outcomes with Two Trifocal IOLs with Similar Optical Design but Different Materials. Clin. Ophthalmol. 2020, 14, 3237–3247. [Google Scholar] [CrossRef]
- Buehl, W.; Findl, O. Effect of intraocular lens design on posterior capsule opacification. J. Cataract Refract. Surg. 2008, 11, 1976–1985. [Google Scholar] [CrossRef]
- Iliescu, I.M.; Constantin, M.A.; Cozma, C.; Moraru, O.M.; Moraru, C.M. Posterior Capsule Opacification and Nd-YAG rates evaluation in a large series of pseudophakic cases. Rom. J. Ophthalmol. 2017, 4, 267–274. [Google Scholar] [CrossRef]
- Billotte, C.; Berdeaux, G. Adverse clinical consequences of neodymium:YAG laser treatment of posterior capsule opacification. J. Cataract Refract. Surg. 2004, 10, 2064–2071. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 20, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Novacek, L. Comparison of clinical outcomes, visual quality and visual function of two presbyopia-correcting intraocular lenses made from the same material, but with different design and optics. Mendeley Data V1 2021. [Google Scholar] [CrossRef]
- Reinstein, D.Z.; Archer, T.J.; Srinivasan, S.; Mamalis, N.; Kohnen, T.; Dupps, W.J., Jr.; Randleman, J.B. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J. Cataract Refract. Surg. 2017, 4, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Serdiuk, V.; Ustymenko, S.; Fokina, S.; Ivantsov, I. Comparison of three different presbyopia-correcting intraocular lenses. Rom. J. Ophthalmol. 2020, 4, 364–379. [Google Scholar] [CrossRef]
- Piovella, M.; Colonval, S.; Kapp, A.; Reiter, J.; Van Cauwenberge, F.; Alfonso, J. Patient outcomes following implantation with a trifocal toric IOL: Twelve-month prospective multicentre study. Eye 2019, 1, 144–153. [Google Scholar] [CrossRef]
- Gyory, J.F.; Madár, E.; Srinivasan, S. Implantation of a diffractive-refractive trifocal intraocular lens with centralized diffractive rings: Two-year results. J. Cataract Refract. Surg. 2019, 5, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Tauste, A.; Piñero, D.P. Biometric Factors Associated with the Visual Performance of a High Addition Multifocal Intraocular Lens. Curr. Eye Res. 2018, 8, 998–1005. [Google Scholar] [CrossRef] [Green Version]
- García-Bella, J.; Ventura-Abreu, N.; Morales-Fernández, L.; Talavero-González, P.; Carballo-Álvarez, J.; Sanz-Fernández, J.C.; Vázquez-Moliní, J.M.; Martínez-de-la-Casa, J.M. Visual outcomes after progressive apodized diffractive intraocular lens implantation. Eur. J. Ophthalmol. 2018, 3, 282–286. [Google Scholar] [CrossRef]
- Kim, B.H.; Hyon, J.Y.; Kim, M.K. Effects of Bifocal versus Trifocal Diffractive Intraocular Lens Implantation on Visual Quality after Cataract Surgery. Korean J. Ophthalmol. 2019, 4, 333–342. [Google Scholar] [CrossRef]
- Lapid-Gortzak, R.; Bhatt, U.; Sanchez, J.G.; Guarro, M.; Hida, W.T.; Bala, C.; Nosé, R.M.; Rodriguez Alvira, F.J.; Martinez, A. Multicenter visual outcomes comparison of 2 trifocal presbyopia-correcting IOLs: 6-month postoperative results. J. Cataract Refract. Surg. 2020, 11, 1534–1542. [Google Scholar] [CrossRef]
- Webers, V.S.C.; Bauer, N.J.C.; Saelens, I.E.Y.; Creten, O.J.M.; Berendschot, T.T.J.M.; van den Biggelaar, F.J.H.M.; Nuijts, R.M.M.A. Comparison of the intermediate distance of a trifocal IOL with an extended depth-of-focus IOL: Results of a prospective randomized trial. J. Cataract Refract. Surg. 2020, 2, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Mojzis, P.; Majerova, K.; Hrckova, L.; Piñero, D.P. Implantation of a diffractive trifocal intraocular lens: One-year follow-up. J. Cataract Refract. Surg. 2015, 8, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Tarib, I.; Diakonis, V.F.; Breyer, D.; Höhn, F.; Hahn, U.; Kretz, F.T.A. Outcomes of combining a trifocal and a low-addition bifocal intraocular lens in patients seeking spectacle independence at all distances. J. Cataract Refract. Surg. 2019, 5, 620–629. [Google Scholar] [CrossRef]
- de Silva, S.R.; Evans, J.R.; Kirthi, V.; Ziaei, M.; Leyland, M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst. Rev. 2016, 12, CD003169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Peris-Martinez, C.; Reinhard, T.; Vinciguerra, P. Visual outcomes after cataract surgery: Multifocal versus monofocal intraocular lenses. J. Refract. Surg. 2015, 10, 658–666. [Google Scholar] [CrossRef] [Green Version]
- Cao, K.; Friedman, D.S.; Jin, S.; Yusufu, M.; Zhang, J.; Wang, J.; Hou, S.; Zhu, G.; Wang, B.; Xiong, Y.; et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: A system review and meta-analysis based on randomized controlled trials. Surv. Ophthalmol. 2019, 5, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Javitt, J.C.; Steinert, R.F. Cataract extraction with multifocal intraocular lens implantation: A multinational clinical trial evaluating clinical, functional, and quality-of-life outcomes. Ophthalmology 2000, 11, 2040–2048. [Google Scholar] [CrossRef]
- Javitt, J.C.; Wang, F.; Trentacost, D.J.; Rowe, M.; Tarantino, N. Outcomes of cataract extraction with multifocal intraocular lens implantation: Functional status and quality of life. Ophthalmology 1997, 4, 589–599. [Google Scholar] [CrossRef]
- Vingolo, E.M.; Grenga, P.; Iacobelli, L.; Grenga, R. Visual acuity and contrast sensitivity: AcrySof ReSTOR apodized diffractive versus AcrySof SA60AT monofocal intraocular lenses. J. Cataract Refract. Surg. 2007, 7, 1244–1247. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.E.; Webers, C.A.; Touwslager, W.R.; Bauer, N.J.; de Brabander, J.; Berendschot, T.T.; Nuijts, R.M. Dissatisfaction after implantation of multifocal intraocular lenses. J. Cataract Refract. Surg. 2011, 5, 859–865. [Google Scholar] [CrossRef]
- Woodward, M.A.; Randleman, J.B.; Stulting, R.D. Dissatisfaction after multifocal intraocular lens implantation. J. Cataract Refract. Surg. 2009, 6, 992–997. [Google Scholar] [CrossRef] [Green Version]
- Meng, J.; He, W.; Rong, X.; Miao, A.; Lu, Y.; Zhu, X. Decentration and tilt of plate-haptic multifocal intraocular lenses in myopic eyes. Eye Vis. 2020, 7, 17. [Google Scholar] [CrossRef]
- Ashena, Z.; Maqsood, S.; Ahmed, S.N.; Nanavaty, M.A. Effect of Intraocular Lens Tilt and Decentration on Visual Acuity, Dysphotopsia and Wavefront Aberrations. Vision 2020, 3, 41. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Hayashi, H. Influence on posterior capsule opacification and visual function of intraocular lens optic material. Am. J. Ophthalmol. 2007, 144, 195–202. [Google Scholar] [CrossRef]
- Nishi, O.; Yamamoto, N.; Nishi, K.; Nishi, Y. Contact inhibition of migrating lens epithelial cells at the capsuler bend created by a sharp-edged intraocular lens after cataract surgery. J. Cataract Refract. Surg. 2007, 33, 1065–1070. [Google Scholar] [CrossRef]
- Buehl, W.; Menapace, R.; Findl, O.; Neumayer, T.; Bolz, M.; Prinz, A. Long-term effect of optic edge design in a silicone intraocular lens on posterior capsule opacification. Am. J. Ophthalmol. 2007, 143, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.W.; Wei, R.L.; Cai, J.P.; Xi, G.L.; Zhu, H.; Li, Y.; Ma, X.Y. Efficacy of different intraocular lens material and optic edge designs in preventing posterior capsular opacification: A meta-analysis. Am. J. Ophthalmol. 2007, 143, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Findl, O.; Buehl, W.; Bauer, P.; Sycha, T. Interventions for preventing posterior capsule opacification. Cochrane Database Syst. Rev. 2010, 17, CD003738. [Google Scholar] [CrossRef] [PubMed]
- Wormstone, I.M.; Wormstone, Y.M.; Smith, A.J.O.; Eldred, J.A. Posterior capsule opacification: What’s in the bag? Prog. Retin. Eye Res. 2021, 82, 100905. [Google Scholar] [CrossRef]
- Bachernegg, A.; Rückl, T.; Strohmaier, C.; Jell, G.; Grabner, G.; Dexl, A.K. Vector Analysis, Rotational Stability, and Visual Outcome after Implantation of a New Aspheric Toric IOL. J. Refract. Surg. 2015, 8, 513–520. [Google Scholar] [CrossRef]
- Győry, J.F. Long-term evaluation of contrast sensitivity prior to and after the implantation of the Liberty 677MY trifocal intraocular lens. In Proceedings of the 37th ESCRS Congress, Paris, France, 14–18 September 2019. Abstract Number FP-298695. [Google Scholar]
- Law, E.M.; Aggarwal, R.K.; Buckhurst, H.; Kasaby, H.E.; Marsden, J.; Shum, G.; Buckhurst, P.J. Visual function and subjective perception of vision after bilateral implantation of monofocal and multifocal IOLs: A randomized controlled trial. J. Cataract Refract. Surg. 2020, 7, 1020–1029. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Residual Refraction | IOL | Month 3 | Month 12 | Month 3 vs. Month 12 p = 1 |
|---|---|---|---|---|
| SPH | Liberty | 0.05 ± 0.21 | −0.47 ± 0.47 | 0.6193 |
| AT LISA tri | −0.06 ± 0.36 | −0.27 ± 0.43 | 0.3189 | |
| p = 2 | 0.0004 * | 0.0739 | ||
| Cyl | Liberty | −0.39 ± 0.63 | −0.44 ± 0.27 | 0.3276 |
| AT LISA tri | −0.35 ± 0.37 | −0.54 ± 0.30 | 0.0879 | |
| p= | 0.7865 | 0.0499 * | ||
| SEQ | Liberty | −0.20 ± 0.32 | −0.23 ± 0.39 | >0.9999 |
| AT LISA tri | −0.24 ± 0.39 | −0.60 ± 0.44 | 0.6062 | |
| p= | 0.0021 * | 0.0054 * |
| Visual Acuity | IOL | Month 3 | Month 12 | Month 3 vs. Month 12 p = 1 |
|---|---|---|---|---|
| UDVA | Liberty | 0.02 ± 0.04 | 0.03 ± 0.07 | 0.0469 * |
| AT LISA tri | 0.13 ± 0.06 | 0.10 ± 0.19 | 0.3125 | |
| p = 2 | 0.0033 * | 0.2206 | ||
| CDVA | Liberty | 0.00 ± 0.03 | 0.00 ± 0.04 | >0.9999 |
| AT LISA tri | 0.04 ± 0.06 | 0.01 ± 0.05 | 0.2500 | |
| p = 2 | 0.0394 * | 0.4720 | ||
| DCIVA | Liberty | N/A | 0.30 ± 0.10 | N/A |
| AT LISA tri | N/A | 0.18 ± 0.08 | N/A | |
| p = 2 | N/A | 0.0001 * | ||
| Liberty | 0.02 ± 0.05 | 0.02 ± 0.05 | >0.9999 | |
| UNVA | AT LISA tri | 0.00 ± 0.00 | 0.05 ± 0.08 | 0.2500 |
| p = 2 | 0.2258 | 0.2092 | ||
| Liberty | 0.03 ± 0.06 | 0.01 ± 0.03 | 0.3714 | |
| CNVA | AT LISA tri | 0.00 ± 0.00 | 0.03 ± 0.06 | 0.5539 |
| p = 2 | 0.4286 | 0.5252 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nováček, L.V.; Němcová, M.; Tyx, K.; Lahodová, K.; Rejmont, L.; Rozsíval, P.; Studený, P. Comparison of Clinical Outcomes, Visual Quality and Visual Function of Two Presbyopia-Correcting Intraocular Lenses Made from the Same Material, but with Different Design and Optics. J. Clin. Med. 2021, 10, 3268. https://doi.org/10.3390/jcm10153268
Nováček LV, Němcová M, Tyx K, Lahodová K, Rejmont L, Rozsíval P, Studený P. Comparison of Clinical Outcomes, Visual Quality and Visual Function of Two Presbyopia-Correcting Intraocular Lenses Made from the Same Material, but with Different Design and Optics. Journal of Clinical Medicine. 2021; 10(15):3268. https://doi.org/10.3390/jcm10153268
Chicago/Turabian StyleNováček, Ladislav Viktor, Marie Němcová, Kateřina Tyx, Kristýna Lahodová, Leoš Rejmont, Pavel Rozsíval, and Pavel Studený. 2021. "Comparison of Clinical Outcomes, Visual Quality and Visual Function of Two Presbyopia-Correcting Intraocular Lenses Made from the Same Material, but with Different Design and Optics" Journal of Clinical Medicine 10, no. 15: 3268. https://doi.org/10.3390/jcm10153268
APA StyleNováček, L. V., Němcová, M., Tyx, K., Lahodová, K., Rejmont, L., Rozsíval, P., & Studený, P. (2021). Comparison of Clinical Outcomes, Visual Quality and Visual Function of Two Presbyopia-Correcting Intraocular Lenses Made from the Same Material, but with Different Design and Optics. Journal of Clinical Medicine, 10(15), 3268. https://doi.org/10.3390/jcm10153268