
Extracorporeal Membrane Oxygenation in Infarct-Related Cardiogenic Shock

 ,
,
Abstract
:1. Introduction
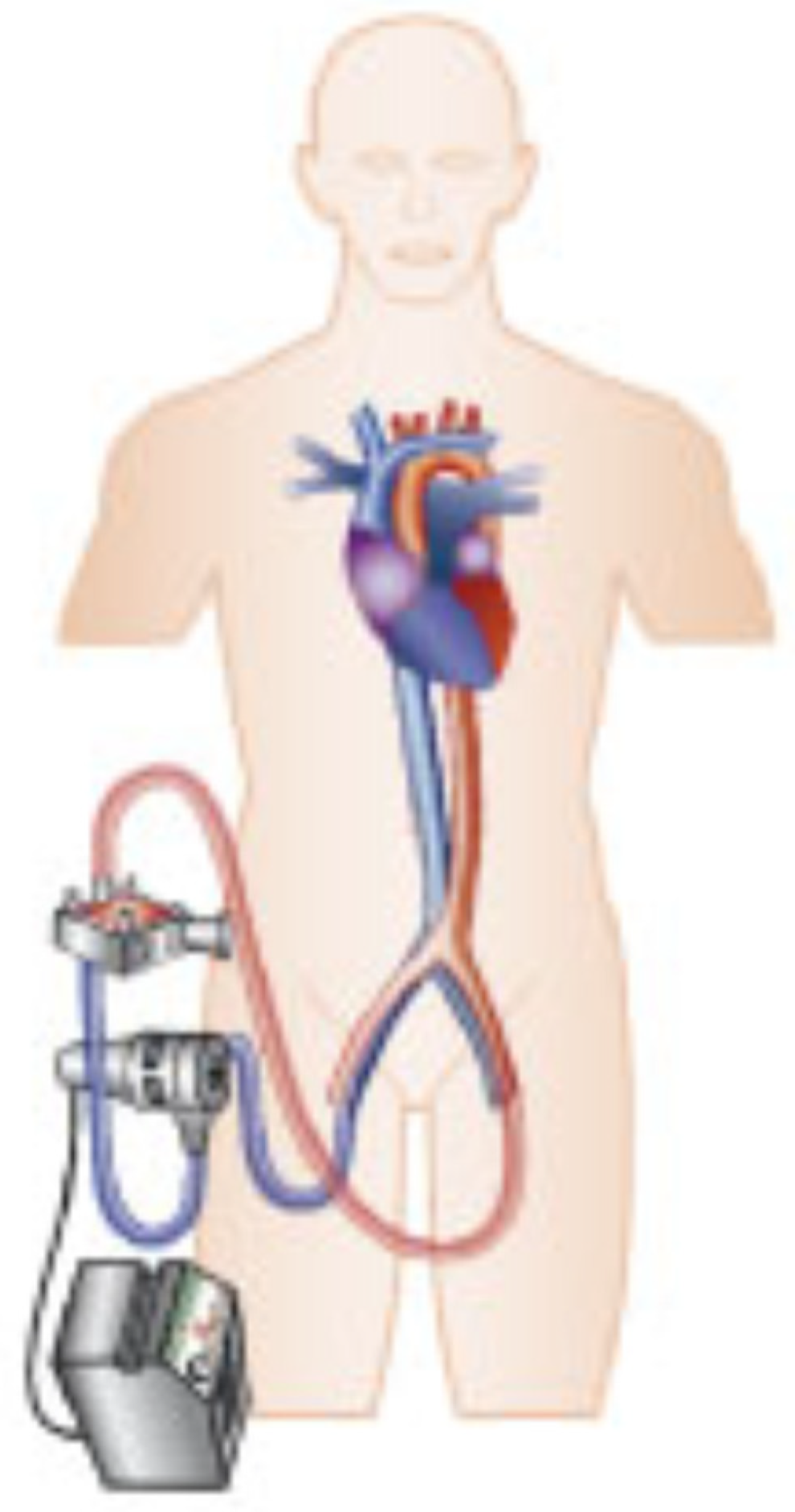
2. Basic Operating Principle of VA-ECMO
3. Evidence of VA-ECMO Therapy in AMI-CS
4. Patient Selection
5. Timing of VA-ECMO Initiation
6. Intensive Care Treatment
6.1. Pulmonary Artery Catheter
6.2. Catecholamine Therapy
6.3. Mechanical Ventilation
6.4. Renal Replacement Therapy
7. Extracorporeal Cardiopulmonary Resuscitation
8. Complications of VA-ECMO Therapy
- -
- Bleeding
- -
- Clotting
- -
- Hemolysis
- -
- Limb ischemia
- -
- Inadequate LV unloading
- -
- Harlequin syndrome
- -
- Infection
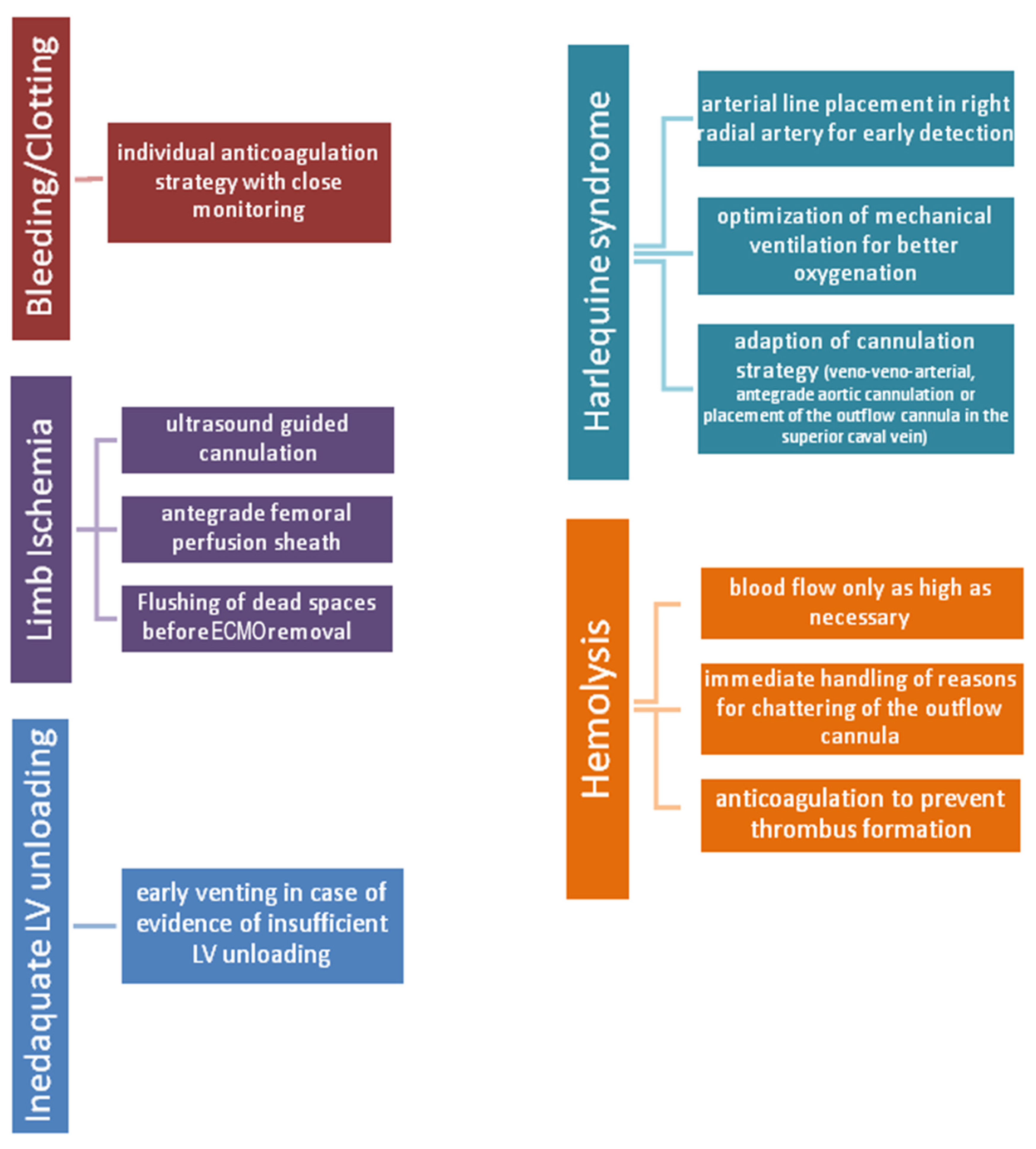
8.1. Bleeding/Clotting
8.2. Hemolysis
8.3. Limb Ischemia
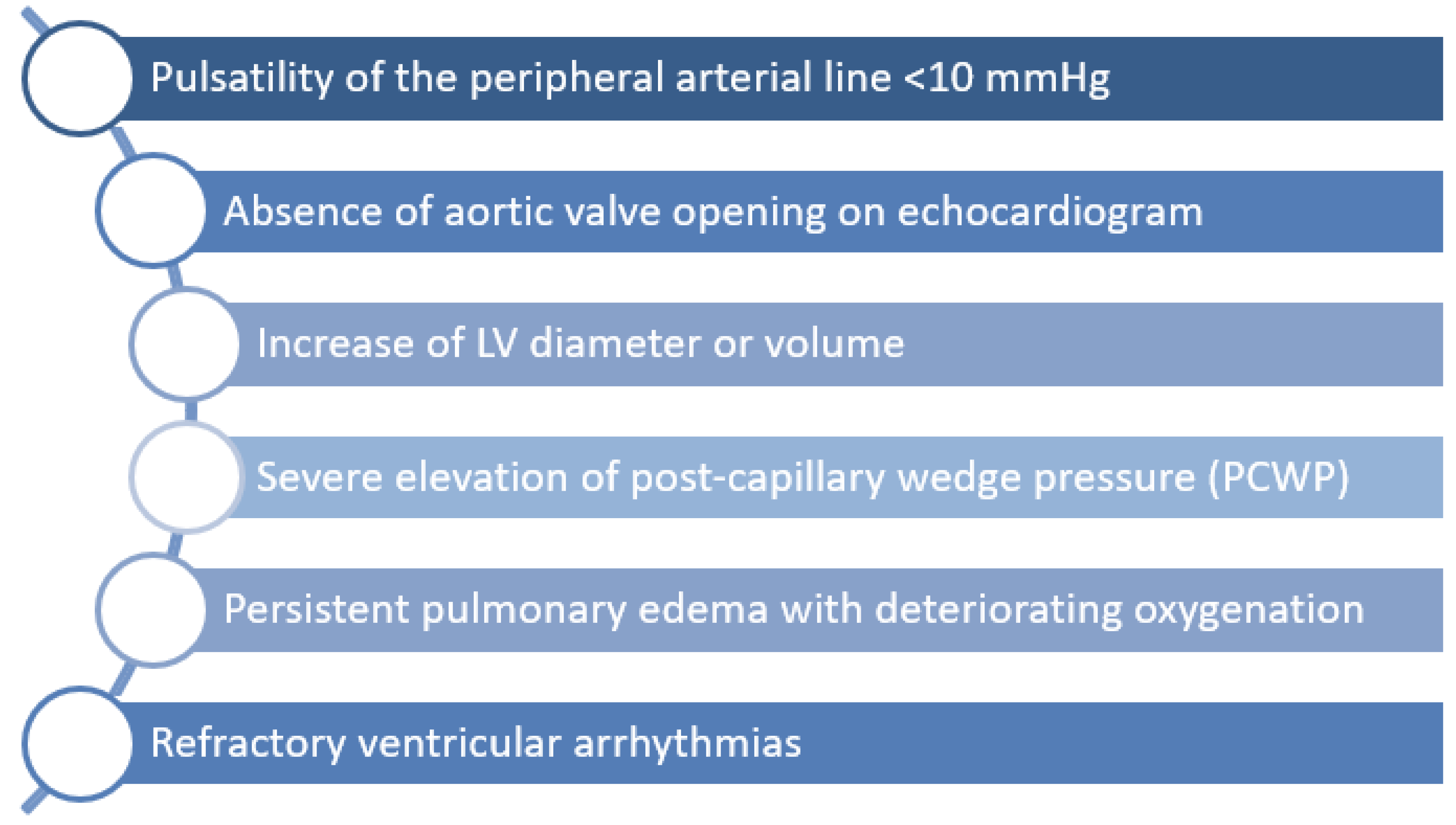
8.4. Inadequate LV Unloading
8.4.1. LV Unloading Using LV Microaxial Flow Pump
8.4.2. LV Unloading Using Intra-Aortic Balloon Counterpulsation
8.4.3. Other Venting Strategies
8.5. Harlequin Syndrome (North-South Syndrome)
9. Weaning and Decannulation
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fox, K.A.A.; Steg, P.G.; Eagle, K.A.; Goodman, S.G.; Anderson, F.A.; Granger, C.B.; Flather, M.D.; Budaj, A.; Quill, A.; Gore, J.M.; et al. Decline in Rates of Death and Heart Failure in Acute Coronary Syndromes, 1999–2006. JAMA 2007, 297, 1892–1900. [Google Scholar] [CrossRef] [Green Version]
- Hochman, J.S.; Buller, C.E.; Sleeper, L.A.; Boland, J.; Dzavik, V.; Sanborn, T.A.; Godfrey, E.; White, H.D.; Lim, J.; LeJemtel, T. Cardiogenic shock complicating acute myocardial infarction--etiologies, management and outcome: A report from the SHOCK Trial Registry. J. Am. Coll. Cardiol. 2000, 36, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Kleber, F.X.; Thiele, H.; Zeymer, U.; Werdan, K.; Rekhraj, S.; Noman, A. Intraaortic Balloon Support for Cardiogenic Shock. N. Engl. J. Med. 2013, 368, 80–81. [Google Scholar] [PubMed]
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.; Vis, M.M.; Wykrzykowska, J.; Koch, K.T.; Baan, J.; et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 69, 278–287. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Christopher, E.B.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef] [Green Version]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; De Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; Mcmullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2016, 63, 60–67. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Sattler, S.; Khaladj, N.; Zaruba, M.-M.; Fischer, M.; Hausleiter, J.; Mehilli, J.; Kääb, S.; Hagl, C.; Massberg, S.; Theiss, H.D. Extracorporal life support (ECLS) in acute ischaemic cardiogenic shock. Int. J. Clin. Pr. 2014, 68, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Sheu, J.-J.; Tsai, T.-H.; Lee, F.-Y.; Fang, H.-Y.; Sun, C.-K.; Leu, S.; Yang, C.-H.; Chen, S.-M.; Hang, C.-L.; Hsieh, Y.-K.; et al. Early extracorporeal membrane oxygenator-assisted primary percutaneous coronary intervention improved 30-day clinical outcomes in patients with ST-segment elevation myocardial infarction complicated with profound cardiogenic shock. Crit. Care Med. 2010, 38, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Brunner, S.; Guenther, S.P.; Lackermair, K.; Peterss, S.; Orban, M.; Boulesteix, A.-L.; Michel, S.; Hausleiter, J.; Massberg, S.; Hagl, C. Extracorporeal Life Support in Cardiogenic Shock Complicating Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 2355–2357. [Google Scholar] [CrossRef] [PubMed]
- Hoebers, L.P.; Vis, M.M.; Claessen, B.; Van Der Schaaf, R.J.; Kikkert, W.J.; Baan, J.; De Winter, R.J.; Piek, J.J.; Tijssen, J.G.; Dangas, G.D.; et al. The impact of multivessel disease with and without a co-existing chronic total occlusion on short- and long-term mortality in ST-elevation myocardial infarction patients with and without cardiogenic shock. Eur. J. Heart Fail. 2013, 15, 425–432. [Google Scholar] [CrossRef]
- Lackermair, K.; Brunner, S.; Orban, M.; Peterss, S.; Orban, M.; Theiss, H.D.; Huber, B.C.; Juchem, G.; Born, F.; Boulesteix, A.-L.; et al. Outcome of patients treated with extracorporeal life support in cardiogenic shock complicating acute myocardial infarction: 1-year result from the ECLS-Shock study. Clin. Res. Cardiol. 2020, 110, 1412–1420. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevationThe Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Ronco, D.; Matteucci, M.; Ravaux, J.M.; Marra, S.; Torchio, F.; Corazzari, C.; Massimi, G.; Beghi, C.; Maessen, J.; Lorusso, R. Mechanical Circulatory Support as a Bridge to Definitive Treatment in Post-Infarction Ventricular Septal Rupture. JACC Cardiovasc. Interv. 2021, 14, 1053–1066. [Google Scholar] [CrossRef]
- Tsao, N.-W.; Shih, C.-M.; Yeh, J.-S.; Kao, Y.-T.; Hsieh, M.-H.; Ou, K.-L.; Chen, J.-W.; Shyu, K.-G.; Weng, Z.-C.; Chang, N.-C.; et al. Extracorporeal membrane oxygenation–assisted primary percutaneous coronary intervention may improve survival of patients with acute myocardial infarction complicated by profound cardiogenic shock. J. Crit. Care 2012, 27, 530.e1–530.e11. [Google Scholar] [CrossRef]
- de Waha, S.; Graf, T.; Desch, S.; Fuernau, G.; Eitel, I.; Pöss, J.; Jobs, A.; Stiermaier, T.; Ledwoch, J.; Wiedau, A.; et al. Outcome of elderly undergoing extracorporeal life support in refractory cardiogenic shock. Clin. Res. Cardiol. 2017, 106, 379–385. [Google Scholar] [CrossRef]
- Pöss, J.; Köster, J.; Fuernau, G.; Eitel, I.; de Waha, S.; Ouarrak, T.; Lassus, J.; Harjola, V.-P.; Zeymer, U.; Thiele, H.; et al. Risk Stratification for Patients in Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 69, 1913–1920. [Google Scholar] [CrossRef]
- Harjola, V.-P.; Lassus, J.; Sionis, A.; Køber, L.; Tarvasmäki, T.; Spinar, J.; Parissis, J.; Banaszewski, M.; Silva-Cardoso, J.; Carubelli, V.; et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur. J. Heart Fail. 2015, 17, 501–509. [Google Scholar] [CrossRef]
- Freund, A.; Pöss, J.; de Waha-Thiele, S.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Feistritzer, H.-J.; Rubini, M.; Huber, K.; Windecker, S.; et al. Comparison of risk prediction models in infarct-related cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 890–897. [Google Scholar] [CrossRef]
- Ceglarek, U.; Schellong, P.; Rosolowski, M.; Scholz, M.; Willenberg, A.; Kratzsch, J.; Zeymer, U.; Fuernau, G.; de Waha-Thiele, S.; Büttner, P.; et al. The novel cystatin C, lactate, interleukin-6, and N-terminal pro-B-type natriuretic peptide (CLIP)-based mortality risk score in cardiogenic shock after acute myocardial infarction. Eur. Heart J. 2021, 42, 2344–2352. [Google Scholar] [CrossRef] [PubMed]
- Muller, G.; Flecher, E.; Lebreton, G.; Luyt, C.-E.; Trouillet, J.-L.; Bréchot, N.; Schmidt, M.; Mastroianni, C.; Chastre, J.; Leprince, P.; et al. The ENCOURAGE mortality risk score and analysis of long-term outcomes after VA-ECMO for acute myocardial infarction with cardiogenic shock. Intensiv. Care Med. 2016, 42, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Burrell, A.; Roberts, L.; Bailey, M.; Sheldrake, J.; Rycus, P.T.; Hodgson, C.; Scheinkestel, C.; Cooper, D.J.; Thiagarajan, R.R.; et al. Predicting survival after ECMO for refractory cardiogenic shock: The survival after veno-arterial-ECMO (SAVE)-score. Eur. Heart J. 2015, 36, 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- Semaan, C.; Charbonnier, A.; Pasco, J.; Darwiche, W.; Etienne, C.S.; Bailleul, X.; Bourguignon, T.; Fauchier, L.; Angoulvant, D.; Ivanes, F.; et al. Risk Scores in ST-Segment Elevation Myocardial Infarction Patients with Refractory Cardiogenic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation. J. Clin. Med. 2021, 10, 956. [Google Scholar] [CrossRef] [PubMed]
- Wengenmayer, T.; Duerschmied, D.; Graf, E.; Chiabudini, M.; Benk, C.; Mühlschlegel, S.; Philipp, A.; Lubnow, M.; Bode, C.; Staudacher, D. Development and validation of a prognostic model for survival in patients treated with venoarterial extracorporeal membrane oxygenation: The PREDICT VA-ECMO score. Eur. Heart J. Acute Cardiovasc. Care 2018, 8, 350–359. [Google Scholar] [CrossRef]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter. Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar]
- Jentzer, J.C.; Schrage, B.; Holmes, D.R.; Dabboura, S.; Anavekar, N.S.; Kirchhof, P.; Barsness, G.W.; Blankenberg, S.; Bell, M.R.; Westermann, D. Influence of age and shock severity on short-term survival in patients with cardiogenic shock. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Schrage, B.; Dabboura, S.; Yan, I.; Hilal, R.; Neumann, J.; Sörensen, N.A.; Goßling, A.; Becher, P.M.; Grahn, H.; Wagner, T.; et al. Application of the SCAI classification in a cohort of patients with cardiogenic shock. Catheter. Cardiovasc. Interv. 2020, 96, E213–E219. [Google Scholar] [CrossRef]
- Jentzer, J.C.; van Diepen, S.; Barsness, G.W.; Henry, T.D.; Menon, V.; Rihal, C.S.; Naidu, S.S.; Baran, D.A. Cardiogenic Shock Classification to Predict Mortality in the Cardiac Intensive Care Unit. J. Am. Coll. Cardiol. 2019, 74, 2117–2128. [Google Scholar] [CrossRef]
- Baran, D.A.; Long, A.; Badiye, A.P.; Rn, K.S. Prospective validation of the SCAI shock classification: Single center analysis. Catheter. Cardiovasc. Interv. 2020, 96, 1339–1347. [Google Scholar] [CrossRef]
- Naidu, S.S.; Baran, D.A.; Jentzer, J.C.; Hollenberg, S.M.; van Diepen, S.; Basir, M.B.; Grines, C.L.; Diercks, D.B.; Hall, S.; Kapur, N.K.; et al. SCAI SHOCK Stage Classification Expert Consensus Update: A Review and Incorporation of Validation Studies: This statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J. Am. Coll. Cardiol. 2022. [Google Scholar] [CrossRef]
- Lee, H.-H.; Kim, H.C.; Ahn, C.-M.; Lee, S.-J.; Hong, S.-J.; Yang, J.H.; Kim, J.-S.; Kim, B.-K.; Ko, Y.-G.; Choi, D.; et al. Association Between Timing of Extracorporeal Membrane Oxygenation and Clinical Outcomes in Refractory Cardiogenic Shock. JACC Cardiovasc. Interv. 2021, 14, 1109–1119. [Google Scholar] [CrossRef]
- Choi, K.H.; Yang, J.H.; Hong, D.; Park, T.K.; Lee, J.M.; Bin Song, Y.; Hahn, J.-Y.; Choi, S.-H.; Choi, J.-H.; Chung, S.R.; et al. Optimal Timing of Venoarterial-Extracorporeal Membrane Oxygenation in Acute Myocardial Infarction Patients Suffering From Refractory Cardiogenic Shock. Circ. J. 2020, 84, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Kolte, D.; Khera, S.; Aronow, W.S.; Mujib, M.; Palaniswamy, C.; Sule, S.; Jain, D.; Gotsis, W.; Ahmed, A.; Frishman, W.H.; et al. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J. Am. Heart Assoc. 2014, 3, e000590. [Google Scholar] [CrossRef] [Green Version]
- Garan, A.R.; Kanwar, M.; Thayer, K.L.; Whitehead, E.; Zweck, E.; Hernandez-Montfort, J.; Mahr, C.; Haywood, J.L.; Harwani, N.M.; Wencker, D.; et al. Complete Hemodynamic Profiling With Pulmonary Artery Catheters in Cardiogenic Shock Is Associated With Lower In-Hospital Mortality. JACC Heart Fail. 2020, 8, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Samuels, L.E.; Kaufman, M.S.; Thomas, M.P.; Holmes, E.C.; Brockman, S.K.; Wechsler, A.S. Pharmacological Criteria for Ventricular Assist Device Insertion Following Postcardiotomy Shock: Experience with the Abiomed BVS System. J. Card. Surg. 1999, 14, 288–293. [Google Scholar] [CrossRef]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.L. Comparison of dopamine and norepinephrine in the treatment of shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Zotzmann, V.; Rilinger, J.; Lang, C.N.; Kaier, K.; Benk, C.; Duerschmied, D.; Biever, P.M.; Bode, C.; Wengenmayer, T.; Staudacher, D.L. Epinephrine, inodilator, or no inotrope in venoarterial extracorporeal membrane oxygenation implantation: A single-center experience. Crit. Care 2019, 23, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Yu, R.-G.; Yin, N.-N.; Zhou, J.-X. Combination of extracorporeal membrane oxygenation and continuous renal replacement therapy in critically ill patients: A systematic review. Crit. Care 2014, 18, 675. [Google Scholar] [CrossRef] [Green Version]
- Fleming, G.M.; Askenazi, D.J.; Bridges, B.C.; Cooper, D.S.; Paden, M.L.; Selewski, D.T.; Zappitelli, M. A multicenter international survey of renal supportive therapy during ECMO: The Kidney Intervention During Extracorporeal Membrane Oxygenation (KIDMO) group. ASAIO J. 2012, 58, 407–414. [Google Scholar] [CrossRef] [Green Version]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary management of cardiogenic shock—A scientific statement. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef]
- Geri, G.; Passouant, O.; Dumas, F.; Bougouin, W.; Champigneulle, B.; Arnaout, M.; Chelly, J.; Chiche, J.-D.; Varenne, O.; Guillemet, L.; et al. Etiological diagnoses of out-of-hospital cardiac arrest survivors admitted to the intensive care unit: Insights from a French registry. Resuscitation 2017, 117, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-S.; Lin, J.-W.; Yu, H.-Y.; Ko, W.-J.; Jerng, J.-S.; Chang, W.-T.; Chen, W.-J.; Huang, S.-C.; Chi, N.-H.; Wang, C.-H.; et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 2008, 372, 554–561. [Google Scholar] [CrossRef]
- Shin, T.G.; Choi, J.-H.; Jo, I.J.; Sim, M.S.; Song, H.G.; Jeong, Y.K.; Song, Y.-B.; Hahn, J.-Y.; Choi, S.-H.; Gwon, H.-C.; et al. Extracorporeal cardiopulmonary resuscitation in patients with inhospital cardiac arrest: A comparison with conventional cardiopulmonary resuscitation. Crit. Care Med. 2011, 39, 1–7. [Google Scholar] [CrossRef]
- Holmberg, M.J.; Geri, G.; Wiberg, S.; Guerguerian, A.-M.; Donnino, M.W.; Nolan, J.; Deakin, C.D.; Andersen, L.W. Extracorporeal cardiopulmonary resuscitation for cardiac arrest: A systematic review. Resuscitation 2018, 131, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Walser, E.; Connett, J.; Murray, T.A.; Collins, G.; Zhang, L.; Kalra, R.; Kosmopoulos, M.; et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 2020, 396, 1807–1816. [Google Scholar] [CrossRef]
- Belohlavek, J. Hyperinvasive Approach In Refractory Out-of-hospital Cardiac Arrest: An Open-label Randomized Controlled Trial. In Proceedings of the American College of Cardiology’s 70th Annual Scientific Session & Expo, Atlanta, GA, USA, 15–17 May 2021. [Google Scholar]
- Rao, S.V.; Jollis, J.G.; Harrington, R.A.; Granger, C.B.; Newby, L.K.; Armstrong, P.W.; Moliterno, D.J.; Lindblad, L.; Pieper, K.; Topol, E.J.; et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004, 292, 1555–1562. [Google Scholar] [CrossRef] [Green Version]
- Combes, A.; Brodie, D.; Chen, Y.-S.; Fan, E.; Henriques, J.P.S.; Hodgson, C.; Lepper, P.M.; Leprince, P.; Maekawa, K.; Muller, T.; et al. The ICM research agenda on extracorporeal life support. Intensiv. Care Med. 2017, 43, 1306–1318. [Google Scholar] [CrossRef]
- Sy, E.; Sklar, M.C.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation practices and the prevalence of major bleeding, thromboembolic events, and mortality in venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis. J. Crit. Care 2017, 39, 87–96. [Google Scholar] [CrossRef]
- Nasr, D.M.; Rabinstein, A.A. Neurologic Complications of Extracorporeal Membrane Oxygenation. J. Clin. Neurol. 2015, 11, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Freund, A.; Jobs, A.; Lurz, P.; Feistritzer, H.-J.; de Waha-Thiele, S.; Meyer-Saraei, R.; Montalescot, G.; Huber, K.; Noc, M.; Windecker, S.; et al. Frequency and Impact of Bleeding on Outcome in Patients With Cardiogenic Shock. JACC Cardiovasc. Interv. 2020, 13, 1182–1193. [Google Scholar] [CrossRef]
- Extracorporeal Life Support Organization. ECLS Registry Report: International Summary. February 2017. Available online: https://www.elso.org/Portals/0/Files/Reports/2017/International%20Summary%20January%202017.pdf (accessed on 4 December 2021).
- Lyu, L.; Yao, J.; Gao, G.; Long, C.; Hei, F.; Ji, B.; Liu, J.; Yu, K.; Hu, Q.; Hu, J. Incidence, Risk Factors, and Outcomes of Hyperbilirubinemia in Adult Cardiac Patients Supported by Veno-Arterial ECMO. Artif. Organs 2017, 42, 148–154. [Google Scholar] [CrossRef]
- Omar, H.R.; Mirsaeidi, M.; Socias, S.; Sprenker, C.; Caldeira, C.; Camporesi, E.M.; Mangar, D. Plasma Free Hemoglobin Is an Independent Predictor of Mortality among Patients on Extracorporeal Membrane Oxygenation Support. PLoS ONE 2015, 10, e0124034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulimov, D.S.; Markuske, M.; Desch, S.; Thiele, H. Management of dead space thrombosis during decannulation of peripherally inserted venoarterial extracorporeal membrane oxygenation. Catheter. Cardiovasc. Interv. 2021, 98, E122–E123. [Google Scholar] [CrossRef]
- Kawashima, D.; Gojo, S.; Nishimura, T.; Itoda, Y.; Kitahori, K.; Motomura, N.; Morota, T.; Murakami, A.; Takamoto, S.; Kyo, S.; et al. Left Ventricular Mechanical Support with Impella Provides More Ventricular Unloading in Heart Failure Than Extracorporeal Membrane Oxygenation. ASAIO J. 2011, 57, 169–176. [Google Scholar] [CrossRef]
- Baldetti, L.; Gramegna, M.; Beneduce, A.; Melillo, F.; Moroni, F.; Calvo, F.; Melisurgo, G.; Ajello, S.; Fominskiy, E.; Pappalardo, F.; et al. Strategies of left ventricular unloading during VA-ECMO support: A network meta-analysis. Int. J. Cardiol. 2020, 312, 16–21. [Google Scholar] [CrossRef]
- Schrage, B.; Becher, P.M.; Bernhardt, A.; Bezerra, H.; Blankenberg, S.; Brunner, S.; Colson, P.; Cudemus Deseda, G.; Dabboura, S.; Eckner, D.; et al. Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study. Circulation 2020, 142, 2095–2106. [Google Scholar] [CrossRef]
- Sauren, L.D.; Reesink, K.D.; Selder, J.L.; Beghi, C.; Van Der Veen, F.H.; Maessen, J.G. The Acute Effect of Intra-aortic Balloon Counterpulsation During Extracorporeal Life Support: An Experimental Study. Artif. Organs 2007, 31, 31–38. [Google Scholar] [CrossRef]
- Kida, H.; Sotomi, Y.; Hikoso, S.; Nakatani, D.; Mizuno, H.; Suna, S.; Okada, K.; Kitamura, T.; Komukai, S.; Dohi, T.; et al. Prognostic significance of intra-aortic balloon pumping support in patients with acute myocardial infarction and veno-arterial extracorporeal membrane oxygenation therapy. J. Cardiol. 2021, 79, 179–185. [Google Scholar] [CrossRef]
- Mlcek, M.; Meani, P.; Cotza, M.; Kowalewski, M.; Raffa, G.M.; Kuriscak, E.; Popkova, M.; Pilato, M.; Arcadipane, A.; Ranucci, M.; et al. Atrial Septostomy for Left Ventricular Unloading During Extracorporeal Membrane Oxygenation for Cardiogenic Shock: Animal Model. JACC Cardiovasc. Interv. 2021, 14, 2698–2707. [Google Scholar] [CrossRef] [PubMed]
- Lüsebrink, E.; Orban, M.; Kupka, D.; Scherer, C.; Hagl, C.; Zimmer, S.; Luedike, P.; Thiele, H.; Westermann, D.; Massberg, S.; et al. Prevention and treatment of pulmonary congestion in patients undergoing venoarterial extracorporeal membrane oxygenation for cardiogenic shock. Eur. Heart J. 2020, 41, 3753–3761. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; Luyt, C.-E.; Leprince, P.; Trouillet, J.-L.; Léger, P.; Pavie, A.; Diebold, B.; Chastre, J.; Combes, A. Predictors of successful extracorporeal membrane oxygenation (ECMO) weaning after assistance for refractory cardiogenic shock. Intensiv. Care Med. 2011, 37, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, D.H.; Daly, A.L.; Luk, A.C.; Fan, E.; Billia, F. Response by Brahmbhatt et al. to Letter Regarding Article, “Liberation From Venoarterial Extracorporeal Membrane Oxygenation: A Review”. Circ. Heart Fail. 2022, 14, e007679. [Google Scholar] [CrossRef]
- Distelmaier, K.; Roth, C.; Schrutka, L.; Binder, C.; Steinlechner, B.; Heinz, G.; Lang, I.M.; Maurer, G.; Koinig, H.; Niessner, A.; et al. Beneficial effects of levosimendan on survival in patients undergoing extracorporeal membrane oxygenation after cardiovascular surgery. Br. J. Anaesth. 2016, 117, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Guilherme, E.; Jacquet-Lagrèze, M.; Pozzi, M.; Achana, F.; Armoiry, X.; Fellahi, J.L. Can levosimendan reduce ECMO weaning failure in cardiogenic shock?: A cohort study with propensity score analysis. Crit. Care 2020, 24, 442. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ECLS-SHOCK | EURO-SHOCK | ANCHOR | |
|---|---|---|---|
| Identifier | NCT03637205 | NCT03813134 | NCT04184635 |
| Sample Size | 420 patients | 428 patients | 400 patients |
| First Patient in | June 2019 | January 2020 | October 2021 |
| Patient enrolment as of January 2022 | 300 | 33 | <10 |
| Main Inclusion Criteria |
|
|
|
| Treatment Arms | Optimal medical therapy vs. VA-ECMO plus optimal medical therapy | Optimal medical therapy vs. Early VA-ECMO plus optimal medical therapy | Optimal medical therapy vs. Early VA-ECMO and IABP plus optimal medical therapy |
| Primary Outcome | All-cause 30-day mortality | All-cause 30-day mortality | Treatment failure at day 30 (death in the ECMO group and death or rescue ECMO in the control group) |
| Special Characteristics | VA-ECMO arm: VA-ECMO insertion preferably prior PCI Non-VA-ECMO arm: Use of other mechanical circulatory support than VA-ECMO possible in case of defined escalation criteria | VA-ECMO arm: VA-ECMO insertion 30 min until 6 h after PCI Non-VA-ECMO arm: IABP insertion not permitted | VA-ECMO arm: VA-ECMO insertion as soon as possible Non-VA-ECMO arm: Use of IABP not recommended, other mechanical circulatory support devices not permitted |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freund, A.; Desch, S.; Pöss, J.; Sulimov, D.; Sandri, M.; Majunke, N.; Thiele, H. Extracorporeal Membrane Oxygenation in Infarct-Related Cardiogenic Shock. J. Clin. Med. 2022, 11, 1256. https://doi.org/10.3390/jcm11051256
Freund A, Desch S, Pöss J, Sulimov D, Sandri M, Majunke N, Thiele H. Extracorporeal Membrane Oxygenation in Infarct-Related Cardiogenic Shock. Journal of Clinical Medicine. 2022; 11(5):1256. https://doi.org/10.3390/jcm11051256
Chicago/Turabian StyleFreund, Anne, Steffen Desch, Janine Pöss, Dmitry Sulimov, Marcus Sandri, Nicolas Majunke, and Holger Thiele. 2022. "Extracorporeal Membrane Oxygenation in Infarct-Related Cardiogenic Shock" Journal of Clinical Medicine 11, no. 5: 1256. https://doi.org/10.3390/jcm11051256
APA StyleFreund, A., Desch, S., Pöss, J., Sulimov, D., Sandri, M., Majunke, N., & Thiele, H. (2022). Extracorporeal Membrane Oxygenation in Infarct-Related Cardiogenic Shock. Journal of Clinical Medicine, 11(5), 1256. https://doi.org/10.3390/jcm11051256