
Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems—Experience from One Center

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment of the Thyroid Hormone Concentration and Anti-Thyroid Antibody Titer
2.3. Thyroid Ultrasonography, Elastography and Fine Needle Aspiration Biopsy
2.4. Data Analysis
3. Results
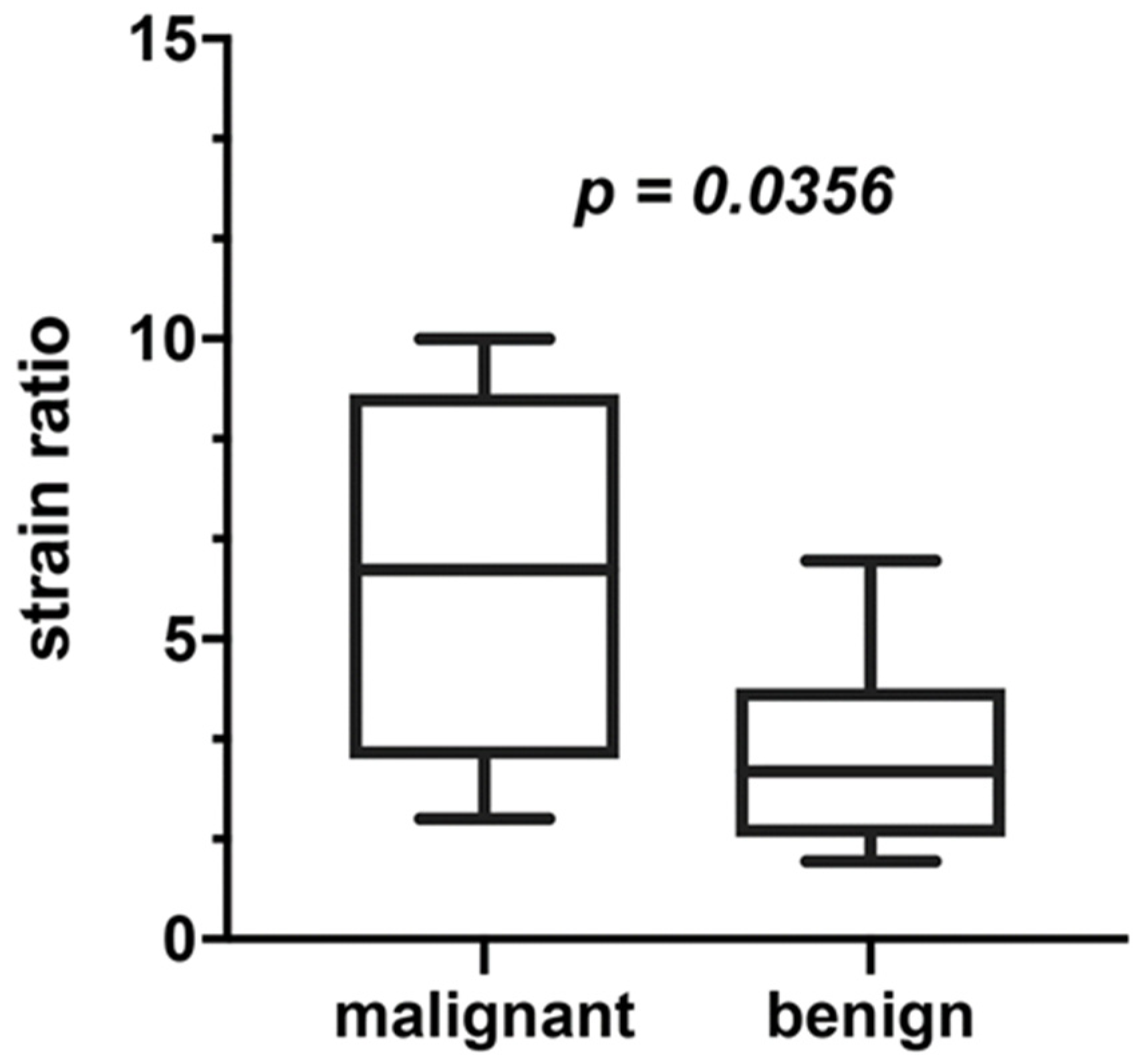
3.1. Elastography
3.2. The ATA, BTA Risk Stratification Systems
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [Green Version]
- Paulson, V.A.; Rudzinski, E.R.; Hawkins, D.S. Thyroid Cancer in the Pediatric Population. Genes 2019, 10, 723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monaco, S.E.; Pantanowitz, L.; Khalbuss, W.E.; Benkovich, V.A.; Ozolek, J.; Nikiforova, M.N.; Simons, J.P.; Nikiforov, Y.E. Cytomorphological and molecular genetic findings in pediatric thyroid fine-needle aspiration. Cancer Cytopathol. 2012, 120, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Essenmacher, A.C.; Joyce, P.H., Jr.; Kao, S.C.; Epelman, M.; Pesce, L.M.; D’Alessandro, M.P.; Sato, Y.; Johnson, C.M.; Podberesky, D.J. Sonographic Evaluation of Pediatric Thyroid Nodules. Radiographics 2017, 37, 1731–1752. [Google Scholar] [CrossRef]
- Niedziela, M.; Handkiewicz-Junak, D.; Małecka-Tendera, E.; Czarniecka, A.; Dedecjus, M.; Lange, D.; Kucharska, A.; Gawlik, A.; Pomorski, L.; Włoch, J.; et al. Diagnostics and treatment of differentiated thyroid carcinoma in children—Guidelines of Polish National Societies. Endokrynol. Pol. 2016, 67, 628–642. [Google Scholar] [CrossRef] [Green Version]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard Ba, G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the management of thyroid cancer.British Thyroid Association. Clin. Endocrinol. 2014, 81, 1–122. [Google Scholar] [CrossRef]
- Xie, C.; Cox, P.; Taylor, N.; LaPorte, S. Ultrasonography of thyroid nodules: A pictorial review. Insights Imaging 2016, 7, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Tritou, I.; Vakaki, M.; Sfakiotaki, R.; Kalaitzaki, K.; Raissaki, M. Pediatric thyroid ultrasound: A radiologist’s checklist. Pediatr. Radiol. 2020, 50, 563–574. [Google Scholar] [CrossRef]
- Januś, D.; Wójcik, M.; Drabik, G.; Wyrobek, Ł.; Starzyk, J.B. Ultrasound variants of autoimmune thyroiditis in children and adolescents and their clinical implication in relation to papillary thyroid carcinoma development. J. Endocrinol. Investig. 2018, 41, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chng, C.L.; Tan, H.C.; Too, C.W.; Lim, W.Y.; Chiam, P.P.S.; Zhu, L.; Nadkarni, N.V.; Lim, A.Y.Y. Diagnostic performance of ATA, BTA and TIRADS sonographic patterns in the prediction of malignancy in histologically proven thyroid nodules. Singap. Med. J. 2018, 59, 578–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russ, G.; Royer, B.; Bigorgne, C.; Rouxel, A.; Bienvenu-Perrard, M.; Leenhardt, L. Prospective evaluation of thyroid imaging reporting and data system on 4550 nodules with and without elastography. Eur. J. Endocrinol. 2013, 168, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Horvath, E.; Majlis, S.; Rossi, R.; Franco, C.; Niedmann, J.P.; Castro, A.; Dominguez, M. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management. J. Clin. Endocrinol. Metab. 2009, 94, 1748–1751. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.; Lee, Y.H.; Lim, H.K.; Moon, W.; Na, D.G.; Park, J.S.; et al. Korean Society of Thyroid Radiology (KSThR) and Korean Society of Radiology. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean Society of Thyroid Radiology consensus statement and recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubaltelli, L.; Corradin, S.; Dorigo, A.; Stabilito, M.; Tregnaghi, A.; Borsato, S.; Stramare, R. Differential Diagnosis of Benign and Malignant Thyroid Nodules at Elastosonography. Ultraschall Med. 2009, 30, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Hoang, J.K.; Middleton, W.D.; Farjat, A.E.; Langer, J.E.; Reading, C.C.; Teefey, S.A.; Abinanti, N.; Boschini, F.J.; Bronner, A.J.; Dahiya, N.; et al. Reduction in Thyroid Nodule Biopsies and Improved Accuracy with American College of Radiology Thyroid Imaging Reporting and Data System. Radiology 2018, 287, 185–193. [Google Scholar] [CrossRef]
- Weller, A.; Sharif, B.; Qarib, M.H.; St Leger, D.; De Silva, H.S.L.; Lingam, R.K. British Thyroid Association 2014 classification ultrasound scoring of thyroid nodules in predicting malignancy: Diagnostic performance and inter-observer agreement. Ultrasound 2020, 28, 4–13. [Google Scholar] [CrossRef]
- Arambewela, M.H.; Wijesinghe, A.M.; Randhawa, K.; Bull, M.; Wadsley, J.; Balasubramanian, S.P. A pragmatic assessment of the British Thyroid Association “U classification” of thyroid nodules with a focus on their follow-up. Clin. Radiol. 2020, 75, 466–473. [Google Scholar] [CrossRef]
- Al-Chalabi, H.; Karthik, S.; Vaidyanathan, S. Radiological-pathological correlation of the British Thyroid Association ultrasound classification of thyroid nodules: A real-world validation study. Clin. Radiol. 2019, 74, 702–711. [Google Scholar] [CrossRef] [Green Version]
- Kanona, H.; Virk, J.S.; Offiah, C.; Stimpson, P. Ultrasound-guided assessment of thyroid nodules based on the 2014 British Thyroid Association guidelines for the management of thyroid cancer—How we do it. Clin. Otolaryngol. 2017, 42, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Radu, T.G.; Ciurea, M.E.; Mogoanta, S.S.; Busuioc, C.J.; Grosu, F.; Ţenovici, M.; Petrescu, I.O.; Vladu, I.M. Papillary thyroid cancer stroma—histological and immunohistochemical study. Rom. J. Morphol. Embryol. 2016, 57, 801–809. [Google Scholar] [PubMed]
- Yi, L.; Qiong, W.; Yan, W.; Youben, F.; Bing, H. Correlation between Ultrasound Elastography and Histologic Characteristics of Papillary Thyroid Carcinoma. Sci. Rep. 2017, 7, 45042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riegler, J.; Labyed, Y.; Rosenzweig, S.; Javinal, V.; Castiglioni, A.; Dominguez, C.X.; Long, J.E.; Li, Q.; Sandoval, W.; Junttila, M.R.; et al. Tumor Elastography and Its Association with Collagen and the Tumor Microenvironment. Clin. Cancer Res. 2018, 24, 4455–4467. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, C.F.; Barr, R.G.; Farrokh, A.; Dighe, M.; Hocke, M.; Jenssen, C.; Dong, Y.; Saftoiu, A.; Havre, R.F. Strain Elastography—How to do it? Ultrasound Int. Open 2017, 3, E137–E149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogan, A.R.; Zhuge, Y.; Perez, E.A.; Koniaris, L.G.; Lew, J.I.; Sola, J.E. Pediatric thyroid carcinoma: Incidence and outcomes in 1753 patients. J. Surg. Res. 2009, 156, 167–172. [Google Scholar] [CrossRef]
- Monpeyssen, H.; Tramalloni, J.; Poirée, S.; Hélénon, O.; Correas, J.M. Elastography of the thyroid. Diagn. Interv. Imaging 2013, 94, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carneiro-Pla, D. Ultrasound Elastography in the evaluation of thyroid nodules for thyroid cancer. Curr. Opin. Oncol. 2013, 25, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Ly, S.; Castroneves, L.A.; Frates, M.C.; Benson, C.B.; Feldman, H.A.; Wassner, A.J.; Smith, J.R.; Marqusee, E.; Alexander, E.K.; et al. A standardized assessment of thyroid nodules in children confirms higher cancer prevalence than in adults. J. Clin. Endocrinol. Metab. 2013, 98, 3238–3245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, Y.D.; Öztürk, V.S.; Ersoz, N.; Anık, A.; Karaman, C.Z. Is Thyroid Imaging Reporting and Data System Useful as an Adult Ultrasonographic Malignancy Risk Stratification Method ın Pediatric Thyroid Nodules? J. Med. Ultrasound 2019, 27, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Piccardo, A.; Fiz, F.; Bottoni, G.; De Luca, C.; Massollo, M.; Catrambone, U.; Foppiani, L.; Muraca, M.; Garaventa, A.; Trimboli, P. Facing Thyroid Nodules in Paediatric Patients Previously Treated with Radiotherapy for Non-Thyroidal Cancers: Are Adult Ultrasound Risk Stratification Systems Reliable? Cancers 2021, 13, 4692. [Google Scholar] [CrossRef]
- Arora, S.; Khoury, J.; Trout, A.T.; Chuang, J. Improving Malignancy Prediction in AUS/FLUS Pediatric Thyroid Nodules with the Aid of Ultrasound. Horm. Res. Paediatr. 2020, 93, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Lim-Dunham, J.E.; Toslak, I.E.; Alsabban, K.; Aziz, A.; Martin, B.; Okur, G.; Longo, K.C. Ultrasound risk stratification for malignancy using the 2015 American Thyroid Association Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Pediatr. Radiol. 2017, 47, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rios, C.; Daneman, A.; Bajno, L.; van der Kaay, D.C.M.; Moineddin, R.; Wasserman, J.D. Utility of adult-based ultrasound malignancy risk stratifications in pediatric thyroid nodules. Pediatr. Radiol. 2018, 48, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Creo, A.; Alahdab, F.; Al Nofal, A.; Thomas, K.; Kolbe, A.; Pittock, S.T. Ultrasonography and the American Thyroid Association Ultrasound-Based Risk Stratification Tool: Utility in Pediatric and Adolescent Thyroid Nodules. Horm. Res. Paediatr. 2018, 90, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Richman, D.M.; Benson, C.B.; Doubilet, P.M.; Wassner, A.J.; Asch, E.; Cherella, C.E.; Smith, J.R.; Frates, M.C. Assessment of American College of Radiology Thyroid Imaging Reporting and Data System (TI-RADS) for Pediatric Thyroid Nodules. Radiology 2020, 294, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.Y.; Amenabar, E.V.; Munoz, A.C.; Vallejo, A.L.; Leon, M.C.; Planes-Conangla, M.; Felip, I.C.; Alvarez, S.C.; Burrieza, G.G.; Campos-Martorell, A. Ultrasound criteria (EU-TIRADS) to identify thyroid nodule malignancy risk in adolescents. Correlation with cyto-histological findings. Endocrinol. Diabetes Nutr. (Engl. Ed.) 2021, 68, 728–734. [Google Scholar] [CrossRef]
- Borysewicz-Sanczyk, H.; Dzieciol, J.; Sawicka, B.; Bossowski, A. Practical Application of Elastography in the Diagnosis of Thyroid Nodules in Children and Adolescents. Horm. Res. Paediatr. 2016, 86, 39–44. [Google Scholar] [CrossRef]
- Cunha, G.B.; Marino, L.C.I.; Yamaya, A.; Kochi, C.; Monte, O.; Longui, C.A.; Cury, A.N.; Fleury, E.D. Elastography for the evaluation of thyroid nodules in pediatric patients. Radiol. Bras. 2019, 52, 141–147. [Google Scholar] [CrossRef]
- Yang, X.; Zhai, D.; Zhang, T.; Zhang, S. Use of strain ultrasound elastography versus fine-needle aspiration cytology for the differential diagnosis of thyroid nodules: A retrospective analysis. Clinics 2020, 75, e1594. [Google Scholar] [CrossRef] [PubMed]
- Hairu, L.; Yulan, P.; Yan, W.; Hong, A.; Xiaodong, Z.; Lichun, Y.; Kun, Y.; Ying, X.; Lisha, L.; Baoming, L.; et al. Elastography for the diagnosis of high-suspicion thyroid nodules based on the 2015 American Thyroid Association guidelines: A multicenter study. BMC Endocr. Disord. 2020, 20, 43. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Chen, J.; Sun, Y.; Xu, F.; Wu, L.; Huang, P. A retrospective study of reducing unnecessary thyroid biopsy for American College of Radiology Thyroid Imaging Reporting and Data Systems 4 assessment through applying shear wave elastography. Arch. Endocrinol. Metab. 2020, 64, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.R.; Song, Y.; Xue, S.S.; Ruan, L.T. Suggested amendment of TI-RADS classification of thyroid nodules by shear wave elastography. Acta Radiol. 2020, 61, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Jing, H.; Han, X.; Shao, H.; Sun, Y.; Wang, Q.; Cheng, W. Shear wave elastography combined with the thyroid imaging reporting and data system for malignancy risk stratification in thyroid nodules. Oncotarget 2017, 8, 43406–43416. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (Mean ± SD) | Malignant (Mean ± SD) | Benign (Mean ± SD) | p | |
|---|---|---|---|---|
| number of patients | 17 a | 5 | 11 | |
| sex (boys/girls) | 4/13 | 1/4 | 3/9 | |
| age (years) | 5–18 (15.29 ± 3.27) | 14–18 (16.4 ± 1.57) | 5–18 (14.8 ± 3.7) | ns |
| history of cervical irradiation | 0/17 | 0/5 | 0/11 | |
| nodular goitre in family history | 4/17 | 1/5 | 3/11 | |
| palpable thyroid nodule | 3/17 | 1/5 | 2/11 | |
| TPO (μlU/L) | 1–367 (92.7 ± 122.3) | 9.4–243 (114.8 ± 118.5) | 1–367 (85.4 ± 129.6) | ns |
| size I (mm) | 3.4–21.0 (12.22 ± 5.6) | 6.0–21.0 (15.3 ± 6.16) | 3.4–17.9 (10.9 ± 5.13) | <0.01 |
| size II (mm) | 2.0–22.6 (10.8 ± 6.6) | 4.5–19.0 (13.1 ± 5.86) | 2.0–22.6 (9.9 ± 6.95) | <0.05 |
| Patient | Sex | Lobe | Nodule Size (mm × mm) | SR | FNAB (Bethesda) | ATA Classification | BTA U Classification | Histopathology |
|---|---|---|---|---|---|---|---|---|
| 1 | F | R | 21 × 15 | 6.3 | VI | high suspicion | U 5b | PTC |
| 2 | M | R | 20 × 17 | 10 | VI | high suspicion | U 5b | PTC |
| 3 | F | R | 6 × 4.5 | 2 | V | high suspicion | U 4d | PTC |
| 4 | F | R | 19 × 17 | nm | V | high suspicion | U 5a | PTC |
| 5 | F | L | 12.5 × 10 | 6 | V | high suspicion | U 5b | PTC |
| 6 | F | R | 7 × 5.7 | 4.7 | IV | high suspicion | U 5a | benign |
| 7 | F | R | 16 × 16 | 3.6 | IV | high suspicion | U 4b | benign |
| 8 | F | R | 17.9 × 7.4 | 4 | III | low suspicion | U 2a | benign |
| 9 | M | R | 6.5 × 4 | 1.7 | III | low suspicion | U 3b | clinical observation |
| 10 | M | L | 22.6 × 15 | 2.6 | III | low suspicion | U 3c | benign in repeated FNAB |
| 11 | F | R | 13 × 9.5 | nm | III | low suspicion | U 3b | follicular adenoma |
| 12 | F | L | 7 × 6 | nm | III | low suspicion | U 3c | benign in repeated FNAB |
| 13 | F | L | 12 × 10 | 6.3 | III | low suspicion | U 3b | benign |
| 14 | M | R | 3.4 × 2 | 3 | III | low suspicion | U 3b | clinical observation |
| 15 | F | R | 6.8 × 5 | 1.7 | III | high suspicion | U 3c | clinical observation |
| 16 | F | R | 5.6 × 4.5 | 1.3 | III | low suspicion | U 3c | benign in repeated FNAB |
| 17 | F | R | 22 × 15 | 2 | III | low suspicion | U 3b | at diagnosis |
| Final Diagnosis Malignant | Final Diagnosis Benign | Sensitivity | Specificity | ||
|---|---|---|---|---|---|
| ATA classification | high suspicion | 100% | 27% | 100.00% 95% CI: 47.82–100.00% | 75.00% 95% CI: 42.81–94.51% |
| intermediate suspicion | - | - | |||
| low suspicion | - | 73% | |||
| very low suspicion | - | - | |||
| benign | - | - | |||
| BTA U classification | U5 | 80% | 9% | 80.00% 95% CI: 28.36–99.49% | 91.67% 95% CI: 61.52–99.79% |
| U4 | 20% | 9% | |||
| U3 | - | 83% | |||
| U2 | - | 9% | |||
| U1 | - | - | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borysewicz-Sańczyk, H.; Sawicka, B.; Karny, A.; Bossowski, F.; Marcinkiewicz, K.; Rusak, A.; Dzięcioł, J.; Bossowski, A. Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems—Experience from One Center. J. Clin. Med. 2022, 11, 1768. https://doi.org/10.3390/jcm11071768
Borysewicz-Sańczyk H, Sawicka B, Karny A, Bossowski F, Marcinkiewicz K, Rusak A, Dzięcioł J, Bossowski A. Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems—Experience from One Center. Journal of Clinical Medicine. 2022; 11(7):1768. https://doi.org/10.3390/jcm11071768
Chicago/Turabian StyleBorysewicz-Sańczyk, Hanna, Beata Sawicka, Agata Karny, Filip Bossowski, Katarzyna Marcinkiewicz, Aleksandra Rusak, Janusz Dzięcioł, and Artur Bossowski. 2022. "Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems—Experience from One Center" Journal of Clinical Medicine 11, no. 7: 1768. https://doi.org/10.3390/jcm11071768
APA StyleBorysewicz-Sańczyk, H., Sawicka, B., Karny, A., Bossowski, F., Marcinkiewicz, K., Rusak, A., Dzięcioł, J., & Bossowski, A. (2022). Suspected Malignant Thyroid Nodules in Children and Adolescents According to Ultrasound Elastography and Ultrasound-Based Risk Stratification Systems—Experience from One Center. Journal of Clinical Medicine, 11(7), 1768. https://doi.org/10.3390/jcm11071768