1. Introduction
Prader–Willi syndrome was described for the first time by Prader, Labhart and Willi in 1956 and is considered the most common genetic cause of obesity. The incidence is estimated to be around 1 in 20,000 live births, and the population prevalence is about 1 in 50,000 [
1]. The syndrome is caused by the loss of function of paternal genes on chromosome 15q11-q13 due to: (i) de novo paternal deletion of this region (65–75% of affected individuals); (ii) maternal uniparental disomy of chromosome 15 (20–30%); or (iii) an imprinting defect on the paternal chromosome resulting in the silence of the paternal alleles (1–3%) [
1]. PWS is characterised by severe neonatal hypotonia and poor suck, feeding disorders (hyperphagia and lack of satiety) and early-onset childhood weight gain, often leading to obesity. Other characteristics include scoliosis, dysmorphic features, cognitive impairment and behavioural problems [
1,
2]. There is a large body of evidence to suggest common pathophysiology linked to hypothalamic dysfunction [
2], implicated in many PWS manifestations, such as hyperphagia, multiple endocrine deficiencies (above all hypogonadism and growth hormone deficiency), temperature instability and high pain threshold. The hypothalamus is also implicated in sleep/wake regulation and in the control of breathing. Accordingly, sleep abnormalities are frequent in PWS and begin in childhood [
3,
4]. These disturbances include sleep-disordered breathing (SDB) and central disorders of hypersomnolence. In both cases, the principal symptom reported by the patients themselves is sleepiness, which negatively affects the quality of life [
5,
6,
7]. The expert’s role is to classify the severity of this sleepiness according to its frequency and impact on daily activities to determine whether or not it is clinically excessive.
The aim of this review is to summarise current knowledge of the characteristics, diagnosis and treatment options of sleep disorders in PWS to provide the clinician with a practical tool for managing patients with PWS. We focus primarily on excessive daytime sleepiness (EDS), the main sleep-related symptom of PWS, detailing the clinical assessment of PWS patients. We then go on to address the two main causes of EDS in PWS—SDB and central disorders of hypersomnolence. In keeping with our background and experience, we focused on adults.
2. Materials and Methods
This article is the result of a long, close clinical and scientific collaboration between the National Reference Center for “Prader–Willi syndrome and rare obesities with eating disorders” (PRADORT) and the National Reference Center for Narcolepsy and Rare Hypersomnias in Pitié-Salpêtrière hospital (Sorbonne University), Paris, France. Comprehensive research of electronic literature on the PubMed/MEDLINE and Embase databases was conducted to find relevant, English-language published articles. The following medical subject headings (MeSH terms and not) were used: “sleepiness”, “excessive daytime sleepiness”, “sleep disorders”, “sleep abnormalities”, “sleep disturbances”, “sleep-related disorders”, “polysomnography”, “sleep study”, “insomnia”, “hypersomnia”, “narcolepsy”, “sleep-onset REM”, “cataplexy”, “orexin-A”, “hypocretin-1”, “modafinil”, “melatonin”, “circadian system”, “circadian rhythm”, “parasomnia”, “rhythm disorders”, “central apnea”, “obstructive apnea”, “ sleep apnea”, “sleep hypoventilation”, “sleep hypoxemia”, “hypoventilation”, “breathing sleep disordered”, “non-invasive ventilation”, “continuous positive airway pressure” [AND] “Prader-Willi syndrome”. The most relevant studies were selected by a group of expert neurologists and pulmonologists if at least one of the following topics was covered: (i) the main sleep-related symptom including sleepiness or excessive daytime sleepiness, detailing clinical examination, and questioning of patients and caregivers and the main tools for assessing sleep disorders; (ii) the SDB and its treatment, and (iii) the diagnosis and treatment of central disorders of hypersomnolence. The vastness and complexity of the subject led us to conduct a narrative review. This choice was also made on account of the great diversity of study designs in the published articles, including numerous case reports and multiple case series with a small number of patients.
3. Results
After eliminating 56 duplicates, 316 articles published between 1971 and 2021 were found. After reading the abstracts of each of these articles, 241 were discarded because they did not fit our inclusion criteria. We then read each of the remaining 75 articles, eliminating the irrelevant and redundant ones, to finally select only 47 articles to complete this narrative review.
3.1. Excessive Daytime Sleepiness
3.1.1. Clinical Characteristics
Daytime sleepiness is the desire to fall asleep during the day. The expert’s role is to determine whether or not the patient is experiencing daytime sleepiness, to classify the severity of this sleepiness according to its frequency and impact on daily activities, and to determine whether or not it is clinically excessive. EDS is defined as such by the urge to sleep at abnormal times during the day, often resulting in involuntary lapses into sleep, called sleep attacks. EDS is particularly marked in passive situations (including reading, sitting or watching TV), but it can also occur in active situations (including working, eating or driving a vehicle).
EDS is the most frequent sleep-related symptom of PWS and is, at least partly, specific to PWS. In a study comparing sleep disorders in patients with different intellectual disabilities, EDS and daytime napping differentiated children with PWS from children with autism, Down Syndrome and familial intellectual disability [
5]. Previous evidence from our group supports the relevance of this symptom determined through face-to-face interviews with patients and caregivers in 40 out of 60 (67%) adults with PWS [
8]. Similar results on the high frequency of EDS in PWS patients are reported in a clinical review pooling 12 studies based on questionnaires or interviews [
9]. EDS begins in early infancy and seems to worsen in adulthood [
10,
11], with significant negative consequences for the quality of life of patients and their families [
4,
5], on the ability to focus, and detrimental effects on daily routines and daytime activity when napping becomes too frequent. Consequently, patients with decreased activity gain weight. EDS is an invisible handicap that is often misunderstood.
In addition to EDS, the spectrum of hypersomnolence includes hypersomnia, which is defined in its strict sense as longer sleep time (more than 11 h of sleep per 24 h). However, this manifestation was reported in only 3 out of 60 patients in our above-mentioned cohort study from our research group [
8].
The Epworth Sleepiness Scale (ESS) is a self-administered questionnaire routinely used to measure a patient’s sleepiness, but it has some limitations in patients with PWS, who may be too cognitively impaired to understand all the questions, even when supported by the caregivers. Indeed, in the assessment of sleepiness in adults with PWS, our group found low sensitivity of the ESS since 22% of patients determined as sleepy in the face-to-face interview had a normal (<11–24) score on the ESS [
8]. On the other hand, specificity was good since only 1 patient out of 60 scored more than 10 on the ESS and did not complain of excessive sleepiness in the interview. These data suggest that ESS alone is an insufficient gauge of EDS, and the information it provides should be supplemented by face-to-face interviews with patients and caregivers.
3.1.2. Sleep Recording
Overnight polysomnography combined with transcutaneous monitoring of carbon dioxide pressure is performed to assess SDB, including obstructive and central sleep apnoea and hypopnoea, as well as sleep hypoxemia and sleep hypoventilation. Night recording is followed by the multiple sleep latency test (MSLT), which corresponds to five 20-min-long nap opportunities performed from 8 am to 4 pm. An abnormal propensity to fall asleep during daytime is determined when the mean sleep onset latency is shorter than or equal to 8 min. In addition, it is considered abnormal to present two or more naps containing rapid eye movement (REM) sleep within 15 min after sleep onset (sleep-onset REM sleep periods (SOREMPs)). The combination of a daytime mean sleep onset latency below 8 min and 2 or more SOREMPs defines the narcolepsy phenotype. Abnormally long sleep time can be objectively documented using bed rest 24-h protocols, consisting of (after a habituation night followed by MSLT) second overnight polysomnography followed by full day polysomnography, allowing patients to nap as long as they can in the morning and in the afternoon [
12]. A total daily sleep time greater than 11 h during 24-h bed rest condition is considered as abnormal, representing an objective marker of central hypersomnia.
EDS is, therefore, the most frequent sleep-related symptom in patients with PWS and can result from SDB, central disorders of hypersomnolence or both.
3.2. Sleep-Disordered Breathing: Sleep Apnoea, Sleep Hypoxemia and Sleep Hypoventilation
3.2.1. Pathophysiology
The efficiency of the respiratory system in maintaining normal levels of oxygen and carbon dioxide in the blood is determined by the efficiency of ventilatory control functions and the mechanical properties of the respiratory system [
13]. During sleep, ventilatory control is less effective against an increased respiratory load. Patients with PWS show impaired ventilatory control [
14,
15], together with multiple physical traits that contribute to suboptimal pulmonary mechanics, including hypotonia [
16], respiratory muscle weakness [
16], scoliosis [
17] and obesity [
18]. Moreover, hypotonia of upper airway muscle and fat deposition in the pharyngeal wall in association with increased upper airway collapsibility due to lung volume reduction may predispose patients to obstructive sleep apnoea. As a consequence, respiratory abnormalities are frequent and can be severe in patients with PWS, in particular during sleep [
19].
Ventilatory control abnormalities. Abnormal ventilatory control may play a significant role in the pathophysiology of SDB and has been observed in PWS patients during both wakefulness and during sleep. During wakefulness, the hypoxic ventilatory response is absent or reduced, and the hypercapnic ventilatory response is blunted in obese subjects with PWS [
20]. Because arousal from sleep after rapidly developing hypoxia and hypercapnia requires intact peripheral chemoreceptor function, hypoxic [
14] and hypercapnic [
15] arousal responses during sleep are weakened in PWS. These elevated hypercapnic arousal thresholds during sleep predispose patients to sleep hypoxemia, sleep hypoventilation and sleep apnoea and can negatively affect the course of respiratory infections or respiratory disorders in these patients. These conditions represent a common cause of death in PWS patients [
21].
Hypotonia and respiratory muscle weakness. Hypotonia and decreased lean muscle mass characterising PWS may lead to decreased respiratory muscle strength and upper airway tone, particularly during sleep, predisposing patients to sleep hypoventilation and obstructive sleep apnoea, respectively. Moreover, the restrictive ventilatory impairment described in obese and non-obese PWS patients [
16] is thought to be due, at least in part, to reduced ventilatory muscle strength.
Scoliosis. Scoliosis, which alters chest wall mechanics, contributes to the restrictive ventilatory defect in PWS, impairing pulmonary function and increasing the likelihood of alveolar hypoventilation [
17].
Obesity. Obesity is another factor contributing to the restrictive ventilatory defect in PWS. Lung volume reduction is due to the effect of excess weight on the expansion of the chest wall and the downward movement of the diaphragm toward the abdomen. Lung volume reduction is also associated with increased upper airway collapsibility, which predisposes patients to obstructive sleep apnoea. Moreover, obesity is also associated with increased upper airway resistance in relation to fat deposition in the pharyngeal wall. Most PWS patients develop hyperphagia and morbid obesity during childhood and adulthood. Consequently, the phenotype of SDB evolves over time from predominantly central sleep apnoea in infants to obstructive sleep apnoea in older children, adolescents and adults [
18]. Obesity is also considered a major cause of sleep-related hypoxemia and hypoventilation in PWS.
3.2.2. Epidemiology
Adults with PWS have a higher rate of sleep apnoea, sleep hypoxemia and sleep hypoventilation compared to controls matched for age, sex distribution and body mass index (BMI) [
19]. A study of 19 adult and adolescent PWS patients revealed that 21% had severe obstructive sleep apnoea (OSA, defined by more than 30 apnoea or hypopnoea episodes per hour of sleep), and 47% had sleep hypoventilation [
19]. In addition, sleep hypoxemia was more common in PWS patients compared to the control group, together with stronger evidence of lower oxyhaemoglobin saturations and percentages of sleep time spent at less than 80% oxyhaemoglobin saturation [
19]. In accordance with this study, in our previously mentioned cohort of 60 adults with PWS, we found 20% of patients with moderate-to-severe OSA, which was being treated in only half of the cases [
8]. In addition, one patient had isolated sleep hypoxemia, whereas 8% of patients presented hypoventilation [
8].
3.2.3. Sleep Recording
Full-night polysomnography combined with transcutaneous monitoring of carbon dioxide pressure (PtcCO
2) is the gold standard for the diagnosis of SDB, allowing the identification and the exact graduation of sleep apnoea, sleep hypoxemia and sleep hypoventilation, which are defined according to the following international criteria [
22]: (1) untreated sleep apnoea as an apnoea–hypopnoea index > 15/h; (2) treated sleep apnoea as an apnoea–hypopnoea index < 5/h on a sleep study performed with continuous positive airway pressure (CPAP) and a CPAP adherence > 4 h/day; (3) sleep hypoxemia as >5 min of sleep with SpO
2 < 88%; and (4) sleep hypoventilation as ≥10 min of sleep with PtcCO
2 ≥ 55 mmHg or ≥50 mmHg in the presence of an increase >10 mmHg, as compared to the awake prone position. In the case of sleep hypoventilation, diurnal arterial blood gas analysis is used to evaluate if hypoventilation is also present during wakefulness (diurnal PaCO
2 > 45 mmHg). At this point, an initial MSLT is recommended to objectively assess baseline EDS. In patients with behavioural disorders who cannot tolerate technically complex sleep recording with a large number of sensors, a basic assessment combining ventilatory polygraphy and diurnal arterial blood gas analysis can be proposed.
3.2.4. Clinical Characteristics
Interestingly, many patients with polysomnography-confirmed OSA may not report any obvious OSA-associated symptoms [
23]. In our cohort of 60 adult PWS patients, the symptoms usually related to SDB (heavy snoring, witnessed apnoea, nocturia, morning headaches) were common, although not specifically associated with the presence of objective SDB [
8], showing low sensitivity in PWS. Clinicians should, therefore, anticipate and investigate OSA. Moreover, SDB in PWS patients has been associated with some behavioural disturbances, such as autism-like manifestations and impulsiveness [
10].
3.2.5. Growth Hormone
Failure to grow due to defects in growth hormone (GH) secretion has been described in patients with PWS [
24,
25]. Therefore, GH replacement therapy is currently used from childhood to improve the phenotypic appearance of subjects affected by PWS. GH treatment increases adult height, and studies in adults with PWS have consistently reported improved body composition, muscle mass, exercise capacity, as well as beneficial effects on neurocognitive functions and quality of life [
23,
24]. However, concerns have been raised following reports of sudden death that occurred shortly after GH initiation and were attributed to worsened OSA due to adenotonsillar hypertrophy [
15]. Consequently, some randomised control trials have been conducted to investigate the effects of GH treatment on SDB. The results showed that GH does not cause a significant increase in the apnoea–hypopnoea index, indicating that GH can be safely administered [
26,
27]. Nevertheless, current recommendations point to the necessity of multidisciplinary evaluation, including sleep recording in PWS patients before starting GH treatment.
3.2.6. Treatments
Continuous positive airway pressure (CPAP) ventilation is the first-line treatment of OSA in PWS adults, reported to be very effective in normalising respiration during sleep [
28,
29]. Nevertheless, compliance with CPAP treatment is low [
30]. In patients with hypoventilation with or without sleep apnoea, non-invasive ventilation (NIV) is indicated. Considering the high prevalence of intellectual disability and behavioural disorders, establishing successful therapy with CPAP or, alternatively, NIV in PWS continues to pose a challenge.
3.2.7. Residual Excessive Daytime Sleepiness
Treatment of OSA with CPAP leads to an improvement in EDS, according to a parental report [
29,
31,
32,
33]. Still, EDS can persist in some PWS patients even after OSA treatment [
8]. There is also evidence to suggest that EDS can be disproportionate to the severity of the respiratory disturbance [
30]. A retrospective study by Williams et al. found no significant correlation of sleepiness, evaluated by MSLT and ESS, with the apnoea–hypopnoea index (AHI). The authors also showed that EDS can be present in PWS patients without SDB, indicating that SDB alone cannot be the only causative trigger of EDS in PWS patients [
34]. A sleep analysis by Vela Bueno et al. in nine PWS patients reported for the first time that, although most of them had symptoms of EDS, none experienced significant sleep apnoea [
5].
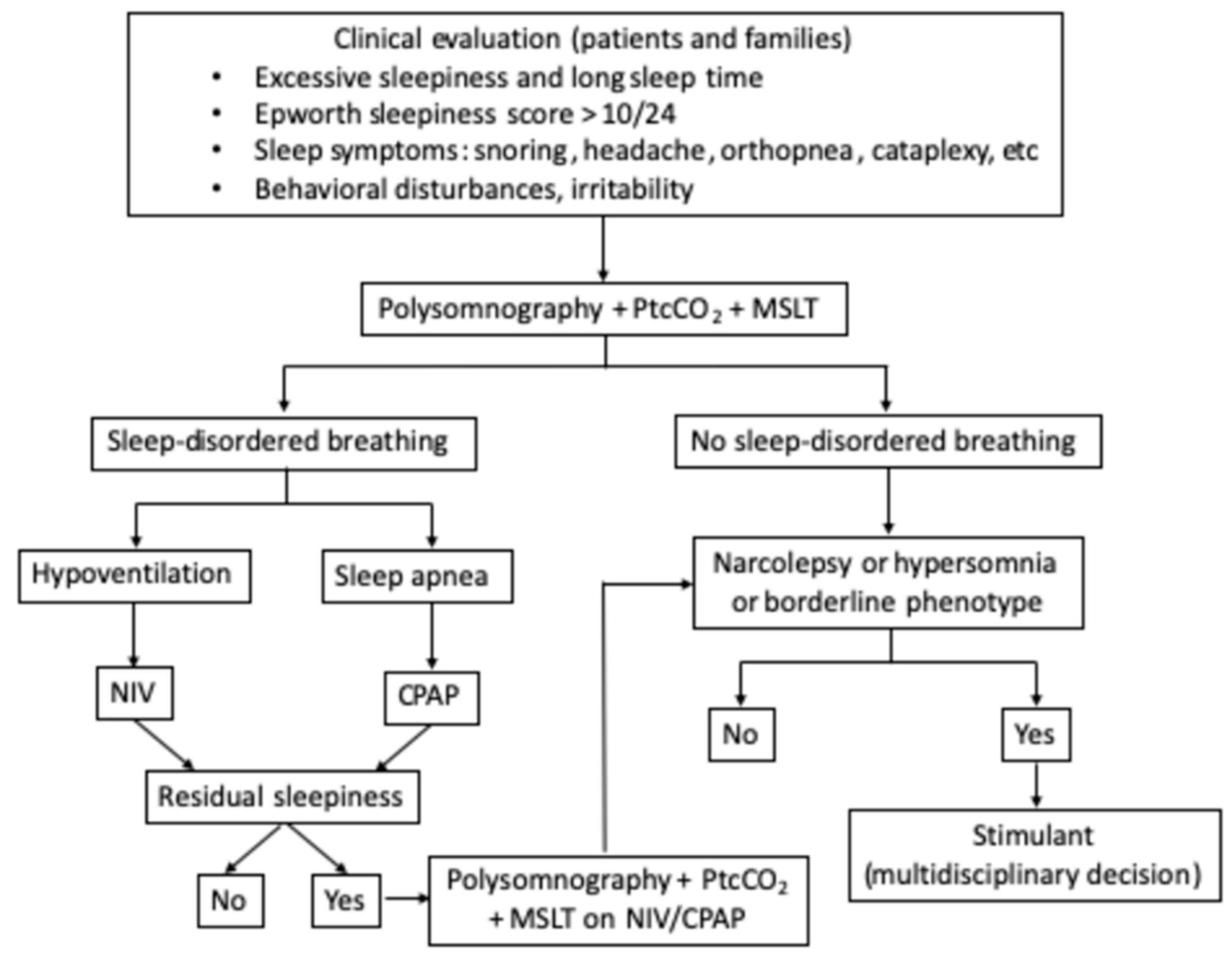
In conclusion, considering the high prevalence of SDB and its potentially severe consequences in adults with PWS, systematic screening and targeted treatment are highly recommended in these patients. Residual EDS after control of respiratory disturbance during sleep is common, and it should be properly investigated to identify and treat the other causes of EDS (
Figure 1).
3.3. Central Disorders of Hypersomnolence
3.3.1. Pathophysiology
Central disorders of hypersomnolence can result from a dysfunction of the hypothalamus, which contains two main arousal systems, the hypocretin and histamine neurons. The hypocretin neurons, involved in wakefulness and arousal [
35], are damaged in narcolepsy with and without cataplexy. In PWS, many of the genes located in the lost region of paternal chromosome 15q11–q13 are expressed highly in the hypothalamus and are potential regulators of mammalian sleep and sleep-mediated metabolism [
36]. This hypothesis is supported by animal models. Specifically, microdeletion of the small nuclear RNA 116 (SNORD116) cluster within the PWS locus in mice causes an EEG profile characterised by the intrusion of rapid eye movement (REM) sleep episodes during the transition between wakefulness and sleep, associated with an increase in body temperature [
37]. With regard to humans, a meta-analysis confirmed that PWS patients have lower hypocretin levels in cerebrospinal fluid compared with normal subjects but higher hypocretin levels than patients with primary narcolepsy [
38]. In PWS patients, decreased levels of cerebrospinal fluid hypocretin predict greater EDS [
39]. A study of 8 PWS adults, 3 PWS infants, and 11 controls post-mortem failed to find hypocretin deficiency in PWS brains since no difference in the hypocretin cell number or staining intensity was observed between affected cases and controls. However, these data should be taken with caution in view of the limited sample size and lack of information about the EDS status of patients [
40].
3.3.2. Epidemiology and Sleep Recording
Different definitions have been used to objectively describe central disorders of hypersomnolence in PWS, which hampers a rigorous comparison of the available studies. Multiple case reports [
32,
41] and studies of small groups [
31,
42] have found excessive sleepiness in the MSLT, often associated with SOREMPs. In a review based on eight studies, Camfferman et al. reported that 29 (40%) out of 72 PWS patients (19 children and 53 adults) had a documented EDS (defined as a mean sleep onset latency < 5 min at MSLT) 9 [
7]. Our previous data by Ghergan et al. in 60 adult PWS patients found an objective EDS (defined as mean sleep onset latency < 8 min at MSLT) in 13 (22%) of them [
8]. This lower difference may be explained by the systematic aspect of our study. All patients underwent the sleep study even when not complaining of sleep disorder or EDS, which was not the case in the former study.
Several studies emphasised the probable deregulation of REM sleep [
43,
44]. In 11–21 (52%) patients with PWS [
43], REM sleep abnormalities including SOREMPs, REM sleep during daytime naps, fragmented REM sleep and a decrease in the percentage of REM sleep during the night were observed.
In total, 43% (26 out of 60) of our 60 PWS adult patients in the study by Gerghan et al. displayed an isolated central disorder of hypersomnolence, which included different profiles: (i) 35% had secondary narcolepsy (MSLT ≤ 8 min and 2 or more SOREMPs); (ii) 12% had hypersomnia (including N = 2 with total sleep time > 11 h, and N = 1 with MSLT ≤ 8 min and 0 or 1 SOREMPs,
n = 1), and 53% had a borderline phenotype (including N = 10 with ≥2 SOREMPs and MSLT > 8 min, and N = 4 with MSLT between 8 and 10 min). These established and borderline phenotypes in a genetic disease are suggestive of a hypersomnia spectrum disorder. No genetic, clinical or biological determinant was associated with the presence of central disorders of hypersomnolence [
8]. The finding that the HLA DQB1*0602 genotype is strongly associated with primary narcolepsy but not with PWS [
8,
43,
45] is of particular interest.
There are some limitations to the generalisation of our study because this kind of detailed and prolonged assessment may not be feasible in all centres, but the results here suggest that nighttime polysomnography (including CO2 monitoring) followed by systematic MSLT is sufficient to screen all sleep disorders in patients with PWS. Other studies need to be performed to confirm these data.
3.3.3. Clinical Characteristics
EDS is the principal symptom of central disorders of hypersomnolence, but there are no specific clinical features to differentiate between the respiratory or neurological origin of EDS. However, in a central disorder of hypersomnolence, EDS tends to be more severe, with sleep lapses occurring several times per day, plus more brutal and irrepressible sleepiness, culminating in sleep attacks [
8]. The dysfunction of REM sleep regulation can be associated with episodes of sleep–wake state dissociation such as cataplexies, sleep paralysis or sleep-related hallucinations. Cataplexy, which is a medical condition characterised by sudden and brief muscle weakness caused by strong emotion or laughter, has been described in some children and adults with PWS [
31,
43,
46]. In our previous study of 60 adults with PWS, five patients exhibited partial or complete cataplexy, all showing a narcolepsy phenotype during sleep recording [
8]. The other symptoms, such as sleep paralysis and hypnagogic hallucinations, are rarely reported in the literature. In our cohort, sleep paralysis was observed in two patients (one narcolepsy and one SOREMPs disorder in MSLT). None had hypnagogic hallucinations [
8].
3.3.4. Treatment
To our knowledge, there are no randomised studies evaluating the benefit and tolerance of a specific treatment of EDS in PWS. Consequently, the management of central disorders of hypersomnolence is only based on expert opinion and case reports. It is nevertheless necessary to take them into consideration because the expected benefits are multiple. Improved vigilance raises levels of concentration and the ability to take part in social or learning activities [
47,
48]. This contributes to increased self-esteem and better quality of life [
47]. For this purpose, sleep experts treating PWS patients must be accustomed to using stimulants and wake-enhancing treatments in primary central disorders of hypersomnolence and must be aware of the specificity of these patients. Indeed, they are more exposed than others to the risk of adverse events due to the other symptoms of PWS, such as cognitive and behavioural disorders. In addition, all of the proposed stimulants and wake-enhancing drugs (except pitolisant) may have the potential to increase cardiovascular risk, which must be taken into consideration given the prevalence of obesity in this population. A careful assessment of the benefit/risk ratio of treatments is important. Sleep experts and PWS experts must work together closely to obtain the best benefits and avoid adverse effects. An overview of the different possible treatments is described below.
Sleep hygiene. A regular sleep–wake rhythm with a sufficient number of sleep hours is recommended. All those factors that can degrade sleep quality should be limited (tobacco, use of electronic devices in the evening, etc.). In addition, short naps of less than an hour can be refreshing and helpful if possible. However, these sleep hygiene measures are often insufficient, and in this case, a wake-enhancing may be required.
Wake-enhancing treatment. Modafinil and pitolisant are employed in current practice as stimulants in primary narcolepsy. These therapies have also been used for reducing EDS in PWS. To our knowledge, there are no randomised studies evaluating the benefit and tolerance of these stimulants in PWS, but there is some evidence confirming their usefulness [
47,
48,
49,
50]. A careful assessment of the benefit/risk ratio of stimulants and monitoring of the side effects are important when starting and following up treatment. In the authors’ opinion, the use of classical stimulants including methylphenidate, solriamfetol or dexamphetamine cannot be recommended at this point, in the absence of data on benefit and because they carry a higher risk of adverse cardiovascular effects than modafinil and pitolisant.
Modafinil. Modafinil is a non-amphetamine central stimulant with an unknown mechanism of action that selectively promotes alertness and is not associated with dependence or tolerance [
49]. Various case reports and an open-label pilot study showed positive efficacy (reduced ESS score) without side effects in nine children and adolescents with PWS complaining of EDS (without SDB) [
50]. In the mentioned study by our group, Gerghan et al. described 16 adults in the 60 PWS cohort who received a low dose of modafinil (between 100 mg and 200 mg/day). The levels of sleepiness in fourteen patients showed long-lasting improvement (ESS score decreased from 14 to 9, which was statistically and clinically significant), according to caregivers and patients. The benefit was maintained for 3.6 ± 3.1 years. The main side effects were psychological (repeated panic attacks in one patient and depressive mood in another one), occurring early after treatment start, and later (anxiety, aggressiveness, and delusional episodes), which stopped when the drug was withdrawn. Caution should be exercised regarding potential interaction with other drugs, as modafinil is an enzyme inducer. Modafinil has no impact on weight gain or loss.
Pitolisant. Pitolisant is a first-in-class histamine H3 receptor inverse agonist that enhances the activity of histaminergic neurons. This effective treatment for EDS is tolerated better than the standard-of-care drug modafinil. In three case series, although the children with PWS had not received a diagnosis of narcolepsy, parents reported that upon treatment with pitolisant, the children were not only less sleepy but also more active and more engaged [
47]. Pitolisant was given to two patients who stopped modafinil because of the side effects, one reporting positive benefits and no side effects, and one lost to follow-up [
8]. There is a theoretical risk of weight gain associated with increased appetite, as observed in some patients with primary narcolepsy.
4. Conclusions
Sleep examinations should be performed routinely on PWS patients. Indeed, as illustrated in this article, both respiratory and neurological sleep disorders are common in adults with PWS and are associated with EDS. This EDS impacts neurocognitive and psychological functions and possibly results in behavioural disorders. A clinical and instrumental assessment of sleep disorders should be carried out in a multidisciplinary expert sleep centre to customise treatment using a patient-tailored approach, with potential positive clinical and social implications for PWS patients and their families.
Author Contributions
P.D., F.S., S.L.-S., S.R., C.P. and A.B. conceived and designed the manuscript. P.D., F.S. and S.R. collected and analysed the data. P.D., F.S., S.R., S.L.-S., M.C., A.B., I.A. and C.P. drafted the manuscript, which was reviewed and approved by all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
P.D. received funds for travel to conferences by UCB Pharma, F.S. declares no conflict of interest, S.L.-S. received funds for travel to conferences by UCB Pharma, M.C. declares no conflict of interest, A.B. declares no conflict of interest, I.A. declares no conflict of interest, C.P. declares no conflict of interest, S.R. declares no conflict of interest.
References
- Bar, C.; Diene, G.; Molinas, C.; Bieth, E.; Casper, C.; Tauber, M. Early diagnosis and care is achieved but should be improved in infants with Prader-Willi syndrome. Orphanet J. Rare Dis. 2017, 12, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tauber, M.; Hoybye, C. Endocrine disorders in Prader-Willi syndrome: A model to understand and treat hypothalamic dysfunction. Lancet Diabetes Endocrinol. 2021, 9, 235–246. [Google Scholar] [CrossRef]
- Passone, C.B.G.; Pasqualucci, P.L.; Franco, R.R.; Ito, S.S.; Mattar, L.B.F.; Koiffmann, C.P.; Damiani, D. Prader-Willi Syndrome: What Is the General Pediatrician Supposed to Do?—A Review. Rev. Paul Pediatr. 2018, 36, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, H.-L.; Urquhart, D. Respiratory Complications in Children with Prader Willi Syndrome. Paediatr. Respir. Rev. 2017, 22, 52–59. [Google Scholar] [CrossRef]
- Vela-Bueno, A.; Kales, A.; Soldatos, C.R.; Dobladez-Blanco, B.; Campos-Castello, J.; Espino-Hurtado, P.; Olivan-Palacios, J. Sleep in the Prader-Willi Syndrome. Clinical and polygraphic findings. Arch. Neurol. 1984, 41, 294–296. [Google Scholar] [CrossRef]
- Clarke, D.J.; Waters, J.; Corbett, J.A. Adults with Prader-Willi Syndrome: Abnormalities of Sleep and Behaviour. J. R. Soc. Med. 1989, 82, 21–24. [Google Scholar] [CrossRef] [Green Version]
- Cotton, S.; Richdale, A. Brief report: Parental descriptions of sleep problems in children with autism, Down syndrome, and Prader–Willi syndrome. Res. Dev. Disabil. 2006, 27, 151–161. [Google Scholar] [CrossRef]
- Ghergan, A.; Coupaye, M.; Leu-Semenescu, S.; Attali, V.; Oppert, J.-M.; Arnulf, I.; Poitou, C.; Redolfi, S. Prevalence and Phenotype of Sleep Disorders in 60 Adults with Prader–Willi Syndrome. Sleep 2017, 40, 40. [Google Scholar] [CrossRef]
- Camfferman, D.; McEvoy, R.D.; O’Donoghue, F.; Lushington, K. Prader Willi Syndrome and excessive daytime sleepiness. Sleep Med. Rev. 2008, 12, 65–75. [Google Scholar] [CrossRef]
- O’Donoghue, F.; Camfferman, D.; Kennedy, J.; Martin, A.; Couper, T.; Lack, L.; Lushington, K.; McEvoy, D. Sleep-Disordered Breathing in Prader-Willi Syndrome and its Association with Neurobehavioral Abnormalities. J. Pediatr. 2005, 147, 823–829. [Google Scholar] [CrossRef]
- Butler, J.V.; Whittington, J.E.; Holland, A.J.; Boer, H.; Clarke, D.; Webb, T. Prevalence of, and risk factors for, physical ill-health in people with Prader-Willi syndrome: A population-based study. Dev. Med. Child Neurol. 2007, 44, 248–255. [Google Scholar] [CrossRef]
- Vernet, C.; Arnulf, I. Idiopathic Hypersomnia with and without Long Sleep Time: A Controlled Series of 75 Patients. Sleep 2009, 32, 753–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, J.B.; Luks, A. West’s Respiratory Physiology: The Essentials; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Arens, R.; Gozal, D.; Burrell, B.C.; Bailey, S.L.; Bautista, D.B.; Keens, T.G.; Ward, S.L. Arousal and cardiorespiratory responses to hypoxia in Prader-Willi syndrome. Am. J. Respir. Crit. Care Med. 1996, 153, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Livingston, F.R.; Arens, R.; Bailey, S.L.; Keens, T.G.; Ward, S.L.D. Hypercapnic Arousal Responses in Prader-Willi Syndrome. Chest 1995, 108, 1627–1631. [Google Scholar] [CrossRef]
- Hákonarson, H.; Moskovitz, J.; Daigle, K.L.; Cassidy, S.B.; Cloutier, M.M. Pulmonary function abnormalities in Prader-Willi syndrome. J. Pediatr. 1995, 126, 565–570. [Google Scholar] [CrossRef]
- McPhail, G.L.; Ehsan, Z.; Howells, S.A.; Boesch, R.P.; Fenchel, M.C.; Szczesniak, R.; Jain, V.; Agabegi, S.; Sturm, P.; Wall, E.; et al. Obstructive Lung Disease in Children with Idiopathic Scoliosis. J. Pediatr. 2015, 166, 1018–1021. [Google Scholar] [CrossRef]
- Hertz, G.; Cataletto, M.; Feinsilver, S.H.; Angulo, M. Developmental trends of sleep-disordered breathing in Prader-Willi syndrome: The role of obesity. Am. J. Med. Genet. 1995, 56, 188–190. [Google Scholar] [CrossRef]
- Yee, B.J.; Buchanan, P.R.; Mahadev, S.; Banerjee, D.; Liu, P.Y.; Phillips, C.; Grunstein, R.R. Assessment of sleep and breathing in adults with prader-willi syndrome: A case control series. J. Clin. Sleep Med. 2007, 3, 713–718. [Google Scholar] [CrossRef] [Green Version]
- Arens, R.; Gozal, D.; Omlin, K.J.; Livingston, F.R.; Liu, J.; Keens, T.G.; Ward, S.L. Hypoxic and hypercapnic ventilatory responses in Prader-Willi syndrome. J. Appl. Physiol. 1994, 77, 2224–2230. [Google Scholar] [CrossRef]
- Tauber, M.; Diene, G.; Molinas, C.; Hébert, M. Review of 64 cases of death in children with Prader–Willi syndrome (PWS). Am. J. Med. Genet. A 2008, 146A, 881–887. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Vandeleur, M.; Davey, M.J.; Nixon, G.M. Are sleep studies helpful in children with Prader-Willi syndrome prior to commencement of growth hormone therapy? J. Paediatr. Child Health 2013, 49, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Coupaye, M.; Lorenzini, F.; Lloret-Linares, C.; Molinas, C.; Pinto, G.; Diene, G.; Mimoun, E.; Demeer, G.; Labrousse, F.; Jauregi, J.; et al. Growth Hormone Therapy for Children and Adolescents with Prader-Willi Syndrome Is Associated with Improved Body Composition and Metabolic Status in Adulthood. J. Clin. Endocrinol. Metab. 2013, 98, E328–E335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupaye, M.; Tauber, M.; Cuisset, L.; Laurier, V.; Bieth, E.; Lacorte, J.-M.; Oppert, J.-M.; Clément, K.; Poitou, C. Effect of Genotype and Previous GH Treatment on Adiposity in Adults with Prader-Willi Syndrome. J. Clin. Endocrinol. Metab. 2016, 101, 4895–4903. [Google Scholar] [CrossRef]
- Donze, S.H.; de Weerd, A.W.; van den Bossche, R.A.; Joosten, K.F.; Hokken-Koelega, A.C. Sleep-related breathing disorders in young adults with Prader-Willi syndrome: A placebo-controlled, cross-over GH trial. J. Clin. Endocrinol. Metab. 2019, 104, 3931–3938. [Google Scholar] [CrossRef]
- Miller, J.; Silverstein, J.; Shuster, J.; Driscoll, D.J.; Wagner, M. Short-term effects of growth hormone on sleep abnormalities in Prader-Willi syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 413–417. [Google Scholar] [CrossRef] [Green Version]
- Pavone, M.; Caldarelli, V.; Khirani, S.; Colella, M.; Ramirez, A.; Aubertin, G.; Crinò, A.; Brioude, F.; Gastaud, F.; Beydon, N.; et al. Sleep disordered breathing in patients with Prader-Willi syndrome: A multicenter study. Pediatr. Pulmonol. 2015, 50, 1354–1359. [Google Scholar] [CrossRef]
- Doshi, A.; Udwadia, Z. Prader-Willi syndrome with sleep disordered breathing: Effect of two years nocturnal CPAP. Indian J. chest Dis. Allied Sci. 2001, 43, 51–53. [Google Scholar]
- Butler, M.G.; Miller, J.L.; Forster, J.L. Prader-Willi Syndrome—Clinical Genetics, Diagnosis and Treatment Approaches: An Update. Curr. Pediatr. Rev. 2019, 15, 207–244. [Google Scholar] [CrossRef]
- Clift, S.; Dahlitz, M.; Parkes, J.D. Sleep apnoea in the Prader-Willi syndrome. J. Sleep Res. 1994, 3, 121–126. [Google Scholar] [CrossRef]
- Sforza, E.; Krieger, J.; Geisert, J.; Kurtz, D. Sleep and Breathing Abnormalities in a Case of Prader-Willi Syndrome: The Effects of Acute Continuous Positive Airway Pressure Treatment. Acta Paediatr. Scand. 1991, 80, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Smith, I.; King, M.; Siklos, P.; Shneerson, J. Treatment of ventilatory failure in the Prader-Willi syndrome. Eur. Respir. J. 1998, 11, 1150–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, K.; Scheimann, A.; Sutton, V.; Hayslett, E.; Glaze, D.G. Sleepiness and Sleep Disordered Breathing in Prader-Willi Syndrome: Relationship to Genotype, Growth Hormone Therapy, and Body Composition. J. Clin. Sleep Med. 2008, 4, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Ganjavi, H.; Shapiro, C.M. Hypocretin/Orexin: A molecular link between sleep, energy regulation, and pleasure. J. Neuropsychiatry Clin. Neurosci. 2007, 19, 413–419. [Google Scholar] [CrossRef]
- Tucci, V. Genomic Imprinting: A New Epigenetic Perspective of Sleep Regulation. PLoS Genet. 2016, 12, e1006004. [Google Scholar] [CrossRef]
- Lassi, G.; Priano, L.; Maggi, S.; Garcia-Garcia, C.; Balzani, E.; El-Assawy, N.; Tucci, V. Deletion of the Snord116/SNORD116 Alters Sleep in Mice and Patients with Prader-Willi Syndrome. Sleep 2016, 39, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Cataldi, M.; Arnaldi, D.; Tucci, V.; De Carli, F.; Patti, G.; Napoli, F.; Pace, M.; Maghnie, M.; Nobili, L. Sleep disorders in Prader-Willi syndrome, evidence from animal models and humans. Sleep Med. Rev. 2021, 57, 101432. [Google Scholar] [CrossRef]
- Nevsimalova, S.; Vaňková, J.; Štěpánová, I.; Seemanova, E.; Mignot, E.; Nishino, S. Hypocretin deficiency in Prader-Willi syndrome. Eur. J. Neurol. 2005, 12, 70–72. [Google Scholar] [CrossRef]
- Fronczek, R.; Lammers, G.J.; Balesar, R.; Unmehopa, U.A.; Swaab, D.F. The Number of Hypothalamic Hypocretin (Orexin) Neurons Is Not Affected in Prader-Willi Syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 5466–5470. [Google Scholar] [CrossRef] [Green Version]
- Vgontzas, A.N.; Bixler, E.O.; Kales, A.; Vela-Bueno, A. Prader-Willi syndrome: Effects of weight loss on sleep-disordered breathing, daytime sleepiness and REM sleep disturbance. Acta Paediatr. 1995, 84, 813–814. [Google Scholar] [CrossRef]
- Priano, L.; Grugni, G.; Miscio, G.; Guastamacchia, G.; Toffolet, L.; Sartorio, A.; Mauro, A. Sleep cycling alternating pattern (CAP) expression is associated with hypersomnia and GH secretory pattern in Prader–Willi syndrome. Sleep Med. 2006, 7, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Helbing-Zwanenburg, B.; Kamphuisen, H.A.C.; Mourtazaev, M.S. The origin of excessive daytime sleepiness in the Prader-Willi syndrome. J. Intellect. Disabil. Res. 1993, 37, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Bixler, E.O.; Kales, A.; Centurione, A.; Rogan, P.K.; Mascari, M.; Vela-Bueno, A. Daytime sleepiness and REM abnormalities in Prader-Willi syndrome: Evidence of generalized hypoarousal. Int. J. Neurosci. 1996, 87, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Manni, R.; Politini, L.; Nobili, L.; Ferrillo, F.; Livieri, C.; Veneselli, E.; Biancheri, R.; Martinetti, M.; Tartara, A. Hypersomnia in the Prader Willi syndrome: Clinical-electrophysiological features and underlying factors. Clin. Neurophysiol. 2001, 112, 800–805. [Google Scholar] [CrossRef]
- Tobias, E.S.; Tolmie, J.L.; Stephenson, J.B.P. Cataplexy in the Prader-Willi syndrome. Arch. Dis. Child. 2002, 87, 170. [Google Scholar] [CrossRef] [Green Version]
- Pullen, L.C.; Picone, M.; Tan, L.; Johnston, C.; Stark, H. Cognitive Improvements in Children with Prader-Willi Syndrome Following Pitolisant Treatment—Patient Reports. J. Pediatr. Pharmacol. Ther. 2019, 24, 166–171. [Google Scholar] [CrossRef]
- Pennington, S.; Stutzman, D.; Sannar, E. Pitolisant in an Adolescent with Prader-Willi Syndrome. J. Pediatr. Pharmacol. Ther. 2021, 26, 405–410. [Google Scholar] [CrossRef]
- Beusterien, K.M.; Rogers, A.E.; Walsleben, J.A.; Emsellem, H.A.; Reblando, J.A.; Wang, L.; Goswami, M.; Steinwald, B. Health-related quality of life effects of modafinil for treatment of narcolepsy. Sleep 1999, 22, 757–765. [Google Scholar] [CrossRef] [Green Version]
- De Cock, V.C.; Diene, G.; Molinas, C.; Masson, V.D.L.; Kieffer, I.; Mimoun, E.; Tauber, M. Efficacy of modafinil on excessive daytime sleepiness in Prader-Willi syndrome. Am. J. Med. Genet. A 2011, 155, 1552–1557. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, {kind=link}
