
Insomnia Symptoms, Sleep Hygiene, Mental Health, and Academic Performance in Spanish University Students: A Cross-Sectional Study

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Aim
2.2. Study Design and Setting
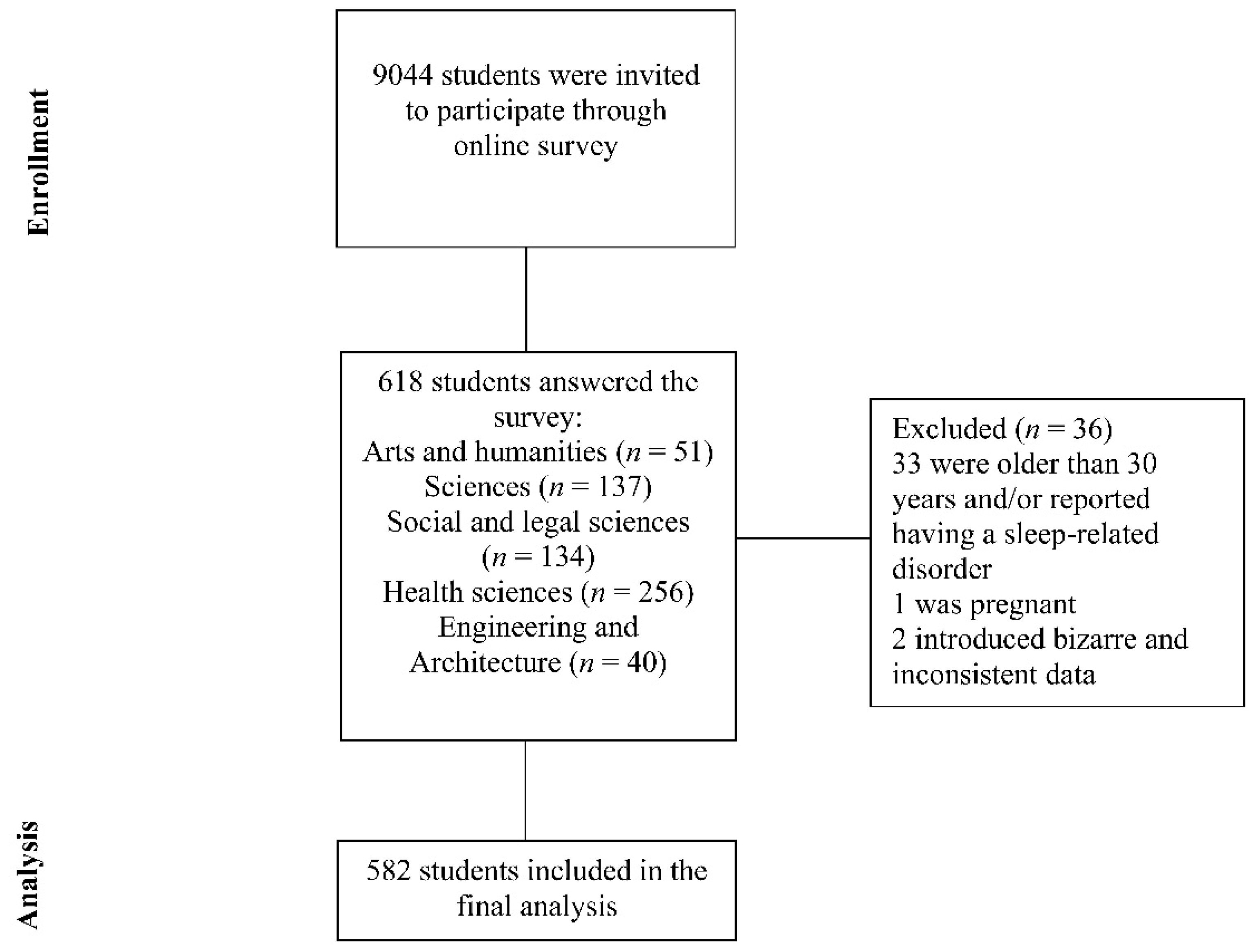
2.3. Participants and Data Collection
2.4. Measurement Instruments
2.4.1. Data on Sociodemographic and Academic Aspects and Life Habits
2.4.2. Insomnia Severity Index (ISI)
2.4.3. Pittsburgh Sleep Quality Index (PSQI)
2.4.4. Stanford Sleepiness Scale (SSS)
2.4.5. Depression, Anxiety, and Stress Scales (DASS-21)
2.4.6. Sleep Hygiene Index (SHI)
2.5. Data Analysis
3. Results
3.1. Description of the Sample
3.2. Insomnia Complaints and Sociodemographic-, Lifestyle-, Academic-, and Psychological-Related Factors
3.3. Predictors of Insomnia Symptoms
3.4. Predictors of Academic Performance
4. Discussion
4.1. High Prevalence of Insomnia Symptoms in University Students
4.2. Relationship between Insomnia Symptoms, Depression, Anxiety, and Stress
4.3. Relationship between Insomnia Symptoms and Sleep Hygiene
4.4. Insomnia Symptoms as a Predictor of Academic Performance
4.5. Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hershner, S.D.; Chervin, R.D. Causes and consequences of sleepiness among college students. Nat. Sci. Sleep 2014, 6, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlarb, A.A.; Claßen, M.; Grünwald, J.; Vögele, C. Sleep disturbances and mental strain in university students: Results from an online survey in Luxembourg and Germany. Int. J. Ment. Health Syst. 2017, 11, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, D.J.; Gardner, C.E.; Bramoweth, A.D.; Williams, J.M.; Roane, B.M.; Grieser, E.A.; Tatum, J.I. Insomnia and mental health in college students. Behav. Sleep. Med. 2011, 9, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Vedaa, Ø.; Erevik, E.K.; Hysing, M.; Hayley, A.C.; Sivertsen, B. Insomnia, sleep duration and academic performance: A national survey of Norwegian college and university students. Sleep Med. X 2019, 1, 100005. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013; ISBN 0890425558. [Google Scholar]
- Beattie, L.; Kyle, S.D.; Espie, C.A.; Biello, S.M. Social Interactions, Emotion and Sleep: A Systematic Review and Research Agenda. Sleep Med. Rev. 2015, 24, 83–100. [Google Scholar] [CrossRef] [Green Version]
- Kyle, S.D.; Espie, C.A.; Morgan, K. “...Not just a minor thing, it is something major, which stops you from functioning daily”: Quality of life and daytime functioning in insomnia. Behav. Sleep. Med. 2010, 8, 123–140. [Google Scholar] [CrossRef]
- Morin, C.M.; Jarrin, D.C. Epidemiology of insomnia: Prevalence, course, risk factors, and public health burden. Sleep Med. Clin. 2013, 8, 281–297. [Google Scholar] [CrossRef] [Green Version]
- Alqudah, M.; Balousha, S.A.M.; Al-Shboul, O.; Al-Dwairi, A.; Alfaqih, M.A.; Alzoubi, K.H. Insomnia among Medical and Paramedical Students in Jordan: Impact on Academic Performance. BioMed Res. Int. 2019, 2019, 7136906. [Google Scholar] [CrossRef] [Green Version]
- Ramón-Arbués, E.; Martínez Abadía, B.; Granada López, J.M.; Echániz Serrano, E.; Pellicer García, B.; Juárez Vela, R.; Guerrero Portillo, S.; Saéz Guinoa, M. Eating behavior and relationships with stress, anxiety, depression and insomnia in university students. Nutr. Hosp. 2019, 36, 1339–1345. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.M.; Craun, E.A.; Bravo, A.J.; Pearson, M.R. Protective Strategies Study Team Insomnia symptoms, cannabis protective behavioral strategies, and hazardous cannabis use among U.S. college students. Exp. Clin. Psychopharmacol. 2019, 27, 309–317. [Google Scholar] [CrossRef]
- Choueiry, N.; Salamoun, T.; Jabbour, H.; El Osta, N.; Hajj, A.; Rabbaa Khabbaz, L. Insomnia and Relationship with Anxiety in University Students: A Cross-Sectional Designed Study. PLoS ONE 2016, 11, e0149643. [Google Scholar] [CrossRef] [Green Version]
- Khader, W.S.; Tubbs, A.S.; Haghighi, A.; Athey, A.B.; Killgore, W.D.S.; Hale, L.; Perlis, M.L.; Gehrels, J.-A.; Alfonso-Miller, P.; Fernandez, F.-X.; et al. Onset insomnia and insufficient sleep duration are associated with suicide ideation in university students and athletes. J. Affect. Disord. 2020, 274, 1161–1164. [Google Scholar] [CrossRef]
- Jiang, X.L.; Zheng, X.Y.; Yang, J.; Ye, C.P.; Chen, Y.Y.; Zhang, Z.G.; Xiao, Z.J. A systematic review of studies on the prevalence of insomnia in university students. Public Health 2015, 129, 1579–1584. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, B.Y.; Bakhshaie, J.; Lam, H.; Alfano, C.; Zvolensky, M.J. Insomnia and eating expectancies among college students: The role of emotion dysregulation. Cogn. Behav. Ther. 2018, 47, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Sing, C.Y.; Wong, W.S. Prevalence of insomnia and its psychosocial correlates among college students in Hong Kong. J. Am. Coll. Health J. ACH 2010, 59, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Allan, S.; Beattie, L.; Bohan, J.; MacMahon, K.; Rasmussen, S. Sleep problem, suicide and self-harm in university students: A systematic review. Sleep Med. Rev. 2019, 44, 58–69. [Google Scholar] [CrossRef] [Green Version]
- Prichard, J.R. Sleep Predicts Collegiate Academic Performance: Implications for Equity in Student Retention and Success. Sleep Med. Clin. 2020, 15, 59–69. [Google Scholar] [CrossRef]
- Gellis, L.A.; Park, A.; Stotsky, M.T.; Taylor, D.J. Associations between sleep hygiene and insomnia severity in college students: Cross-sectional and prospective analyses. Behav. Ther. 2014, 45, 806–816. [Google Scholar] [CrossRef]
- Jansson-Fröjmark, M.; Lindblom, K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J. Psychosom. Res. 2008, 64, 443–449. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014; ISBN 9780991543410. [Google Scholar]
- Friedrich, A.; Schlarb, A.A. Let’s talk about sleep: A systematic review of psychological interventions to improve sleep in college students. J. Sleep Res. 2018, 27, 4–22. [Google Scholar] [CrossRef] [Green Version]
- Lubas, M.M.; Szklo-Coxe, M. A Critical Review of Education-Based Sleep Interventions for Undergraduate Students: Informing Future Directions in Intervention Development. Adolesc. Res. Rev. 2019, 4, 249–266. [Google Scholar] [CrossRef]
- Mastin, D.F.; Bryson, J.; Corwyn, R. Assessment of sleep hygiene using the Sleep Hygiene Index. J. Behav. Med. 2006, 29, 223–227. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Rodriguez-Muñoz, A.; Vela-Bueno, A.; Olavarrieta-Bernardino, S.; Calhoun, S.L.; Bixler, E.O.; Vgontzas, A.N. The Spanish version of the Insomnia Severity Index: A confirmatory factor analysis. Sleep Med. 2012, 13, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Sierra, J.C.; Guillén-Serrano, V.; Santos-Iglesias, P. Insomnia Severity Index: Some indicators about its reliability and validity on an older adults sample. Rev. Neurol. 2008, 47, 566–570. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Royuela, A.; Fernández, J. Propiedades clinimetricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Buela-Casal, G.; Freire, J.C.S. Escala para evaluar la activación-somnolencia. Vigilia Sueño 1994, 6, 13–19. [Google Scholar]
- MacLean, A.W.; Fekken, G.C.; Saskin, P.; Knowles, J.B. Psychometric evaluation of the Stanford Sleepiness Scale. J. Sleep Res. 1992, 1, 35–39. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; Paino, M.; Lemos-Giráldez, S.; Muñiz, J. Psychometric properties of the Depression Anxiety and Stress Scales-21 (dass-21) in Spanish college students. Ansiedad Estres 2010, 16, 215–226. [Google Scholar]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, D.J.; Bramoweth, A.D.; Grieser, E.A.; Tatum, J.I.; Roane, B.M. Epidemiology of insomnia in college students: Relationship with mental health, quality of life, and substance use difficulties. Behav. Ther. 2013, 44, 339–348. [Google Scholar] [CrossRef]
- Aernout, E.; Benradia, I.; Hazo, J.-B.; Sy, A.; Askevis-Leherpeux, F.; Sebbane, D.; Roelandt, J.-L. International study of the prevalence and factors associated with insomnia in the general population. Sleep Med. 2021, 82, 186–192. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S.; Yung, T.K.C.; Aounallah-Skhiri, H.; Rehman, R. Comparison of health risk behavior, awareness, and health benefit beliefs of health science and non-health science students: An international study. Nurs. Health Sci. 2016, 18, 180–187. [Google Scholar] [CrossRef] [Green Version]
- Akram, U.; Akram, A.; Gardani, M.; Ypsilanti, A.; McCarty, K.; Allen, S.; Lazuras, L. The relationship between depression and insomnia symptoms amongst a sample of UK university students. Sleep Med. Res. 2019, 10, 49–53. [Google Scholar] [CrossRef]
- Amaral, A.P.; Soares, M.J.; Pinto, A.M.; Pereira, A.T.; Madeira, N.; Bos, S.C.; Marques, M.; Roque, C.; Macedo, A. Sleep difficulties in college students: The role of stress, affect and cognitive processes. Psychiatry Res. 2018, 260, 331–337. [Google Scholar] [CrossRef]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep patterns and predictors of disturbed sleep in a large population of college students. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2010, 46, 124–132. [Google Scholar] [CrossRef]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Younes, F.; Halawi, G.; Jabbour, H.; El Osta, N.; Karam, L.; Hajj, A.; Rabbaa Khabbaz, L. Internet Addiction and Relationships with Insomnia, Anxiety, Depression, Stress and Self-Esteem in University Students: A Cross-Sectional Designed Study. PLoS ONE 2016, 11, e0161126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairholme, C.P.; Nosen, E.L.; Nillni, Y.I.; Schumacher, J.A.; Tull, M.T.; Coffey, S.F. Sleep disturbance and emotion dysregulation as transdiagnostic processes in a comorbid sample. Behav. Res. Ther. 2013, 51, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltz, J.S.; Rogge, R.D. The indirect effects of sleep hygiene and environmental factors on depressive symptoms in college students. Sleep Health 2016, 2, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Peach, H.; Gaultney, J.F.; Gray, D.D. Sleep hygiene and sleep quality as predictors of positive and negative dimensions of mental health in college students. Cogent Psychol. 2016, 3, 1168768. [Google Scholar] [CrossRef]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: An American Academy of Sleep Medicine clinical practice guideline. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2021, 17, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A.H.; Awaiz, M.; Ghanghro, Z.; Jafferi, M.A.; Aziz, S. Pre-examination stress in second year medical students in a government college. J. Ayub Med. Coll. Abbottabad JAMC 2010, 22, 152–155. [Google Scholar] [PubMed]
- Koudela-Hamila, S.; Smyth, J.; Santangelo, P.; Ebner-Priemer, U. Examination stress in academic students: A multimodal, real-time, real-life investigation of reported stress, social contact, blood pressure, and cortisol. J. Am. Coll. Health J. ACH 2020, 1–12. [Google Scholar] [CrossRef]
- Campbell, R.; Soenens, B.; Beyers, W.; Vansteenkiste, M. University students’ sleep during an exam period: The role of basic psychological needs and stress. Motiv. Emot. 2018, 42, 671–681. [Google Scholar] [CrossRef] [Green Version]
- Zunhammer, M.; Eichhammer, P.; Busch, V. Sleep Quality during Exam Stress: The Role of Alcohol, Caffeine and Nicotine. PLoS ONE 2014, 9, e109490. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Nocturnal sleep problems among university students from 26 countries. Sleep Breath. Schlaf Atm. 2015, 19, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Gellis, L.A.; Park, A. Nighttime thought control strategies and insomnia severity. Cogn. Ther. Res. 2013, 37, 383–389. [Google Scholar] [CrossRef]
- Phillips, A.J.K.; Clerx, W.M.; O’Brien, C.S.; Sano, A.; Barger, L.K.; Picard, R.W.; Lockley, S.W.; Klerman, E.B.; Czeisler, C.A. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 2017, 7, 3216. [Google Scholar] [CrossRef] [PubMed]
- Gaultney, J.F. The prevalence of sleep disorders in college students: Impact on academic performance. J. Am. Coll. Health J. ACH 2010, 59, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortier-Brochu, E.; Beaulieu-Bonneau, S.; Ivers, H.; Morin, C.M. Insomnia and daytime cognitive performance: A meta-analysis. Sleep Med. Rev. 2012, 16, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Wilckens, K.A.; Ferrarelli, F.; Walker, M.P.; Buysse, D.J. Slow-Wave Activity Enhancement to Improve Cognition. Trends Neurosci. 2018, 41, 470–482. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 582) | No Insomnia Symptoms (n = 350) | Insomnia Symptoms (n = 232) | p | |
|---|---|---|---|---|
| Sex (n, %) | 0.640 | |||
| Male | 225 (38.6%) | 138 (39.4%) | 87 (37.5%) | |
| Female | 357 (63.3%) | 212 (60.6%) | 145 (62.5%) | |
| Relationship status (n, %) | 0.779 | |||
| Single | 550 (94.5%) | 330 (94.3%) | 220 (94.8%) | |
| Committed relationship † | 32 (5.5%) | 20 (5.7%) | 12 (5.2%) | |
| Living situation (n, %) | 0.606 | |||
| Parent/guardian | 203 (34.9%) | 129 (36.9%) | 74 (31.9%) | |
| Roommates | 299 (51.4%) | 174 (49.7%) | 125 (53.9%) | |
| Alone | 31 (5.3%) | 17 (4.9%) | 14 (6.0%) | |
| Other | 49 (8.4%) | 30 (8.6%) | 19 (8.2%) | |
| Monthly household income (n, %) | 0.068 | |||
| Less than EUR 1000 | 143 (24.6%) | 76 (21.7%) | 67 (28.9%) | |
| From EUR 1000 to EUR 2000 | 264 (45.3%) | 157 (44.9%) | 107 (46.1%) | |
| From EUR 2000 to EUR 3000 | 120 (20.6%) | 83 (23.7%) | 37 (15.9%) | |
| More than EUR 3000 | 55 (9.4%) | 34 (9.7%) | 21 (9.1%) | |
| Significant alcohol consumption (n, %) | 0.377 | |||
| No significant alcohol consumption | 467 (80.2%) | 285 (81.4%) | 182 (78.4%) | |
| Significant alcohol consumption | 115 (19.7%) | 65 (18.6%) | 50 (21.6%) | |
| Tobacco consumption (n, %) | 87 (14.9%) | 45 (12.9%) | 42 (18.1%) | 0.082 |
| Age (y) | 21 (19–22) | 21 (19–22) | 21 (19–22) | 0.521 |
| Body mass index (kg/m2) | 22.5 (20.4–24.8) | 22.4 (20.4–25.0) | 22.5 (20.4–24.7) | 0.593 |
| Hours exercise/week (h) | 4 (2–6) | 4 (2–6) | 4 (1.5–6) | 0.139 |
| ISI-Insomnia (/28) | 9 (6–13) | 7 (4–8.25) | 14 (12–16) | < 0.001 |
| PSQI total (/21) | 7 (4–9) | 6 (4–7) | 8 (5–10) | < 0.001 |
| PSQI disturbances (/3) | 1 (1–1) | 1 (1–1) | 1 (1–2) | < 0.001 |
| PSQI efficiency (/3) | 1 (0–1) | 0 (0–1) | 1 (0–1) | < 0.001 |
| PSQI latency (/3) | 1 (1–2) | 1 (1–2) | 2 (1–2) | < 0.001 |
| DASS-Depression (/7) | 3 (1–7) | 2 (1–4.25) | 5 (2–10) | < 0.001 |
| DASS-Anxiety (/7) | 3 (1–6) | 2 (1–4) | 5 (2–8) | < 0.001 |
| DASS-Stress (/7) | 6 (2–10) | 4 (1–7) | 9 (5–12) | < 0.001 |
| Sleep Hygiene Index (/52) | 17 (13–22) | 15 (11–19.25) | 20 (16–25) | < 0.001 |
| Stanford Sleepiness Scale (/24) | 10 (8–12) | 9 (7–11) | 11 (9–13) | < 0.001 |
| Total (n = 582) | No Insomnia Symptoms (n = 350) | Insomnia Symptoms (n = 232) | p | |
|---|---|---|---|---|
| Exam period (n, %) | 0.046 | |||
| Non-exam | 308 (52.9%) | 197 (54.3%) | 111 (47.8%) | |
| Exam | 274 (47.1%) | 153 (43.7%) | 121 (52.2%) | |
| University year (n, %) | 0.746 | |||
| Freshmen students | 153 (26.3%) | 86 (24.6%) | 67 (43,8%) | |
| Sophomore students | 144 (24.7%) | 90 (25.7%) | 54 (37,5%) | |
| Junior students | 125 (21.5%) | 72 (20.6%) | 53 (42,4%) | |
| Senior students | 135 (23.2%) | 87 (24.9%) | 48 (35,6%) | |
| Fifth-/Sixth-year students | 20 (3.4%) | 12 (3.4%) | 8 (3.4%) | |
| Master’s/Other students | 5 (0.9%) | 3 (0.9%) | 2 (0.9%) | |
| Health Sciences (n, %) | 0.002 | |||
| Non-health-related degree | 337 (57.9%) | 185 (52.9%) | 152 (65.5%) | |
| Health-related degree | 245 (42.1%) | 165 (47.1%) | 80 (34.5%) | |
| GPA | 7.2 (6.6–8.0) | 7.5 (6.7–8.0) | 7.0 (6.4–7.9) | < 0.001 |
| Crude OR | CI 95% | p | Adjusted OR 1 † | CI 95% | p | Adjusted OR 2 ‡ | CI 95% | p | |
|---|---|---|---|---|---|---|---|---|---|
| DASS_Depression | 1.16 | 1.12–1.21 | < 0.001 | 1.16 | 1.11–1.22 | < 0.001 | 1.02 | 0.96–1.09 | 0.470 |
| DASS_Anxiety | 1.10 | 1.02–1.18 | 0.010 | 1.24 | 1.18–1.32 | < 0.001 | 1.07 | 0.99–1.12 | 0.092 |
| DASS_Stress | 1.10 | 1.04–1.17 | < 0.001 | 1.20 | 1.15–1.25 | < 0.001 | 1.10 | 1.03–1.18 | 0.003 |
| SHI_total | 1.08 | 1.05–1.12 | < 0.001 | 1.12 | 1.09–1.16 | < 0.001 | 1.08 | 1.04–1.12 | < 0.001 |
| Crude | Model 1 † | Model 2 ‡ | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Crude r2 | Crude t | p | Adjusted r2 | Adjusted t | p | Adjusted r2 | Adjusted t | p | |
| PSQI total | <0.10 | −2.10 | 0.046 | 0.15 | −1.18 | 0.238 | |||
| PSQI disturbances | <0.10 | −2.27 | 0.024 | 0.15 | −1.58 | 0.114 | |||
| PSQI efficiency | <0.10 | −3.12 | 0.002 | 0.16 | −2.26 | 0.023 | 0.16 | −1.71 | 0.087 |
| PSQI latency | <0.10 | −2.08 | 0.038 | 0.15 | −1.21 | 0.228 | |||
| SHI_total | <0.10 | −3.90 | < 0.001 | 0.15 | −1.59 | 0.113 | |||
| ISI | <0.10 | −3.27 | 0.001 | 0.16 | −2.24 | 0.026 | 0.16 | −1.09 | 0.275 |
| DASS_depression | <0.10 | −4.02 | < 0.001 | 0.16 | −2.26 | 0.024 | 0.16 | −1.42 | 0.154 |
| DASS_Anxiety | <0.10 | −2.31 | 0.020 | 0.15 | −0.81 | 0.416 | |||
| DASS_Stress | <0.10 | −1.98 | 0.048 | 0.15 | −0.55 | 0.580 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrión-Pantoja, S.; Prados, G.; Chouchou, F.; Holguín, M.; Mendoza-Vinces, Á.; Expósito-Ruiz, M.; Fernández-Puerta, L. Insomnia Symptoms, Sleep Hygiene, Mental Health, and Academic Performance in Spanish University Students: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 1989. https://doi.org/10.3390/jcm11071989
Carrión-Pantoja S, Prados G, Chouchou F, Holguín M, Mendoza-Vinces Á, Expósito-Ruiz M, Fernández-Puerta L. Insomnia Symptoms, Sleep Hygiene, Mental Health, and Academic Performance in Spanish University Students: A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(7):1989. https://doi.org/10.3390/jcm11071989
Chicago/Turabian StyleCarrión-Pantoja, Sara, Germán Prados, Florian Chouchou, Martha Holguín, Ángela Mendoza-Vinces, Manuela Expósito-Ruiz, and Laura Fernández-Puerta. 2022. "Insomnia Symptoms, Sleep Hygiene, Mental Health, and Academic Performance in Spanish University Students: A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 7: 1989. https://doi.org/10.3390/jcm11071989
APA StyleCarrión-Pantoja, S., Prados, G., Chouchou, F., Holguín, M., Mendoza-Vinces, Á., Expósito-Ruiz, M., & Fernández-Puerta, L. (2022). Insomnia Symptoms, Sleep Hygiene, Mental Health, and Academic Performance in Spanish University Students: A Cross-Sectional Study. Journal of Clinical Medicine, 11(7), 1989. https://doi.org/10.3390/jcm11071989