
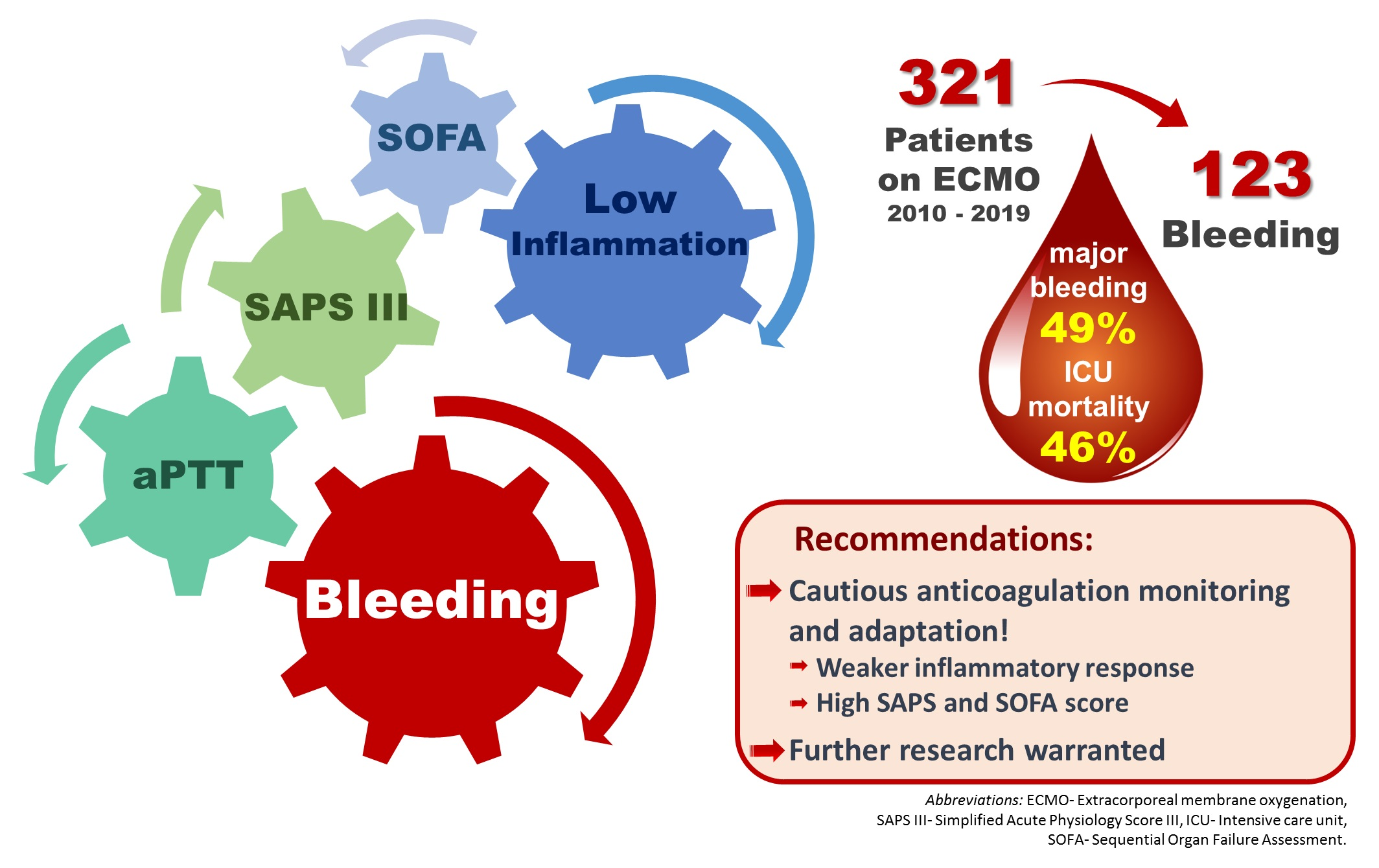
The Role of Excessive Anticoagulation and Missing Hyperinflammation in ECMO-Associated Bleeding

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Anticoagulation Protocol
2.4. Objectives and Outcomes
2.5. Statistical Analyses
3. Results
3.1. Adverse Events during ECMO Support
3.2. Factors Associated with Bleeding Events
3.3. Subgroup Analyses
4. Discussion
4.1. Factors Associated with Haemorrhage
4.2. Further Directions
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biancari, F.; Mariscalco, G.; Dalén, M.; Settembre, N.; Welp, H.; Perrotti, A.; Wiebe, K.; Leo, E.; Loforte, A.; Chocron, S.; et al. Six-Month Survival After Extracorporeal Membrane Oxygenation for Severe COVID-19. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Lawler, P.R.; Silver, D.A.; Scirica, B.M.; Couper, G.S.; Weinhouse, G.L.; Camp, P.C., Jr. Extracorporeal membrane oxygenation in adults with cardiogenic shock. Circulation 2015, 131, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munshi, L.; Walkey, A.; Goligher, E.; Pham, T.; Uleryk, E.M.; Fan, E. Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: A systematic review and meta-analysis. Lancet Respir. Med. 2019, 7, 163–172. [Google Scholar] [CrossRef]
- Inoue, A.; Hifumi, T.; Sakamoto, T.; Kuroda, Y. Extracorporeal Cardiopulmonary Resuscitation for Out-of-Hospital Cardiac Arrest in Adult Patients. J. Am. Heart Assoc. 2020, 9, e015291. [Google Scholar] [CrossRef]
- Bougouin, W.; Dumas, F.; Lamhaut, L.; Marijon, E.; Carli, P.; Combes, A.; Pirracchio, R.; Aissaoui, N.; Karam, N.; Deye, N.; et al. Extracorporeal cardiopulmonary resuscitation in out-of-hospital cardiac arrest: A registry study. Eur. Heart J. 2020, 41, 1961–1971. [Google Scholar] [CrossRef]
- Extracorporeal Life Support Organization (ELSO). Guidelines for Cardiopulmonary Extracorporeal Life Support. Available online: https://www.elso.org/Portals/0/ELSO%20Guidelines%20For%20Adult%20Respiratory%20Failure%201_4.pdf (accessed on 31 October 2021).
- Extracorporeal Life Support Organization (ELSO). Registry Report on Extracorporeal Life Support, International Summary. Available online: https://www.elso.org/Registry/Statistics/InternationalSummary.aspx (accessed on 31 October 2021).
- Stokes, J.W.; Gannon, W.D.; Sherrill, W.H.; Armistead, L.B.; Bacchetta, M.; Rice, T.W.; Semler, M.W.; Casey, J.D. Bleeding, Thromboembolism, and Clinical Outcomes in Venovenous Extracorporeal Membrane Oxygenation. Crit. Care Explor. 2020, 2, e0267. [Google Scholar] [CrossRef]
- Winkler, A.M. Managing the Precarious Hemostatic Balance during Extracorporeal Life Support: Implications for Coagulation Laboratories. Semin. Thromb. Hemost. 2017, 43, 291–299. [Google Scholar] [CrossRef]
- Gray, B.W.; Haft, J.W.; Hirsch, J.C.; Annich, G.M.; Hirschl, R.B.; Bartlett, R.H. Extracorporeal life support: Experience with 2,000 patients. ASAIO J. 2015, 61, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Capodanno, D.; Angiolillo, D.J. Management of Antiplatelet Therapy in Patients with Coronary Artery Disease Requiring Cardiac and Noncardiac Surgery. Circulation 2013, 128, 2785–2798. [Google Scholar] [CrossRef]
- Schlimp, C.B.Z.; Schöchl, H.; Alber, H. Empfehlung der Arbeitsgruppe Perioperative Gerinnung der ÖGARI zum Thema: Perioperatives Management von PatientInnen mit Koronarstents unter Dualer Plättchenhemmung bei Nicht-Kardiochirurgischen Eingriffen; Extracorporeal Life Support Organization (ELSO): Ann Arbor, MI, USA, 2018. [Google Scholar]
- Lequier, L.A.G.; Al-Ibrahim, O.; Bembea, M.; Brodie, D.; Brogan, T.; Buckvold, S.; Chicoine, L.; Conrad, S.; Cooper, D.; Dalton, H.; et al. ELSO Anticoagulation Guideline; Extracorporeal Life Support Organization (ELSO): Ann Arbor, MI, USA, 2014. [Google Scholar]
- Zangrillo, A.; Landoni, G.; Biondi-Zoccai, G.; Greco, M.; Greco, T.; Frati, G.; Patroniti, N.; Antonelli, M.; Pesenti, A.; Pappalardo, F. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit. Care Resusc. 2013, 15, 172–178. [Google Scholar]
- Oude Lansink-Hartgring, A.; de Vries, A.J.; Droogh, J.M.; van den Bergh, W.M. Hemorrhagic complications during extracorporeal membrane oxygenation—The role of anticoagulation and platelets. J. Crit. Care 2019, 54, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Aubron, C.; DePuydt, J.; Belon, F.; Bailey, M.; Schmidt, M.; Sheldrake, J.; Murphy, D.; Scheinkestel, C.; Cooper, D.J.; Capellier, G.; et al. Predictive factors of bleeding events in adults undergoing extracorporeal membrane oxygenation. Ann. Intensive Care 2016, 6, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; McMullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L. Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017, 63, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Arachchillage, D.J.; Rajakaruna, I.; Scott, I.; Gaspar, M.; Odho, Z.; Banya, W.; Vlachou, A.; Isgro, G.; Cagova, L.; Wade, J.; et al. Impact of major bleeding and thrombosis on 180-day survival in patients with severe COVID-19 supported with veno-venous extracorporeal membrane oxygenation in the United Kingdom: A multicentre observational study. Br. J. Haematol. 2021, 196, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Vakil, D.; Soto, C.; D’Costa, Z.; Volk, L.; Kandasamy, S.; Iyer, D.; Ikegami, H.; Russo, M.J.; Lee, L.Y.; Lemaire, A. Short-term and intermediate outcomes of cardiogenic shock and cardiac arrest patients supported by venoarterial extracorporeal membrane oxygenation. J. Cardiothorac. Surg. 2021, 16, 290. [Google Scholar] [CrossRef]
- Lotz, C.; Streiber, N.; Roewer, N.; Lepper, P.M.; Muellenbach, R.M.; Kredel, M. Therapeutic Interventions and Risk Factors of Bleeding During Extracorporeal Membrane Oxygenation. ASAIO J. 2017, 63, 624–630. [Google Scholar] [CrossRef]
- Halaweish, I.; Cole, A.; Cooley, E.; Lynch, W.R.; Haft, J.W. Roller and Centrifugal Pumps: A Retrospective Comparison of Bleeding Complications in Extracorporeal Membrane Oxygenation. ASAIO J. 2015, 61, 496–501. [Google Scholar] [CrossRef]
- Werho, D.K.; Pasquali, S.K.; Yu, S.; Donohue, J.; Annich, G.M.; Thiagarajan, R.R.; Hirsch-Romano, J.C.; Gaies, M.G. Hemorrhagic complications in pediatric cardiac patients on extracorporeal membrane oxygenation: An analysis of the Extracorporeal Life Support Organization Registry. Pediatric Crit. Care Med. 2015, 16, 276–288. [Google Scholar] [CrossRef] [Green Version]
- Tauber, H.; Ott, H.; Streif, W.; Weigel, G.; Loacker, L.; Fritz, J.; Heinz, A.; Velik-Salchner, C. Extracorporeal membrane oxygenation induces short-term loss of high-molecular-weight von Willebrand factor multimers. Anesth. Analg. 2015, 120, 730–736. [Google Scholar] [CrossRef]
- Kalbhenn, J.; Schmidt, R.; Nakamura, L.; Schelling, J.; Rosenfelder, S.; Zieger, B. Early diagnosis of acquired von Willebrand Syndrome (AVWS) is elementary for clinical practice in patients treated with ECMO therapy. J. Atheroscler. Thromb. 2015, 22, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Doyle, A.J.; Hunt, B.J. Current Understanding of How Extracorporeal Membrane Oxygenators Activate Haemostasis and Other Blood Components. Front. Med. 2018, 5, 352. [Google Scholar] [CrossRef] [PubMed]
- Bachler, M.; Niederwanger, C.; Hell, T.; Höfer, J.; Gerstmeyr, D.; Schenk, B.; Treml, B.; Fries, D. Influence of factor XII deficiency on activated partial thromboplastin time (aPTT) in critically ill patients. J. Thromb. Thrombolysis 2019, 48, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajsic, S.; Breitkopf, R.; Bachler, M.; Treml, B. Diagnostic Modalities in Critical Care: Point-of-Care Approach. Diagnostics 2021, 11, 2202. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Ballotta, A.; Di Dedda, U.; Baryshnikova, E.; Dei Poli, M.; Resta, M.; Falco, M.; Albano, G.; Menicanti, L. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. J. Thromb. Haemost. 2020, 18, 1747–1751. [Google Scholar] [CrossRef]
- Lim, M.S.; McRae, S. COVID-19 and immunothrombosis: Pathophysiology and therapeutic implications. Crit. Rev. Oncol. Hematol. 2021, 168, 103529. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef]
- Delabranche, X.; Helms, J.; Meziani, F. Immunohaemostasis: A new view on haemostasis during sepsis. Ann. Intensive Care 2017, 7, 117. [Google Scholar] [CrossRef] [Green Version]
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef] [Green Version]
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 18, 666–682. [Google Scholar] [CrossRef]
- Gro, G.; Trond, I.; Ynse Ieuwe Gerardus Vladimir, T.; Jan, B.; Sigrid Kufaas, B.; John-Bjarne, H. C-reactive protein and risk of venous thromboembolism: Results from a population-based case-crossover study. Haematologica 2018, 103, 1245–1250. [Google Scholar] [CrossRef]
- Asoğlu, R.; Tibilli, H.; Afşin, A.; Türkmen, S.; Barman, H.A.; Asoğlu, E. Procalcitonin is a predictor of disseminated intravascular coagulation in patients with fatal COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11953–11959. [Google Scholar] [CrossRef]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.L.; Esmon, C.T.; Esmon, N.L. Tumor necrosis factor leads to the internalization and degradation of thrombomodulin from the surface of bovine aortic endothelial cells in culture. Blood 1989, 73, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, E.M. Thrombomodulin and its role in inflammation. Semin. Immunopathol. 2012, 34, 107–125. [Google Scholar] [CrossRef]
- Lindmark, E.; Tenno, T.; Siegbahn, A. Role of platelet P-selectin and CD40 ligand in the induction of monocytic tissue factor expression. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 2322–2328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Wouwer, M.; Collen, D.; Conway, E.M. Thrombomodulin-protein C-EPCR system: Integrated to regulate coagulation and inflammation. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1374–1383. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H. Inflammation and thrombosis: Roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis. J. Thromb. Haemost. 2018, 16, 231–241. [Google Scholar] [CrossRef]
- Bernardo, A.; Ball, C.; Nolasco, L.; Moake, J.F.; Dong, J.F. Effects of inflammatory cytokines on the release and cleavage of the endothelial cell-derived ultralarge von Willebrand factor multimers under flow. Blood 2004, 104, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Han, K.H.; Hong, K.H.; Park, J.H.; Ko, J.; Kang, D.H.; Choi, K.J.; Hong, M.K.; Park, S.W.; Park, S.J. C-reactive protein promotes monocyte chemoattractant protein-1--mediated chemotaxis through upregulating CC chemokine receptor 2 expression in human monocytes. Circulation 2004, 109, 2566–2571. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, S.; Xu, D.Y.; Jialal, I. C-reactive protein increases plasminogen activator inhibitor-1 expression and activity in human aortic endothelial cells: Implications for the metabolic syndrome and atherothrombosis. Circulation 2003, 107, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolbink, G.J.; Bossink, A.W.; Groeneveld, A.B.; de Groot, M.C.; Thijs, L.G.; Hack, C.E. Complement activation in patients with sepsis is in part mediated by C-reactive protein. J. Infect. Dis. 1998, 177, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esmon, C.T. The interactions between inflammation and coagulation. Br. J. Haematol. 2005, 131, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.H.; Connors, J.M. Heparin Resistance—Clinical Perspectives and Management Strategies. New Engl. J. Med. 2021, 385, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Mulloy, B.; Hogwood, J.; Gray, E.; Lever, R.; Page, C.P. Pharmacology of Heparin and Related Drugs. Pharmacol. Rev. 2016, 68, 76–141. [Google Scholar] [CrossRef]
- Malhotra Kapoor, P.; Karanjkar, A.; Bhardwaj, V. Evaluation of coagulopathy on veno-arterial ECMO (VA) extracorporeal membrane oxygenation using platelet aggregometry and standard tests: A narrative review. Egypt. J. Crit. Care Med. 2018, 6, 73–78. [Google Scholar] [CrossRef]
- McVeen, R.V.; Lorch, V.; Carroll, R.C.; Goldberg, L.; Keszler, M.; Podlasek, S.; Stewart, D.L. Changes in fibrinolytic factors in newborns during extracorporeal membrane oxygenation (ECMO). Am. J. Hematol. 1991, 38, 254–255. [Google Scholar] [CrossRef]
- Ghiselli, G. Heparin Binding Proteins as Therapeutic Target: An Historical Account and Current Trends. Medicine 2019, 6, 80. [Google Scholar] [CrossRef] [Green Version]
- Boneu, B.; Caranobe, C.; Sie, P. Pharmacokinetics of heparin and low molecular weight heparin. Bailliere’s Clin. Haematol. 1990, 3, 531–544. [Google Scholar] [CrossRef]
- Wiggins, R.C.; Bouma, B.N.; Cochrane, C.G.; Griffin, J.H. Role of high-molecular-weight kininogen in surface-binding and activation of coagulation Factor XI and prekallikrein. Proc. Natl. Acad. Sci. USA 1977, 74, 4636–4640. [Google Scholar] [CrossRef] [Green Version]
- DeLoughery, E.P.; Olson, S.R.; Puy, C.; McCarty, O.J.T.; Shatzel, J.J. The Safety and Efficacy of Novel Agents Targeting Factors XI and XII in Early Phase Human Trials. Semin. Thromb. Hemost. 2019, 45, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Wallisch, M.; Lorentz, C.U.; Lakshmanan, H.H.S.; Johnson, J.; Carris, M.R.; Puy, C.; Gailani, D.; Hinds, M.T.; McCarty, O.J.T.; Gruber, A.; et al. Antibody inhibition of contact factor XII reduces platelet deposition in a model of extracorporeal membrane oxygenator perfusion in nonhuman primates. Res. Pract. Thromb. Haemost. 2020, 4, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrovolskaia, M.A.; McNeil, S.E. Safe anticoagulation when heart and lungs are “on vacation”. Ann. Transl. Med. 2015, 3 (Suppl. S1), S11. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | All Patients (n = 321) | No Bleeding Event (n = 198) | Bleeding Event (n = 123) | p-Value | Missing Data (n/Total) | |
|---|---|---|---|---|---|---|
| Age (years) | 57.5 ± 16.1 | 57.9 ± 16.1 | 56.7 ± 16.1 | 0.515 | 0/321 | |
| <30 | 25 (7.8) | 16 (8.1) | 9 (7.3) | 0.256 | 0/321 | |
| 31–45 | 39 (12.1) | 22 (11.1) | 17 (13.8) | |||
| 46–60 | 99 (30.8) | 59 (29.8) | 40 (32.5) | |||
| 61–75 | 124 (38.6) | 75 (37.9) | 49 (39.8) | |||
| >76 | 34 (10.6) | 26 (13.1) | 8 (6.5) | |||
| Male sex | 229 (71.3) | 141 (71.2) | 88 (71.5) | 0.949 | 0/321 | |
| Height (cm) | 173 ± 10.0 | 173 ± 8.7 | 171 ± 11.8 | 0.295 | 10/321 | |
| Weight (kg) | 81.6 ± 17.9 | 82.0 ± 17.4 | 80.8 ± 18.7 | 0.566 | 10/321 | |
| Body mass index (kg/m2) | 27.3 ± 5.3 | 27.3 ± 5.3 | 27.2 ± 5.3 | 0.845 | 10/321 | |
| SAPS III score (points) | 67 (28–117) | 65 (28–112) | 69 (28–117) | 0.023 | 1/321 | |
| SAPS III-score-predicted mortality (%) | 50 (1–96) | 46 (1–95) | 54 (1–96) | 0.023 | 1/321 | |
| SOFA score (points) | 12 (2–21) | 12 (2–21) | 13 (4–21) | 0.005 | 0/321 | |
| SOFA respiratory | 2 (0–4) | 2 (0–4) | 3 (0–4) | 0.016 | ||
| SOFA coagulation | 1 (0–4) | 1 (0–4) | 1 (0–3) | 0.270 | ||
| SOFA liver | 0 (0–4) | 0 (0–4) | 1 (0–4) | 0.045 | ||
| SOFA cardiovascular | 4 (0–4) | 4 (0–4) | 4 (0–4) | 0.076 | ||
| SOFA neurology | 4 (0–4) | 4 (0–4) | 4 (0–4) | 0.092 | ||
| SOFA renal | 1 (0–4) | 1 (0–4) | 1 (0–4) | 0.070 | ||
| CPR before ECMO initiation | 61 (19.0) | 35 (17.7) | 26 (21.1) | 0.442 | 0/321 | |
| Length of ICU stay (days) | 18 (1–170) | 18 (2–170) | 17 (1–98) | 0.576 | 0/321 | |
| ICU admission reason | 0/321 | |||||
| Respiratory failure | 79 (24.6) | 49 (24.7) | 30 (24.4) | 0.999 | ||
| Cardiac nonsurgical | 166 (51.7) | 102 (51.5) | 64 (52.0) | |||
| Cardiac surgery | 61 (19.0) | 37 (18.7) | 24(19.5) | |||
| Trauma | 3 (0.9) | 2 (1.0) | 1 (0.8) | |||
| Hypothermi | 12 (4.0) | 8 (4.0) | 4 (3.3) | |||
| ICU department | 0/321 | |||||
| ICU 1 | 178 (55.5) | 112 (56.6) | 66 (53.7) | 0.610 | ||
| ICU 2 | 143 (44.5) | 86 (43.4) | 57 (46.3) | |||
| Mortality-related outcomes | 0/321 | |||||
| Time from admission to death within 90 days (days) | 10 (1–88) | 9.5 (2–79) | 11.5 (1–88) | 0.457 | ||
| ICU mortality | 115 (35.8) | 58 (29.3) | 57 (46.3) | 0.002 | ||
| Clinical Characteristics | All Patients (n = 321) | No Bleeding Event (n = 198) | Bleeding Event (n = 123) | p-Value | Missing Data (n/Total) | |
|---|---|---|---|---|---|---|
| ECMO indications | 0/321 | |||||
| Cardiogenic shock | 223 (69.5) | 136 (68.7) | 87 (70.7) | 0.928 | ||
| Respiratory failure | 87 (27.1) | 55 (27.8) | 32 (26.0) | |||
| Hypothermia | 11 (3.4) | 7 (3.5) | 4 (3.3) | |||
| Type of ECMO support | 0/321 | |||||
| Venoarterial | 247 (76.9) | 154 (77.8) | 93 (75.6) | 0.654 | ||
| Venovenous | 74 (23.1) | 44 (22.2) | 30 (24.4) | |||
| ECMO related clinical course | 0/321 | |||||
| ECMO support duration (days) | 6 (1–36), mean 7.3 | 6 (1–30), mean 6.8 | 7 (1–36), mean 8.2 | 0.053 | ||
| ECMO support duration < 7 days | 209 (65.1) | 141 (71.2) | 68 (55.3) | 0.004 | ||
| Time from admission to ECMO initiation (days) | 0 (0–36) | 0 (0–17) | 0 (0–36) | 0.773 | ||
| Day of ECMO initiation | 0/321 | |||||
| Weekday | 255 (79.4) | 153 (77.3) | 102 (82.9) | 0.223 | ||
| Weekend | 66 (20.6) | 45 (22.7) | 21 (17.1) | |||
| Anticoagulation during ECMO support | 1/321 | |||||
| None | 29 (9.1) | 15 (7.6) | 14 (11.4) | 0.465 | ||
| UFH | 256 (80.0) | 162 (82.2) | 94 (76.4) | |||
| Argatroban | 30 (9.4) | 17 (8.6) | 13(10.6) | |||
| Epoprostenol | 1 (0.3) | 0 (0) | 1 (0.8) | |||
| Argatroban and epoprostenol | 4 (1.3) | 3 (1.5) | 1 (0.8) | |||
| Complications | ||||||
| Major haemorrhage | 60 (18.7) | - | 60 (48.8) | 0/123 | ||
| Minor haemorrhage | 62 (19.3) | - | 62 (50.4) | 0/123 | ||
| Day of haemorrhage | - | - | 2 (1–14), mean 3.2 | 0/123 | ||
| Haemorrhage at first ECMO day | 52 (16.2) | - | 52 (42.3) | 0/123 | ||
| Haemorrhage within first three ECMO support days | 117 (36.4) | - | 117 (95.1) | 0/123 | ||
| Coagulopathy | 41 (12.8) | 19 (9.6) | 22 (17.9) | 0.031 | 27/321 | |
| Thrombosis | 74 (23.1) | 47 (23.7) | 27 (22.0) | 0.712 | 0/321 | |
| Sepsis | 67 (20.9) | 36 (18.2) | 31 (25.2) | 0.132 | 0/321 | |
| Reason for termination of ECMO support | 0/321 | |||||
| Improvement (weaned) | 230 (71.7) | 148 (74.7) | 82 (66.7) | 0.002 | ||
| Bridge to other assistance (heart transplant or ventricular assist device) | 17 (5.3) | 13 (6.6) | 4 (3.3) | |||
| Haemorrhage | 7 (2.2) | - | 7 (5.7) | |||
| Death | 67 (20.9) | 37 (18.7) | 30 (24.4) | |||
| All Patients (n = 321) | No Bleeding Event (n = 198) | Bleeding Event (n = 123) | p-Value | Missing Data (n/Total) | |
|---|---|---|---|---|---|
| Haemoglobin (g/dL) | 92.6 ± 13.3 | 91.0 ± 7.7 | 94.4 ± 17.7 | 0.054 | 13/321 |
| Red blood cells (T/L) | 3.2 ± 0.5 | 3.2 ± 0.4 | 3.2 ± 0.6 | 0.952 | 13/321 |
| Haematocrit (%) | 0.3 ± 0.1 | 0.3 ± 0.1 | 0.3 ± 0.1 | 0.947 | 13/321 |
| Leucocytes (g/L) | 10.2 (1.3–71.7) | 10.2 (1.5–71.7) | 10.3 (1.3–29.6) | 0.899 | 13/321 |
| C-reactive protein (mg/L) | 7.0 (0.1–35.5) | 7.7 (0.1–35.5) | 5.5 (0.1–35.1) | 0.002 | 15/321 |
| Procalcitonin (µg/L) | 5.0 (0.1–1272.4) | 7.0 (0.1–1272.4) | 3.4 (0.1–118.9) | <0.001 | 30/321 |
| Platelets (g/L) | 87.0 (14–309) | 89.0 (18–309) | 84.5 (14–276) | 0.373 | 13/321 |
| International normalised ratio | 1.5 (0.8–6) | 1.5 (1.0–6) | 1.4 (0.8–6.0) | 0.422 | 11/321 |
| Activated partial thromboplastin time (s) | 58.0 (28–201) | 56.5 (28–201) | 58.0 (32–201) | 0.255 | 21/321 |
| Prothrombin time (%) | 51.0 (9–104) | 49.0 (9–104) | 54.0 (9–101) | 0.625 | 10/321 |
| Fibrinogen (mg/dL) | 256.5 (39–1053) | 258.0 (44–1053) | 251.0 (39–941) | 0.226 | 15/321 |
| Antithrombin (%) | 45.0 (19–118) | 43.0 (19–92) | 51.0 (19–118) | 0.018 | 14/321 |
| Factor XIII (%) | 59.0 (13–131) | 59.0 (13–131) | 60.0 (29–129) | 0.500 | 188/321 |
| InTEM clotting time (s) | 211 (54–671) | 204.5 (151–413) | 214 (54–671) | 0.350 | 191/321 |
| InTEM maximal clot firmness (mm) | 49 (5–71) | 48 (25–71) | 51 (5–68) | 0.982 | 216/321 |
| FibTEM maximal clot firmness (mm) | 14 (2–31) | 13.5 (3–31) | 14 (2–30) | 0.432 | 217/321 |
| Substitution of blood products during ECMO support | |||||
| Packed red blood cells (units) | 5 (0–60) | 4 (0–36) | 8 (0–60) | <0.001 | 15/321 |
| Fresh-frozen plasma (units) | 0 (0–92), mean 2.7 | 0 (0–27), mean 1.8 | 0 (0–92), mean 4.3 | 0.011 | 15/321 |
| Platelets (units) | 1 (0–30), mean 2.0 | 0 (0–15), mean 1.3 | 1 (0–30), mean 3.2 | <0.001 | 15/321 |
| Fibrinogen (g) | 0 (0–26), mean 2.8 | 0 (0–22), mean 1.8 | 1 (0–26), mean 4.4 | <0.001 | 15/321 |
| Antithrombin (IU) | 0 (0–32,000), mean 614.5 | 0 (0–16,500), mean 505.7 | 0 (0–32,000), mean 790.5 | 0.164 | 15/321 |
| Prothrombin complex concentrate (IU) | 0 (0–7200), mean 386.0 | 0 (0–6000), mean 285.4 | 0 (0–7200), mean 548.0 | 0.020 | 15/321 |
| Factor XIII concentrate (IU) | 0 (0–10,000), mean 570.0 | 0 (0–6250), mean 246.2 | 0 (0–10,000), mean 1096.3 | <0.001 | 15/321 |
| Desmopressin (µg) | 0 (0–30), mean 0.6 | 0 (0–30), mean 0.3 | 0 (0–30), mean 1.1 | 0.070 | 18/321 |
| Von Willebrand factor (IU) | 0 (0–5000), mean 100.3 | 0 (0–2000), mean 10.1 | 0 (0–5000), mean 245.5 | <0.001 | 27/321 |
| Variable | B-Coefficient | p-Value | HR | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| SAPS III score | 0.012 | 0.047 | 1.01 | 1.00 | 1.03 |
| C-reactive protein (mg/L) | −0.046 | 0.005 | 0.96 | 0.93 | 1.00 |
| aPTT (s) | 0.006 | 0.007 | 1.01 | 1.00 | 1.01 |
| Fibrinogen (mg/dL) | 0.001 | 0.176 | 1.00 | 1.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajsic, S.; Breitkopf, R.; Oezpeker, U.C.; Bukumirić, Z.; Dobesberger, M.; Treml, B. The Role of Excessive Anticoagulation and Missing Hyperinflammation in ECMO-Associated Bleeding. J. Clin. Med. 2022, 11, 2314. https://doi.org/10.3390/jcm11092314
Rajsic S, Breitkopf R, Oezpeker UC, Bukumirić Z, Dobesberger M, Treml B. The Role of Excessive Anticoagulation and Missing Hyperinflammation in ECMO-Associated Bleeding. Journal of Clinical Medicine. 2022; 11(9):2314. https://doi.org/10.3390/jcm11092314
Chicago/Turabian StyleRajsic, Sasa, Robert Breitkopf, Ulvi Cenk Oezpeker, Zoran Bukumirić, Moritz Dobesberger, and Benedikt Treml. 2022. "The Role of Excessive Anticoagulation and Missing Hyperinflammation in ECMO-Associated Bleeding" Journal of Clinical Medicine 11, no. 9: 2314. https://doi.org/10.3390/jcm11092314
APA StyleRajsic, S., Breitkopf, R., Oezpeker, U. C., Bukumirić, Z., Dobesberger, M., & Treml, B. (2022). The Role of Excessive Anticoagulation and Missing Hyperinflammation in ECMO-Associated Bleeding. Journal of Clinical Medicine, 11(9), 2314. https://doi.org/10.3390/jcm11092314