
Real-Time Monitoring of Blood Parameters in the Intensive Care Unit: State-of-the-Art and Perspectives

 ,
,  , , , , ,
, , , , , 
 ,
,  and
and 
Abstract
:1. Introduction
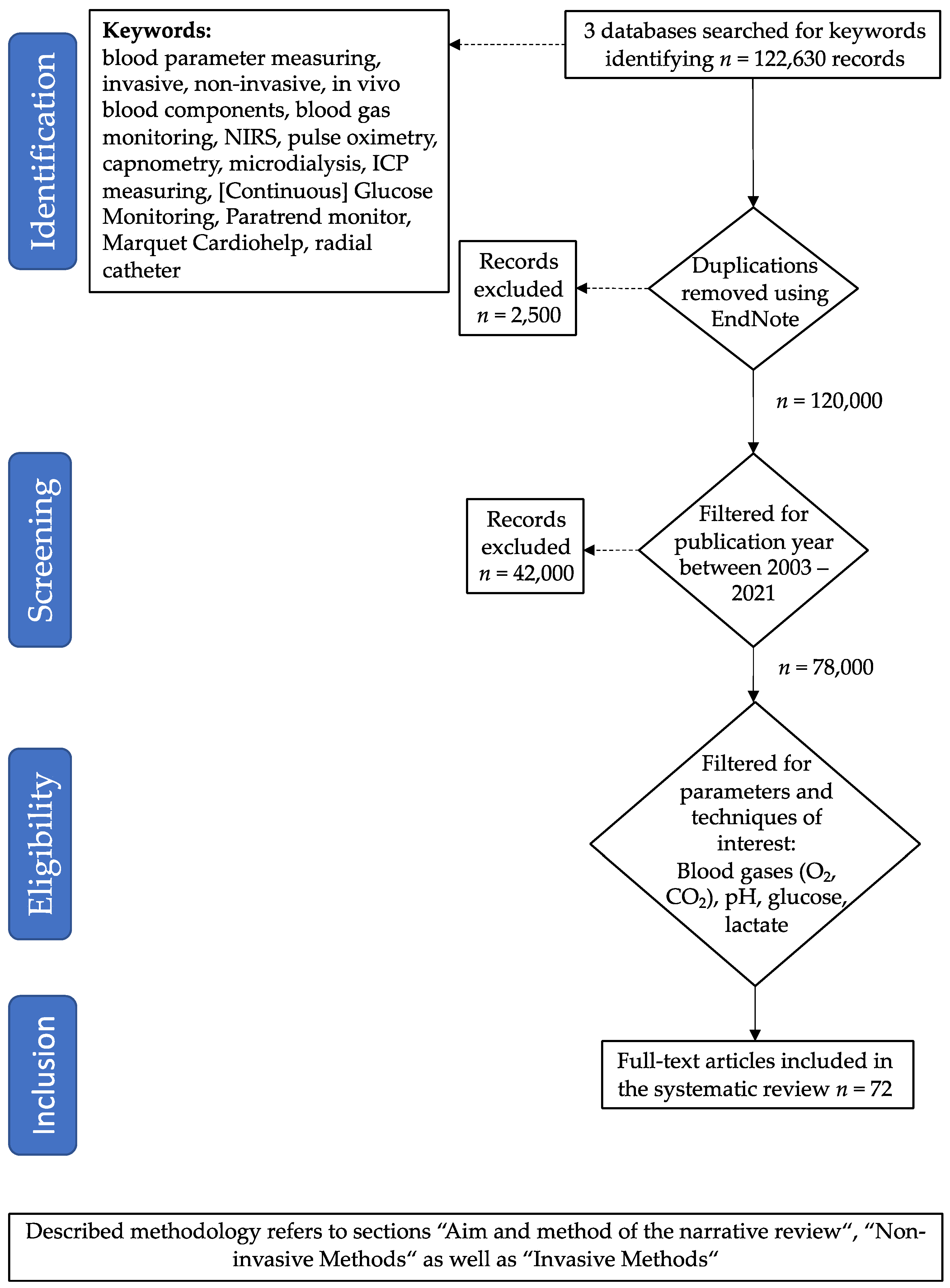
2. Aim and Method of This Review
3. Non-Invasive Methods
3.1. Pulse Oximetry
3.2. Capnometry and Capnography
3.3. Transcutaneous Blood Gas Monitoring
3.4. Near Infrared Spectroscopy (NIRS)
3.5. Transcutaneous Bilirubinometry
3.6. Non-Invasive Lactate Sensors
3.7. Sweat Sensors
4. Invasive Methods
4.1. Oxygen Sensors
4.2. Intracranial Probes
4.3. Microdialysis
4.4. Paratrend Monitor System
4.5. Devices in Combination with ECMO Systems
4.6. Continuous Measurement of pH, pCO2, pO2
4.7. Continuous Glucose Monitoring
5. Towards the New Generation of Biosensing Systems
5.1. Point-of-Care-Devices
5.2. Miniaturization Processes and Biosensor Development
6. Complete Electronic Sensing Solutions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistische Bundesamt (Destatis). Zahl der Intensivbetten in Deutschland von 1991 bis 2018. 2021. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/10/PD20_N064_231.html (accessed on 13 April 2021).
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Peeler, A.; Gleason, K.T.; Cho, S.-M.; Davidson, P.M. Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: How do we Expand Capacity in the COVID-19 Era? Heart Lung Circ. 2021, 30, 623–625. [Google Scholar] [CrossRef]
- EuroELSO. EuroELSO Survey on ECMO Use in Adult COVID-19 Patients in Europe. Available online: https://www.euroelso.net/covid-19/covid-19-survey/ (accessed on 16 March 2021).
- Vincent, J.L.; Baron, J.F.; Reinhart, K.; Gattinoni, L.; Thijs, L.; Webb, A.; Meier-Hellmann, A.; Nollet, G.; Peres-Bota, D. Anemia and blood transfusion in critically ill patients. JAMA 2002, 288, 1499–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freire Jorge, P.; Wieringa, N.; de Felice, E.; van der Horst, I.C.C.; Oude Lansink, A.; Nijsten, M.W. The association of early combined lactate and glucose levels with subsequent renal and liver dysfunction and hospital mortality in critically ill patients. Crit. Care 2017, 21, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, J.; Nijsten, M.W.; Jansen, T.C. Clinical use of lactate monitoring in critically ill patients. Ann. Intensive Care 2013, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Castro, R.; Kattan, E.; Ferri, G.; Pairumani, R.; Valenzuela, E.D.; Alegría, L.; Oviedo, V.; Pavez, N.; Soto, D.; Vera, M.; et al. Effects of capillary refill time-vs. lactate-targeted fluid resuscitation on regional, microcirculatory and hypoxia-related perfusion parameters in septic shock: A randomized controlled trial. Ann. Intensive Care 2020, 10, 150. [Google Scholar] [CrossRef]
- Vincent, J.L.; Quintairos, E.S.A.; Couto, L., Jr.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: A systematic review. Crit. Care 2016, 20, 257. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Hafen, B.B.; Sharma, S.; Chan, E.D.; Chan, M.M.M.; Chan, M.M.M. Oxygen Saturation. In Respiratory Medicine; Elsevier Ltd.: Amsterdam, The Netherlands, 2021; Volume 107, pp. 789–799. [Google Scholar]
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse oximetry: Understanding its basic principles facilitates appreciation of its limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef] [Green Version]
- Sanders, A.B. Capnometry in emergency medicine. Ann. Emerg. Med. 1989, 18, 1287–1290. [Google Scholar] [CrossRef]
- Newell, C.; Grier, S.; Soar, J. Airway and ventilation management during cardiopulmonary resuscitation and after successful resuscitation. Crit. Care 2018, 22, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Resuscitation Council. ERC Guidelines. Available online: https://cprguidelines.eu/ (accessed on 24 April 2022).
- Nassar, B.S.; Schmidt, G.A. Capnography During Critical Illness. CHEST 2016, 149, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Kupnik, D.; Skok, P. Capnometry in the prehospital setting: Are we using its. Emerg. Med. J. 2007, 24, 614–617. [Google Scholar] [CrossRef]
- Rüdiger, M.; Töpfer, K.; Hammer, H.; Schmalisch, G.; Wauer, R.R. A survey of transcutaneous blood gas monitoring among European neonatal intensive care units. BMC Pediatr. 2005, 5, 30. [Google Scholar] [CrossRef] [Green Version]
- Weinmann, K.; Lenz, A.; Heudorfer, R.; Aktolga, D.; Rattka, M.; Bothner, C.; Pott, A.; Öchsner, W.; Rottbauer, W.; Dahme, T. Continuous transcutaneous carbon-dioxide monitoring to avoid hypercapnia in complex catheter ablations under conscious sedation. Int. J. Cardiol. 2021, 325, 69–75. [Google Scholar] [CrossRef]
- Andrews, K.L.; Dib, M.Y.; Shives, T.C.; Hoskin, T.L.; Liedl, D.A.; Boon, A.J. Noninvasive arterial studies including transcutaneous oxygen pressure measurements with the limbs elevated or dependent to predict healing after partial foot amputation. Am. J. Phys. Med. Rehabil. 2013, 92, 385–392. [Google Scholar] [CrossRef]
- Huch, R.; Lübbers, D.W.; Huch, A. Quantitative continuous measurement of partial oxygen pressure on the skin of adults and new-born babies. Pflügers Archiv. 1972, 337, 185–198. [Google Scholar] [CrossRef]
- Severinghaus, J.W. A combined transcutaneous PO2-PCO2 electrode with electrochemical HCO3- stabilization. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 51, 1027–1032. [Google Scholar] [CrossRef]
- Weteringen, W.v.; Essen, T.v.; Gangaram-Panday, N.H.; Goos, T.G.; Jonge, R.C.J.d.; Reiss, I.K.M. Validation of a New Transcutaneous tcPO2/tcPCO2 Sensor with an Optical Oxygen Measurement in Preterm Neonates. Neonatology 2020, 117, 628–636. [Google Scholar] [CrossRef]
- Fraunhofer IPM, Freiburg, Germany, Arterial Blood Gas Test. Available online: https://www.ipm.fraunhofer.de/en/bu/gas-and-process-technology/applications/health/patient-monitoring/arterial-blood-gas-test.html (accessed on 24 April 2022).
- Hampton, D.A.; Schreiber, M.A. Near infrared spectroscopy: Clinical and research uses. Transfusion 2013, 53, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.N.; Gopinath, S.P.; Robertson, C.S. Clinical application of near-infrared spectroscopy in patients with traumatic brain injury: A review of the progress of the field. Neurophotonics 2016, 3, 031409. [Google Scholar] [CrossRef] [PubMed]
- Scheeren, T.W.L.; Schober, P.; Schwarte, L.A. Monitoring tissue oxygenation by near infrared spectroscopy (NIRS): Background and current applications. J. Clin. Monit. Comput. 2012, 26, 279–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fallgatter, A.J.; Ehlis, A.C.; Wagener, A.; Michel, T.; Herrmann, M.J. Nah-Infrarot-Spektroskopie in der Psychiatrie. Der Nervenarzt 2004, 75, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Bolkenius, D.; Dumps, C.; Rupprecht, B. Nahinfrarotspektroskopie. Der Anaesthesist 2021, 70, 190–203. [Google Scholar] [CrossRef] [PubMed]
- Mille, T.; Tachimiri, M.E.; Klersy, C.; Ticozzelli, G.; Bellinzona, G.; Blangetti, I.; Pirrelli, S.; Lovotti, M.; Odero, A. Near Infrared Spectroscopy Monitoring During Carotid Endarterectomy: Which Threshold Value is Critical? Eur. J. Vasc. Endovasc. Surg. 2004, 27, 646–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, N.; Thabut, D. Neurological Complications Occurring After Liver Transplantation: Role of Risk Factors, Hepatic Encephalopathy, and Acute (on Chronic) Brain Injury. Liver Transpl. 2019, 25, 469–487. [Google Scholar] [CrossRef]
- Edmonds, H.L., Jr.; Ganzel, B.L.; Austin, E.H., 3rd. Cerebral oximetry for cardiac and vascular surgery. Semin. Cardiothorac. Vasc. Anesth. 2004, 8, 147–166. [Google Scholar] [CrossRef]
- De Luca, D.; Romagnoli, C.; Tiberi, E.; Zuppa, A.A.; Zecca, E. Skin bilirubin nomogram for the first 96 h of life in a European normal healthy newborn population, obtained with multiwavelength transcutaneous bilirubinometry. Acta Paediatr. Int. J. Paediatr. 2008, 97, 146–150. [Google Scholar] [CrossRef]
- Rizvi, M.R.; Alaskar, F.M.; Albaradie, R.S.; Rizvi, N.F.; Al-Abdulwahab, K. A Novel Non-invasive Technique of Measuring Bilirubin Levels Using BiliCapture. Oman Med. J. 2019, 34, 26–33. [Google Scholar] [CrossRef]
- El-Beshbishi, S.N.; Shattuck, K.E.; Mohammad, A.A.; Petersen, J.R. Hyperbilirubinemia and transcutaneous bilirubinometry. Clin. Chem. 2009, 55, 1280–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastasova, S.; Crewther, B.; Bembnowicz, P.; Curto, V.; Ip, H.M.; Rosa, B.; Yang, G.Z. A wearable multisensing patch for continuous sweat monitoring. Biosens. Bioelectron. 2017, 93, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Sakharov, D.A.; Shkurnikov, M.U.; Vagin, M.Y.; Yashina, E.I.; Karyakin, A.A.; Tonevitsky, A.G. Relationship between lactate concentrations in active muscle sweat and whole blood. Bull. Exp. Biol. Med. 2010, 150, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Emaminejad, S.; Nyein, H.Y.Y.; Challa, S.; Chen, K.; Peck, A.; Fahad, H.M.; Ota, H.; Shiraki, H.; Kiriya, D.; et al. Fully integrated wearable sensor arrays for multiplexed in situ perspiration analysis. Nature 2016, 529, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Rassaei, L.; Olthuis, W.; Tsujimura, S.; Sudhölter, E.J.; van den Berg, A. Lactate biosensors: Current status and outlook. Anal. Bioanal. Chem. 2014, 406, 123–137. [Google Scholar] [CrossRef]
- Wang, Z.; Shin, J.; Park, J.-H.; Lee, H.; Kim, D.-H.; Liu, H. Engineering Materials for Electrochemical Sweat Sensing. Adv. Funct. Mater. 2021, 31, 2008130. [Google Scholar] [CrossRef]
- Berthomieu, C.; Hienerwadel, R. Fourier transform infrared (FTIR) spectroscopy. Photosynth. Res. 2009, 101, 157–170. [Google Scholar] [CrossRef]
- Klein, K.U.; Boehme, S.; Hartmann, E.K.; Szczyrba, M.; David, M.; Markstaller, K.; Engelhard, K. A Novel Technique for Monitoring of Fast Variations in Brain Oxygen Tension Using an Uncoated Fluorescence Quenching Probe (Foxy AL-300). J. Neurosurg. Anesthesiol. 2011, 23, 341–346. [Google Scholar] [CrossRef]
- Orakcioglu, B.; Sakowitz, O.W.; Neumann, J.O.; Kentar, M.M.; Unterberg, A.; Kiening, K.L. Evaluation of a novel brain tissue oxygenation probe in an experimental swine model. Neurosurgery 2010, 67, 1716–1722; discussion 1722–1723. [Google Scholar] [CrossRef]
- Evensen, K.B.; Eide, P.K. Measuring intracranial pressure by invasive, less invasive or non-invasive means: Limitations and avenues for improvement. Fluids Barriers CNS 2020, 17, 34. [Google Scholar] [CrossRef]
- Schulte am Esch, J.; Bause, H.; Kochs, E.; Scholz, J.; Standl, T.; Werner, C. Duale Reihe Anästhesie, 4th ed.; Thieme: Stuttgart, Germany, 2011. [Google Scholar] [CrossRef]
- Keller, E.; Froehlich, J.; Muroi, C.; Sikorski, C.; Muser, M. Neuromonitoring in Intensive Care: A New Brain Tissue Probe for Combined Monitoring of Intracranial Pressure (ICP) Cerebral Blood Flow (CBF) and Oxygenation. In Early Brain Injury or Cerebral Vasospasm; Feng, H., Mao, Y., Zhang, J.H., Eds.; Springer: Vienna, Austria, 2011; pp. 217–220. [Google Scholar]
- Seule, M.; Sikorski, C.; Sakowitz, O.; von Campe, G.; Santos, E.; Orakcioglu, B.; Unterberg, A.; Keller, E. Evaluation of a New Brain Tissue Probe for Intracranial Pressure, Temperature, and Cerebral Blood Flow Monitoring in Patients with Aneurysmal Subarachnoid Hemorrhage. Neurocrit. Care 2016, 25, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chefer, V.I.; Thompson, A.C.; Zapata, A.; Shippenberg, T.S. Overview of brain microdialysis. Curr. Protoc. Neurosci. 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millan, M.J.; Panayi, F.; Rivet, J.M.; Di Cara, B.; Cistarelli, L.; Billiras, R.; Girardon, S.; Gobert, A. Chapter 6.1 The role of microdialysis in drug discovery: Focus on antipsychotic agents. Handb. Behav. Neurosci. 2006, 16, 485–511. [Google Scholar] [CrossRef]
- Lajtha, A.; Gibson, G.E.; Dienel, G.A. Handbook of Neurochemistry and Molecular Neurobiology; Springer: Boston, MA, USA, 2008. [Google Scholar]
- Hammarlund-Udenaes, M. Microdialysis as an Important Technique in Systems Pharmacology—A Historical and Methodological Review. AAPS J. 2017, 19, 1294–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shippenberg, T.S.; Thompson, A.C. Overview of Microdialysis. Available online: https://currentprotocols.onlinelibrary.wiley.com/doi/10.1002/0471142301 (accessed on 24 April 2022).
- Gamo, M.; Hirose, Y.; Matsuo, K. Problems in clinical use of intraarterial blood gas monitoring system, Paratrend 7. Masui. Jpn. J. Anesthesiol. 2000, 49, 1387–1390. [Google Scholar]
- Pavlidis, T.; Papaziogas, B.; Vretzakis, G.; Argiriadou, H.; Sfira, E.; Papaziogas, T. Continuous monitoring of arterial blood gases and pH during laparoscopic cholecystectomy using a Paratrend sensor. Minerva Chir. 2002, 57, 17–22. [Google Scholar]
- Ganter, M.; Zollinger, A. Continuous intravascular blood gas monitoring: Development, current techniques, and clinical use of a commercial device. Br. J. Anaesth. 2003, 91, 397–407. [Google Scholar] [CrossRef] [Green Version]
- Mantouvalou, M.; Latrelli, I.; Kyriazopoulos, G.; Nikolaidis, C.; Sfiras, D. The Paratrend sensor as a tool for continuous measurement of arterial blood gases: A-730. Eur. J. Anaesthesiol. 2004, 21, 338–340. [Google Scholar] [CrossRef]
- Saich, C.; Graystone, S.J.; Hendry, S.P.; Clutton-Brock, T.H. Nursing care of the paratrend 7 sensor. Intensive Crit. Care Nurs. 1997, 13, 338–340. [Google Scholar] [CrossRef]
- Baldini, F. Chemical and biochemical optical fibre sensing for invasive and intracellular application: Past, present and future. In Proceedings of the 2020 Asia Communications and Photonics Conference (ACP) and International Conference on Information Photonics and Optical Communications (IPOC), Beijing, China, 24–27 October 2020; pp. 1–3. [Google Scholar]
- Staudinger, T. Extrakorporale Lungenersatzver fahren–was gibt es Neues, was kommt? Med. Klin.-Intensivmed. Notfallmed. 2016, 113, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Alwardt, C.M.; Wilson, D.S.; Alore, M.L.; Lanza, L.A.; DeValeria, P.A.; Pajaro, O.E. Performance and safety of an integrated portable extracorporeal life support system for adults. J. Extra-Corpor. Technol. 2015, 47, 38–43. [Google Scholar] [PubMed]
- Arlt, M.; Philipp, A.; Voelkel, S.; Camboni, D.; Rupprecht, L.; Graf, B.M.; Schmid, C.; Hilker, M. Hand-held minimised extracorporeal membrane oxygenation: A new bridge to recovery in patients with out-of-centre cardiogenic shock. Eur. J. Cardio-thorac. Surg. 2011, 40, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Menzel, M.; Soukup, J.; Henze, D.; Engelbrecht, K.; Senderreck, M.; Scharf, A.; Rieger, A.; Grond, S. Experiences with continuous intra-arterial blood gas monitoring: Precision and drift of a pure optode-system. Intensive Care Med. 2003, 29, 2180–2186. [Google Scholar] [CrossRef] [PubMed]
- Gelsomino, S.; Lorusso, R.; Livi, U.; Romagnoli, S.; Romano, S.M.; Carella, R.; Lucà, F.; Billè, G.; Matteucci, F.; Renzulli, A.; et al. Assessment of a continuous blood gas monitoring system in animals during circulatory stress. BMC Anesthesiol. 2011, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, W.W.; Yafuso, M.; Yan, C.F.; Hui, H.K.; Arick, S. Performance of an in-vivo, continuous blood-gas monitor with disposable probe. Clin. Chem. 1987, 33, 1538–1542. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.J.; Gavin, J.R., 3rd. Flash Continuous Glucose Monitoring: A Summary Review of Recent Real-World Evidence. Clin. Diabetes 2021, 39, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, V.; Stimson, R.H.; Zammitt, N.N.; Ritchie, S.A.; McKnight, J.A.; Dover, A.R.; Gibb, F.W. Marked improvement in HbA(1c) following commencement of flash glucose monitoring in people with type 1 diabetes. Diabetologia 2019, 62, 1349–1356. [Google Scholar] [CrossRef] [Green Version]
- Fokkert, M.; van Dijk, P.; Edens, M.; Barents, E.; Mollema, J.; Slingerland, R.; Gans, R.; Bilo, H. Improved well-being and decreased disease burden after 1-year use of flash glucose monitoring (FLARE-NL4). BMJ Open Diabetes Res. Care 2019, 7, e000809. [Google Scholar] [CrossRef] [Green Version]
- Charleer, S.; De Block, C.; Van Huffel, L.; Broos, B.; Fieuws, S.; Nobels, F.; Mathieu, C.; Gillard, P. Quality of Life and Glucose Control After 1 Year of Nationwide Reimbursement of Intermittently Scanned Continuous Glucose Monitoring in Adults Living With Type 1 Diabetes (FUTURE): A Prospective Observational Real-World Cohort Study. Diabetes Care 2020, 43, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Krinsley, J.S.; Chase, J.G.; Gunst, J.; Martensson, J.; Schultz, M.J.; Taccone, F.S.; Wernerman, J.; Bohe, J.; De Block, C.; Desaive, T.; et al. Continuous glucose monitoring in the ICU: Clinical considerations and consensus. Crit. Care 2017, 21, 197. [Google Scholar] [CrossRef] [Green Version]
- Finfer, S.; Liu, B.; Chittock, D.R.; Norton, R.; Myburgh, J.A.; McArthur, C.; Mitchell, I.; Foster, D.; Dhingra, V.; Henderson, W.R.; et al. Hypoglycemia and risk of death in critically ill patients. N. Engl. J. Med. 2012, 367, 1108–1118. [Google Scholar] [CrossRef] [PubMed]
- Perez-Guzman, M.C.; Shang, T.; Zhang, J.Y.; Jornsay, D.; Klonoff, D.C. Continuous Glucose Monitoring in the Hospital. Endocrinol. Metab. 2021, 36, 240–255. [Google Scholar] [CrossRef] [PubMed]
- Heo, Y.J.; Shibata, H.; Okitsu, T.; Kawanishi, T.; Takeuchi, S. Long-term in vivo glucose monitoring using fluorescent hydrogel fibers. Proc. Natl. Acad. Sci. USA 2011, 108, 13399–13403. [Google Scholar] [CrossRef] [Green Version]
- Sawayama, J.; Okitsu, T.; Nakamata, A.; Kawahara, Y.; Takeuchi, S. Hydrogel Glucose Sensor with In Vivo Stable Fluorescence Intensity Relying on Antioxidant Enzymes for Continuous Glucose Monitoring. iScience 2020, 23, 101243. [Google Scholar] [CrossRef] [PubMed]
- Leland, C.; Clark, J.; Wolf, R.; Granger, D.; Taylor, Z. Continuous Recording of Blood Oxygen Tensions by Polarography. J. Appl. Physiol. 1953, 6, 189–193. [Google Scholar] [CrossRef]
- Clark, L.C., Jr.; Lyons, C. Electrode systems for continuous monitoring in cardiovascular surgery. Ann. N. Y. Acad. Sci. 1962, 102, 29–45. [Google Scholar] [CrossRef]
- Cho, I.-H.; Kim, D.H.; Park, S. Electrochemical biosensors: Perspective on functional nanomaterials for on-site analysis. Biomater. Res. 2020, 24, 6. [Google Scholar] [CrossRef] [Green Version]
- Ronkainen, N.J.; Halsall, H.B.; Heineman, W.R. Electrochemical biosensors. Chem. Soc. Rev. 2010, 39, 1747–1763. [Google Scholar] [CrossRef]
- Sanati, A.; Jalali, M.; Raeissi, K.; Karimzadeh, F.; Kharaziha, M.; Mahshid, S.S.; Mahshid, S. A review on recent advancements in electrochemical biosensing using carbonaceous nanomaterials. Microchim. Acta 2019, 186, 773. [Google Scholar] [CrossRef]
- Luo, X.; Davis, J.J. Electrical biosensors and the label free detection of protein disease biomarkers. Chem. Soc. Rev. 2013, 42, 5944–5962. [Google Scholar] [CrossRef]
- Choi, H.K.; Lee, J.-H.; Lee, T.; Lee, S.-N.; Choi, J.-W. Flexible Electronics for Monitoring in vivo Electrophysiology and Metabolite Signals. Front. Chem. 2020, 8, 547591. [Google Scholar] [CrossRef] [PubMed]
- Vadgama, P. Monitoring with In Vivo Electrochemical Sensors: Navigating the Complexities of Blood and Tissue Reactivity. Sensors 2020, 20, 3149. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Arroyo-Currás, N.; Kang, D.; Ricci, F.; Plaxco, K.W. Dual-Reporter Drift Correction To Enhance the Performance of Electrochemical Aptamer-Based Sensors in Whole Blood. J. Am. Chem. Soc. 2016, 138, 15809–15812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundblad, M.; Price, D.A.; Burmeister, J.J.; Quintero, J.E.; Huettl, P.; Pomerleau, F.; Zahniser, N.R.; Gerhardt, G.A. Tonic and Phasic Amperometric Monitoring of Dopamine Using Microelectrode Arrays in Rat Striatum. Appl. Sci. 2020, 10, 6449. [Google Scholar] [CrossRef]
- Li, S.; Dai, J.; Zhu, M.; Arroyo-Currás, N.; Li, H.; Wang, Y.; Wang, Q.; Lou, X.; Kippin, T.E.; Wang, S.; et al. Hydrogel-coating improves the in-vivo stability of electrochemical aptamer-based biosensors. bioRxiv 2020. [Google Scholar] [CrossRef]
- Burugapalli, K.; Wijesuriya, S.; Wang, N.; Song, W. Biomimetic electrospun coatings increase the in vivo sensitivity of implantable glucose biosensors. J. Biomed. Mater. Res. Part A 2018, 106, 1072–1081. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Wang, S.; Liu, Y.; Xu, Z.; Zhang, K.; Guo, Y. Development of Cu nanoflowers modified the flexible needle-type microelectrode and its application in continuous monitoring glucose in vivo. Biosens. Bioelectron. 2018, 110, 44–51. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, S.; Zhang, S.; Li, Y.; Qu, Z.; Chen, Y.; Lu, B.; Wang, X.; Feng, X. Skin-like biosensor system via electrochemical channels for noninvasive blood glucose monitoring. Sci. Adv. 2017, 3, e1701629. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.-C.; Kim, K.-B.; Gurudatt, N.G.; Hussain, K.K.; Choi, C.S.; Park, D.-S.; Shim, Y.-B. Comparison of enzymatic and non-enzymatic glucose sensors based on hierarchical Au-Ni alloy with conductive polymer. Biosens. Bioelectron. 2019, 130, 48–54. [Google Scholar] [CrossRef]
- Haghparas, Z.; Kordrostami, Z.; Sorouri, M.; Rajabzadeh, M.; Khalifeh, R. Highly sensitive non-enzymatic electrochemical glucose sensor based on dumbbell-shaped double-shelled hollow nanoporous CuO/ZnO microstructures. Sci. Rep. 2021, 11, 344. [Google Scholar] [CrossRef]
- Ahmad, R.; Tripathy, N.; Ahn, M.-S.; Bhat, K.S.; Mahmoudi, T.; Wang, Y.; Yoo, J.-Y.; Kwon, D.-W.; Yang, H.-Y.; Hahn, Y.-B. Highly Efficient Non-Enzymatic Glucose Sensor Based on CuO Modified Vertically-Grown ZnO Nanorods on Electrode. Sci. Rep. 2017, 7, 5715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Chang, S.J.; Chen, C.J.; Liu, J.T. Non-Invasive Blood Glucose Monitoring Technology: A Review. Sensors 2020, 20, 6925. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, T.; Foster, R.; Hao, Y. Radio-Frequency and Microwave Techniques for Non-Invasive Measurement of Blood Glucose Levels. Diagnostics 2019, 9, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omer, A.E.; Shaker, G.; Safavi-Naeini, S.; Kokabi, H.; Alquié, G.; Deshours, F.; Shubair, R.M. Low-cost portable microwave sensor for non-invasive monitoring of blood glucose level: Novel design utilizing a four-cell CSRR hexagonal configuration. Sci. Rep. 2020, 10, 15200. [Google Scholar] [CrossRef] [PubMed]
- Omer, A.E.; Safavi-Naeini, S.; Hughson, R.; Shaker, G. Blood Glucose Level Monitoring Using an FMCW Millimeter-Wave Radar Sensor. Remote Sens. 2020, 12, 385. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.; Cano-Garcia, H.; Sotiriou, I.; Lipscombe, O.; Gouzouasis, I.; Koutsoupidou, M.; Palikaras, G.; Mackenzie, R.; Reeve, T.; Kosmas, P.; et al. A Glucose Sensing System Based on Transmission Measurements at Millimetre Waves using Micro strip Patch Antennas. Sci. Rep. 2017, 7, 6855. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Measuring Method | Area of Detection | Measured Parameters | Scope of Application (Selection) | References |
|---|---|---|---|---|
| Pulse oximetry | Fingertip, earlap, tip of the nose | Oxygen saturation | Evaluation of vital parameters in various settings, esp. respiratory failure | Hafen et al., 2021, ref. [12] Chan et al., 2013, ref. [13] |
| Capnometry | Endotracheal ventilation tube | Exspiratory pCO2 | Efficiency of CPR, monitoring of intubation, detection of respiratory failure | Nassar et al., 2016, ref. [17] Kupnik et al., 2007, ref. [18] |
| NIRS (Near Infra-Red Spectroscopy) | Scalp | Brain tissue oxygenation | General surgery, traumatic brain injury (TBI) | Sen et al., 2016, ref. [27] Scheeren et al., 2012, ref. [28] |
| Bilirubinometry | Skin, mostly forehead/sternum | Subcutaneous bilirubin concentration | Consideration of therapy, continual monitoring | De Luca et al., 2008, ref. [34] Rizvi et al., 2019, ref. [35] |
| Measuring Method | Area of Detection | Measured Parameters | Scope of Application (Selection) | References |
|---|---|---|---|---|
| Intracranial probes | Intracranial (brain tissue) | ICP, pH, pO2, lactate, temperature | traumatic brain injury, intracerebral bleeding, infection | Evensen et al., 2020, ref. [45] Keller et al., 2011, ref. [47] Seule et al., 2016, ref. [48] |
| Microdialysis | Intracranial (in the blood cycle) | Neurotransmitters, metabolic substrates | Neurosurgical and general intensive care | Chefer et al., 2009, ref. [49] Hammarlund-Udenaes et al., 2017, ref. [52] Shippenberg et al., 1997, ref. [53] |
| Paratrend monitor | Blood vessels, mostly radial or femoral artery | pH, pO2, pCO2, temperature | ICU, thoracic and great vessel surgery | Ganter et al., 2003, ref. [56] Mantouvalou et al., 2004, ref. [57] |
| Marquet Cardiohelp (ECMO) | Sensors and probes within the device | Blood pressure, temperature, hemoglobin, hematocrit | ARDS, aortic surgery, extracorporeal CPR, rewarming | Staudinger et al., 2016, ref. [60] Alwardt et al., 2015, ref. [61] Arlt et al., 2011, ref. [62] |
| CGM (Continuous glucose monitoring) | Subcutaneous, mostly arm | Interstitial blood glucose level | Diabetes monitoring | Bailey et al., 2021, ref. [66] Krinsley et al., 2017, ref. [70] Perez-Guzman et al., 2021, ref. [72] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bockholt, R.; Paschke, S.; Heubner, L.; Ibarlucea, B.; Laupp, A.; Janićijević, Ž.; Klinghammer, S.; Balakin, S.; Maitz, M.F.; Werner, C.; et al. Real-Time Monitoring of Blood Parameters in the Intensive Care Unit: State-of-the-Art and Perspectives. J. Clin. Med. 2022, 11, 2408. https://doi.org/10.3390/jcm11092408
Bockholt R, Paschke S, Heubner L, Ibarlucea B, Laupp A, Janićijević Ž, Klinghammer S, Balakin S, Maitz MF, Werner C, et al. Real-Time Monitoring of Blood Parameters in the Intensive Care Unit: State-of-the-Art and Perspectives. Journal of Clinical Medicine. 2022; 11(9):2408. https://doi.org/10.3390/jcm11092408
Chicago/Turabian StyleBockholt, Rebecca, Shaleen Paschke, Lars Heubner, Bergoi Ibarlucea, Alexander Laupp, Željko Janićijević, Stephanie Klinghammer, Sascha Balakin, Manfred F. Maitz, Carsten Werner, and et al. 2022. "Real-Time Monitoring of Blood Parameters in the Intensive Care Unit: State-of-the-Art and Perspectives" Journal of Clinical Medicine 11, no. 9: 2408. https://doi.org/10.3390/jcm11092408
APA StyleBockholt, R., Paschke, S., Heubner, L., Ibarlucea, B., Laupp, A., Janićijević, Ž., Klinghammer, S., Balakin, S., Maitz, M. F., Werner, C., Cuniberti, G., Baraban, L., & Spieth, P. M. (2022). Real-Time Monitoring of Blood Parameters in the Intensive Care Unit: State-of-the-Art and Perspectives. Journal of Clinical Medicine, 11(9), 2408. https://doi.org/10.3390/jcm11092408