
Evinacumab, an ANGPTL3 Inhibitor, in the Treatment of Dyslipidemia

 , ,
, , 
Abstract
:1. Homozygous Familial Hypercholesterolemia
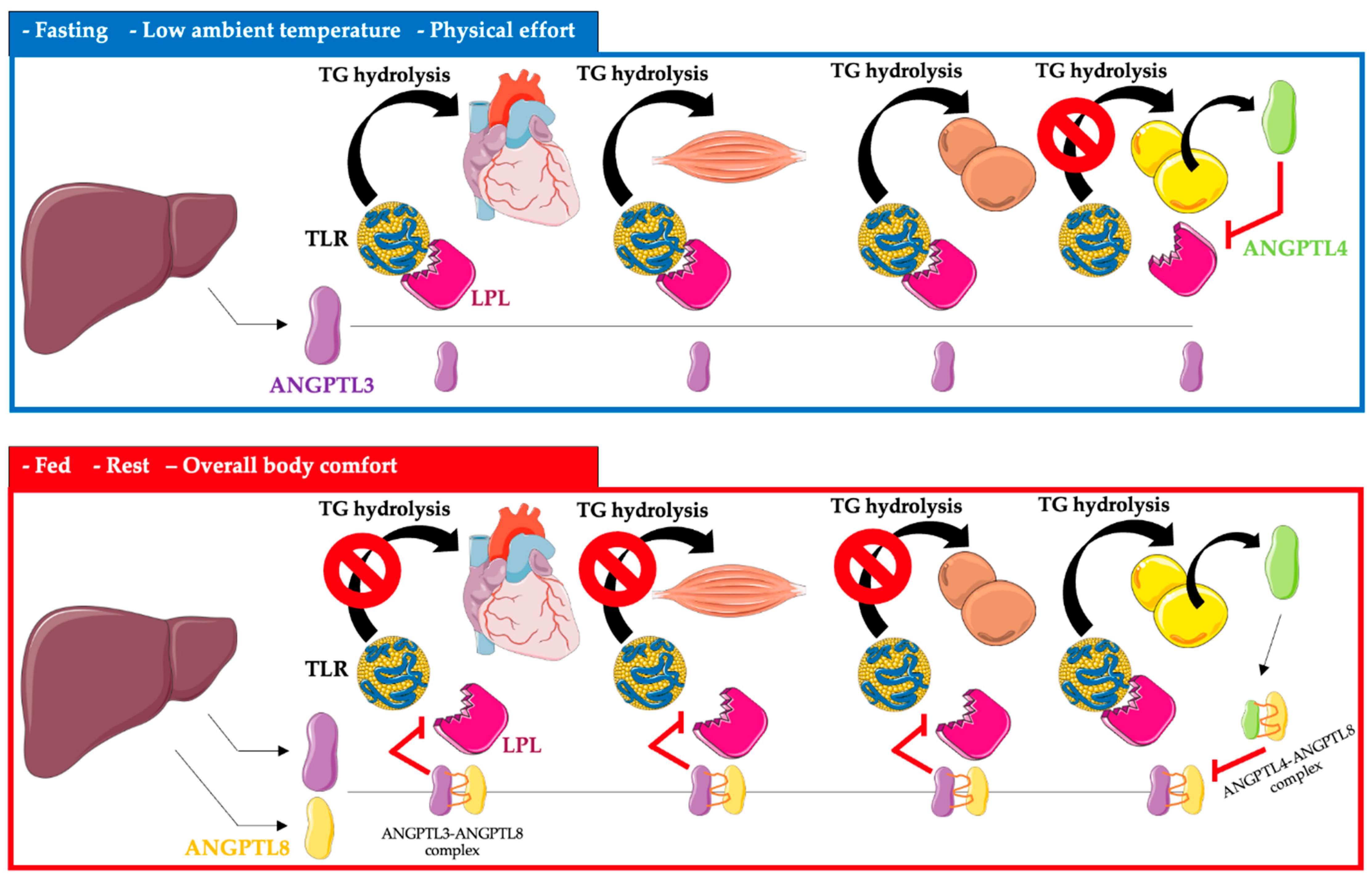
2. ANGPTL3, 4, and 8 Protein System-Characteristics and Role in Lipid Metabolism
3. ANGPTL3, 4, and 8 as Biomarkers of Cardiovascular Risk
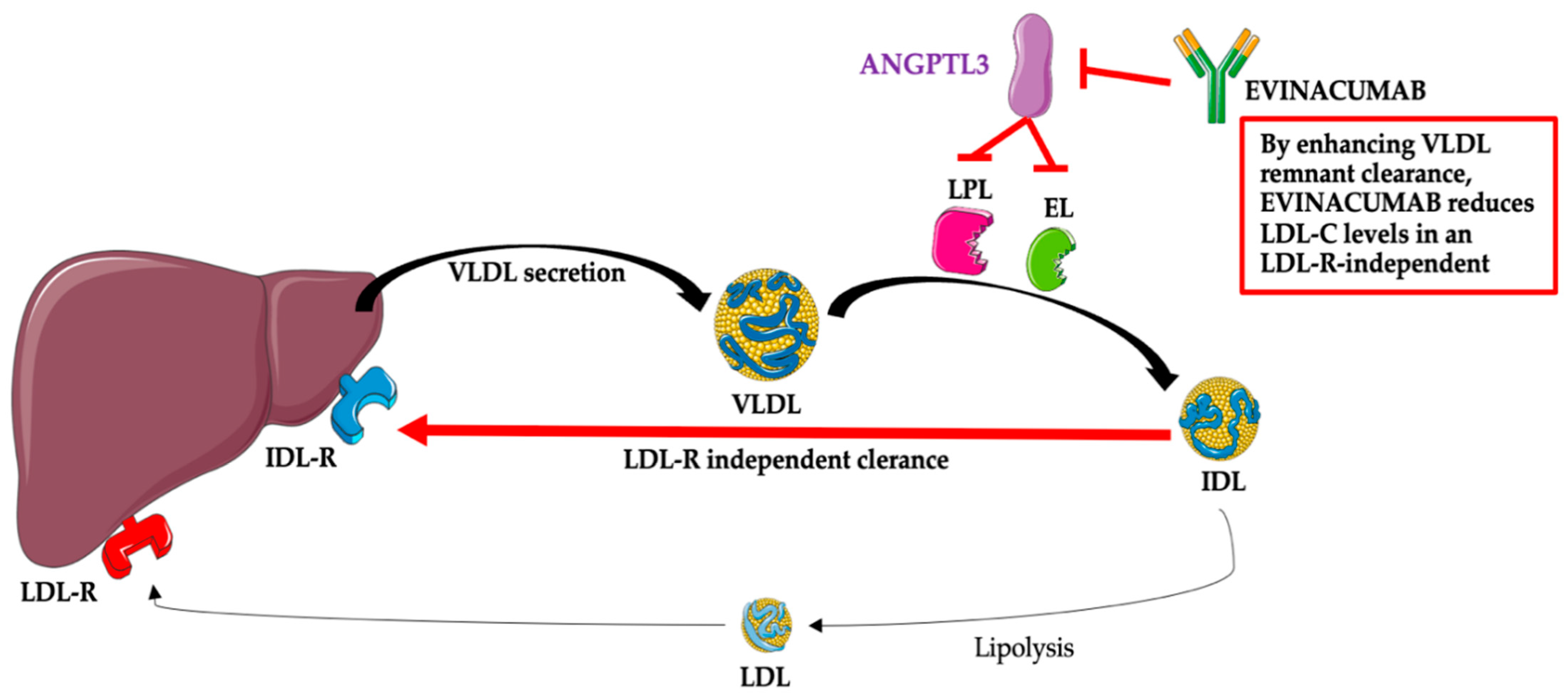
4. Evinacumab-Structure and the Mechanism of Action
Clinical Trials and Scientific Research
5. Perspectives of Evinacumab in Clinical Lipidology
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenson, R.S. Existing and emerging therapies for the treatment of familial hypercholesterolemia. J. Lipid Res. 2021, 62, 100060. [Google Scholar] [CrossRef] [PubMed]
- Cuchel, M.; Bruckert, E.; Ginsberg, H.N.; Raal, F.J.; Santos, R.D.; Hegele, R.A.; Kuivenhoven, J.A.; Nordestgaard, B.G.; Descamps, O.S.; Steinhagen-Thiessen, E.; et al. Homozygous familial hypercholesterolaemia: New insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur. Heart J. 2014, 35, 2146–2157. [Google Scholar] [CrossRef] [PubMed]
- Raal, F.J.; Rosenson, R.S.; Reeskamp, L.F.; Hovingh, G.K.; Kastelein, J.J.P.; Rubba, P.; Ali, S.; Banerjee, P.; Chan, K.C.; Gipe, D.A.; et al. Evinacumab for Homozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 383, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Harada-Shiba, M.; Ali, S.; Gipe, D.A.; Gasparino, E.; Son, V.; Zhang, Y.; Pordy, R.; Catapano, A.L. A randomized study investigating the safety, tolerability, and pharmacokinetics of evinacumab, an ANGPTL3 inhibitor, in healthy Japanese and Caucasian subjects. Atherosclerosis 2020, 314, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S.; Burgess, L.J.; Ebenbichler, C.F.; Baum, S.J.; Stroes, E.S.G.; Ali, S.; Khilla, N.; Hamlin, R.; Pordy, R.; Dong, Y.; et al. Evinacumab in Patients with Refractory Hypercholesterolemia. N. Engl. J. Med. 2020, 383, 2307–2319. [Google Scholar] [CrossRef] [PubMed]
- Dijk, W.; Kersten, S. Regulation of lipid metabolism by angiopoietin-like proteins. Curr. Opin. Lipidol. 2016, 27, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Abu-Farha, M.; Ghosh, A.; Al-Khairi, I.; Madiraju, S.R.M.; Abubaker, J.; Prentki, M. The multi-faces of Angptl8 in health and disease: Novel functions beyond lipoprotein lipase modulation. Prog. Lipid Res. 2020, 80, 101067. [Google Scholar] [CrossRef]
- Solnica, B.; Sygitowicz, G.; Sitkiewicz, D.; Cybulska, B.; Jóźwiak, J.; Odrowąż-Sypniewska, G.; Banach, M. 2020 Guidelines of the Polish Society of Laboratory Diagnostics (PSLD) and the Polish Lipid Association (PoLA) on laboratory diagnostics of lipid metabolism disorders. Arch. Med. Sci. 2020, 16, 237–252. [Google Scholar] [CrossRef]
- Li, J.; Li, L.; Guo, D.; Li, S.; Zeng, Y.; Liu, C.; Fu, R.; Huang, M.; Xie, W. Triglyceride metabolism and angiopoietin-like proteins in lipoprotein lipase regulation. Clin. Chim. Acta 2020, 503, 19–34. [Google Scholar] [CrossRef]
- Morelli, M.B.; Chavez, C.; Santulli, G. Angiopoietin-like proteins as therapeutic targets for cardiovascular disease: Focus on lipid disorders. Expert Opin. Ther. Targets 2020, 24, 79–88. [Google Scholar] [CrossRef]
- Zhang, R. The ANGPTL3-4-8 model, a molecular mechanism for triglyceride trafficking. Open Biol. 2016, 6, 150272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stitziel, N.O.; Khera, A.V.; Wang, X.; Bierhals, A.J.; Vourakis, A.C.; Sperry, A.E.; Natarajan, P.; Klarin, D.; Emdin, C.A.; Zekavat, S.M.; et al. ANGPTL3 Deficiency and Protection Against Coronary Artery Disease. J. Am. Coll. Cardiol. 2017, 69, 2054–2063. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Romańczyk, M.; Filipiak, K.J. Angiopoietin-like proteins inhibitors: New horizons in the treatment of atherogenic dyslipidemia and familial hypercholesterolemia. Cardiol. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Romańczyk, M.; Filipiak, K.J. Evinacumab—The new kid on the block. Is it important for cardiovascular prevention? Int. J. Cardiol. Cardiovasc. Risk Prev. 2021, 11, 200107. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Romańczyk, M.; Filipiak, K.J. Evinacumab—An ANGPTL3 inhibitor; a new drug in the treatment of lipid disorders. Review on the literature and clinical studies. Folia Cardiol. 2021, 16, 30–39. [Google Scholar] [CrossRef]
- Khetarpal, S.A.; Vitali, C.; Levin, M.G.; Klarin, D.; Park, J.; Pampana, A.; Millar, J.S.; Kuwano, T.; Sugasini, D.; Subbaiah, P.V.; et al. Endothelial lipase mediates efficient lipolysis of triglyceride-rich lipoproteins. PLoS Genet. 2021, 17, e1009802. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Zhan, W.; Wei, L.; Xu, Z.; Fan, L.; Zhuo, Y.; Wang, C.; Zhang, J. Circulating ANGPTL3 and ANGPTL4 levels predict coronary artery atherosclerosis severity. Lipids Health Dis. 2021, 20, 154. [Google Scholar] [CrossRef]
- Dewey, F.E.; Gusarova, V.; Dunbar, R.L.; O’Dushlaine, C.; Schurmann, C.; Gottesman, O.; McCarthy, S.; Van Hout, C.V.; Bruse, S.; Dansky, H.M.; et al. Genetic and Pharmacologic Inactivation of ANGPTL3 and Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 211–221. [Google Scholar] [CrossRef]
- Stitziel, N.O.; Stirrups, K.E.; Masca, N.G.; Erdmann, J.; Ferrario, P.G.; König, I.R.; Weeke, P.E.; Webb, T.R.; Auer, P.L.; Schick, U.M.; et al. Coding Variation in ANGPTL4, LPL, and SVEP1 and the Risk of Coronary Disease. N. Engl. J. Med. 2016, 374, 1134–1144. [Google Scholar]
- Gusarova, V.; O’Dushlaine, C.; Teslovich, T.M.; Benotti, P.N.; Mirshahi, T.; Gottesman, O.; Van Hout, C.V.; Murray, M.F.; Mahajan, A.; Nielsen, J.B.; et al. Genetic inactivation of ANGPTL4 improves glucose homeostasis and is associated with reduced risk of diabetes. Nat. Commun. 2018, 9, 2252. [Google Scholar] [CrossRef]
- Klarin, D.; Damrauer, S.M.; Cho, K.; Sun, Y.V.; Teslovich, T.M.; Honerlaw, J.; Gagnon, D.R.; DuVall, S.L.; Li, J.; Peloso, G.M.; et al. Genetics of blood lipids among ~300,000 multi-ethnic participants of the Million Veteran Program. Nat. Genet. 2018, 50, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Evkeeza. EMA/250315/2021, 22 April 2021, Assesment Report. Procedure No. EMEA/H/C/005449/000. Available online: https://www.ema.europa.eu/en/documents/assessment-report/evkeeza-h-c-5449-0000-epar-assessment-report_en.pdf. (accessed on 20 October 2022).
- Evkeeza. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/evkeeza (accessed on 31 October 2022).
- Gusarova, V.; Banfi, S.; Alexa-Braun, C.A.; Shihanian, L.M.; Mintah, I.J.; Lee, J.S.; Xin, Y.; Su, Q.; Kamat, V.; Cohen, J.C.; et al. ANGPTL8 Blockade With a Monoclonal Antibody Promotes Triglyceride Clearance, Energy Expenditure, and Weight Loss in Mice. Endocrinology 2017, 158, 1252–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, Z.; Pordy, R.; Rader, D.J.; Gaudet, D.; Ali, S.; Gonzaga-Jauregui, C.; Ponda, M.P.; Shumel, B.; Banerjee, P.; Dunbar, R.L. Inhibition of Angiopoietin-Like Protein 3 With Evinacumab in Subjects With High and Severe Hypertriglyceridemia. J. Am. Coll. Cardiol. 2021, 78, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Z.; Banerjee, P.; Hamon, S.; Chan, K.C.; Bouzelmat, A.; Sasiela, W.J.; Pordy, R.; Mellis, S.; Dansky, H.; Gipe, D.A.; et al. Inhibition of Angiopoietin-Like Protein 3 With a Monoclonal Antibody Reduces Triglycerides in Hypertriglyceridemia. Circulation 2021, 140, 470–486, Erratum in Circulation 2021, 143, e799. [Google Scholar] [CrossRef]
- Gaudet, D.; Gipe, D.A.; Pordy, R.; Ahmad, Z.; Cuchel, M.; Shah, P.K.; Chyu, K.Y.; Sasiela, W.J.; Chan, K.C.; Brisson, D.; et al. ANGPTL3 Inhibition in Homozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2017, 377, 296–297. [Google Scholar] [CrossRef]
- Banerjee, P.; Chan, K.C.; Tarabocchia, M.; Benito-Vicente, A.; Alves, A.C.; Uribe, K.B.; Bourbon, M.; Skiba, P.J.; Pordy, R.; Gipe, D.A.; et al. Functional Analysis of LDLR (Low-Density Lipoprotein Receptor) Variants in Patient Lymphocytes to Assess the Effect of Evinacumab in Homozygous Familial Hypercholesterolemia Patients With a Spectrum of LDLR Activity. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 2248–2260. [Google Scholar] [CrossRef]
- Reeskamp, L.F.; Millar, J.S.; Wu, L.; Jansen, H.; van Harskamp, D.; Schierbeek, H.; Gipe, D.A.; Rader, D.J.; Dallinga-Thie, G.M.; Hovingh, G.K.; et al. ANGPTL3 Inhibition With Evinacumab Results in Faster Clearance of IDL and LDL apoB in Patients With Homozygous Familial Hypercholesterolemia-Brief Report. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1753–1759. [Google Scholar] [CrossRef]
- Reeskamp, L.F.; Nurmohamed, N.S.; Bom, M.J.; Planken, R.N.; Driessen, R.S.; van Diemen, P.A.; Luirink, I.K.; Groothoff, J.W.; Kuipers, I.M.; Knaapen, P.; et al. Marked plaque regression in homozygous familial hypercholesterolemia. Atherosclerosis 2021, 327, 13–17. [Google Scholar] [CrossRef]
- Jin, M.; Meng, F.; Yang, W.; Liang, L.; Wang, H.; Fu, Z. Efficacy and Safety of Evinacumab for the Treatment of Hypercholesterolemia: A Meta-Analysis. J. Cardiovasc. Pharmacol. 2021, 78, 394–402. [Google Scholar] [CrossRef]
- NCT04863014. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04863014 (accessed on 24 October 2022).
- NCT03409744. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03409744 (accessed on 24 October 2022).
- NCT04233918. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04233918 (accessed on 24 October 2022).
- Banach, M.; Burchardt, P.; Chlebus, K.; Dobrowolski, P.; Dudek, D.; Dyrbuś, K.; Gąsior, M.; Jankowski, P.; Jóźwiak, J.; Kłosiewicz-Latoszek, L.; et al. PoLA/CFPiP/PCS/PSLD/PSD/PSH guidelines on diagnosis and therapy of lipid disorders in Poland 2021. Arch. Med. Sci. 2021, 17, 1447–1547. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Catapano, A.L. Evinacumab: A new option in the treatment of homozygous familial hypercholesterolemia. Expert Opin. Biol. Ther. 2022, 22, 813–820. [Google Scholar] [CrossRef]
- Banach, M.; Surma, S.; Reiner, Z.; Katsiki, N.; Penson, P.E.; Fras, Z.; Sahebkar, A.; Paneni, F.; Rizzo, M.; Kastelein, J. Personalized Management of Dyslipidemias in Patients with Diabetes—It Is Time for a New Approach (2022). Cardiovasc. Diabetol. 2022, 21, 263. [Google Scholar] [CrossRef] [PubMed]
- Surma, S.; Romańczyk, M.; Filipiak, K.J. Evinacumab—A new drug in the treatment of severe lipid disorders. Up-to-date review of the literature and clinical studies. Kardiol. Inwaz. 2022, 17, 8–18. [Google Scholar]
- Deng, M.; Kutrolli, E.; Sadewasser, A.; Michel, S.; Joibari, M.M.; Jaschinski, F.; Olivecrona, G.; Nilsson, S.K.; Kersten, S. ANGPTL4 silencing via antisense oligonucleotides reduces plasma triglycerides and glucose in mice without causing lymphadenopathy. J. Lipid Res. 2022, 63, 100237. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; López-Sendon, J.L.; Averna, M.; Cariou, B.; Loy, M.; Manvelian, G.; Batsu, I.; Poulouin, Y.; Gaudet, D. Treatment adherence and effect of concurrent statin intensity on the efficacy and safety of alirocumab in a real-life setting: Results from ODYSSEY APPRISE. Arch. Med. Sci. 2021, 18, 285–292. [Google Scholar] [CrossRef]
- Momtazi-Borojeni, A.A.; Jaafari, M.R.; Afshar, M.; Banach, M.; Sahebkar, A. PCSK9 immunization using nanoliposomes: Preventive efficacy against hypercholesterolemia and atherosclerosis. Arch. Med. Sci. 2021, 17, 1365–1377. [Google Scholar] [CrossRef]
- Banach, M.; Kaźmierczak, J.; Mitkowski, P.; Wita, K.; Broncel, M.; Gąsior, M.; Gierlotka, M.; Gil, R.; Jankowski, P.; Niewada, M.; et al. Which patients at risk of cardiovascular disease might benefit the most from inclisiran? Polish experts’ opinion. The compromise between EBM and possibilities in healthcare. Arch. Med. Sci. 2022, 18, 569–576. [Google Scholar] [CrossRef]
- Gupta, S. LDL cholesterol, statins and PCSK 9 inhibitors. Indian Heart J. 2015, 67, 419–424. [Google Scholar] [CrossRef] [Green Version]
- D’Erasmo, L.; Gallo, A.; Cefalù, A.B.; Di Costanzo, A.; Saheb, S.; Giammanco, A.; Averna, M.; Buonaiuto, A.; Iannuzzo, G.; Fortunato, G.; et al. Long-term efficacy of lipoprotein apheresis and lomitapide in the treatment of homozygous familial hypercholesterolemia (HoFH): A cross-national retrospective survey. Orphanet J. Rare Dis. 2021, 16, 381. [Google Scholar] [CrossRef]
- D’Erasmo, L.; Steward, K.; Cefalù, A.B.; Di Costanzo, A.; Boersma, E.; Bini, S.; Arca, M.; van Lennep, J.R. Italian and European Working Group on Lomitapide in HoFH. Efficacy and safety of lomitapide in homozygous familial hypercholesterolaemia: The pan-European retrospective observational study. Eur. J. Prev. Cardiol. 2022, 29, 832–841, Erratum in Eur. J. Prev. Cardiol. 2022, 29, 1812. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, B.M. Evinacumab Approval Adds a New Option for Homozygous Familial Hypercholesterolemia with a Hefty Price Tag. Circulation 2021, 143, 2494–2496. [Google Scholar] [CrossRef] [PubMed]
- Kosmas, C.E.; Bousvarou, M.D.; Sourlas, A.; Papakonstantinou, E.J.; Peña Genao, E.; Echavarria Uceta, R.; Guzman, E. Angiopoietin-Like Protein 3 (ANGPTL3) Inhibitors in the Management of Refractory Hypercholesterolemia. Clin. Pharmacol. 2022, 14, 49–59. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Phase/Status | NCT Identification Number | Population/N | Duration | Dose/Treatment Arms | Key Results | Safety | Ref. |
|---|---|---|---|---|---|---|---|
| Phase 1 Completed | NCT01749878 | HTG Cohort A: 150 < TG ≤ 450 mg/dL or LDL-C ≥ 100 mg/dL N = 83 Cohort B: 450 ≤ TG < 1500 mg/dL N = 7 Cohort C: LPL pathway sequence variations, TG > 1000 mg/dL N = 9 | 126 days | Single dose: Cohort A: 75, 150, 250 mg SC or 5, 10, 20 mg/kg IV vs. placebo Cohort B: 10 mg/kg IV vs. placebo Cohort C: 250 mg SC or 20 mg/kg IV vs. placebo | Max reduction: Cohort A: At a dose of 20 mg/kg IV TG: 76.0% LDL-C: 23.2% HDL: 18.4% Cohort B TG: 81.8% VLDL-C: 82.2% Cohort C TG: 0.9 to 93.2%, VLDL-C: 64.9% (IV 20 mg/kg), 37.8% (SC 250 mg) | TEAEs Cohort A 51.6% vs. 42.9% placebo Cohorts B and C 100% vs. 81.8% placebo Frequent AE (cohort A): headache (11% vs. 0% placebo), upper respiratory tract infection (6.5% vs. 4.0% placebo), increased alanine aminotransferase (11.3% vs. 0% placebo), increased aspartate aminotransferase (4.8% vs. 0% placebo) | [18,25,26] |
| Phase 1 Completed | NCT02107872 | HTG: 150< TG ≤500 mg/dL and LDL-C ≥ 100 mg/dL N = 56 | 183 days | Multiple doses: SC: 150, 300, 450 mg QW or 300, 450 mg Q2W IV: 20 mg/kg Q4W up to day 56 vs. placebo | Max reduction at IV 20 mg/kg Q4W TG: 88.2% (day 2) non-HDL: 45.8% (day 36) apoB: 30.7% (day 57) LDL-C: 25.1% (day 57) total cholesterol: 33.8% (day 57) | TEAEs SC: 51.6% vs. 42.9% placebo IV: 85.7% vs. 50% placebo Common AE: SC: nausea (13% vs. 0% placebo) IV: headache (42.9% vs. 0% placebo); No SAE | [26] |
| Phase 2 Completed | NCT02265952 | HoFH N = 9 | 26 weeks | Two doses: 250 mg SC on day 1 and 15 mg/kg IV on week 2 | Max reduction (week 4): LDL-C: 49 ± 23% non-HDL-C: 49 ± 22% TG: 47 ± 17% apo B: 46 ± 18% HDL-C: 36 ± 16% | TEAEs: Injection-site reactions (11%), myalgia (11%), hot flush (11%), epistaxis (11%); No SAE | [27,28] |
| Phase 1 Completed | NCT03146416 | Healthy Japanese and Caucasian N = 96 | 24 weeks | Cohorts: I: single dose of 300 mg (SC) II: 300 mg (SC) QW for eight doses III: 5 mg/kg (IV) IV: 15 mg/kg (IV) Q4W for two doses vs. placebo | Max reduction, 15 mg/kg (IV) Q4W for two doses (week 8): LDL: 40.2% TG: 63.1% non-HDL: 44.2% HDL: 23.8% total cholesterol: 40.2% apoB: 37.4% apoA-I: 33.5% apoC-III: 77.1% Lp(a): 22.2% | TEAEs SC: 52.8% vs. 25.0% placebo IV: 41.7% vs. 50% placebo Common TEAEs: nausea, fatigue, nasopharyngitis, upper respiratory infection, rhinitis, back pain, headache, tension headache; No SAE | [4] |
| Phase 2 Completed | NCT03175367 | Hypercholesterolemia: HeFH or non-HeFH with ASCVD ASCVD: LDL-C ≥ 70 mg/dL or non-ASCVD: LDL-C ≥ 100 mg/dL N = 272 | 16 weeks | SC: 450 mg QW, 300 mg QW, or 300 mg Q2W vs. placebo; IV: 15 mg/kg Q4W or 5 mg/kg Q4W vs. placebo | LDL-C reduction: SC: 38.5% to 56.0%, IV: 24.2% to 50.5% | SC AE: 68–82% vs. 54% placebo; urinary tract infection (11% vs. 8%), injection-site erythema (6% vs. 3%), arthralgia (5% vs. 3%), myalgia (5% vs. 0%) SAE: 5–8% vs. 8% IV AE: 75–84% vs. 70% placebo; abdominal pain (6% vs. 0%), back pain (7% vs. 6%), dizziness (7% vs. 0%), fatigue (7% vs. 6%), pain in an arm or leg (7% vs. 6%), nausea (7% vs. 0%), and nasopharyngitis (12% vs. 6%); SAE: 6–16% vs. 3% | [5] |
| Phase 2 Completed | NCT03452228 | sHTG, TG values ≥ 500 mg/dL (5.6 mmol/L) N = 52 | 24 weeks | Evinacumab IV vs. placebo | NA | NA | |
| Phase 3 Completed | NCT03399786 | HoFH LDL-C ≥ 70 mg/dL (1.8 mmol/L) N = 65 | 24 weeks | Evinacumab IV 15 mg/kg Q4W vs. placebo | Reduction: LDL-C: 47.1%, total cholesterol: 47.4%, non-HDL: 49.7%, HDL: 29.6%, TG: 55.0%, apoB: 41.4%, apoC-III: 84.1% Lp(a): 5.5% | AE: 66% vs. 81% placebo, SAE: 5% vs. 0 placebo | [3] |
| Kinetics test | NCT04722068 | HoFH N = 4 | 8 weeks | Evinacumab IV 15 mg/kg | Decrease: LDL-C: 59 ± 2%, Increase: IDL-ApoB: 616 ± 504%, LDL-ApoB: 113 ± 14%, | NA | [29] |
| Phase 3 Ongoing | NCT03409744 | HoFH, adolescent subjects (≥12 years) N = 116 | 192 weeks | Evinacumab IV | Study completion date: January 2023 | [23] | |
| Phase 3 Ongoing | NCT04233918 | HoFH, pediatric subjects (5–11 years), LDL-C > 130 mg/dL N = 20 | 24 weeks | Part A: single IV dose; Part B: IV dose Q4W until week 20; Part C: IV dose Q4W | Study completion date: May 2023 | [23] | |
| Phase 2 Ongoing | NCT04863014 | sHTG, adult subjects (18–80 years) TG > 880 mg/dL (10 mmol/L) or >500 mg/dL (5.6 mmol/L); N = 21 | 52 weeks | IV Q4W vs. placebo | Study completion date: February 2023 | [23] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sosnowska, B.; Adach, W.; Surma, S.; Rosenson, R.S.; Banach, M. Evinacumab, an ANGPTL3 Inhibitor, in the Treatment of Dyslipidemia. J. Clin. Med. 2023, 12, 168. https://doi.org/10.3390/jcm12010168
Sosnowska B, Adach W, Surma S, Rosenson RS, Banach M. Evinacumab, an ANGPTL3 Inhibitor, in the Treatment of Dyslipidemia. Journal of Clinical Medicine. 2023; 12(1):168. https://doi.org/10.3390/jcm12010168
Chicago/Turabian StyleSosnowska, Bożena, Weronika Adach, Stanisław Surma, Robert S. Rosenson, and Maciej Banach. 2023. "Evinacumab, an ANGPTL3 Inhibitor, in the Treatment of Dyslipidemia" Journal of Clinical Medicine 12, no. 1: 168. https://doi.org/10.3390/jcm12010168
APA StyleSosnowska, B., Adach, W., Surma, S., Rosenson, R. S., & Banach, M. (2023). Evinacumab, an ANGPTL3 Inhibitor, in the Treatment of Dyslipidemia. Journal of Clinical Medicine, 12(1), 168. https://doi.org/10.3390/jcm12010168