
Cardiopulmonary Profiling of Athletes with Post-Exertional Malaise after COVID-19 Infection—A Single-Center Experience

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
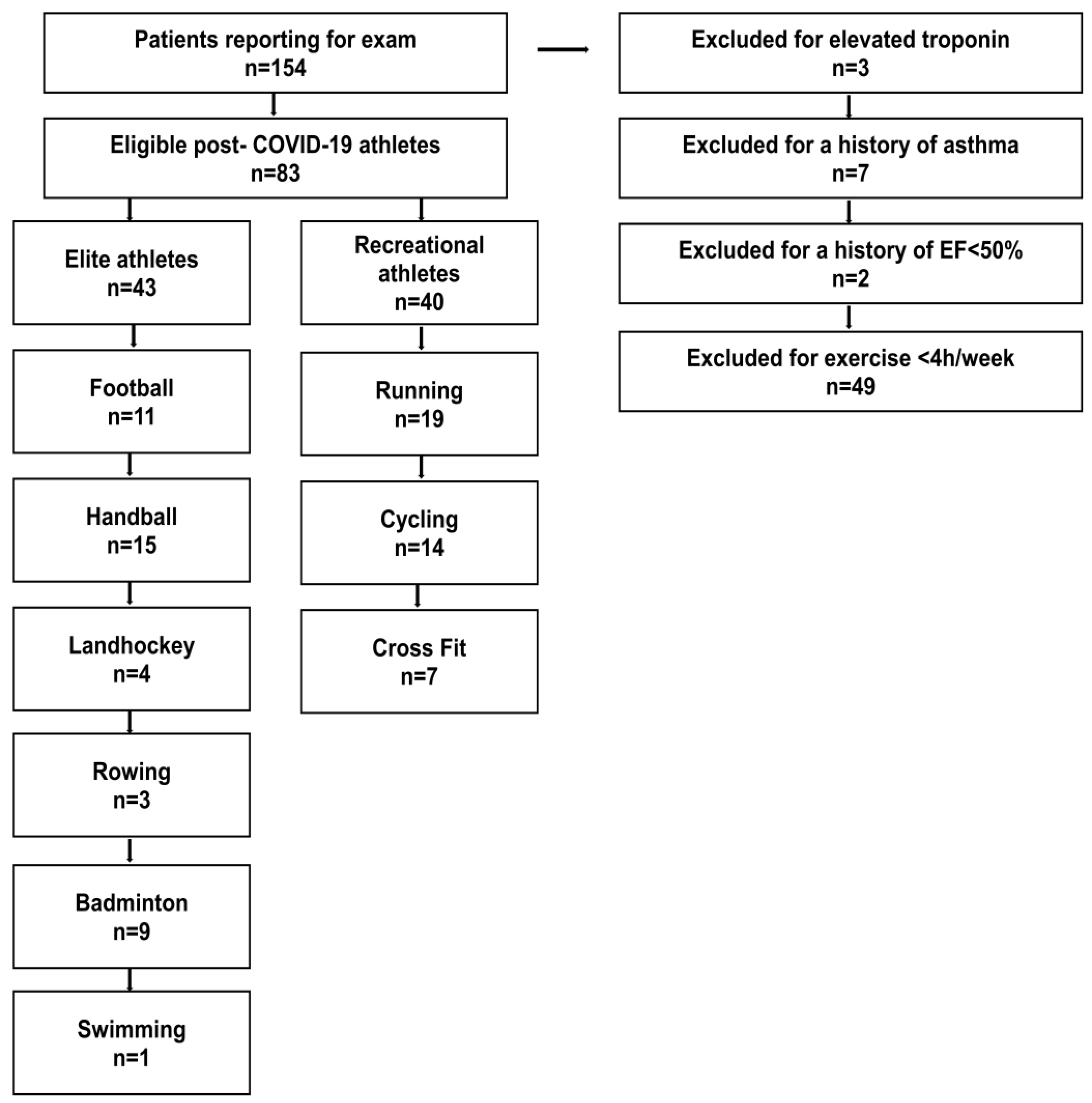
2.1. Setting and Participants
2.2. Cardiopulmonary Exercise Protocol
2.3. Statistical Methods
3. Results
3.1. Baseline Characteristics
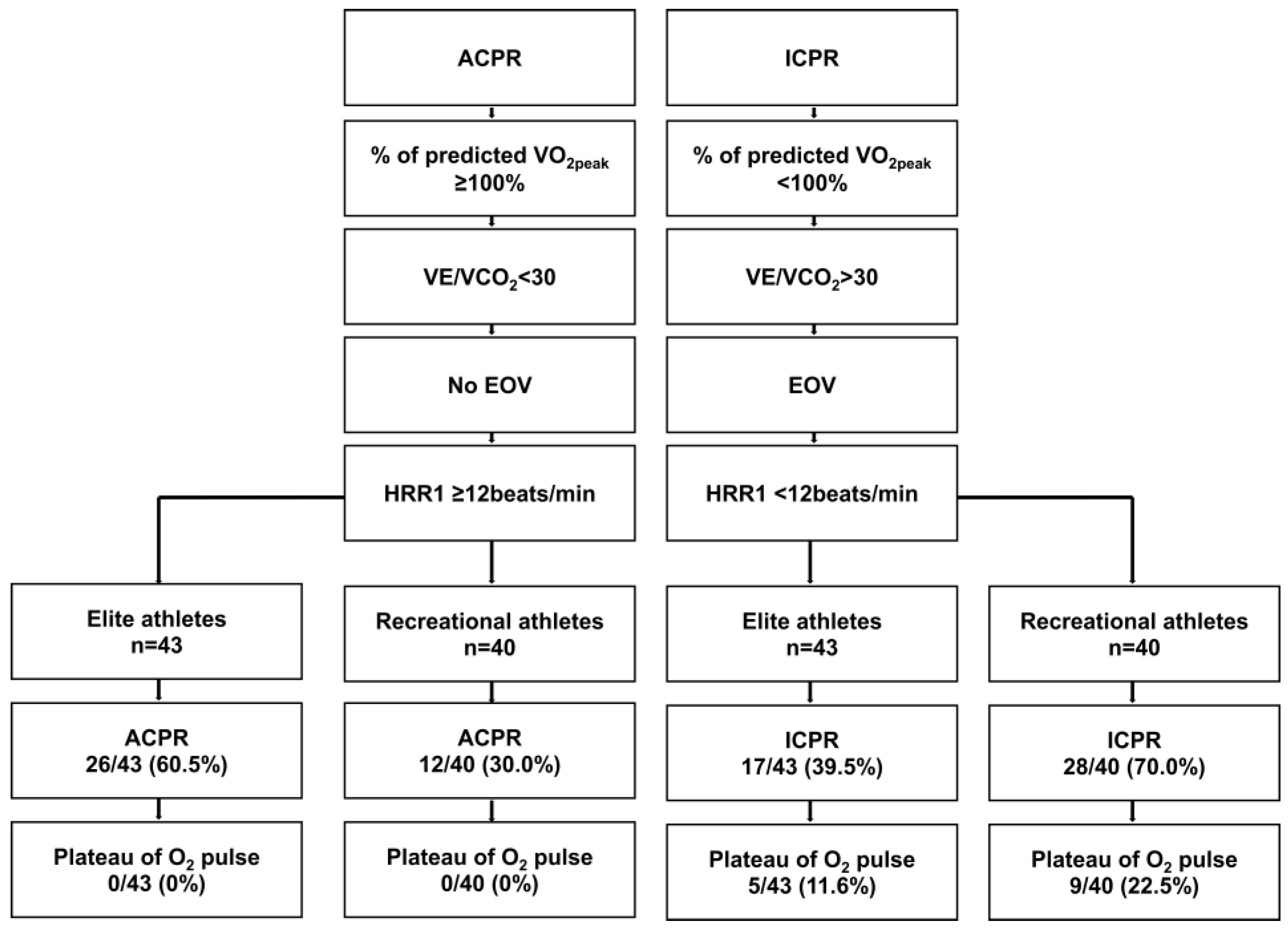
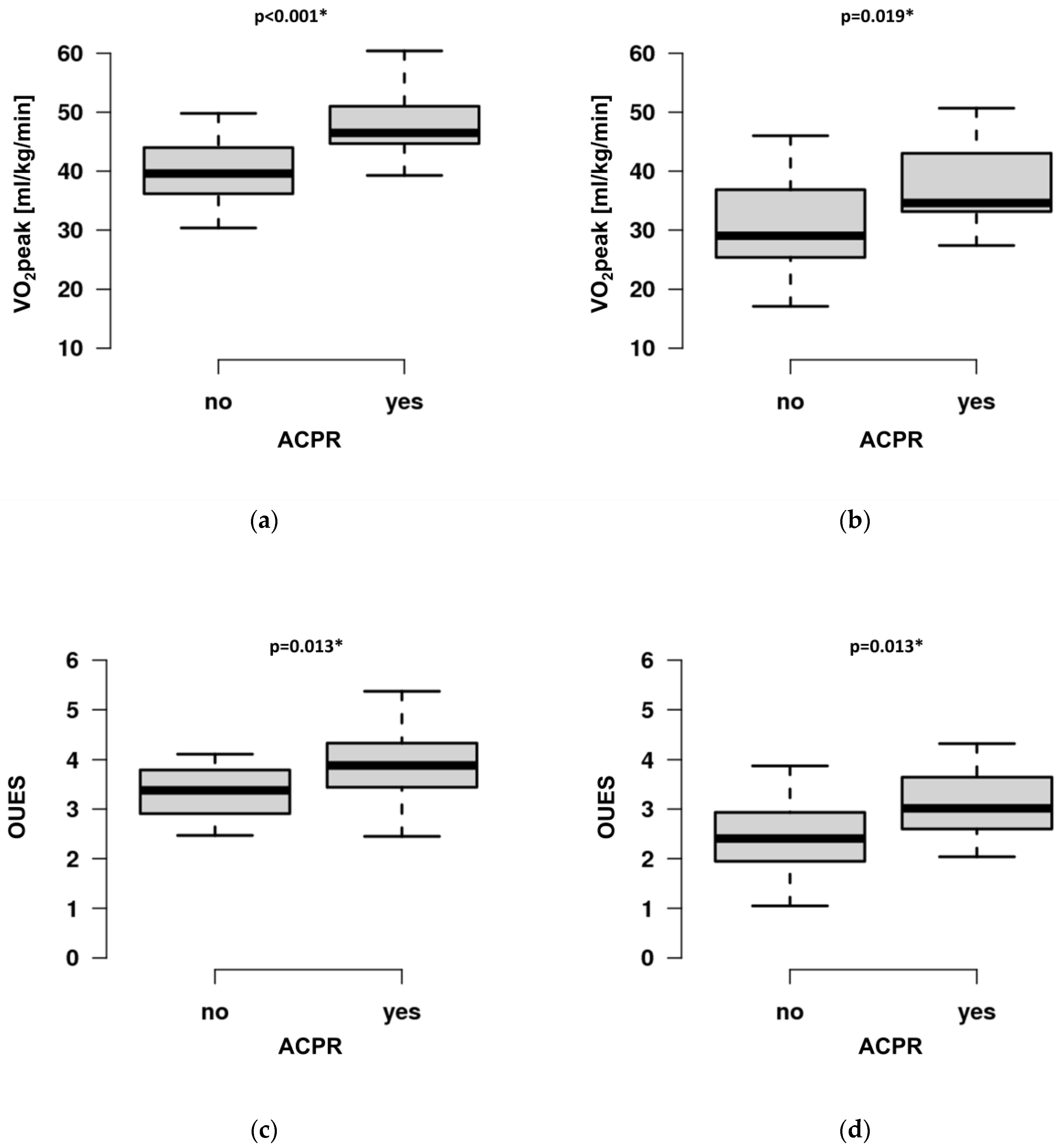
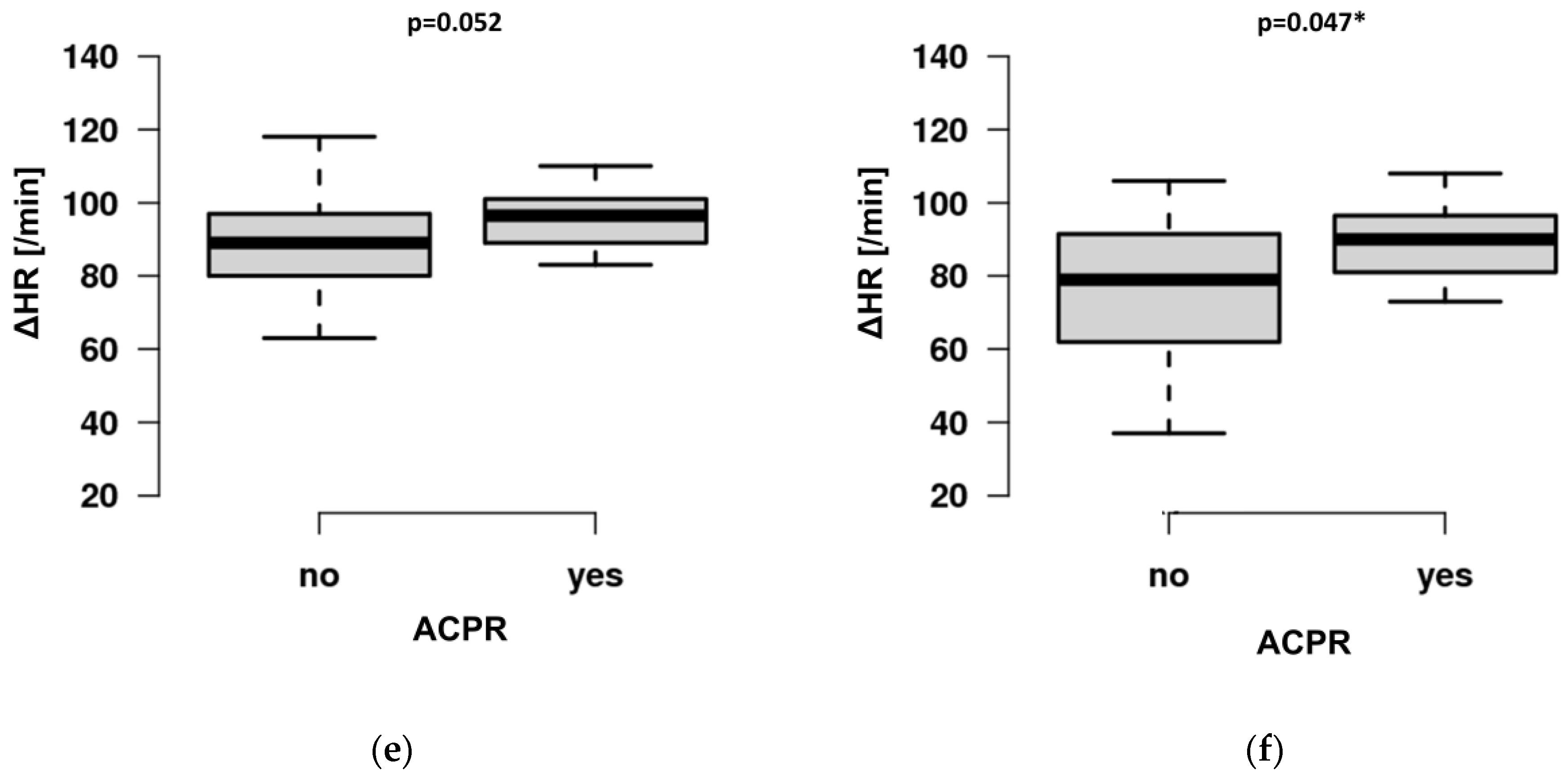
3.2. CPET Outcome Variables
4. Discussion
4.1. CPET Performance of Athletes with PEM
4.2. The Benefit of CPET in Athletes with PEM
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Estimate | Standard Error | R2 | p-Value |
|---|---|---|---|---|
| VO2peak Intercept Sports category ACPR Age | 47.409 −6.009 6.873 −0.310 | 1.979 1.619 1.367 0.070 | R2 = 0.614 | p < 0.001 * p = 0.001 * p < 0.001 * p < 0.001 * |
| OUES Intercept Sports category ACPR Age Female | 3.611 −0.388 0.748 −0.014 −0.750 | 0.190 0.167 0.137 0.007 0.152 | R2 = 0.581 | p < 0.001 * p = 0.023 * p < 0.001 * p = 0.045 * p < 0.001 * |
| ΔHR Intercept ACPR Age | 101.052 10.943 −0.0667 | 5.113 3.436 0.1518 | R2 = 0.296 | p < 0.001 * p = 0.002 * p < 0.001 * |
References
- Jennifer, K.; Shirley, S.B.D.; Avi, P.; Daniella, R.C.; Naama, S.S.; Anat, E.Z.; Miri, M.R. Post-acute sequelae of COVID-19 infection. Prev. Med. Rep. 2023, 31, 102097. [Google Scholar] [CrossRef]
- Wilson, M.G.; Hull, J.H.; Rogers, J.; Pollock, N.; Dodd, M.; Haines, J.; Harris, S.; Loosemore, M.; Malhotra, A.; Pieles, G.; et al. Cardiorespiratory considerations for return-to-play in elite athletes after COVID-19 infection: A practical guide for sport and exercise medicine physicians. Br. J. Sport. Med. 2020, 54, 1157–1161. [Google Scholar] [CrossRef]
- Evers, G.; Schulze, A.B.; Osiaevi, I.; Harmening, K.; Vollenberg, R.; Wiewrodt, R.; Pistulli, R.; Boentert, M.; Tepasse, P.R.; Sindermann, J.R.; et al. Sustained Impairment in Cardiopulmonary Exercise Capacity Testing in Patients after COVID-19: A Single Center Experience. Can. Respir. J. 2022, 2022, 2466789. [Google Scholar] [CrossRef]
- Skjørten, I.; Ankerstjerne, O.A.W.; Trebinjac, D.; Brønstad, E.; Rasch-Halvorsen, Ø.; Einvik, G.; Lerum, T.V.; Stavem, K.; Edvardsen, A.; Ingul, C.B. Cardiopulmonary exercise capacity and limitations 3 months after COVID-19 hospitalisation. Eur. Respir. J. 2021, 58, 2100996. [Google Scholar] [CrossRef]
- Baratto, C.; Caravita, S.; Faini, A.; Perego, G.B.; Senni, M.; Badano, L.P.; Parati, G. Impact of COVID-19 on exercise pathophysiology: A combined cardiopulmonary and echocardiographic exercise study. J. Appl. Physiol. 2021, 130, 1470–1478. [Google Scholar] [CrossRef]
- Lemos, M.M.; Cavalini, G.R.; Pugliese Henrique, C.R.; Perli, V.A.S.; de Moraes Marchiori, G.; Marchiori, L.L.M.; Sordi, A.F.; Franzói de Moraes, S.M.; de Paula Ramos, S.; Valdés-Badilla, P.; et al. Body composition and cardiorespiratory fitness in overweight or obese people post COVID-19: A comparative study. Front. Physiol. 2022, 13, 949351. [Google Scholar] [CrossRef]
- Silva, F.B.D.; Fonseca, B.; Domecg, F.; Facio, M.R.; Prado, C.; Toledo, L.; Tuche, W. Athletes health during pandemic times: Hospitalization rates and variables related to COVID-19 prevalence among endurance athletes. Int. J. Cardiovasc. Sci. 2021, 3, 274–283. [Google Scholar] [CrossRef]
- Śliż, D.; Wiecha, S.; Gąsior, J.S.; Kasiak, P.S.; Ulaszewska, K.; Lewandowski, M.; Barylski, M.; Mamcarz, A. Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes-CAESAR Study. J. Clin. Med. 2023, 12, 3002. [Google Scholar] [CrossRef]
- Deng, M.C. An exercise immune fitness test to unravel mechanisms of Post-Acute Sequelae of COVID-19. Expert Rev. Clin. Immunol. 2023, 1–5. [Google Scholar] [CrossRef]
- Buonsenso, D.; Di Giuda, D.; Sigfrid, L.; Pizzuto, D.A.; Di Sante, G.; De Rose, C.; Lazzareschi, I.; Sali, M.; Baldi, F.; Chieffo, D.P.R.; et al. Evidence of lung perfusion defects and ongoing inflammation in an adolescent with post-acute sequelae of SARS-CoV-2 infection. Lancet Child Adolesc. Health 2021, 5, 677–680. [Google Scholar] [CrossRef]
- Twomey, R.; DeMars, J.; Franklin, K.; Culos-Reed, S.N.; Weatherald, J.; Wrightson, J.G. Chronic Fatigue and Postexertional Malaise in People Living with Long COVID: An Observational Study. Phys. Ther. 2022, 102, 1–12. [Google Scholar] [CrossRef]
- Chu, L.; Valencia, I.J.; Garvert, D.W.; Montoya, J.G. Deconstructing post-exertional malaise in myalgic encephalomyelitis/chronic fatigue syndrome: A patient-centered, cross-sectional survey. PLoS ONE 2018, 13, e0197811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotler, J.; Holtzman, C.; Dudun, C.; Jason, L.A. A Brief Questionnaire to Assess Post-Exertional Malaise. Diagnostics 2018, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- NINDS Common Data Elements (CDE) Group Post-Exertional Malaise Subgroup Summary. Myalgic Encephalomyelitis/Chronicfatiguesyndrome. Available online: https://www.commondataelements.ninds.nih.gov/sites/nindscde/files/Doc/MECFS/PEM_Subgroup_Summary.pdf (accessed on 13 June 2023).
- Phelan, D.; Kim, J.H.; Elliott, M.D.; Wasfy, M.M.; Cremer, P.; Johri, A.M.; Emery, M.S.; Sengupta, P.P.; Sharma, S.; Martinez, M.W.; et al. Screening of Potential Cardiac Involvement in Competitive Athletes Recovering From COVID-19: An Expert Consensus Statement. JACC Cardiovasc. Imaging 2020, 13, 2635–2652. [Google Scholar] [CrossRef] [PubMed]
- Symanski, J.D.; Tso, J.V.; Phelan, D.M.; Kim, J.H. Myocarditis in the Athlete: A Focus on COVID-19 Sequelae. Clin. Sport. Med. 2022, 41, 455–472. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 focused update: Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur. Heart J. 2018, 39, 1144–1161. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- McKinney, J.; Velghe, J.; Fee, J.; Isserow, S.; Drezner, J.A. Defining Athletes and Exercisers. Am. J. Cardiol. 2019, 123, 532–535. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef] [Green Version]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, J.E.; Sue, D.Y.; Wasserman, K. Predicted values for clinical exercise testing. Am. Rev. Respir. Dis. 1984, 129, S49–S55. [Google Scholar] [CrossRef] [PubMed]
- Kremser, C.B.; O’Toole, M.F.; Leff, A.R. Oscillatory hyperventilation in severe congestive heart failure secondary to idiopathic dilated cardiomyopathy or to ischemic cardiomyopathy. Am. J. Cardiol. 1987, 59, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Araújo, C.G.S.; Kurl, S.; Khan, H.; Jae, S.Y.; Guazzi, M.; Kunutsor, S.K. Relative peak exercise oxygen pulse is related to sudden cardiac death, cardiovascular and all-cause mortality in middle-aged men. Eur. J. Prev. Cardiol. 2018, 25, 772–782. [Google Scholar] [CrossRef]
- Laukkanen, J.A.; Savonen, K.; Hupin, D.; Araújo, C.G.S.; Kunutsor, S.K. Cardiorespiratory optimal point during exercise testing and sudden cardiac death: A prospective cohort study. Prog. Cardiovasc. Dis. 2021, 68, 12–18. [Google Scholar] [CrossRef]
- Baba, R.; Nagashima, M.; Goto, M.; Nagano, Y.; Yokota, M.; Tauchi, N.; Nishibata, K. Oxygen uptake efficiency slope: A new index of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. J. Am. Coll. Cardiol. 1996, 28, 1567–1572. [Google Scholar] [CrossRef]
- Bhatia, R.; Cohen, B.H.; McNinch, L.N. A novel exercise testing algorithm to diagnose mitochondrial myopathy. Muscle Nerve 2021, 63, 715–723. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Guazzi, M. The clinical and research applications of aerobic capacity and ventilatory efficiency in heart failure: An evidence-based review. Heart Fail. Rev. 2008, 13, 245–269. [Google Scholar] [CrossRef]
- A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 22 April 2022).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdalde, NJ, USA, 1988. [Google Scholar]
- Gluckman, T.J.; Bhave, N.M.; Allen, L.A.; Chung, E.H.; Spatz, E.S.; Ammirati, E.; Baggish, A.L.; Bozkurt, B.; Cornwell, W.K., 3rd; Harmon, K.G.; et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 79, 1717–1756. [Google Scholar] [CrossRef]
- Halle, M.; Bloch, W.; Niess, A.M.; Predel, H.G.; Reinsberger, C.; Scharhag, J.; Steinacker, J.; Wolfarth, B.; Scherr, J.; Niebauer, J. Exercise and sports after COVID-19-Guidance from a clinical perspective. Transl. Sport Med. 2021, 4, 310–318. [Google Scholar] [CrossRef]
- Hu, Y.F.; Chen, Y.J.; Lin, Y.J.; Chen, S.A. Inflammation and the pathogenesis of atrial fibrillation. Nat. Rev. Cardiol. 2015, 12, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.D.; Talwar, A.; Lee, J.T. A Proposed Framework and Timeline of the Spectrum of Disease Due to SARS-CoV-2 Infection: Illness Beyond Acute Infection and Public Health Implications. JAMA 2020, 324, 2251–2252. [Google Scholar] [CrossRef] [PubMed]
- Milovancev, A.; Avakumovic, J.; Lakicevic, N.; Stajer, V.; Korovljev, D.; Todorovic, N.; Bianco, A.; Maksimovic, N.; Ostojic, S.; Drid, P. Cardiorespiratory Fitness in Volleyball Athletes Following a COVID-19 Infection: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4059. [Google Scholar] [CrossRef]
- Ganesananthan, S.; Rajkumar, C.A.; Foley, M.; Thompson, D.; Nowbar, A.N.; Seligman, H.; Petraco, R.; Sen, S.; Nijjer, S.; Thom, S.A.; et al. Cardiopulmonary exercise testing and efficacy of percutaneous coronary intervention: A substudy of the ORBITA trial. Eur. Heart J. 2022, 43, 3132–3145. [Google Scholar] [CrossRef] [PubMed]
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sánchez-Alcaraz Martínez, B.J.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-COVID-19 Syndrome and the Potential Benefits of Exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Faghy, M.A.; Ashton, R.E.M.; Parizher, G.; Smith, A.; Arena, R.; Gough, L.A.; Emery, M.S. COVID-19 and elite sport: Cardiovascular implications and return-to-play. Prog. Cardiovasc. Dis. 2022, 76, 61–68. [Google Scholar] [CrossRef]
- Malhotra, R.; Bakken, K.; D’Elia, E.; Lewis, G.D. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail. 2016, 4, 607–616. [Google Scholar] [CrossRef]
- Samper-Pardo, M.; León-Herrera, S.; Oliván-Blázquez, B.; Gascón-Santos, S.; Sánchez-Recio, R. Clinical characterization and factors associated with quality of life in Long COVID patients: Secondary data analysis from a randomized clinical trial. PLoS ONE 2023, 18, e0278728. [Google Scholar] [CrossRef]
- Hausswirth, C.; Schmit, C.; Rougier, Y.; Coste, A. Positive Impacts of a Four-Week Neuro-Meditation Program on Cognitive Function in Post-Acute Sequelae of COVID-19 Patients: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1361. [Google Scholar] [CrossRef]




| Medical History | Elite (n = 43) | Recreational (n = 40) | p-Value |
|---|---|---|---|
| Age (years) | 21.9 ± 3.7 | 34.7 ± 13.0 | p < 0.001 * |
| BMI (kg/m2) | 23.7 ± 2.2 | 24.3 ± 3.7 | p = 0.716 |
| Women (%) | 14.0 (6/43) | 47.5 (19/40) | p = 0.001 * |
| Patients vaccinated (%) | 42 | 37 | p = 0.845 |
| Vaccinations received | 2.5 ± 0.4 | 2.2 ± 0.5 | p = 0.345 |
| Time since last vaccination (months) | 3.4 ± 2.1 | 2.8 ± 1.9 | p = 0.324 |
| NTproBNP (pg/mL) | 44.6 ± 0.25.1 | 50.2 ± 38.4 | p = 0.481 |
| Hemoglobin (g/dL) | 15.1 ± 1.0 | 14.3 ± 1.2 | p < 0.001 * |
| Troponin (ng/L) a | 4.8 ± 5.7 | 3.4 ± 1.7 | p = 0.008 * |
| D-Dimer (mg/L) | 0.3 ± 0.1 | 0.3 ± 0.2 | p = 0.268 |
| Ferritin (mg/L) | 90.0 ± 54.2 | 81.0 ± 50.6 | p = 0.581 |
| CRP (mg/dL) | 0.3 ± 0.1 | 0.2 ± 0.1 | p < 0.001 * |
| LVEF (%) | 59.6 ± 4.8 | 59.2 ± 4.6 | p = 0.330 |
| LAVI (mL/m2) | 28.3 ± 9.2 | 24.5 ± 5.6 | p = 0.073 |
| LVMI (g/m2) | 93.5 ± 18.9 | 81.0 ± 25.4 | p = 0.001 * |
| LVEDD (mm) | 51.6 ± 5.1 | 49.1 ± 5.0 | p = 0.024 * |
| TAPSE (mm) | 25.9 ± 3.9 | 25.6 ± 4.3 | p = 0.945 |
| sPAP (mmHg) | 17.3 ± 5.4 | 17.6 ± 5.4 | p = 0.434 |
| RV basal (mm) | 38.6 ± 4.5 | 33.5 ± 6.1 | p < 0.001 * |
| RV mid (mm) | 29.3 ± 4.8 | 25.6 ± 6.0 | p = 0.002 * |
| CPET Variables | Elite (n = 43) | Recreational (n = 40) | p-Value |
|---|---|---|---|
| HRmin (beats/min) | 84.4 ± 14.3 | 93.0 ± 16.9 | p = 0.025 * |
| HRmax (beats/min) | 180.2 ± 12.5 | 172.3 ± 17.1 | p = 0.028 * |
| HRR1 (beats/min) | 28.5 ± 7.7 | 28.7 ± 14.1 | p = 0.587 |
| RRsysmax (mmHg) | 194.1 ± 30.4 | 179.5 ± 27.3 | p = 0.047 * |
| RRdiamax (mmHg) | 90.0 ± 16.8 | 89.6 ± 14.4 | p = 0.906 |
| P max (W) | 302.9 ± 45.5 | 204.6 ± 59.3 | p < 0.001 * |
| VO2peak (mL/kg/min) | 44.8 ± 6.8 | 32.7 ± 7.9 | p < 0.001 * |
| % of VO2pred | 107.4 ± 17.7 | 101.3 ± 24.5 | p = 0.204 |
| VE (L) | 117.9 ± 26.5 | 93.4 ± 24.4 | p < 0.001 * |
| VE/VCO2 | 24.5 ± 2.4 | 28.4 ± 5.4 | p < 0.001 * |
| BR (%) | 23.7 ± 17.5 | 26.3 ± 16.6 | p = 0.542 |
| Plateau of O2 pulse (%) | 11.6 (5/43) | 22.5 (9/40) | p = 0.152 |
| O2 pulserest (mL/beat/kg × 100) | 10.4 ± 2.2 | 9.2 ± 2.7 | p = 0.012 * |
| O2 pulsemax (mL/beat/kg × 100) | 24.2 ± 3.9 | 18.6 ± 4.4 | p < 0.001 * |
| ΔO2pulse | 13.8 ± 4.0 | 9.4 ± 3.4 | p < 0.001 * |
| O2 pulse25 (mL/beat/kg × 100) | 16.5 ± 3.3 | 13.4 ± 3.2 | p < 0.001 * |
| O2 pulse50 (mL/beat/kg × 100) | 20.5 ± 3.8 | 16.4 ± 4.0 | p < 0.001 * |
| O2 pulse75 (mL/beat/kg × 100) | 22.8 ± 4.1 | 18.1 ± 4.1 | p < 0.001 * |
| EqO2 at VT1 | 19.0 ± 2.3 | 21.1 ± 2.7 | p < 0.001 * |
| OUES | 3.7 ± 0.7 | 2.6 ± 0.7 | p < 0.001 * |
| EOV | 14.0 (6/43) | 22.5 (9/40) | p = 0.234 |
| ACPR ≥100% of predVO2peak VE/VCO2 < 30 No EOV HRR1≥ 12 beats/min | 26/43 (60.5%) 29/43 (67.4%) 42/43 (97.7%) 37/43 (86.0%) 43/43 (100.0%) | 12/40 (30.0%) 20/40 (50%) 26/40 (65%) 31/40 (77.5%) 37/40 (92.5%) | p = 0.005 * p = 0.082 p < 0.001 * p = 0.234 p = 0.108 |
| CPET Variables | ACPR (n = 43) | ICPR (n = 40) | P-Value |
|---|---|---|---|
| HRmin (beats/min) | 84.3 ± 13.7 | 93.1 ± 16.8 | p = 0.017 * |
| HRmax (beats/min) | 179.2 ± 11.3 | 174.0 ± 17.9 | p = 0.320 |
| RRsysmax (mmHg) | 194.9 ± 30.9 | 180.4 ± 27.2 | p = 0.046 * |
| RRdiamax (mmHg) | 87.0 ± 15.5 | 92.2 ± 15.5 | p = 0.179 |
| Pmax (W) | 291.8 ± 64.7 | 224.8 ± 63.4 | p < 0.001 * |
| VO2peak (mL/kg/min) | 44.4 ± 8.0 | 34.3 ± 8.2 | p < 0.001 * |
| VE (L) | 117.6 ± 31.8 | 96.3 ± 22.6 | p = 0.004 * |
| BR (%) | 23.6 ± 15.6 | 26.1 ± 18.2 | p = 0.567 |
| O2 pulserest (mL/beat/kg × 100) | 10.4 ± 2.5 | 9.4 ± 2.5 | p < 0.001 * |
| O2 pulsemax (mL/beat/kg × 100) | 24.2 ± 4.3 | 19.2 ± 4.4 | p < 0.001 * |
| ΔO2pulse | 13.9 ± 4.2 | 9.8 ± 3.5 | p < 0.001 * |
| O2 pulse25 (mL/beat/kg × 100) | 16.5 ± 3.4 | 13.8 ± 3.3 | p < 0.001 * |
| O2 pulse50 (mL/beat/kg × 100) | 20.5 ± 4.1 | 16.9 ± 3.9 | p < 0.001 * |
| O2 pulse75 (mL/beat/kg × 100) | 23.0 ± 4.4 | 18.5 ± 4.0 | p < 0.001 * |
| EqO2 at VT1 | 19.6 ± 2.7 | 20.3 ± 2.7 | p = 0.221 |
| OUES | 3.6 ± 0.8 | 2.8 ± 0.8 | p < 0.001 * |
| CPET Variables | Female (n = 12) | Male (n = 33) | p-Value |
|---|---|---|---|
| HRmin (beats/min) | 97.3 ± 17.8 | 91.4 ± 16.0 | p = 0.292 |
| HRmax (beats/min) | 171.3 ± 24.5 | 176.0 ± 24.5 | p = 0.443 |
| RRsysmax (mmHg) | 170.7 ± 21.8 | 182.9 ± 21.8 | p = 0.175 |
| RRdiamax (mmHg) | 91.8 ± 9.6 | 91.7 ± 17.1 | p = 0.978 |
| Pmax (W) | 163.3 ± 42.4 | 249.3 ± 56.3 | p < 0.001 * |
| VO2peak (mL/kg/min) | 32.2 ± 7.4 | 35.8 ± 8.7 | p = 0.210 |
| VE (L) | 76.1 ± 18.9 | 104.5 ± 19.8 | p < 0.001 * |
| BR (%) | 22.4 ± 15.5 | 26.9 ± 18.8 | p = 0.460 |
| O2 pulserest (mL/beat/kg × 100) | 10.1 ± 3.0 | 9.3 ± 2.3 | p = 0.317 |
| O2 pulsemax (mL/beat/kg × 100) | 18.3 ± 5.0 | 19.8 ± 4.2 | p = 0.316 |
| ΔO2pulse | 8.2 ± 3.1 | 10.6 ± 3.7 | p = 0.056 |
| O2 pulse25 (mL/beat/kg × 100) | 13.9 ± 3.9 | 13.9 ± 3.1 | p = 0.983 |
| O2 pulse50 (mL/beat/kg × 100) | 16.4 ± 4.7 | 17.2 ± 3.7 | p = 0.547 |
| O2 pulse75 (mL/beat/kg × 100) | 18.2 ± 4.6 | 18.8 ± 3.8 | p = 0.637 |
| EqO2 at VT1 | 21.2 ± 2.8 | 19.8 ± 2.6 | p = 0.172 |
| OUES | 2.2 ± 0.7 | 3.0 ± 0.7 | p = 0.001 * |
| 10-Item DSQ-PEM | Elite (n = 43) | Recreational (n = 40) | p-Value |
|---|---|---|---|
| Diagnosed PEM (%) in scoring step 1 | 43 (100.0) | 40 (100.0) | p > 0.999 |
| Diagnosed PEM (%) in scoring step 2 | 43 (100.0) | 40 (100.0) | p > 0.999 |
| 1. Dead, heavy feeling after launching of exercise | 40 (93.0) | 35 (87.5) | p = 0.564 |
| 2. Soreness of fatigue the next day after non-strenuous, everyday activity | 28 (65.1) | 24 (60.0) | p = 0.346 |
| 3. Mentally tired after low effort | 31 (72.1) | 27 (67.5) | p = 0.397 |
| 4. A minimum amount of exercise leads to physical exhaustion | 39 (90.7) | 36 (90.0) | p = 0.897 |
| 5. A feeling of sickness after mild physical activity | 25 (58.1) | 21 (52.5) | p = 0.721 |
| 6. A lack of recovery within 2 h after exhausting activity | 43 (100.0) | 40 (100.0) | p > 0.999 |
| 7. A worsening of fatigue after minimal physical effort | 43 (100.0) | 40 (100.0) | p > 0.999 |
| 8. A worsening of fatigue after minimal mental effort | 43 (100.0) | 40 (100.0) | p > 0.999 |
| 9. Feeling worse after activities and persistence for at least 14 h | 43 (100.0) | 40 (100.0) | p > 0.999 |
| 10. Evading exercise, as it makes symptoms worse | 2 (4.7) | 3 (7.5) | p = 0.351 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wernhart, S.; Weihe, E.; Totzeck, M.; Balcer, B.; Rassaf, T.; Luedike, P. Cardiopulmonary Profiling of Athletes with Post-Exertional Malaise after COVID-19 Infection—A Single-Center Experience. J. Clin. Med. 2023, 12, 4348. https://doi.org/10.3390/jcm12134348
Wernhart S, Weihe E, Totzeck M, Balcer B, Rassaf T, Luedike P. Cardiopulmonary Profiling of Athletes with Post-Exertional Malaise after COVID-19 Infection—A Single-Center Experience. Journal of Clinical Medicine. 2023; 12(13):4348. https://doi.org/10.3390/jcm12134348
Chicago/Turabian StyleWernhart, Simon, Eberhard Weihe, Matthias Totzeck, Bastian Balcer, Tienush Rassaf, and Peter Luedike. 2023. "Cardiopulmonary Profiling of Athletes with Post-Exertional Malaise after COVID-19 Infection—A Single-Center Experience" Journal of Clinical Medicine 12, no. 13: 4348. https://doi.org/10.3390/jcm12134348
APA StyleWernhart, S., Weihe, E., Totzeck, M., Balcer, B., Rassaf, T., & Luedike, P. (2023). Cardiopulmonary Profiling of Athletes with Post-Exertional Malaise after COVID-19 Infection—A Single-Center Experience. Journal of Clinical Medicine, 12(13), 4348. https://doi.org/10.3390/jcm12134348