

How Refined Surgical Technical Solutions Can Make Bentall Operation a Low-Risk Procedure: 20-Year Personal Experience at the “Root” of the Aortic Diseases—It Is Time to Change Surgical Guidelines
 , , ,
, , ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Analysis
2.3. Surgical Indications
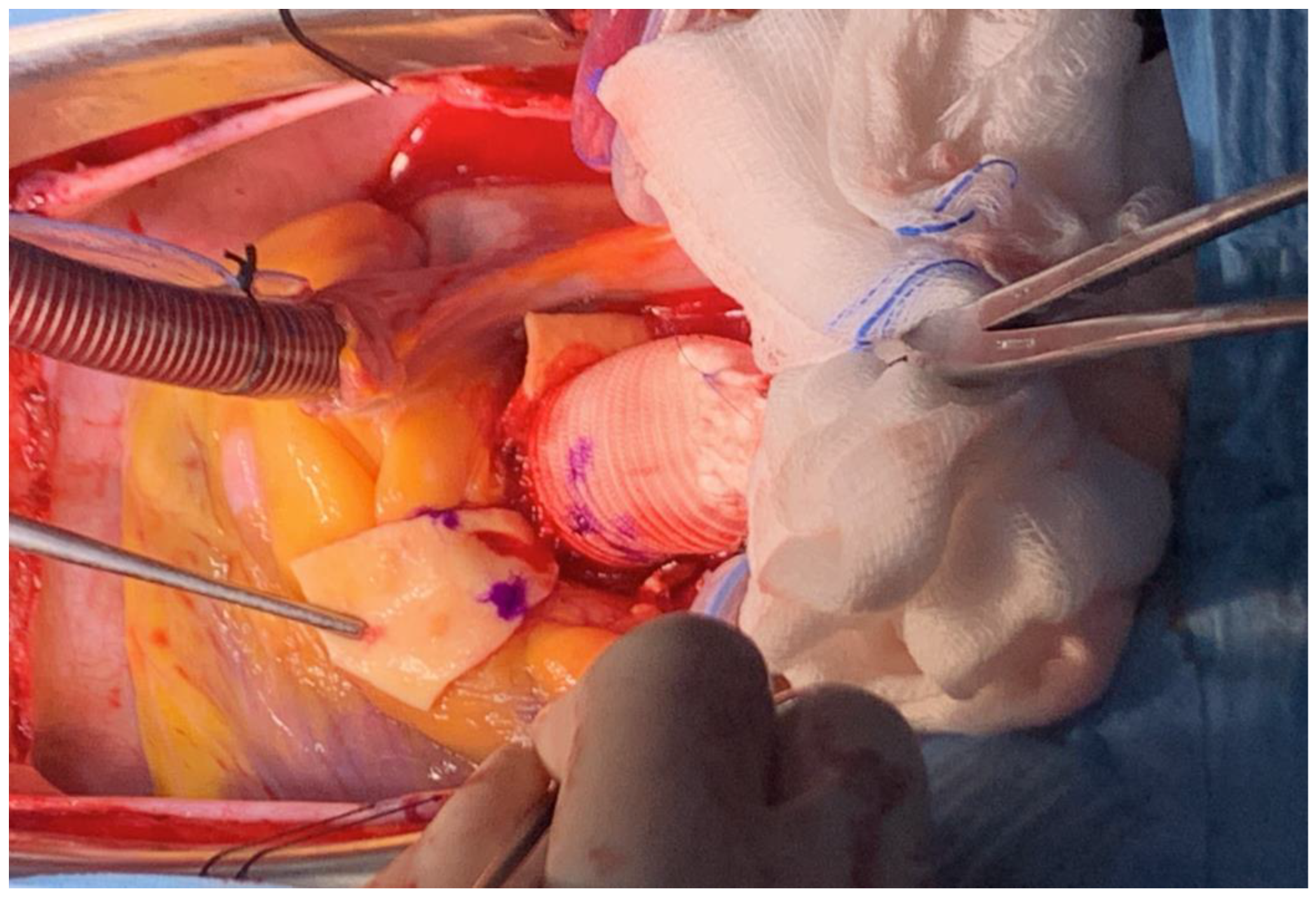
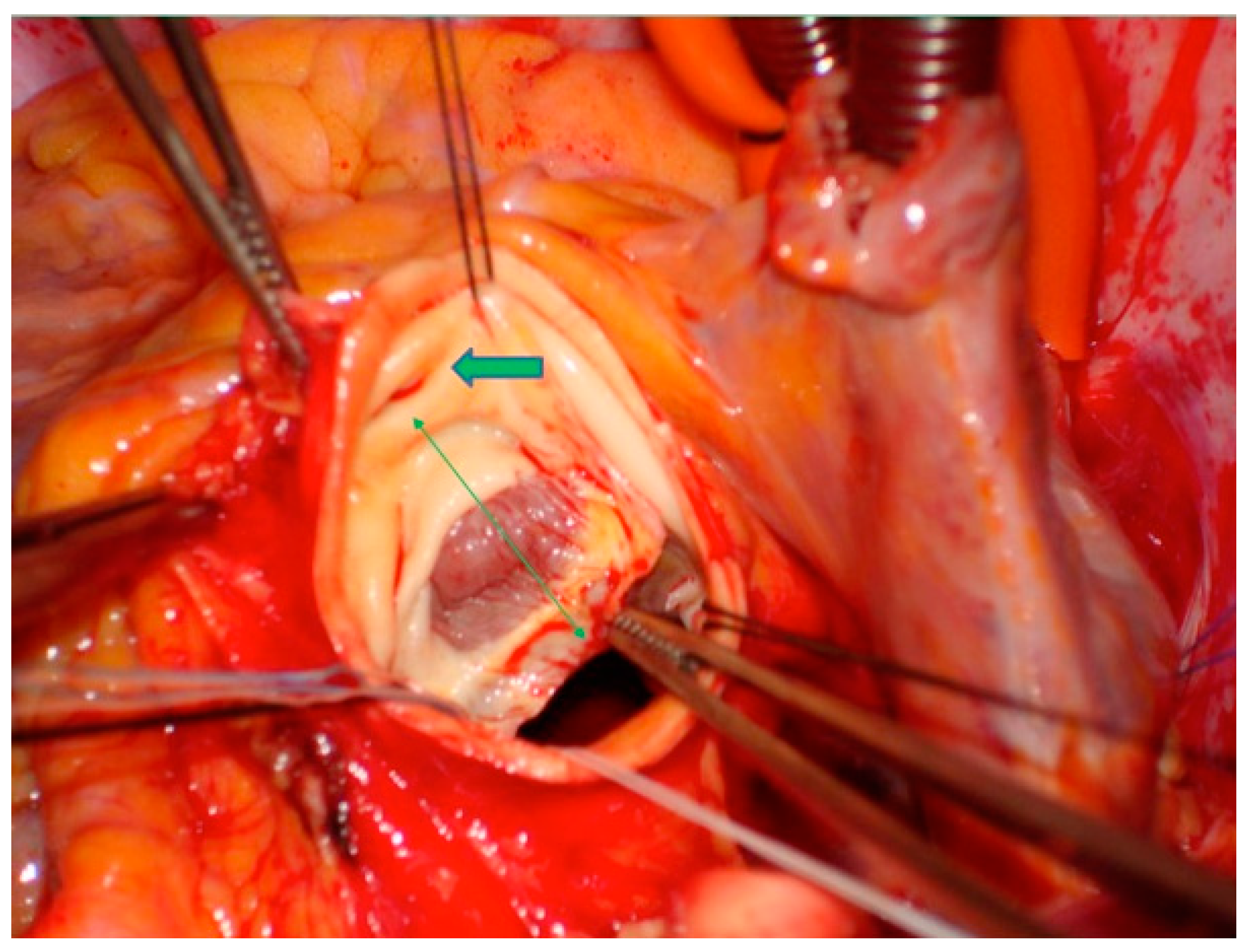
2.4. Surgical Technique
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentall, H.; De Bono, A. A technique for complete replacement of the ascending aorta. Thorax 1968, 23, 338–339. [Google Scholar] [CrossRef] [PubMed]
- Mookhoek, A.; Korteland, N.M.; Arabkhani, B.; Lansac, I.; Bekkers, J.A.; Bogers, A.J.; Takkenberg, J.J. Bentall Procedure: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2016, 101, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Castrovinci, S.; Tian, D.H.; Murana, G.; Cefarelli, M.; Berretta, P.; Alfonsi, J.; Yan, T.D.; Di Bartolomeo, R.; Di Eusanio, M. Aortic Root Replacement With Biological Valved Conduits. Ann. Thorac. Surg. 2015, 100, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, P.P.; Heinz, N.; Zhan, X.; Hijazi, H.; Zacher, M.; Diegeler, A. Modified bio-Bentall procedure: 10-year experience. Eur. J. Cardiothorac. Surg. 2010, 37, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, L.; Pacini, D.; Pantaleo, A.; Leone, A.; Barberio, G.; Marinelli, G.; Di Bartolomeo, R. Composite valve graft implantation for the treatment of aortic valve and root disease: Results in 1045 patients. J. Thorac. Cardiovasc. Surg. 2016, 152, 1041–1048.e1041. [Google Scholar] [CrossRef] [PubMed]
- Lechiancole, A.; Celiento, M.; Isola, M.; Gatti, G.; Melina, G.; Vendramin, I.; Battistella, C.; Pappalardo, A.; Sinatra, R.; Bortolotti, U.; et al. Modified Bentall procedure: Mechanical vs biological valved conduits in patients older than 65 years. Int. J. Cardiol. 2019, 296, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, G.; Pirro, F.; Macchione, A.; Bellisario, A.; Weltert, L. Long-term follow-up after Bentall operation using a stentless Shelhigh NR-2000 bio-conduit. J. Card. Surg. 2020, 35, 988–995. [Google Scholar] [CrossRef]
- Katselis, C.; Samanidis, G.; Papasotiriou, A.; Kriaras, I.; Antoniou, T.; Khoury, M.; Michalis, A.; Perreas, K. Long-Term Results after Modified Bentall Operation in 200 Patients. J. Heart Valve Dis. 2017, 26, 639–645. [Google Scholar]
- Celiento, M.; Ravenni, G.; Margaryan, R.; Ferrari, G.; Blasi, S.; Pratali, S.; Bortolotti, U. The Modified Bentall Procedure: A Single-Institution Experience in 249 Patients with a Maximum Follow Up of 21.5 Years. J. Heart Valve Dis. 2016, 25, 448–455. [Google Scholar]
- Dhurandhar, V.; Parikh, R.; Saxena, A.; Vallely, M.P.; Wilson, M.K.; Black, D.A.; Tran, L.; Reid, C.M.; Bannon, P.G. The Aortic Root Replacement Procedure: 12-year Experience from the Australian and New Zealand Society of Cardiac and Thoracic Surgeons Database. Heart Lung. Circ. 2016, 25, 1245–1251. [Google Scholar] [CrossRef]
- Nardi, P.; Ruvolo, G. Current surgical indications to surgical repair of the aneurysms of the ascending aorta. J. Vasc. Endovasc. Surg. 2016, 1, 9. [Google Scholar]
- Nardi, P.; Pisano, C.; Bassano, C.; Bertoldo, F.; Salvati, A.C.; Buioni, D.; Trombetti, D.; Asta, L.; Scognamiglio, M.; Altieri, C.; et al. Bentall Operation: Early Surgical Results, Seven-Year Outcomes, and Risk Factors Analysis. Int. J. Env. Res. Public. Health 2022, 20, 212. [Google Scholar] [CrossRef]
- Pisano, C.; D’Amico, F.; Balistreri, C.R.; Vacirca, S.R.; Nardi, P.; Altieri, C.; Scioli, M.G.; Bertoldo, F.; Santo, L.; Bellisario, D.; et al. Biomechanical properties and histomorphometric features of aortic tissue in patients with or without bicuspid aortic valve. J. Thorac. Dis. 2020, 12, 2304–2316. [Google Scholar] [CrossRef]
- Scola, L.; Di Maggio, F.M.; Vaccarino, L.; Bova, M.; Forte, G.I.; Pisano, C.; Candore, G.; Colonna-Romano, G.; Lio, D.; Ruvolo, G.; et al. Role of TGF-β pathway polymorphisms in sporadic thoracic aortic aneurysm: rs900 TGF-β2 is a marker of differential gender susceptibility. Mediat. Inflamm. 2014, 2014, 165758. [Google Scholar] [CrossRef]
- Pisano, C.; Balistreri, C.R.; Nardi, P.; Altieri, C.; Bertoldo, F.; Buioni, D.; Ruvolo, G. Risk of aortic dissection in patients with ascending aorta aneurysm: A new biological, morphological and biochemical networkbehind the aortic diameter. Vessel. Plus. 2020, 4, 33. [Google Scholar] [CrossRef]
- Bassano, C.; Vacirca, S.R.; Colella, D.; Bertoldo, F.; Pugliese, M.; Ferrante, M.S.; Ruvolo, G. Is the diameter of the aorta a safe parameter for cardiac surgery indication in aortic aneurysm? Proceedings of XXIX SICCH Meeting, 23–25 November 2018, Rome. J. Cardiovasc. Med. 2018, 19 (Suppl. 2). [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Arabkhani, B.; Klautz, R.J.M.; de Heer, F.; De Kerchove, L.; El Khoury, G.; Lansac, E.; Schäfers, H.J.; El-Hamamsy, I.; Lenoir, M.; Aramendi, J.I.; et al. A multicentre, propensity score matched analysis comparing a valve-sparing approach to valve replacement in aortic root aneurysm: Insight from the AVIATOR database. Eur. J. Cardiothorac. Surg. 2023, 63, 514. [Google Scholar] [CrossRef]
- Wallen, T.; Habertheuer, A.; Bavaria, J.E.; Hughes, G.C.; Badhwar, V.; Jacobs, J.P.; Yerokun, B.; Thibault, D.; Milewski, K.; Desai, N.; et al. Elective Aortic Root Replacement in North America: Analysis of STS Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2019, 107, 1307–1312. [Google Scholar] [CrossRef]
- Stamou, S.C.; Williams, M.L.; Gunn, T.M.; Hagberg, R.C.; Lobdell, K.W.; Kouchoukos, N.T. Aortic root surgery in the United States: A report from the Society of Thoracic Surgeons database. J. Thorac. Cardiovasc. Surg. 2015, 149, 116–122.e114. [Google Scholar] [CrossRef]
- Akins, C.W.; Miller, D.C.; Turina, M.I.; Kouchoukos, N.T.; Blackstone, E.H.; Grunkemeier, G.L.; Takkenberg, J.J.; David, T.E.; Butchart, E.G.; Adams, D.H.; et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. J. Thorac. Cardiovasc. Surg. 2008, 135, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Ziakas, A.G.; Economou, F.I.; Charokopos, N.A.; Pitsis, A.A.; Parharidou, D.G.; Papadopoulos, T.I.; Parharidis, G.E. Coronary ostial stenosis after aortic valve replacement. Tex. Heart Inst. J. 2010, 37, 465–468. [Google Scholar]
- Adamson, C.; Rocchiccioli, P.; Brogan, R.; Berry, C.; Ford, T.J. Post-operative myocardial infarction following aortic root surgery with coronary reimplantation: A case series treated with percutaneous coronary intervention. Eur. Heart J. Case Rep. 2019, 3, 1–6. [Google Scholar] [CrossRef]
- Westaby, S.; Katsumata, T.; Vaccari, G. Aortic root replacement with coronary button re-implantation: Low risk and predictable outcome. Eur. J. Cardiothorac. Surg. 2000, 17, 259–265. [Google Scholar] [CrossRef]
- Sultan, I.; Komlo, C.M.; Bavaria, J.E. How I teach a valve-sparing root replacement. Ann. Thorac. Surg. 2016, 101, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, P.P. Aortic root replacement with coronary button reimplantation. Eur. J. Cardiothorac. Surg. 2000, 18, 732. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruvolo, G.; Altieri, C.; Bassano, C.; Buioni, D.; Nardi, P.; Pisano, C. How Refined Surgical Technical Solutions Can Make Bentall Operation a Low-Risk Procedure: 20-Year Personal Experience at the “Root” of the Aortic Diseases—It Is Time to Change Surgical Guidelines. J. Clin. Med. 2023, 12, 7330. https://doi.org/10.3390/jcm12237330
Ruvolo G, Altieri C, Bassano C, Buioni D, Nardi P, Pisano C. How Refined Surgical Technical Solutions Can Make Bentall Operation a Low-Risk Procedure: 20-Year Personal Experience at the “Root” of the Aortic Diseases—It Is Time to Change Surgical Guidelines. Journal of Clinical Medicine. 2023; 12(23):7330. https://doi.org/10.3390/jcm12237330
Chicago/Turabian StyleRuvolo, Giovanni, Claudia Altieri, Carlo Bassano, Dario Buioni, Paolo Nardi, and Calogera Pisano. 2023. "How Refined Surgical Technical Solutions Can Make Bentall Operation a Low-Risk Procedure: 20-Year Personal Experience at the “Root” of the Aortic Diseases—It Is Time to Change Surgical Guidelines" Journal of Clinical Medicine 12, no. 23: 7330. https://doi.org/10.3390/jcm12237330
APA StyleRuvolo, G., Altieri, C., Bassano, C., Buioni, D., Nardi, P., & Pisano, C. (2023). How Refined Surgical Technical Solutions Can Make Bentall Operation a Low-Risk Procedure: 20-Year Personal Experience at the “Root” of the Aortic Diseases—It Is Time to Change Surgical Guidelines. Journal of Clinical Medicine, 12(23), 7330. https://doi.org/10.3390/jcm12237330