
Classification of Peripheral Blood Leukocyte Phenotypes and Serum Cytokines in Vogt–Koyanagi–Harada Disease before and after Glucocorticoid Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Diagnostics and Treatments
2.3. Leukocyte Phenotypes and Their Proportions in Peripheral Blood
2.4. Serum Cytokines Levels
2.5. Statistical Analysis
3. Results
3.1. Subjects
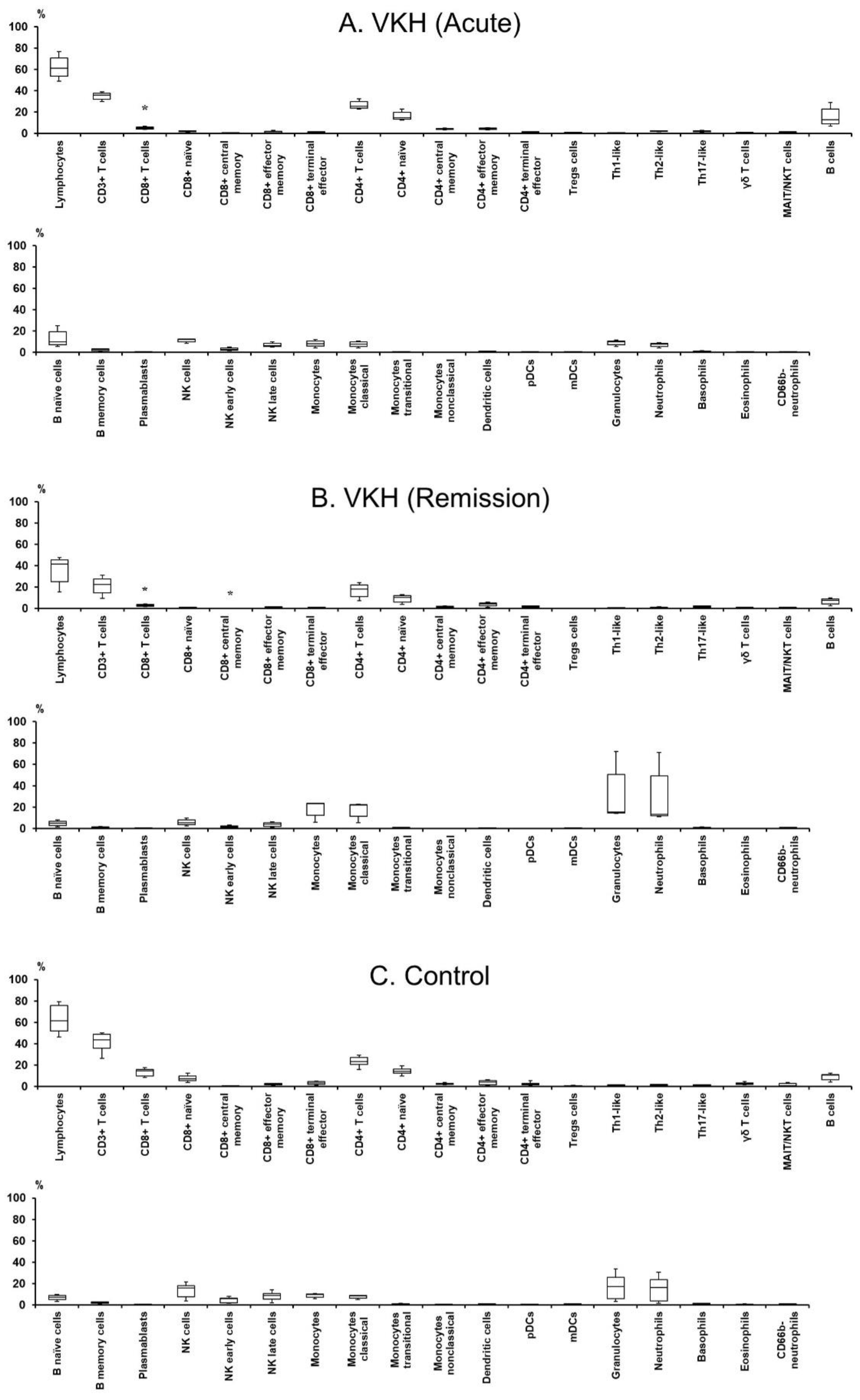
3.2. Profile of Leukocyte Phenotypes and Proportions in Peripheral Blood
3.3. Hierarchical Cluster Analysis of Immune Cell Populations among Leukocytes in Peripheral Blood
3.4. Profile of Serum Cytokine Levels
3.5. Hierarchical Cluster Analysis of Serum Cytokines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Chang, J.H.M.; Wakefield, D. Uveitis: A global perspective. Ocul. Immunol. Inflamm. 2002, 10, 263–279. [Google Scholar] [CrossRef] [PubMed]
- Suttorp-Schulten, M.S.; Rothova, A. The possible impact of uveitis in blindness: A literature survey. Br. J. Ophthalmol. 1996, 80, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Abu El-Asrar, A.M.; Van Damme, J.; Struyf, S.; Opdenakker, G. New Perspectives on the Immunopathogenesis and Treatment of Uveitis Associated With Vogt-Koyanagi-Harada Disease. Front. Med. 2021, 8, 705796. [Google Scholar] [CrossRef] [PubMed]
- Maezawa, N.; Yano, A.; Taniguchi, M.; Kojima, S. The role of cytotoxic T lymphocytes in the pathogenesis of Vogt-Koyanagi-Harada disease. Ophthalmologica 1982, 185, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P.; Mochizuki, M. Vogt–Koyanagi–Harada disease: Inquiry into the genesis of a disease name in the historical context of Switzerland and Japan. Int. Ophthalmol. 2007, 27, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Ma, R.; Zhong, Y.; Chen, Z.; Zhou, H.; Zhou, M.; Chong, W.; Chen, J. Deficiency of IL-27 Signaling Exacerbates Experimental Autoimmune Uveitis with Elevated Uveitogenic Th1 and Th17 Responses. Int. J. Mol. Sci. 2021, 22, 7517. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.; Yang, P.; Li, B.; Wu, C.; Jin, H.; Zhu, X.; Chen, L.; Zhou, H.; Huang, X.; Kijlstra, A. IL-23 promotes CD4+ T cells to produce IL-17 in Vogt-Koyanagi-Harada disease. J. Allergy Clin. Immunol. 2007, 119, 1218–1224. [Google Scholar] [CrossRef]
- Sakamoto, T.; Murata, T.; Inomata, H. Class II major histocompatibility complex on melanocytes of Vogt-Koyanagi-Harada disease. Arch. Ophthalmol. 1991, 109, 1270–1274. [Google Scholar] [CrossRef]
- Jiang, H.; Li, Z.; Yu, L.; Zhang, Y.; Zhou, L.; Wu, J.; Yuan, J.; Han, M.; Xu, T.; He, J.; et al. Immune Phenotyping of Patients With Acute Vogt-Koyanagi-Harada Syndrome Before and After Glucocorticoids Therapy. Front. Immunol. 2021, 12, 659150. [Google Scholar] [CrossRef]
- Jakubzick, C.V.; Randolph, G.J.; Henson, P.M. Monocyte differentiation and antigen-presenting functions. Nat. Rev. Immunol. 2017, 17, 349–362. [Google Scholar] [CrossRef]
- Ziegler-Heitbrock, L.; Ancuta, P.; Crowe, S.; Dalod, M.; Grau, V.; Hart, D.N.; Leenen, P.J.M.; Liu, Y.-J.; MacPherson, G.; Randolph, G.J.; et al. Nomenclature of monocytes and dendritic cells in blood. Blood 2010, 116, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- Cros, J.; Cagnard, N.; Woollard, K.; Patey, N.; Zhang, S.Y.; Senechal, B.; Puel, A.; Biswas, S.K.; Moshous, D.; Picard, C.; et al. Human CD14dim monocytes patrol and sense nucleic acids and viruses via TLR7 and TLR8 receptors. Immunity 2010, 33, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Geissmann, F.; Jung, S.; Littman, D.R. Blood monocytes consist of two principal subsets with distinct migratory properties. Immunity 2003, 19, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Belge, K.U.; Von Hundelshausen, P.; Draude, G.; Steppich, B.; Mack, M.; Frankenberger, M.; Weber, K.S.; Ziegler-Heitbrock, H.W. Differential chemokine receptor expression and function in human monocyte subpopulations. J. Leukoc. Biol. 2000, 67, 699–704. [Google Scholar] [CrossRef]
- Ancuta, P.; Rao, R.; Moses, A.; Mehle, A.; Shaw, S.K.; Luscinskas, F.W.; Gabuzda, D. Fractalkine preferentially mediates arrest and migration of CD16+ monocytes. J. Exp. Med. 2003, 197, 1701–1707. [Google Scholar] [CrossRef]
- Wong, K.L.; Tai, J.J.-Y.; Wong, W.-C.; Han, H.; Sem, X.; Yeap, W.-H.; Kourilsky, P.; Wong, S.-C. Gene expression profiling reveals the defining features of the classical, intermediate, and nonclassical human monocyte subsets. Blood 2011, 118, e16–e31. [Google Scholar] [CrossRef]
- Kapellos, T.S.; Bonaguro, L.; Gemünd, I.; Reusch, N.; Saglam, A.; Hinkley, E.R.; Schultze, J.L. Human monocyte subsets and phenotypes in major chronic inflammatory diseases. Front. Immunol. 2019, 10, 2035. [Google Scholar] [CrossRef]
- Read, R.W.; Holland, G.N.; Rao, N.A.; Tabbara, K.F.; Ohno, S.; Arellanes-Garcia, L.; Pivetti-Pezzi, P.; Tessler, H.H.; Usui, M. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: Report of an international committee on nomenclature. Am. J. Ophthalmol. 2001, 131, 647–652. [Google Scholar] [CrossRef]
- Chui, T.Y.; VanNasdale, D.A.; Elsner, A.E.; Burns, S.A. The association between the foveal avascular zone and retinal thickness. Investig. Ophthalmol. Vis. Sci. 2014, 55, 6870–6877. [Google Scholar] [CrossRef]
- Group ETDRSR. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report no. 4. Int. Ophthalmol. Clin. 1987, 27, 265–272. [Google Scholar] [CrossRef]
- Branchini, L.A.; Adhi, M.; Regatieri, C.V.; Nandakumar, N.; Liu, J.J.; Laver, N.; James G Fujimoto, J.G.; Duker, J.S. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology 2013, 120, 1901–1908. [Google Scholar] [CrossRef] [PubMed]
- Bagwell, C.B.; Hunsberger, B.; Hill, B.; Herbert, D.; Bray, C.; Selvanantham, T.; Li, S.; Villasboas, J.C.; Pavelko, K.; Strausbauch, M. Multi-site reproducibility of a human immunophenotyping assay in whole blood and peripheral blood mononuclear cells preparations using CyTOF technology coupled with Maxpar Pathsetter, an automated data analysis system. Cytometry B Clin. Cytom. 2020, 98, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Enoki, T.; Karasawa, Y.; Someya, H.; Taguchi, M.; Harimoto, K.; Takayama, K.; Kanda, T.; Ito, M.; Takeuchi, M. Inflammatory Factors of Macular Atrophy in Eyes with Neovascular Age-Related Macular Degeneration Treated with Aflibercept. Front. Immunol. 2021, 12, 738521. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Wilks, D.S. Cluster analysis. In International Geophysics. 100; Elsevier: Amsterdam, The Netherlands, 2011; pp. 603–616. [Google Scholar]
- Yamaki, K.; Gocho, K.; Hayakawa, K.; Kondo, I.; Sakuragi, S. Tyrosinase family proteins are antigens specific to Vogt-Koyanagi-Harada disease. J. Immunol. 2000, 165, 7323–7329. [Google Scholar] [CrossRef]
- Liang, L.; Peng, X.-Y.; Wang, H. Th lymphocyte subsets in patients with Vogt-Koyanagi-Harada disease. Int. J. Ophthalmol. 2019, 12, 207–211. [Google Scholar]
- Opdenakker, G.; El-Asrar, A.A.; Van Damme, J. Remnant epitopes generating autoimmunity: From model to useful paradigm. Trends Immunol. 2020, 41, 367–378. [Google Scholar] [CrossRef]
- Rajan, T.V. The Gell-Coombs classification of hypersensitivity reactions: A re-interpretation. Trends Immunol. 2003, 24, 376–379. [Google Scholar] [CrossRef]
- Gell, P.G.H.; Coombs, R.R.A. Clinical Aspects of Immunology; Blackwell Scientific Publications: Oxford, UK, 1963. [Google Scholar]
- Bendiner, E. Baron von Pirquet: The aristocrat who discovered and defined allergy. Hosp. Pract. (Off. Ed.) 1981, 16, 137. [Google Scholar]
- Inomata, H.; Sakamoto, T. Immunohistochemical studies of Vogt-Koyanagi-Harada disease with sunset sky fundus. Curr. Eye Res. 1990, 9, 35–40. [Google Scholar] [CrossRef]
- Damico, F.M.; Cunha-Neto, E.; Goldberg, A.C.; Iwai, L.K.; Marin, M.L.; Hammer, J.; Jorge Kalil, J.; Yamamoto, J.H. T-cell recognition and cytokine profile induced by melanocyte epitopes in patients with HLA-DRB1*0405-positive and -negative Vogt-Koyanagi-Harada uveitis. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2465–2471. [Google Scholar] [CrossRef] [PubMed]
- Hammer, H. Cellular hypersensitivity to uveal pigment confirmed by leucocyte migration tests in sympathetic ophthalmitis and the Vogt-Koyanagi-Harada syndrome. Br. J. Ophthalmol. 1974, 58, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Kay, A.B. Allergy and allergic diseases. N. Engl. J. Med. 2001, 344, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Goto, H.; Zako, M.; Namba, K.; Hashida, N.; Kaburaki, T.; Miyazaki, M.; Sonoda, K.-H.; Abe, T.; Mizuki, N.; Kamoi, K.; et al. Adalimumab in active and inactive, non-infectious uveitis: Global results from the VISUAL I and VISUAL II trials. Ocul. Immunol. Inflamm. 2019, 27, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Jiang, Q.; Lv, J.; Yang, S.; Huang, Z.; Duan, R.; Tao, T.; Li, Z.; Ju, R.; Zheng, Y.; et al. Insights gained from single-cell analysis of immune cells in tofacitinib treatment of Vogt-Koyanagi-Harada disease. JCI Insight. 2022, 7, e162335. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, K.; Lechner, K.; Popp, V.; Offensperger, L.; Zundler, S.; Wiendl, M.; Becker, E.; Atreya, R.; Rath, T.; Neurath, M.F. The JAK1/3 inhibitor to tofacitinib suppresses T cell homing and activation in chronic intestinal inflammation. J. Crohn’s Colitis 2021, 15, 244–257. [Google Scholar] [CrossRef] [PubMed]
- Papasavvas, I.; Tugal-Tutkun, I.; Herbort, C.P., Jr. Vogt–Koyanagi–Harada is a curable autoimmune disease: Early diagnosis and immediate dual steroidal and non-steroidal immunosuppression are crucial prerequisites. J. Curr. Ophthalmol. 2020, 32, 310–314. [Google Scholar]
- Read, R.W.; Rechodouni, A.; Butani, N.; Johnston, R.; LaBree, L.D.; Smith, R.E.; Rao, N.A. Complications and prognostic factors in Vogt-Koyanagi-Harada disease. Am. J. Ophthalmol. 2001, 131, 599–606. [Google Scholar] [CrossRef]
- Meijsing, S.H. Mechanisms of Glucocorticoid-Regulated Gene Transcription. Adv. Exp. Med. Biol. 2015, 872, 59–81. [Google Scholar]
- Sloka, J.; Stefanelli, M. The mechanism of action of methylprednisolone in the treatment of multiple sclerosis. Mult. Scler. 2005, 11, 425–432. [Google Scholar] [CrossRef]
- Oukka, M. Th17 cells in immunity and autoimmunity. Ann. Rheum. Dis. 2008, 67 (Suppl. 3), 26–29. [Google Scholar] [CrossRef] [PubMed]
- Luger, D.; Silver, P.B.; Tang, J.; Cua, D.; Chen, Z.; Iwakura, Y.; Bowman, E.D.; Sgambellone, N.M.; Chan, C.-C.; Caspi, R.R. Either a Th17 or a Th1 effector response can drive autoimmunity: Conditions of disease induction affect dominant effector category. J. Exp. Med. 2008, 205, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, L.; Liotta, F.; Maggi, E.; Romagnani, S.; Annunziato, F. Th17 cells: New players in asthma pathogenesis. Allergy 2011, 66, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Bending, D.; De la Peña, H.; Veldhoen, M.; Phillips, J.M.; Uyttenhove, C.; Stockinger, B.; Cooke, A. Highly purified Th17 cells from BDC2.5NOD mice convert into Th1-like cells in NOD/SCID recipient mice. J. Clin. Investig. 2009, 119, 565–572. [Google Scholar] [CrossRef]
- Nistala, K.; Adams, S.; Cambrook, H.; Ursu, S.; Olivito, B.; de Jager, W.; Evans, J.G.; Cimaz, R.; Bajaj-Elliott, M.; Wedderburn, L.R. Th17 plasticity in human autoimmune arthritis is driven by the inflammatory environment. Proc. Natl. Acad. Sci. USA 2010, 107, 14751–14756. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, L.; Cimaz, R.; Maggi, L.; Santarlasci, V.; Capone, M.; Borriello, F.; Frosali, F.; Querci, V.; Simonini, G.; Barra, G. CD4+ CD161+ T cells showing transient nature of the Th17 phenotype are present in the synovial fluid from patients with juvenile idiopathic arthritis. Arthritis Rheum. 2011, 63, 2504–2515. [Google Scholar] [CrossRef]
- Baker, K.F.; Isaacs, J.D. Novel therapies for immune-mediated inflammatory diseases: What can we learn from their use in rheumatoid arthritis, spondyloarthritis, systemic lupus erythematosus, psoriasis, Crohn’s disease and ulcerative colitis? Ann. Rheum. Dis. 2018, 77, 175–187. [Google Scholar] [CrossRef]
- Leonardi, C.L.; Kimball, A.B.; Papp, K.A.; Yeilding, N.; Guzzo, C.; Wang, Y.; Li, S.; Dooley, L.T.; Gordon, K.B. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). Lancet 2008, 371, 1665–1674. [Google Scholar] [CrossRef]
- Murakami, S.; Inaba, Y.; Mochizuki, M.; Nakajima, A.; Urayama, A. A nationwide survey on the occurrence of Vogt-Koyanagi-Harada disease in Japan. Jpn. J. Ophthalmol. 1994, 38, 208–213. [Google Scholar]
- Lazuardi, L.; Jenewein, B.; Wolf, A.M.; Pfister, G.; Tzankov, A.; Grubeck-Loebenstein, B. Age-related loss of naive T cells and dysregulation of T-cell/B-cell interactions in human lymph nodes. Immunology 2005, 114, 37–43. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | p Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | VKH (Acute) | ||||||||||||
| Disease Stage | Acute | Remission | Remission | vs. | |||||||||
| Median | First | Third | Median | First | Third | Median | First | Third | Control | VKH | |||
| Quartile | Quartile | Quartile | Quartile | Quartile | Quartile | (Remission) | |||||||
| Age | 66 | 60 | 70.5 | 30 | 26.5 | 31 | 0.038 | ||||||
| Gender (M/F) | 1/2 | 4/3 | 1 | ||||||||||
| LogMAR VA | 0 | −0.04 | 0 | 0 | −0.04 | 0 | - | - | 0.604 | ||||
| IOP | 11.0 | 10.5 | 13.3 | 15.0 | 13.5 | 16.5 | - | - | 0.111 | ||||
| CFT | 276.0 | 248.5 | 398.0 | 246.0 | 243.5 | 252.0 | - | - | 0.604 | ||||
| CRT | 329.0 | 328.5 | 438.0 | 296.0 | 293.0 | 311.0 | - | - | 0.111 | ||||
| SFCT | 194.0 | 185.0 | 206.5 | 227.0 | 163.5 | 232.5 | - | - | 1 | ||||
| Populations | Model Phenotypes | VKH | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 3 | ||||||||||
| Disease Stage | Acute | Remission | |||||||||
| Median | First | Third | Median | First | Third | ||||||
| Quartile | Quartile | Quartile | Quartile | ||||||||
| Intact live cells (%) | |||||||||||
| Lymphocytes | CD3 T cells + B cells + NK cells + plasmablasts | 61.1 | 53.6 | 70.8 | 41.5 | 25.3 | 45.3 | ||||
| CD3+ T cells | CD8 T cells + CD4 T cells + γδ T cells + MAIT/NKT cells | 36 | 32.2 | 37.8 | 22.7 | 14.6 | 27.9 | ||||
| CD8+ T cells | CD3+ CD66b− CD19− CD8+ CD4− CD14− CD161− TCRγδ− CD123− CD11c− | 4.98 | 4.25 | 6.27 | 3.14 | 2.35 | 3.79 | ||||
| Naïve | CD8 T cells + CD45RA+ CCR7+ CD27+ | 1.95 | 1.73 | 2.13 | 0.75 | 0.59 | 1.22 | ||||
| Central memory | CD8 T cells + CD45RA− CCR7+ CD27+ | 0.43 | 0.27 | 0.6 | 0.03 | 0.02 | 0.04 | ||||
| Effector memory | CD8 T cells + CCR7− CD27+ | 0.8 | 0.78 | 2.24 | 1.46 | 0.95 | 1.58 | ||||
| Terminal effector | CD8 T cells + CCR7− CD27− | 1.18 | 0.98 | 1.5 | 0.7 | 0.68 | 0.98 | ||||
| CD4+ T cells | CD66b− CD3+ CD8− CD4+ CD14− TCRγδ− CD11c− | 25.7 | 24 | 29.9 | 18.2 | 11.3 | 22 | ||||
| Naïve | CD4 T cells + CD45RA+ CCR7+ CD27+ | 14.7 | 13.3 | 19.9 | 10.2 | 6.16 | 12 | ||||
| Central memory | CD4 T cells + CD45RA− CCR7+ CD27+ | 4.4 | 3.77 | 4.77 | 1.64 | 1.41 | 2.21 | ||||
| Effector memory | CD4 T cells + CD45RA− CCR7− CD27+ | 4.41 | 3.83 | 5.13 | 4.2 | 2.46 | 5.28 | ||||
| Terminal effector | CD4 T cells + CD45RA− CCR7− CD27− | 1.3 | 1.05 | 1.67 | 2.12 | 1.28 | 2.54 | ||||
| Treg cells | CD4 T cells + CD25+ CD127− CCR4+ | 0.66 | 0.51 | 0.7 | 0.12 | 0.12 | 0.36 | ||||
| Th1-like | CD4 T cells + CXCR3+ CCR6− CXCR5− CCR4− | 0.46 | 0.43 | 0.48 | 0.3 | 0.27 | 0.75 | ||||
| Th2-like | CD4 T cells + CXCR3− CCR6− CXCR5− CCR4+ | 2.28 | 2.11 | 2.28 | 0.86 | 0.54 | 1.3 | ||||
| Th17-like | CD4 T cells + CXCR3− CCR6+ CXCR5− CCR4+ | 2.2 | 1.72 | 2.69 | 2.19 | 1.28 | 2.43 | ||||
| γδ T cells | CD66b− CD3+ CD8dim,− CD4− CD14− TCRγδ dim,+ | 1.03 | 0.81 | 1.22 | 0.41 | 0.36 | 1.08 | ||||
| CD4− T Cells | |||||||||||
| MAIT/NKT cells | CD66b− CD3+ CD4− CD14− CD161+ TCRγδ− CD28+ CD16− | 1.1 | 0.89 | 1.19 | 0.98 | 0.58 | 1.01 | ||||
| B cells | CD3− CD14− CD56− CD16 dim,− CD19+ CD20+ HLA-DR dim,+ | 12.9 | 9.09 | 22.9 | 7.76 | 4.44 | 9.01 | ||||
| Naïve | B cells + CD27− | 9.75 | 7.23 | 19.4 | 5.13 | 3.01 | 7.07 | ||||
| Memory | B cells + CD27+ | 2.84 | 1.71 | 3.18 | 1 | 0.6 | 1.59 | ||||
| Plasmablasts | CD3− CD14− CD16−,dim CD66b− CD20− CD19+ CD56− CD38++ CD27+ | 0.28 | 0.16 | 0.38 | 0.24 | 0.13 | 0.35 | ||||
| NK cells | CD14− CD3− CD123− CD66b− CD45RA+ CD56 dim,+ | 12.3 | 10.01 | 12.3 | 5.83 | 3.7 | 8.44 | ||||
| Early | NK cells + CD57− | 2.85 | 2.08 | 4.41 | 1.73 | 1.35 | 2.76 | ||||
| Late | NK cells + CD57+ | 6.33 | 5.6 | 8.67 | 4.11 | 2.35 | 5.68 | ||||
| Monocytes | CD3− CD19− CD56− CD66b− HLA-DR+ CD11c+ | 8.36 | 5.88 | 10.8 | 23.4 | 12.5 | 23.8 | ||||
| Classical | Monocytes + CD14+ CD38+ | 7.77 | 5.48 | 9.78 | 22 | 11.7 | 22.7 | ||||
| Transitional | Monocytes + CD14 dim CD38 dim | 0.44 | 0.32 | 0.69 | 0.73 | 0.42 | 0.89 | ||||
| Nonclassical | Monocytes + CD14− CD38− | 0.15 | 0.09 | 0.37 | 0.14 | 0.11 | 0.25 | ||||
| Dendritic cells | pDCs+ mDCs | 0.82 | 0.53 | 0.85 | 0.61 | 0.35 | 0.66 | ||||
| Plasmacytoid DCs | CD3− CD19− CD14− CD20− CD66b− HLA-DR dim,+ CD11c− CD123+ | 0.25 | 0.15 | 0.26 | 0.06 | 0.03 | 0.1 | ||||
| Myeloid DCs | CD3− CD19− CD14− CD20− HLA-DR dim,+ CD11c dim,+ CD123− CD16 dim,− CD38 dim,+ CD294− HLA−D | 0.56 | 0.37 | 0.59 | 0.55 | 0.32 | 0.55 | ||||
| Granulocytes | Neutrophils + basophils + eosinophils + CD66b− neutrophils | 9.81 | 7.32 | 11 | 15.7 | 14.8 | 50.9 | ||||
| Neutrophils | CD66b dim,+ CD16+ HLA-DR− | 7.6 | 5.62 | 8.46 | 13.4 | 12.1 | 49.5 | ||||
| Basophils | HLA-DR− CD66b− CD123 dim,+ CD38+ CD294+ | 0.96 | 0.86 | 1.43 | 0.91 | 0.52 | 1.43 | ||||
| Eosinophils | CD14− CD3− CD19− HLA-DR− CD294+ CD66b dim,+ | 0.38 | 0.25 | 0.42 | 0.11 | 0.1 | 0.17 | ||||
| CD66b− neutrophils | CD3− CD19− CD66b− CD56− HLA-DR− CD123− CD45− | 0.53 | 0.32 | 0.77 | 0.88 | 0.59 | 1.09 | ||||
| Populations | Control | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| n | 7 | Control vs. | VKH (Acute) vs. | |||||
| Median | First | Third | VKH | VKH | VKH | |||
| Quartile | Quartile | (Acute) | (Remission) | (Remission) | ||||
| Intact live cells (%) | ||||||||
| Lymphocytes | 61.6 | 52.0 | 75.6 | 0.595 | 0.082 | 0.111 | ||
| CD3+ T cells | 43.7 | 35.9 | 48.8 | 0.242 | 0.082 | 0.111 | ||
| CD8+ T cells | 14.6 | 9.99 | 15.8 | 0.038 | 0.038 | 0.111 | ||
| Naïve | 7.26 | 5.44 | 9.90 | 0.082 | 0.056 | 0.111 | ||
| Central memory | 0.20 | 0.12 | 0.25 | 0.385 | 0.038 | 0.111 | ||
| Effector memory | 1.83 | 1.59 | 2.88 | 0.445 | 0.175 | 0.604 | ||
| Terminal effector | 3.33 | 2.09 | 4.44 | 0.175 | 0.082 | 0.287 | ||
| CD4+ T cells | 23.2 | 20.5 | 27.0 | 0.521 | 0.242 | 0.287 | ||
| Naïve | 14.2 | 12.5 | 16.5 | 0.558 | 0.175 | 0.111 | ||
| Central memory | 2.09 | 1.83 | 2.66 | 0.082 | 0.445 | 0.111 | ||
| Effector memory | 4.04 | 1.55 | 5.32 | 0.558 | 0.595 | 1.000 | ||
| Terminal effector | 1.90 | 1.64 | 2.81 | 0.242 | 0.595 | 0.287 | ||
| Treg cells | 0.47 | 0.42 | 0.81 | 0.595 | 0.175 | 0.111 | ||
| Th1-like | 1.00 | 0.30 | 1.27 | 0.332 | 0.539 | 1 | ||
| Th2-like | 1.36 | 1.26 | 1.71 | 0.123 | 0.332 | 0.111 | ||
| Th17-like | 1.25 | 1.11 | 1.43 | 0.175 | 0.445 | 0.604 | ||
| γδT cells | 2.32 | 2.03 | 3.10 | 0.056 | 0.056 | 0.604 | ||
| CD4− T Cells | ||||||||
| MAIT/NKT cells | 0.92 | 0.59 | 2.71 | 0.595 | 0.558 | 0.111 | ||
| B cells | 10.5 | 6.51 | 11.3 | 0.445 | 0.332 | 0.111 | ||
| Naïve | 7.40 | 4.88 | 8.90 | 0.332 | 0.445 | 0.111 | ||
| Memory | 2.08 | 1.57 | 2.71 | 0.521 | 0.332 | 0.111 | ||
| Plasmablasts | 0.06 | 0.06 | 0.07 | 0.445 | 0.521 | 0.111 | ||
| NK cells | 15.7 | 7.64 | 18.1 | 0.521 | 0.242 | 0.287 | ||
| Early | 5.70 | 1.99 | 6.46 | 0.445 | 0.242 | 0.604 | ||
| Late | 8.89 | 5.66 | 10.7 | 0.558 | 0.175 | 0.604 | ||
| Monocytes | 9.65 | 7.29 | 10.0 | 0.558 | 0.445 | 0.287 | ||
| Classical | 8.55 | 6.20 | 8.68 | 0.595 | 0.445 | 0.287 | ||
| Transitional | 0.82 | 0.75 | 1.13 | 0.242 | 0.332 | 1 | ||
| Nonclassical | 0.48 | 0.22 | 0.56 | 0.332 | 0.175 | 1 | ||
| Dendritic cells | 0.79 | 0.57 | 0.93 | 0.558 | 0.242 | 0.111 | ||
| Plasmacytoid DCs | 0.12 | 0.08 | 0.19 | 0.503 | 0.385 | 0.111 | ||
| Myeloid DCs | 0.65 | 0.49 | 0.70 | 0.332 | 0.332 | 0.111 | ||
| Granulocytes | 17.0 | 5.82 | 25.9 | 0.521 | 0.521 | 0.111 | ||
| Neutrophils | 16.4 | 3.63 | 23.6 | 0.521 | 0.521 | 0.111 | ||
| Basophils | 1.08 | 0.48 | 1.29 | 0.595 | 0.613 | 0.604 | ||
| Eosinophils | 0.04 | 0.03 | 0.56 | 0.445 | 0.558 | 0.111 | ||
| CD66b− neutrophils | 0.57 | 0.41 | 0.67 | 0.558 | 0.445 | 0.604 | ||
| Category | VKH | Control | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 3 | 7 | ||||||||||
| Disease Stage | Acute | Remission | ||||||||||
| Detectable | Median | First | Third | Detectable | Median | First | Third | Detectable | Median | First | Third | |
| Rate (%) | Quartile | Quartile | Rate (%) | Quartile | Quartile | Rate (%) | Quartile | Quartile | ||||
| PDGF-BB | 3 (100) | 345.4 | 232.1 | 800.5 | 3 (100) | 288.4 | 171.2 | 760.2 | 7 (100) | 360.4 | 127.7 | 810.1 |
| IL-1β | 2 (66.7) | 0.39 | 0.20 | 0.47 | 0 (0) | 0 | 0 | 0 | 4 (57.1) | 0.31 | 0 | 0.58 |
| IL-1ra | 3 (100) | 24.0 | 22.8 | 30.0 | 3 (100) | 36.1 | 33.6 | 39.1 | 4 (57.1) | 13.1 | 0 | 32.1 |
| IL-2 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-4 | 3 (100) | 1.63 | 1.43 | 2.90 | 3 (100) | 3.46 | 3.45 | 4.08 | 5 (71.4) | 1.36 | 0.14 | 2.05 |
| IL-5 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-6 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-7 | 2 (66.7) | 33.7 | 16.8 | 42.7 | 1 (33.3) | 0 | 0 | 12.8 | 3 (42.9) | 0 | 0 | 17.5 |
| IL-8 | 1 (33.3) | 0 | 0 | 1.28 | 3 (100) | 1.50 | 1.40 | 2.16 | 2 (28.6) | 0 | 0 | 0.55 |
| IL-9 | 3 (100) | 27.4 | 24.1 | 38.3 | 3 (100) | 44.4 | 43.8 | 45.8 | 4 (57.1) | 2.89 | 0 | 40.7 |
| IL-10 | 1 (33.3) | 0 | 0 | 19.9 | 1 (33.3) | 0 | 0 | 9.22 | 0 (0) | 0 | 0 | 0 |
| IL-12 | 1 (33.3) | 0 | 0 | 12.5 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-13 | 1 (33.3) | 0 | 0 | 2.18 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-15 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IL-17A | 2 (66.7) | 3.38 | 1.69 | 4.29 | 2 (66.7) | 3.05 | 1.53 | 3.63 | 2 (28.6) | 0 | 0 | 2.96 |
| Eotaxin | 3 (100) | 139.6 | 119.0 | 168.1 | 3 (100) | 168.8 | 94.1 | 180.2 | 7 (100) | 9.29 | 6.07 | 84.0 |
| bFGF | 2 (66.7) | 4.94 | 2.47 | 5.47 | 0 (0) | 0 | 0 | 0 | 4 (57.1) | 4.67 | 0 | 4.94 |
| G-CSF | 2 (66.7) | 142.8 | 71.4 | 331.3 | 3 (100) | 166.5 | 132.9 | 264.2 | 1 (14.3) | 0 | 0 | 0 |
| GM-CSF | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| IFN-γ | 0 (0) | 0 | 0 | 0 | 1 (33.3) | 0 | 0 | 0.88 | 0 (0) | 0 | 0 | 0 |
| IP-10 | 3 (100) | 542.8 | 347.9 | 695.0 | 3 (100) | 70.5 | 61.4 | 101.7 | 7 (100) | 63.9 | 50.6 | 225.0 |
| MCP-1 | 3 (100) | 5.10 | 4.68 | 6.78 | 3 (100) | 7.16 | 6.48 | 7.97 | 2 (28.6) | 0 | 0 | 0.30 |
| MIP-1α | 2 (66.7) | 0.19 | 0.10 | 0.69 | 3 (100) | 0.53 | 0.49 | 1.45 | 3 (42.9) | 0 | 0 | 0.72 |
| MIP-1β | 3 (100) | 26.3 | 24.4 | 26.7 | 3 (100) | 23.0 | 20.9 | 29.8 | 5 (71.4) | 5.78 | 1.71 | 32.8 |
| RANTES | 3 (100) | 937.3 | 842.9 | 973.7 | 3 (100) | 580.3 | 395.5 | 614.8 | 7 (100) | 93.5 | 56.9 | 333.9 |
| TNFα | 2 (66.7) | 7.32 | 3.66 | 11.4 | 2 (66.7) | 13.4 | 6.68 | 17.3 | 2 (28.6) | 0 | 0 | 7.74 |
| VEGF-A | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 | 0 (0) | 0 | 0 | 0 |
| Category | p Value | Detection Range | ||||
|---|---|---|---|---|---|---|
| Control vs. | VKH (Acute) vs. | |||||
| VKH | VKH | VKH | ||||
| (Acute) | (Remission) | (Remission) | ||||
| PDGF-BB | 0.595 | 0.595 | 0.111 | 7.67 | to | 42,619.2 |
| IL-1β | 0.613 | 0.202 | 0.183 | 0.28 | to | 5036.8 |
| IL-1ra | 0.445 | 0.242 | 0.183 | 8.56 | to | 37,276.7 |
| IL-2 | 0.613 | 0.613 | 1 | 1.50 | to | 8778.3 |
| IL-4 | 0.445 | 0.038 | 0.111 | 0.16 | to | 3539.9 |
| IL-5 | 0.613 | 0.613 | 1 | 4.02 | to | 85,349.0 |
| IL-6 | 0.613 | 0.613 | 1 | 0.37 | to | 5969.6 |
| IL-7 | 0.242 | 0.595 | 0.183 | 1.84 | to | 36,229.8 |
| IL-8 | 0.595 | 0.123 | 0.111 | 0.51 | to | 10,416.3 |
| IL-9 | 0.332 | 0.175 | 0.287 | 0.92 | to | 21,827.0 |
| IL-10 | 0.445 | 0.445 | 0.319 | 0.84 | to | 12,755.7 |
| IL-12 | 0.445 | 0.613 | 0.319 | 1.58 | to | 21,263.1 |
| IL-13 | 0.445 | 0.613 | 0.319 | 0.75 | to | 5003.2 |
| IL-15 | 0.613 | 0.613 | 1 | 231.8 | to | 76,422.6 |
| IL-17A | 0.539 | 0.539 | 0.604 | 2.65 | to | 35,294.2 |
| Eotaxin | 0.123 | 0.123 | 0.604 | 0.09 | to | 1487.0 |
| bFGF | 0.539 | 0.202 | 0.183 | 3.52 | to | 5445.8 |
| G-CSF | 0.175 | 0.056 | 1 | 55.0 | to | 70,102.6 |
| GM-CSF | 0.613 | 0.613 | 1 | 0.33 | to | 1822.9 |
| IFN-γ | 0.613 | 0.445 | 0.319 | 0.74 | to | 22,825.9 |
| IP-10 | 0.123 | 0.595 | 0.111 | 1.53 | to | 23,765.1 |
| MCP-1 | 0.038 | 0.038 | 0.287 | 0.34 | to | 5761.9 |
| MIP-1α | 0.558 | 0.242 | 0.111 | 0.05 | to | 348.6 |
| MIP-1β | 0.558 | 0.445 | 0.604 | 0.46 | to | 2126.1 |
| RANTES | 0.123 | 0.175 | 0.111 | 1.00 | to | 5544.2 |
| TNFα | 0.521 | 0.503 | 0.183 | 2.73 | to | 53,796.5 |
| VEGF-A | 0.613 | 0.613 | 1 | 19.5 | to | 69,174.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, T.; Taniguchi, N.; Nishio, Y.; Ito, M.; Takeuchi, M. Classification of Peripheral Blood Leukocyte Phenotypes and Serum Cytokines in Vogt–Koyanagi–Harada Disease before and after Glucocorticoid Therapy. J. Clin. Med. 2023, 12, 7742. https://doi.org/10.3390/jcm12247742
Sato T, Taniguchi N, Nishio Y, Ito M, Takeuchi M. Classification of Peripheral Blood Leukocyte Phenotypes and Serum Cytokines in Vogt–Koyanagi–Harada Disease before and after Glucocorticoid Therapy. Journal of Clinical Medicine. 2023; 12(24):7742. https://doi.org/10.3390/jcm12247742
Chicago/Turabian StyleSato, Tomohito, Nanae Taniguchi, Yoshiaki Nishio, Masataka Ito, and Masaru Takeuchi. 2023. "Classification of Peripheral Blood Leukocyte Phenotypes and Serum Cytokines in Vogt–Koyanagi–Harada Disease before and after Glucocorticoid Therapy" Journal of Clinical Medicine 12, no. 24: 7742. https://doi.org/10.3390/jcm12247742
APA StyleSato, T., Taniguchi, N., Nishio, Y., Ito, M., & Takeuchi, M. (2023). Classification of Peripheral Blood Leukocyte Phenotypes and Serum Cytokines in Vogt–Koyanagi–Harada Disease before and after Glucocorticoid Therapy. Journal of Clinical Medicine, 12(24), 7742. https://doi.org/10.3390/jcm12247742