
A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Procedure
2.2.1. BESS
2.2.2. Microscopic ULBD
2.3. Outcome Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Surgical Outcome Evaluation
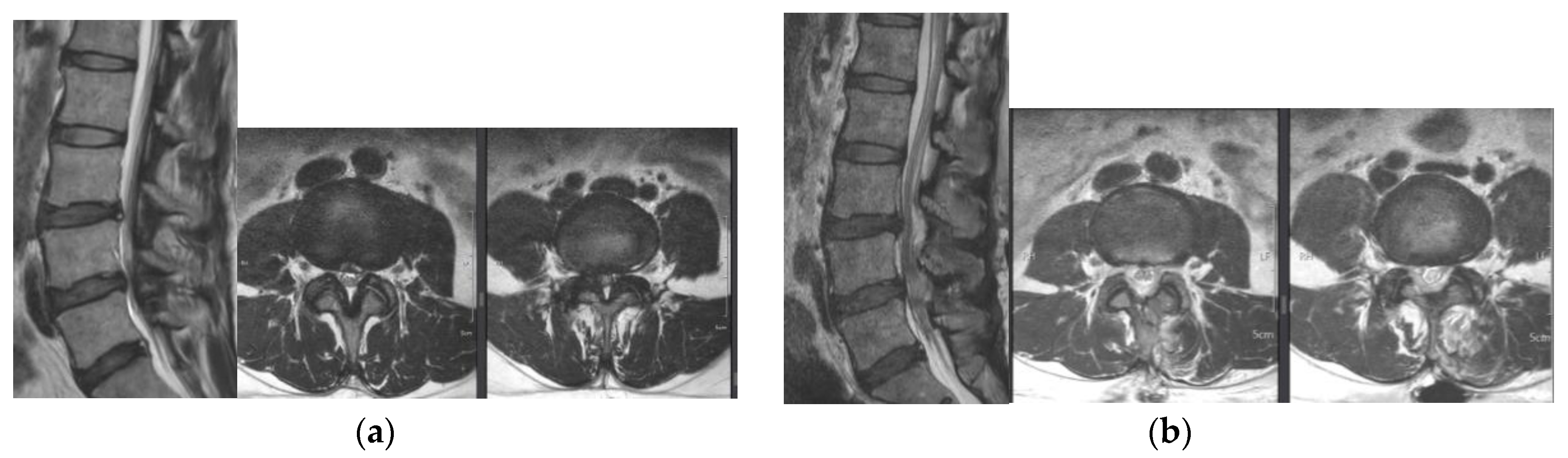
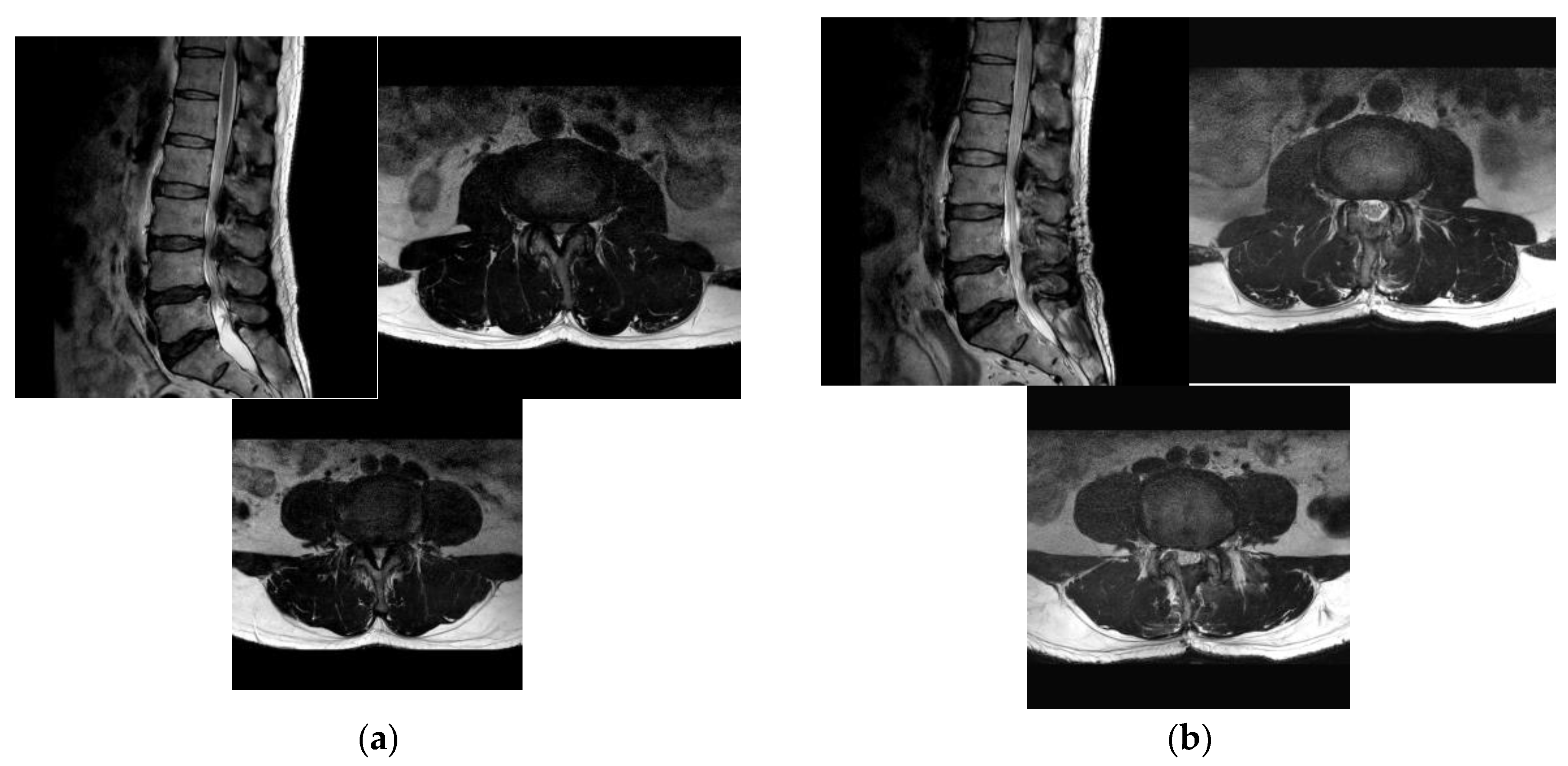
3.3. Radiologic Outcome Evaluation
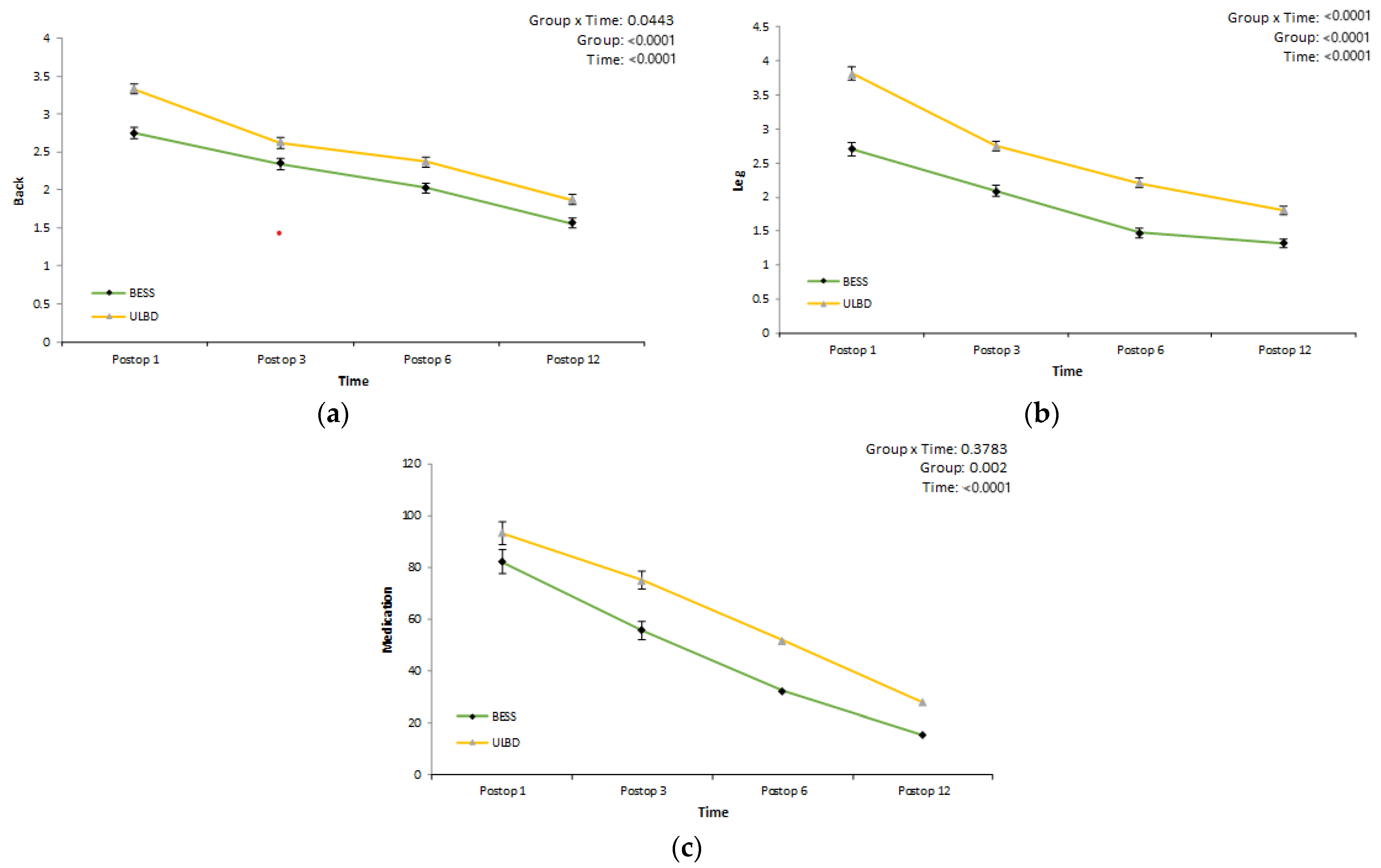
3.4. Clinical Outcome Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phan, K.; Mobbs, R.J. Minimally Invasive Versus Open Laminectomy for Lumbar Stenosis: A Systematic Review and Meta-Analysis. Spine 2016, 41, E91–E100. [Google Scholar] [CrossRef] [PubMed]
- Nerland, U.S.; Jakola, A.S.; Solheim, O.; Weber, C.; Rao, V.; Lønne, G.; Solberg, T.K.; Salvesen, Ø.; Carlsen, S.M.; Nygaard, Ø.P.; et al. Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: Pragmatic comparative effectiveness study. BMJ 2015, 350, h1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, S.; Hamad, A.; Bhalla, A.; Turner, S.; Balain, B.; Jaffray, D. The outcome of decompression alone for lumbar spinal stenosis with degenerative spondylolisthesis. Eur. Spine J. 2017, 26, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Lipson, S.J.; Lew, R.A.; Grobler, L.J.; Weinstein, J.N.; Brick, G.W.; Fossel, A.H.; Liang, M.H. Lumbar laminectomy alone or with instrumented or noninstrumented arthrodesis in degenerative lumbar spinal stenosis. Patient selection, costs, and surgical outcomes. Spine 1997, 22, 1123–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adilay, U.; Guclu, B. Comparison of Single-Level and Multilevel Decompressive Laminectomy for Multilevel Lumbar Spinal Stenosis. World Neurosurg. 2018, 111, e235–e240. [Google Scholar] [CrossRef]
- Yoshikane, K.; Kikuchi, K.; Okazaki, K. Clinical Outcomes of Selective Single-Level Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression of Multilevel Lumbar Spinal Stenosis and Risk Factors of Reoperation. Glob. Spine J. 2021, 21925682211033575. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.; Malone, H.; Keppetipola, K.M.; Deutsch, H.; Fessler, R.G.; Fontes, R.B.; O’Toole, J.E. Multilevel Minimally Invasive Lumbar Decompression: Clinical Efficacy and Durability to 2 Years. Int. J. Spine Surg. 2021, 15, 795–802. [Google Scholar] [CrossRef]
- Lim, K.T.; Nam, H.G.W.; Kim, S.B.; Kim, H.S.; Park, J.S.; Park, C.K. Therapeutic Feasibility of Full Endoscopic Decompression in One- to Three-Level Lumbar Canal Stenosis via a Single Skin Port Using a New Endoscopic System, Percutaneous Stenoscopic Lumbar Decompression. Asian Spine J. 2019, 13, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Schizas, C.; Theumann, N.; Burn, A.; Tansey, R.; Wardlaw, D.; Smith, F.W.; Kulik, G. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine 2010, 35, 1919–1924. [Google Scholar] [CrossRef] [Green Version]
- Soman, S.M.; Chokshi, J.; Chhatrala, N.; Tharadara, G.H.; Prabhakar, M. Qualitative Grading as a Tool in the Management of Multilevel Lumbar Spine Stenosis. Asian Spine J. 2017, 11, 278–284. [Google Scholar] [CrossRef]
- Amundsen, T.; Weber, H.; Nordal, H.J.; Magnaes, B.; Abdelnoor, M.; Lilleâs, F. Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000, 25, 1424–1435. [Google Scholar] [CrossRef] [PubMed]
- Sirvanci, M.; Bhatia, M.; Ganiyusufoglu, K.A.; Duran, C.; Tezer, M.; Ozturk, C.; Aydogan, M.; Hamzaoglu, A. Degenerative lumbar spinal stenosis: Correlation with Oswestry Disability Index and MR imaging. Eur. Spine J. 2008, 17, 679–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Konno, S.; Kikuchi, S. A histologic and functional study on cauda equina adhesion induced by multiple level laminectomy. Spine 2003, 28, 4–8. [Google Scholar] [CrossRef]
- Park, D.K.; An, H.S.; Lurie, J.D.; Zhao, W.; Tosteson, A.; Tosteson, T.D.; Herkowitz, H.; Errico, T.; Weinstein, J.N. Does multilevel lumbar stenosis lead to poorer outcomes? A subanalysis of the Spine Patient Outcomes Research Trial (SPORT) lumbar stenosis study. Spine 2010, 35, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, S.; Nagata, K.; Iwasaki, H.; Hashizume, H.; Yukawa, Y.; Minamide, A.; Nakagawa, Y.; Tsutsui, S.; Takami, M.; Taiji, R.; et al. Long-Term Outcomes after Selective Microendoscopic Laminotomy for Multilevel Lumbar Spinal Stenosis with and without Remaining Radiographic Stenosis: A 10-Year Follow-Up Study. Spine Surg. Relat. Res. 2022, 6, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, N.H.; Burgstaller, J.M.; Held, U.; Winklhofer, S.; Farshad, M.; Pichierri, G.; Steurer, J.; Porchet, F.; LSOS Study Group. The Influence of Single-level Versus Multilevel Decompression on the Outcome in Multisegmental Lumbar Spinal Stenosis: Analysis of the Lumbar Spinal Outcome Study (LSOS) Data. Clin. Spine Surg. 2017, 30, E1367–E1375. [Google Scholar] [CrossRef]
- Lee, C.H.; Choi, M.; Ryu, D.S.; Choi, I.; Kim, C.H.; Kim, H.S.; Sohn, M.J. Efficacy and Safety of Full-endoscopic Decompression via Interlaminar Approach for Central or Lateral Recess Spinal Stenosis of the Lumbar Spine: A Meta-analysis. Spine 2018, 43, 1756–1764. [Google Scholar] [CrossRef]
- Asgarzadie, F.; Khoo, L.T. Minimally invasive operative management for lumbar spinal stenosis: Overview of early and long-term outcomes. Orthop. Clin. N. Am. 2007, 38, 387–399. [Google Scholar] [CrossRef]
- Hong, S.W.; Choi, K.Y.; Ahn, Y.; Baek, O.K.; Wang, J.C.; Lee, S.H.; Lee, H.Y. A comparison of unilateral and bilateral laminotomies for decompression of L4-L5 spinal stenosis. Spine 2011, 36, E172–E178. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, T.; Herno, A.; Paljärvi, L.; Airaksinen, O.; Partanen, J.; Tapaninaho, A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine 1993, 18, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yagi, M.; Suzuki, S.; Takahashi, Y.; Nori, S.; Tsuji, O.; Nagoshi, N.; Ogawa, J.; Matsumoto, M.; Nakamura, M.; et al. Multilevel Decompression Surgery for Degenerative Lumbar Spinal Canal Stenosis Is Similarly Effective with Single-level Decompression Surgery. Spine 2022, 47, 1728–1736. [Google Scholar] [CrossRef] [PubMed]
- El-Abed, K.; Barakat, M.; Ainscow, D. Multilevel lumbar spinal stenosis decompression: Midterm outcome using a modified hinge osteotomy technique. J. Spinal Disord. Tech. 2011, 24, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Oertel, M.F.; Ryang, Y.M.; Korinth, M.C.; Gilsbach, J.M.; Rohde, V. Long-term results of microsurgical treatment of lumbar spinal stenosis by unilateral laminotomy for bilateral decompression. Neurosurgery 2006, 59, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Iqbal, A.; Manning, B.T.; Leblang, S.; Bohl, D.D.; Mayo, B.C.; Massel, D.H.; Singh, K. Minimally invasive lumbar decompression-the surgical learning curve. Spine J. 2016, 16, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Park, C.W.; Yeung, Y.K.; Suen, T.K.; Jun, S.G.; Park, J.H. Unilateral Bi-portal Endoscopic Decompression via the Contralateral Approach in Asymmetric Spinal Stenosis: A Technical Note. Asian Spine J. 2021, 15, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Pao, J.L.; Lin, S.M.; Chen, W.C.; Chang, C.H. Unilateral biportal endoscopic decompression for degenerative lumbar canal stenosis. J. Spine Surg. 2020, 6, 438–446. [Google Scholar] [CrossRef]
- Eguchi, Y.; Aoki, Y.; Yamashita, M.; Fujimoto, K.; Sato, T.; Abe, K.; Sato, M.; Yamanaka, H.; Toyoguchi, T.; Shimizu, K.; et al. Clinical Efficacy of Neurotropin for Lumbar Spinal Stenosis with Low Back Pain. Pain Ther. 2023, 12, 1–13. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (N = 95) | BESS (N = 47) | ULBD (N = 48) | p-Value | |
|---|---|---|---|---|
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Age | 68.716 ± 8.736 | 68.234 ± 11.040 | 69.188 ± 5.734 | 0.6002 |
| Gender | 0.1222 | |||
| F | 56 (58.95) | 24 (51.06) | 32 (66.67) | |
| M | 39 (41.05) | 23 (48.94) | 16 (33.33) | |
| Range of surgical levels | 0.7768 | |||
| 2 | 84 (88.42) | 42 (89.36) | 42 (87.50) | |
| 3 | 11 (11.58) | 5 (10.64) | 6 (12.50) | |
| Spondylolisthesis | 0.2372 | |||
| No | 66 (69.47) | 30 (63.83) | 36 (75.00) | |
| Yes | 29 (30.53) | 17 (36.17) | 12 (25.00) | |
| Scoliosis | 0.1586 | |||
| No | 87 (91.58) | 41 (87.23) | 46 (95.83) | |
| Yes | 8 (8.42) | 6 (12.77) | 2 (4.17) | |
| Post-operative complication | ||||
| No | 87 (91.58) | 44 (93.62) | 43 (89.58) | |
| Yes | 8 (8.42) | 3 (6.38) | 5 (10.42) |
| Total Level | ||||
| Total (N = 95) | BESS (N = 47) | ULBD (N = 48) | p-Value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Hospital day | 5.695 ± 1.963 | 4.426 ± 0.903 | 6.938 ± 1.929 | <0.0001 |
| Operation time (min) | 101.032 ± 22.401 | 111.660 ± 14.073 | 90.625 ± 24.212 | <0.0001 |
| Operation bleeding (cc) | 117.789 ± 56.567 | 92.553 ± 20.105 | 142.500 ± 68.874 | <0.0001 |
| Two Levels | ||||
| Total (N = 84) | BESS (N = 42) | ULBD (N = 42) | p-Value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Hospital day | 5.571 ± 1.947 | 4.357 ± 0.850 | 6.786 ± 1.982 | <0.0001 |
| Operation time (min) | 99.667 ± 21.949 | 111.619 ± 14.675 | 87.714 ± 21.616 | <0.0001 |
| Operation bleeding (cc) | 112.619 ± 55.599 | 88.333 ± 15.526 | 136.905 ± 69.343 | <0.0001 |
| Three Levels | ||||
| Total (N = 11) | BESS (N = 5) | ULBD (N = 6) | p-Value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Hospital day | 6.636 ± 1.912 | 5.000 ± 1.225 | 8.000 ± 1.095 | 0.0020 |
| Operation time (min) | 111.455 ± 24.147 | 112.000 ± 8.367 | 111.000 ± 33.311 | 0.9459 |
| Operation bleeding (cc) | 157.273 ± 49.818 | 128.000 ± 20.494 | 181.667 ± 55.287 | 0.0716 |
| Total | ||||
| Total (N = 205) | BESS (N = 99) | ULBD (N = 106) | p-Value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Expansion ratio of dural sac (%) | 189.546 ± 56.683 | 198.152 ± 64.297 | 181.509 ± 47.421 | 0.0374 |
| Ipsilateral Facet joint Preservation ratio (%) | 85.878 ± 7.097 | 91.192 ± 3.079 | 80.915 ± 6.126 | <0.0001 |
| Contralateral facet joint Preservation ratio (%) | 88.805 ± 7.076 | 93.374 ± 2.427 | 84.538 ± 7.329 | <0.0001 |
| Ipsilateral lateral recess angle increasing ratio (%) | 141.298 ± 22.254 | 151.737 ± 21.104 | 131.547 ± 18.648 | <0.0001 |
| Contralateral lateral recess angle Increasing ratio (%) | 142.366 ± 26.793 | 159.202 ± 19.954 | 126.642 ± 22.500 | <0.0001 |
| Two levels | ||||
| Total (N = 172) | BESS (N = 84) | ULBD (N = 88) | p-Value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Expansion ratio of dural sac (%) | 192.430 ± 59.008 | 204.881 ± 66.491 | 180.545 ± 48.306 | 0.0070 |
| Ipsilateral Facet joint Preservation ratio (%) | 85.657 ± 7.135 | 91.024 ± 3.208 | 80.534 ± 5.990 | <0.0001 |
| Contralateral facet joint Preservation ratio (%) | 88.843 ± 7.118 | 93.405 ± 2.425 | 84.489 ± 7.397 | <0.0001 |
| Ipsilateral lateral recess angle Increasing ratio (%) | 142.599 ± 22.565 | 151.583 ± 22.501 | 134.023 ± 19.117 | <0.0001 |
| Contralateral lateral recess angle Increasing ratio (%) | 142.436 ± 26.297 | 159.226 ± 20.009 | 126.409 ± 21.102 | <0.0001 |
| Three levels | ||||
| Total (N = 33) | BESS (N = 15) | ULBD (N = 18) | p-value | |
| Mean ± SD or N (%) | Mean ± SD or N (%) | Mean ± SD or N (%) | ||
| Expansion ratio of dural sac (%) | 174.515 ± 39.978 | 160.467 ± 30.577 | 186.222 ± 43.809 | 0.0443 |
| Ipsilateral Facet joint Preservation ratio (%) | 87.030 ± 6.890 | 92.133 ± 2.066 | 82.778 ± 6.612 | <0.0001 |
| Contralateral facet joint Preservation ratio (%) | 88.606 ± 6.955 | 93.200 ± 2.513 | 84.778 ± 7.191 | 0.0001 |
| Ipsilateral lateral recess angle Increasing ratio (%) | 134.515 ± 19.487 | 152.600 ± 10.736 | 119.444 ± 9.532 | <0.0001 |
| Contralateral lateral recess angle Increasing ratio (%) | 142.000 ± 29.678 | 159.067 ± 20.335 | 127.778 ± 29.091 | 0.0014 |
| Back | ||||
| Time | Group = BESS (0) Estimated Mean (SE) | Group = ULBD (1) Estimated Mean (SE) | Effect | Overall p-Value |
| Postop 1 month | 2.749(0.070) | 3.329(0.069) | Group | <0.0001 |
| Postop 3 month | 2.345(0.072) | 2.621(0.071) | Time | <0.0001 |
| Postop 6 month | 2.026(0.065) | 2.371(0.064) | Group*time | 0.0443 |
| Postop 12 month | 1.558(0.067) | 1.871(0.067) | ||
| Leg | ||||
| Time | Group = BESS (0) Estimated Mean (SE) | Group = ULBD (1) Estimated Mean (SE) | Effect | Overall p-Value |
| Postop 1 month | 2.706(0.098) | 3.809(0.097) | Group | <0.0001 |
| Postop 3 month | 2.089(0.077) | 2.746(0.076) | Time | <0.0001 |
| Postop 6 month | 1.472(0.075) | 2.205(0.074) | Group*time | <0.0001 |
| Postop 12 month | 1.323(0.063) | 1.809(0.062) | ||
| Medication (mg) | ||||
| Time | Group = BESS (0) Estimated Mean (SE) | Group = ULBD (1) Estimated Mean (SE) | Effect | Overall p-Value |
| Postop 1 month | 82.303(3.089) | 93.370(3.057) | Group | 0.002 |
| Postop 3 month | 55.707(5.795) | 75.141(5.734) | Time | <0.0001 |
| Postop 6 month | 32.303(4.468) | 51.703(4.422) | Group*time | 0.0378 |
| Postop 12 month | 15.282(3.425) | 27.745(3.389) | ||
| Total | ||||
| BESS (N = 47) | ULBD (N = 48) | Difference (SE) | p-Value | |
| Estimated Mean (SE) | Estimated Mean (SE) | |||
| Post-Op ODI | 18.258(0.581) | 19.851(0.575) | −1.593(0.819) | 0.0548 |
| Two levels | ||||
| BESS (N = 47) | ULBD (N = 48) | Difference (SE) | p-Value | |
| Estimated Mean (SE) | Estimated Mean (SE) | |||
| Post-Op ODI | 18.099(0.0.612) | 19.973(0.612) | −1.874(0.867) | 0.0335 |
| Three levels | ||||
| BESS (N = 47) | ULBD (N = 48) | Difference (SE) | p-Value | |
| Estimated Mean (SE) | Estimated Mean (SE) | |||
| Post-Op ODI | 18.998(2.030) | 19.502(1.830) | −0.503(2.918) | 0.8673 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eun, D.-C.; Lee, Y.-H.; Park, J.-O.; Suk, K.-S.; Kim, H.-S.; Moon, S.-H.; Park, S.-Y.; Lee, B.-H.; Park, S.-J.; Kwon, J.-W.; et al. A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients. J. Clin. Med. 2023, 12, 1033. https://doi.org/10.3390/jcm12031033
Eun D-C, Lee Y-H, Park J-O, Suk K-S, Kim H-S, Moon S-H, Park S-Y, Lee B-H, Park S-J, Kwon J-W, et al. A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients. Journal of Clinical Medicine. 2023; 12(3):1033. https://doi.org/10.3390/jcm12031033
Chicago/Turabian StyleEun, Dong-Chan, Yong-Ho Lee, Jin-Oh Park, Kyung-Soo Suk, Hak-Sun Kim, Seong-Hwan Moon, Si-Young Park, Byung-Ho Lee, Sang-Jun Park, Ji-Won Kwon, and et al. 2023. "A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients" Journal of Clinical Medicine 12, no. 3: 1033. https://doi.org/10.3390/jcm12031033
APA StyleEun, D. -C., Lee, Y. -H., Park, J. -O., Suk, K. -S., Kim, H. -S., Moon, S. -H., Park, S. -Y., Lee, B. -H., Park, S. -J., Kwon, J. -W., & Park, S. -R. (2023). A Comparative Analysis of Bi-Portal Endoscopic Spine Surgery and Unilateral Laminotomy for Bilateral Decompression in Multilevel Lumbar Stenosis Patients. Journal of Clinical Medicine, 12(3), 1033. https://doi.org/10.3390/jcm12031033