
Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease

 , , , , , , , , , , ,
, , , , , , , , , , ,  , , and add
Show full author list
, , and add
Show full author list
Abstract
:1. Introduction
2. Material and Methods
PD Patient Assessment
3. Data Analysis
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Activities For Daily Living | ADL |
| Schwab and England Activities of Daily Living Scale | ADLS |
| Beck Depression Inventory-Ii | BDI-II |
| Caregiver Strain Index | CSI |
| Freezing Of Gait Questionnaire | FOGQ |
| Levodopa Equivalent Daily Dose | LEDD |
| Non-Motor Symptoms; Non-Motor Symptoms Scale | NMS |
| Neuropsychiatric Inventory | NPI |
| Parkinson’s Disease | PD |
| Parkinson’s Disease Cognitive Rating Scale | PD-CRS |
| The 39-Item Parkinson’s Disease Questionnaire Summary Index | PDQ-39 |
| Parkinson’s Disease Sleep Scale | PDSS |
| Quality Of Life | QoL |
| Questionnaire For Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale | QUIP-RS |
| Unified Parkinson’s Disease Rating Scale | UPDRS |
| Visual Analogue Scale | VAS |
References
- Picillo, M.; Nicoletti, A.; Fetoni, V.; Garavaglia, B.; Barone, P.; Pellecchia, M.T. The relevance of gender in Parkinson’s disease: A review. J. Neurol. 2017, 264, 1583–1607. [Google Scholar] [CrossRef] [PubMed]
- Russillo, M.C.; Andreozzi, V.; Erro, R.; Picillo, M.; Amboni, M.; Cuoco, S.; Barone, P.; Pellecchia, M.T. Sex Differences in Parkinson’s Disease: From Bench to Bedside. Brain Sci. 2022, 12, 917. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- A Haaxma, C.; Bloem, B.R.; Borm, G.F.; Oyen, W.J.G.; Leenders, K.L.; Eshuis, S.; Booij, J.; E Dluzen, D.; Horstink, M.W.I.M. Gender differences in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2007, 78, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; LaFontant, D.; Bressman, S.; Caspell-Garcia, C.; Coffey, C.; Cho, H.R.; Burghardt, E.L.; Dahodwala, N.; Saunders-Pullman, R.; Tanner, C.M.; et al. Sex-Related Longitudinal Change of Motor, Non-Motor, and Biological Features in Early Parkinson’s Disease. J. Park. Dis. 2022, 12, 421–436. [Google Scholar] [CrossRef]
- Baba, Y.; Putzke, J.D.; Whaley, N.R.; Wszolek, Z.K.; Uitti, R.J. Gender and the Parkinson’s disease phenotype. J. Neurol. 2005, 252, 1201–1205. [Google Scholar] [CrossRef]
- Liu, R.; Umbach, D.M.; Peddada, S.D.; Xu, Z.; Troster, A.I.; Huang, X.; Chen, H. Potential sex differences in non-motor symptoms in early drug-naïve Parkinson disease. Neurology 2015, 84, 2107–2115. [Google Scholar] [CrossRef]
- Martinez-Martin, P.A.P.; Pecurariu, C.F.; Odin, C.A.; van Hilten, J.; Antonini, A.; Rojo-Abuin, J.M.; Borges, V.; Trenkwalder, C.; Aarsland, D.; Brooks, D.; et al. Gender-related differences in the burden of non-motor symptoms in Parkinson’s disease. J. Neurol. 2012, 259, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Cholerton, B.; Johnson, C.O.; Fish, B.; Quinn, J.F.; Chung, K.A.; Peterson-Hiller, A.L.; Rosenthal, L.S.; Dawson, T.M.; Albert, M.S.; Hu, S.-C.; et al. Sex differences in progression to mild cognitive impairment and dementia in Parkinson’s disease. Park. Relat. Disord. 2018, 50, 29–36. [Google Scholar] [CrossRef]
- Szewczyk-Krolikowski, K.; Tomlinson, P.; Nithi, K.; Wade-Martins, R.; Talbot, K.; Ben-Shlomo, Y.; Hu, M.T. The influence of age and gender on motor and non-motor features of early Parkinson’s disease: Initial findings from the Oxford Parkinson Disease Center (OPDC) discovery cohort. Park. Relat. Disord. 2014, 20, 99–105. [Google Scholar] [CrossRef]
- Cerri, S.; Mus, L.; Blandini, F. Parkinson’s Disease in Women and Men: What’s the Difference? J. Park. Dis. 2019, 9, 501–515. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, B.; Dhamija, K.; Guru, P.; Sharma, S.S. Parkinson’s disease in women: Mechanisms underlying sex differences. Eur. J. Pharmacol. 2021, 895, 173862. [Google Scholar] [CrossRef] [PubMed]
- Göttgens, I.; van Halteren, A.D.; de Vries, N.M.; Meinders, M.J.; Ben-Shlomo, Y.; Bloem, B.R.; Darweesh, S.K.L.; Oertelt-Prigione, S. The Impact of Sex and Gender on the Multidisciplinary Management of Care for Persons With Parkinson’s Disease. Front. Neurol. 2020, 11, 576121. [Google Scholar] [CrossRef]
- Benito-Leon, J. Epidemiologia de la enfermedad de Parkinson en España y su contextualizacion mundial [Epidemiology of Parkinson’s disease in Spain and its contextualisation in the world]. Rev. Neurol. 2018, 66, 125–134. [Google Scholar] [PubMed]
- García-Ramos, R.; López Valdés, E.; Ballesteros, L.; Jesús, S.; Mir, P. The social impact of Parkinson’s disease in Spain: Report by the Spanish Foundation for the Brain. Neurologia 2016, 31, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Santos García, D.; Jesús, S.; Aguilar, M.; Planellas, L.L.; García Caldentey, J.; Caballol, N.; Legarda, I.; Hernández Vara, J.; Cabo, I.; López Manzanares, L.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015): An ongoing global Parkinson’s disease project about disease progression with more than 1000 subjects included. Results from the baseline evaluation. Eur. J. Neurol. 2019, 26, 1399–1407. [Google Scholar] [CrossRef]
- Santos-García, D.; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; Martínez-Martín, P.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global-clinical evaluations, serum biomarkers, genetic studies and neuroimaging-prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar]
- Daniel, S.E.; Lees, A.J. Parkinson’s Disease Society Brain Bank, London: Overview and research. J. Neural. Transm. Suppl. 1993, 39, 165–172. [Google Scholar]
- Fahn, S.; Elton, R.L.; Members of the UPDRS Development Committee. Unified Parkinson’s disease rating scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Chaudhuri, K.R.; Rojo, J.M.; Schapira, A.; Brooks, D.; Stocchi, F.; Odin, P.; Antonini, A.; Brown, R.; Martinez-Martin, P. A Proposal for a Comprehensive Grading of Parkinson’s Disease Severity Combining Motor and Non-Motor Assessments: Meeting an Unmet Need. PLoS ONE 2013, 8, e57221. [Google Scholar] [CrossRef]
- Giladi, N.; Shabtai, H.; Simon, E.S.; Biran, S.; Tal, J.; Korczyn, A.D. Construction of freezing of gait questionnaire for patients with Parkinsonism. Park. Relat. Disord. 2000, 6, 165–170. [Google Scholar] [CrossRef]
- Santos-García, D.; on behalf of the COPPADIS Study Group; de Deus-Fonticoba, T.; Castro, E.S.; Díaz, M.A.; Feal-Painceiras, M.J.; Paz-González, J.M.; García-Sancho, C.; Jesús, S.; Mir, P.; et al. The impact of freezing of gait on functional dependency in Parkinson’s disease with regard to motor phenotype. Neurol. Sci. 2020, 41, 2883–2892. [Google Scholar] [CrossRef]
- Jankovic, J.; McDermott, M.; Carter, J.; Gauthier, S.; Goetz, C.; Golbe, L.; Huber, S.; Koller, W.; Olanow, C.; Shoulson, I.; et al. Variable expression of Parkinson’s disease: A base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 1990, 40, 1529–1534. [Google Scholar] [CrossRef]
- García, D.S.; Canfield, H.; Fonticoba, T.D.D.; Bartolomé, C.C.; Ríos, L.N.; Roca, L.G.; Miró, C.M.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Parkinson’s Disease Motor Subtypes Change with the Progression of the Disease: Results from the COPPADIS Cohort at 2-Year Follow-Up. J. Park. Dis. 2021, Preprint, 1–21. [Google Scholar] [CrossRef]
- Fernandez de Bobadilla, R.; Pagonabarraga, J.; Martinez-Horta, S.; Pascual-Sedano, B.; Campolongo, A.; Kulisevsky, J. Parkinson’s disease-cognitive rating scale: Psychometrics for mild cognitive impairment. Mov. Disord. 2013, 28, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Horta, S.; Bejr-Kasem, H.; Horta-Barba, A.; Pascual-Sedano, B.; Santos-García, D.; de Deus-Fonticoba, T.; Jesús, S.; Aguilar, M.; Planellas, L.; García-Caldentey, J.; et al. Identifying comorbidities and lifestyle factors contributing to the cognitive profile of early Parkinson’s disease. BMC Neurol. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Santos-García, D.; Fonticoba, T.D.D.; Bartolomé, C.C.; Castro, E.S.; Jesús, S.; Mir, P.; Pascual-Sedano, B.; Pagonabarraga, J.; Kulisevsky, J.; Hernández-Vara, J.; et al. Depression is Associated with Impulse-compulsive Behaviors in Parkinson’s disease. J. Affect. Disord. 2020, 280, 77–89. [Google Scholar] [CrossRef]
- Weintraub, D.; Mamikonyan, E.; Papay, K.; Shea, J.A.; Xie, S.X.; Siderowf, A. Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale. Mov. Disord. 2012, 27, 242–247. [Google Scholar] [CrossRef]
- Jesús, S.; Labrador-Espinosa, M.A.; Adarmes, A.D.; Barrio, C.M.-D.; Martínez-Castrillo, J.C.; Alonso-Cánovas, A.; Alonso, P.S.; Novo-Ponte, S.; Alonso-Losada, M.G.; Ariztegui, N.L.; et al. Non-motor symptom burden in patients with Parkinson’s disease with impulse control disorders and compulsive behaviours: Results from the COPPADIS cohort. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pract. 2020, 7, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, I.; Mathur, S.; Oosterbaan, A.; Flanagan, R.; Keener, A.M.; Moro, E. Unmet Needs of Women Living with Parkinson’s Disease: Gaps and Controversies. Mov. Disord. 2022, 37, 444–455. [Google Scholar] [CrossRef]
- Nwabuobi, L.; Barbosa, W.; Sweeney, M.; Oyler, S.; Meisel, T.; Di Rocco, A.; Chodosh, J.; E Fleisher, J. Sex-related differences in homebound advanced Parkinson’s disease patients. Clin. Interv. Aging 2019, ume 14, 1371–1377. [Google Scholar] [CrossRef]
- Nag, N.; Jelinek, G.A. A Narrative Review of Lifestyle Factors Associated with Parkinson’s Disease Risk and Progression. Neurodegener. Dis. 2019, 19, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Augustine, E.F.; Perez, A.; Dhall, R.; Umeh, C.C.; Videnovic, A.; Cambi, F.; Wills, A.-M.A.; Elm, J.J.; Zweig, R.M.; Shulman, L.M.; et al. Sex Differences in Clinical Features of Early, Treated Parkinson’s Disease. PLoS ONE 2015, 10, e0133002. [Google Scholar] [CrossRef]
- Crispino, P.; Gino, M.; Barbagelata, E.; Ciarambino, T.; Politi, C.; Ambrosino, I.; Ragusa, R.; Marranzano, M.; Biondi, A.; Vacante, M. Gender Differences and Quality of Life in Parkinson’s Disease. Int. J. Environ. Res. Public Health 2020, 18, 198. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M. Gender differences in Parkinson’s disease. Gend. Med. 2007, 4, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.N.; Cronin-Golomb, A. Gender differences in Parkinson’s disease: Clinical characteristics and cognition. Mov. Disord. 2010, 25, 2695–2703. [Google Scholar] [CrossRef]
- Georgiev, D.; Hamberg, K.; Hariz, M.; Forsgren, L.; Hariz, G.M. Gender differences in Parkinson’s disease: A clinical perspective. Acta Neurol. Scand. 2017, 136, 570–584. [Google Scholar] [CrossRef]
- Shin, J.Y.; Pohlig, R.T.; Habermann, B. Self-Reported Symptoms of Parkinson’s Disease by Sex and Disease Duration. West. J. Nurs. Res. 2017, 39, 1412–1428. [Google Scholar] [CrossRef]
- Pellecchia, M.T.; Picillo, M.; Russillo, M.C.; De Pandis, M.F.; Bonizzoni, E.; Marjanovic, I.; Cattaneo, C. Efficacy of Safinamide and Gender Differences During Routine Clinical Practice. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef]
- Parashos, S.A.; Bloem, B.R.; Browner, N.M.; Giladi, N.; Gurevich, T.; Hausdorff, J.M.; He, Y.; Lyons, K.E.; Mari, Z.; Morgan, J.C.; et al. What predicts falls in Parkinson disease?: Observations from the Parkinson’s Foundation registry. Neurol. Clin. Pract. 2018, 8, 214–222. [Google Scholar] [CrossRef]
- Rusz, J.; Tykalová, T.; Novotný, M.; Zogala, D.; Růžička, E.; Dušek, P. Automated speech analysis in early untreated Parkinson’s disease: Relation to gender and dopaminergic transporter imaging. Eur. J. Neurol. 2022, 29, 81–90. [Google Scholar] [CrossRef]
- Ricciardi, L.; De Angelis, A.; Marsili, L.; Faiman, I.; Pradhan, P.; Pereira, E.A.; Edwards, M.J.; Morgante, F.; Bologna, M. Hypomimia in Parkinson’s disease: An axial sign responsive to levodopa. Eur. J. Neurol. 2020, 27, 2422–2429. [Google Scholar] [CrossRef]
- Ou, R.; Liu, H.; Hou, Y.; Song, W.; Cao, B.; Wei, Q.; Yuan, X.; Chen, Y.; Zhao, B.; Shang, H. Predictors of camptocormia in patients with Parkinson’s disease: A prospective study from southwest China. Park. Relat. Disord. 2018, 52, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.W.; Choi, S.M.; Kim, B.C. Gender differences in motor and non-motor symptoms in early Parkinson disease. Medicine 2022, 101, e28643. [Google Scholar] [CrossRef]
- Abraham, D.S.; Gruber-Baldini, A.L.; Magder, L.S.; McArdle, P.F.; Tom, S.E.; Barr, E.; Schrader, K.; Shulman, L.M. Sex differences in Parkinson’s disease presentation and progression. Park. Relat. Disord. 2019, 69, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Reinoso, G.; Allen, J.C., Jr.; Au, W.L.; Seah, S.H.; Tay, K.Y.; Tan, L.C. Clinical evolution of Parkinson’s disease and prognostic factors affecting motor progression: 9-year follow-up study. Eur. J. Neurol. 2015, 22, 457–463. [Google Scholar] [CrossRef]
- Sieber, B.A.; Landis, S.; Koroshetz, W.; Bateman, R.; Siderowf, A.; Galpern, W.R.; Montine, T.J.; Orr, H.T.; Torborg, C.; Montine, T.J.; et al. arkinson’s Disease 2014: Advancing Research, Improving Lives Conference Organizing Committee. Prioritized research recommendations from the National Institute of Neurological Disorders and Stroke Parkinson’s Disease 2014 Conference. Ann. Neurol. 2014, 76, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Colombo, D.; Abbruzzese, G.; Antonini, A.; Barone, P.; Bellia, G.; Franconi, F.; Simoni, L.; Attar, M.; Zagni, E.; Haggiag, S.; et al. The “gender factor” in wearing-off among patients with Parkinson’s disease: A post hoc analysis of DEEP study. Sci. World J. 2015, 2015, 787451. [Google Scholar] [CrossRef]
- Wan, Z.; Wang, X.; Ma, H.; Wang, Z.; Feng, T. Risk factors for motor complications in female patients with Parkinson’s disease. Neurol. Sci. 2022, 43, 4735–4743. [Google Scholar] [CrossRef] [PubMed]
- Andreasi, N.G.; Romito, L.M.; Telese, R.; Cilia, R.; Elia, A.E.; Novelli, A.; Tringali, G.; Messina, G.; Levi, V.; Devigili, G.; et al. Short- and long-term motor outcome of STN-DBS in Parkinson’s Disease: Focus on sex differences. Neurol. Sci. 2021, 43, 1769–1781. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Palladino, R.; Moccia, M.; Erro, R.; Amboni, M.; Vitale, C.; Barone, P.; Pellecchia, M.T. Gender and non motor fluctuations in Parkinson’s disease: A prospective study. Park. Relat. Disord. 2016, 27, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Farhadi, F.; Vosoughi, K.; Shahidi, G.A.; Delbari, A.; Lökk, J.; Fereshtehnejad, S.M. Sexual dimorphism in Parkinson’s disease: Differences in clinical manifestations, quality of life and psychosocial functioning between males and females. Neuropsychiatr. Dis. Treat. 2017, 13, 329–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrin, A.J.; Nosova, E.; Co, K.; Book, A.; Iu, O.; Silva, V.; Thompson, C.; McKeown, M.; Stoessl, A.J.; Farrer, M.J.; et al. Gender differences in Parkinson’s disease depression. Park. Relat. Disord. 2017, 36, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Fullard, M.E.; Thibault, D.P.; Todaro, V.; Foster, S.; Katz, L.; Morgan, R.; Kern, D.S.; Schwalb, J.M.; Mendoza, E.U.; Dahodwala, N.; et al. Sex disparities in health and health care utilization after Parkinson diagnosis: Rethinking PD associated disability. Park. Relat. Disord. 2017, 48, 45–50. [Google Scholar] [CrossRef]
- Defazio, G.; Antonini, A.; Tinazzi, M.; Gigante, A.F.; Pietracupa, S.; Pellicciari, R.; Bloise, M.; Bacchin, R.; Marcante, A.; Fabbrini, G.; et al. Relationship between pain and motor and non-motor symptoms in Parkinson’s disease. Eur. J. Neurol. 2017, 24, 974–980. [Google Scholar] [CrossRef]
- Guo, X.; Song, W.; Chen, K.; Chen, X.; Zheng, Z.; Cao, B.; Huang, R.; Zhao, B.; Wu, Y.; Shang, H.-F. Gender and onset age-related features of non-motor symptoms of patients with Parkinson’s disease – A study from Southwest China. Park. Relat. Disord. 2013, 19, 961–965. [Google Scholar] [CrossRef]
- Silverdale, M.A.; Kobylecki, C.; Kass-Iliyya, L.; Martinez-Martin, P.; Lawton, M.; Cotterill, S.; Chaudhuri, K.R.; Morris, H.; Baig, F.; Williams, N.; et al. A detailed clinical study of pain in 1957 participants with early/moderate Parkinson’s disease. Park. Relat. Disord. 2018, 56, 27–32. [Google Scholar] [CrossRef]
- Hu, T.; Ou, R.; Liu, H.; Hou, Y.; Wei, Q.; Song, W.; Cao, B.; Chen, Y.; Yuan, X.; Shang, H. Gender and onset age related-differences of non-motor symptoms and quality of life in drug-naïve Parkinson’s disease. Clin. Neurol. Neurosurg. 2018, 175, 124–129. [Google Scholar] [CrossRef]
- Solla, P.; Cannas, A.; Ibba, F.C.; Loi, F.; Corona, M.; Orofino, G.; Marrosu, M.G.; Marrosu, F. Gender differences in motor and non-motor symptoms among Sardinian patients with Parkinson’s disease. J. Neurol. Sci. 2012, 323, 33–39. [Google Scholar] [CrossRef]
- Nicoletti, A.; Vasta, R.; Mostile, G.; Nicoletti, G.; Arabia, G.; Iliceto, G.; Lamberti, P.; Marconi, R.; Morgante, L.; Barone, P.; et al. Gender effect on non-motor symptoms in Parkinson’s disease: Are men more at risk? Park. Relat. Disord. 2017, 35, 69–74. [Google Scholar] [CrossRef]
- Picillo, M.; Erro, R.; Amboni, M.; Longo, K.; Vitale, C.; Moccia, M.; Pierro, A.; Scannapieco, S.; Santangelo, G.; Spina, E.; et al. Gender differences in non-motor symptoms in early Parkinson’s disease: A 2-years follow-up study on previously untreated patients. Park. Relat. Disord. 2014, 20, 850–854. [Google Scholar] [CrossRef]
- Gatto, E.M.; Aldinio, V. Impulse Control Disorders in Parkinson’s Disease. A Brief and Comprehensive Review. Front. Neurol. 2019, 10, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codling, D.; Shaw, P.; David, A.S. Hypersexuality in Parkinson’s Disease: Systematic Review and Report of 7 New Cases. Mov. Disord. Clin. Pract. 2015, 2, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Balash, Y.; Korczyn, A.D.; Migirov, A.A.; Gurevich, T. Quality of life in Parkinson’s disease: A gender-specific perspective. Acta Neurol. Scand. 2019, 140, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Meng, D.; Jin, Z.; Gao, L.; Wang, Y.; Wang, R.; Fang, J.; Qi, L.; Su, Y.; Liu, A.; Fang, B. The quality of life in patients with Parkinson’s disease: Focus on gender difference. Brain Behav. 2022, 12, e2517. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.-E.; Kim, J.S.; Jang, W.; Park, J.; Oh, E.; Youn, J.; Park, S.; Cho, J.W. Gender Differences of Nonmotor Symptoms Affecting Quality of Life in Parkinson Disease. Neurodegener. Dis. 2017, 17, 276–280. [Google Scholar] [CrossRef]
- Sperens, M.; Georgiev, D.; Eriksson Domellöf, M.; Forsgren, L.; Hamberg, K.; Hariz, G.M. Activities of daily living in Parkinson’s disease: Time/gender perspective. Acta Neurol. Scand. 2020, 141, 168–176. [Google Scholar] [CrossRef] [PubMed]
- García, D.S.; Fonticoba, T.D.D.; Cores, C.; Muñoz, G.; González, J.M.P.; Miró, C.M.; Suárez, E.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Predictors of clinically significant quality of life impairment in Parkinson’s disease. npj Park. Dis. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Schrag, A.; Sampaio, C.; Counsell, N.; Poewe, W. Minimal clinically important change on the unified Parkinson’s disease rating scale. Mov. Disord. 2006, 21, 1200–1207. [Google Scholar] [CrossRef]
- Gillies, G.E.; Pienaar, I.S.; Vohra, S.; Qamhawi, Z. Sex differences in Parkinson’s disease. Front. Neuroendocrinol. 2014, 35, 370–384. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Sample (n = 681) | Males (n = 410) | Females (n = 271) | p | |
|---|---|---|---|---|
| Age | 62.54 ± 8.93 | 62.36 ± 8.73 | 62.8 ± 9.24 | 0.297 |
| Education level (%): | 0.006 | |||
| -Primary | 42.1 | 38 | 48.1 | |
| -Secondary | 31.5 | 31.5 | 31.5 | |
| -University | 26.5 | 30.5 | 20.4 | |
| Civil status (%): | <0.0001 | |||
| -Married | 78.4 | 83.9 | 70 | |
| -Single | 7.1 | 4.4 | 11.1 | |
| -Widowed | 6.8 | 3.7 | 11.5 | |
| -Divorced | 6.6 | 6.8 | 6.3 | |
| -Other | 1.1 | 1.2 | 1.1 | |
| Living style (%): | <0.0001 | |||
| -With the partner | 79.3 | 85.1 | 70.4 | |
| -Alone | 10.7 | 7.6 | 15.6 | |
| -With a son/daughter | 5.3 | 2.7 | 9.3 | |
| -Other | 4.7 | 4.6 | 4.8 | |
| Habitat (%): | 0.438 | |||
| -Rural (<5.000) | 11.8 | 12.7 | 10.4 | |
| -Semiurban (5.000–20.000) | 18.9 | 17.6 | 43.8 | |
| -Urban (>20.000) | 69.4 | 69.8 | 68.8 | |
| Arterial hypertension (%) | 33.7 | 35.5 | 31 | 0.229 |
| Diabetes mellitus (%) | 9.1 | 10.3 | 7.4 | 0.200 |
| Dyslipidemia (%) | 30.1 | 30.1 | 30.3 | 0.959 |
| Cardiopathy (%) | 7.9 | 10 | 4.8 | 0.014 |
| Cardiac arrhythmia (%) | 5.1 | 5.9 | 4.1 | 0.296 |
| Smoking (%): | <0.0001 | |||
| -Smoker | 9.4 | 9.5 | 9.2 | |
| -Ex-smoker | 30 | 35.9 | 21 | |
| -Non-smoker | 60.6 | 54.5 | 69.8 | |
| Alcohol consumption (%): | <0.0001 | |||
| -Excessive drinker | 0.3 | 0.5 | 0 | |
| -Non-excessive drinker | 20.6 | 28.4 | 8.9 | |
| -Non-drinker | 79.1 | 71.1 | 91.1 | |
| To be receiving (%): | ||||
| -Antidepressant agent | 24.3 | 18.1 | 33.3 | <0.0001 |
| -Benzodiazepine | 16 | 11.2 | 23.2 | <0.0001 |
| -Antipsychotic | 2.2 | 3.2 | 0.7 | 0.034 |
| -Analgesic | 24.3 | 19.8 | 31 | 0.002 |
| Number of non-antiparkinsonian drugs | 2.58 ± 2.46 | 2.4 ± 2.36 | 2.86 ± 2.6 | 0.029 |
| Assistance to a patient association (%) | 14.1 | 12 | 17.4 | 0.047 |
| Speech therapy (%) | 11.3 | 11.5 | 11.2 | 0.925 |
| Physiotherapy (%) | 28 | 27.6 | 28.5 | 0.800 |
| Regular exercise (%) | 69.8 | 72.6 | 65.6 | 0.050 |
| Cognitive stimulation therapy (%) | 15.8 | 15.2 | 16.7 | 0.598 |
| All Sample (n = 681) | Males (n = 410) | Females (n = 271) | p | |
|---|---|---|---|---|
| Disease Treatments | ||||
| Years from symptoms onset | 5.48 ± 4.38 | 5.66 ± 4.65 | 5.21 ± 4.11 | 0.259 |
| To be receiving (%): | ||||
| -Levodopa | 72.2 | 73.5 | 70.1 | 0.337 |
| -DA | 68.8 | 72.1 | 63.8 | 0.024 |
| -MAO-B inhibitor | 73.5 | 77.2 | 67.9 | 0.007 |
| -COMT inhibitor | 18.6 | 20.3 | 16 | 0.160 |
| -Amantadine | 7.8 | 7.1 | 9 | 0.382 |
| Number of antiparkinsonian drugs | 2.43 ± 1.11 | 2.32 ± 1.09 | 2.51 ± 1.11 | 0.011 |
| Daily dose of levodopa (mg/day) | 346.13 ± 309.64 | 365.95 ± 319.73 | 316.44 ± 291.96 | 0.047 |
| DA equivalent daily dose (mg/day) | 167.49 ± 155.08 | 181.06 ± 159.41 | 147.17 ± 146.32 | 0.005 |
| LEDD (mg/day) | 566.13 ± 515.75 | 607.79 ± 432.61 | 503.71 ± 381.49 | 0.002 |
| Weight (kgs) | 75.77 ± 13.77 | 80.89 ± 11.84 | 68.04 ± 12.31 | <0.0001 |
| LEDD/Kgs | 7.64 ± 5.8 | 7.61 ± 5.5 | 6.69 ± 7.17 | 0.676 |
| Motor Symptoms | ||||
| HY stage (OFF) | 2 [2,2] | 2 [2,2] | 2 [1.5,2] | 0.810 |
| -Stage from 3 to 5 (%) | 9.5 | 8.9 | 10.4 | 0.521 |
| UPDRS-III (OFF) | 22.8 ± 11.21 | 23.24 ± 11.28 | 22.15 ± 11.1 | 0.265 |
| UPDRS-IV | 2.01 ± 2.41 | 1.94 ± 2.82 | 2.11 ± 2.58 | 0.994 |
| -Motor fluctuations (%) | 32.8 | 32.5 | 33.3 | 0.825 |
| -Dyskinesia (%) | 18.7 | 17.9 | 19.8 | 0.552 |
| FOGQ | 3.79 ± 4.59 | 3.79 ± 4.56 | 3.79 ± 4.58 | 0.994 |
| -FOG (%) | 34.5 | 35.1 | 33.6 | 0.680 |
| -Falls (%) | 13.1 | 10.6 | 16.7 | 0.022 |
| Tremoric motor phenotype (%) | 54.9 | 57.7 | 50.6 | 0.067 |
| Non-Motor Symptoms | ||||
| PD-CRS | 91.27 ± 15.83 | 91.24 ± 15.59 | 91.32 ± 16.21 | 0.974 |
| -Cognitive impairment (%) | 25.4 | 25.5 | 25.3 | 0.950 |
| NMSS | 45.26 ± 37.99 | 43.49 ± 36.89 | 47.94 ± 39.52 | 0.208 |
| -Very severe NMS burden (%) | 19.5 | 18.2 | 21.5 | 0.289 |
| BDI-II | 8.75 ± 7.34 | 7.95 ± 6.84 | 9.95 ± 7.89 | 0.001 |
| -Major depression (%) | 16.3 | 12 | 22.9 | <0.0001 |
| PDSS | 114.84 ± 26.99 | 115.27 ± 26.95 | 115.27 ± 26.95 | 0.408 |
| QUIP-RS | 4.33 ± 8.29 | 4.67 ± 8.56 | 3.83 ± 7.85 | 0.049 |
| -ICD and/or CB (%) | 17 | 17.4 | 16.3 | 0.703 |
| NPI | 6.06 ± 8.88 | 5.54 ± 7.23 | 6.86 ± 8.88 | 0.362 |
| VAS-PAIN | 2.62 ± 2.92 | 2.13 ± 2.62 | 3.37 ± 3.17 | <0.0001 |
| -Pain (%) | 57 | 51.7 | 64.9 | 0.001 |
| VAFS–physical | 2.95 ± 2.75 | 2.55 ± 2.58 | 3.57 ± 2.88 | <0.0001 |
| VAFS–mental | 2.16 ± 2.55 | 1.91 ± 2.34 | 2.54 ± 2.8 | 0.012 |
| Autonomy and QOL | ||||
| PDQ-39SI | 17.18 ± 13.56 | 16.05 ± 13.33 | 18.88 ± 13.76 | 0.002 |
| EUROHIS-QOL8 | 3.78 ± 0.55 | 3.82 ± 0.53 | 3.71 ± 0.56 | 0.009 |
| ADLS | 88.56 ± 10.45 | 88.76 ± 10.09 | 88.26 ± 10.98 | 0.835 |
| -Dependency for ADL (%) | 9 | 7.6 | 11.1 | 0.113 |
| All Sample (n = 681) | Males (n = 410) | Females (n = 271) | p | |
|---|---|---|---|---|
| Motor Symptoms | ||||
| UPDRS-III-Off | 22.8 ± 11.21 | 23.24 ± 11.28 | 22.15 ± 11.1 | 0.265 |
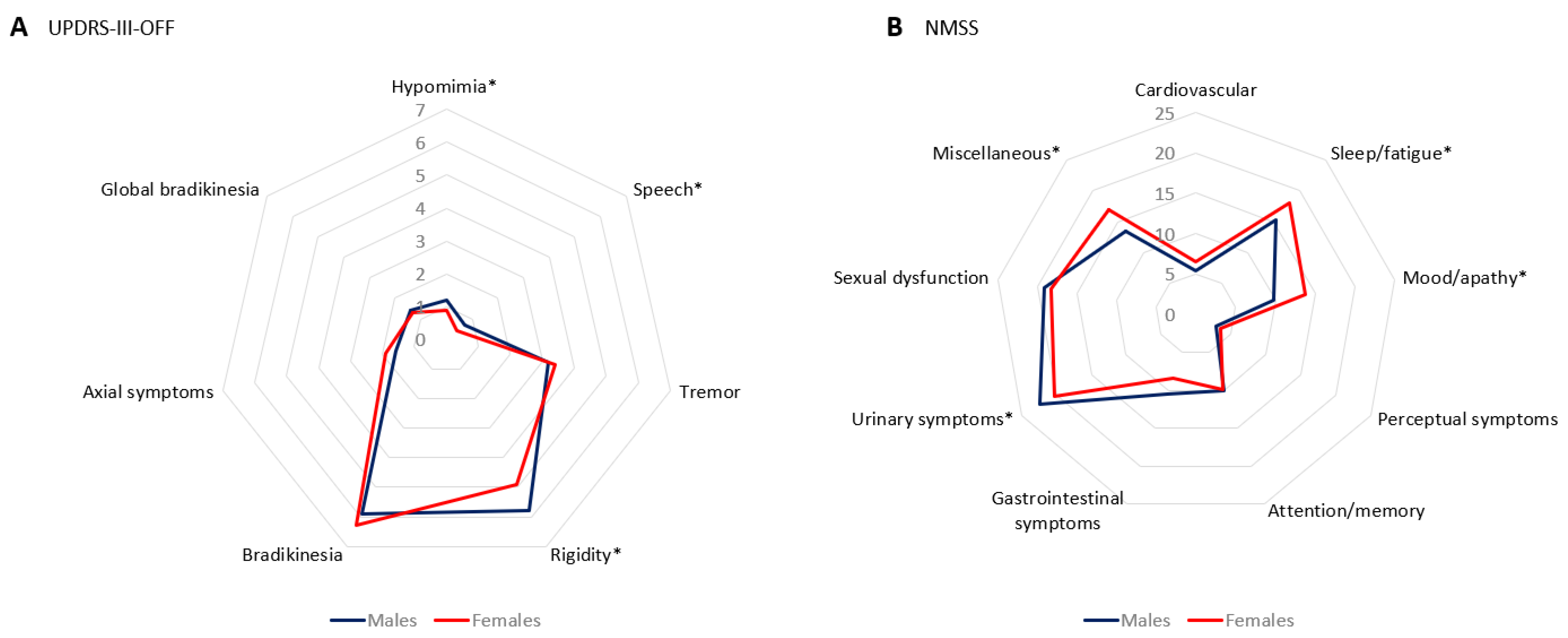
| Hypomimia | 1.16 ± 0.75 | 1.29 ± 0.76 | 0.96 ± 0.69 | <0.0001 |
| Speech | 0.64 ± 0.68 | 0.78 ± 0.71 | 0.43 ± 0.64 | <0.0001 |
| Tremor | 3.29 ± 3.15 | 3.2 ± 3.19 | 3.43 ± 3.09 | 0.226 |
| Rigidity | 5.5 ± 3.26 | 5.87 ± 3.3 | 4.95 ± 3.12 | <0.0001 |
| Bradykinesia | 6.11 ± 3.78 | 5.96 ± 3.7 | 6.32 ± 3.9 | 0.324 |
| Axial symptoms | 1.77 ± 1.86 | 1.67 ± 1.74 | 1.93 ± 2.04 | 0.613 |
| Global bradykinesia | 1.35 ± 0.9 | 1.36 ± 0.88 | 1.33 ± 0.92 | 0.777 |
| Non-Motor Symptoms | ||||
| PD-CRS total score | 91.27 ± 15.83 | 91.24 ± 15.59 | 91.32 ± 16.21 | 0.974 |
| PD-CRS FS sub-score | 63.67 ± 14.49 | 63.5 ± 14.52 | 63.93 ± 14.47 | 0.794 |
| Immediate verbal memory | 8.07 ± 2.1 | 7.91 ± 2.13 | 8.32 ± 2.03 | 0.007 |
| Sustained attention | 8.47 ± 1.89 | 8.56 ± 1.81 | 8.33 ± 2 | 0.160 |
| Working memory | 6.85 ± 2.4 | 7.07 ± 2.38 | 6.51 ± 2.38 | 0.003 |
| Clock drawing | 8.94 ± 1.69 | 8.96 ± 1.77 | 8.92 ± 1.57 | 0.499 |
| Delayed verbal memory | 5.54 ± 2.72 | 5.36 ± 2.64 | 5.81 ± 2.82 | 0.049 |
| Alternating verbal fluency | 11.25 ± 4.74 | 11.26 ± 4.4 | 11.25 ± 4.58 | 0.723 |
| Action verbal fluency | 14.59 ± 5.69 | 14.44 ± 5.85 | 14.8 ± 5.43 | 0.266 |
| PD-CRS PC sub-score | 27.6 ± 3.37 | 27.74 ± 3.31 | 27.39 ± 3.46 | 0.083 |
| Confrontation naming | 18.05 ± 3.06 | 18.23 ± 2.96 | 17.79 ± 3.19 | 0.012 |
| Clock copy | 9.55 ± 1.21 | 9.51 ± 1.29 | 9.6 ± 1.05 | 0.712 |
| NMSS | 45.26 ± 37.99 | 43.49 ± 36.89 | 47.94 ± 39.52 | 0.208 |
| Cardiovascular | 5.85 ± 10.21 | 5.41 ± 10.1 | 6.52 ± 10.36 | 0.137 |
| Sleep/fatigue | 16.42 ± 16.12 | 15.35 ± 15.63 | 18.03 ± 16.72 | 0.041 |
| Mood/apathy | 11.38 ± 16.45 | 9.79 ± 15.19 | 13.78 ± 17.96 | 0.003 |
| Perceptual symptoms | 3.13 ± 8.71 | 2.86 ± 7.98 | 3.52 ± 9.71 | 0.529 |
| Attention/memory | 9.97 ± 14.05 | 10 ± 14.13 | 9.92 ± 13.96 | 0.912 |
| Gastrointestinal symptoms | 9.69 ± 13.13 | 10.51 ± 13.9 | 8.46 ± 11.79 | 0.057 |
| Urinary symptoms | 21.61 ± 22.48 | 22.48 ± 22.22 | 20.29 ± 22.84 | 0.047 |
| Sexual dysfunction | 18.79 ± 25.69 | 19.1 ± 25.31 | 18.32 ± 26.3 | 0.201 |
| Miscellaneous | 14.92 ± 15.49 | 13.56 ± 14.49 | 16.98 ± 16.71 | 0.010 |
| QUIP-RS | ||||
| Any ICD and/or CB (%) | 17 | 17.4 | 16.3 | 0.703 |
| Any ICD (%) | 12.2 | 12.5 | 11.8 | 0.782 |
| Compulsive gambling (%) | 1.5 | 1.9 | 0.8 | 0.268 |
| Hypersexuality (%) | 4.7 | 7.6 | 0.4 | <0.0001 |
| Compulsive shopping (%) | 2.4 | 1.6 | 3.7 | 0.112 |
| Compulsive eating (%) | 6.7 | 5.2 | 8.9 | 0.067 |
| Any CB (%) | 9.3 | 9.3 | 9.3 | 0.972 |
| Hobbyism–punding (%) | 6.9 | 6.8 | 6.9 | 0.962 |
| Compulsive medication (%) | 3.8 | 3.8 | 3.7 | 0.921 |
| Quality of Life | ||||
| PDQ-39SI | 17.18 ± 13.56 | 16.05 ± 13.33 | 18.88 ± 13.76 | 0.002 |
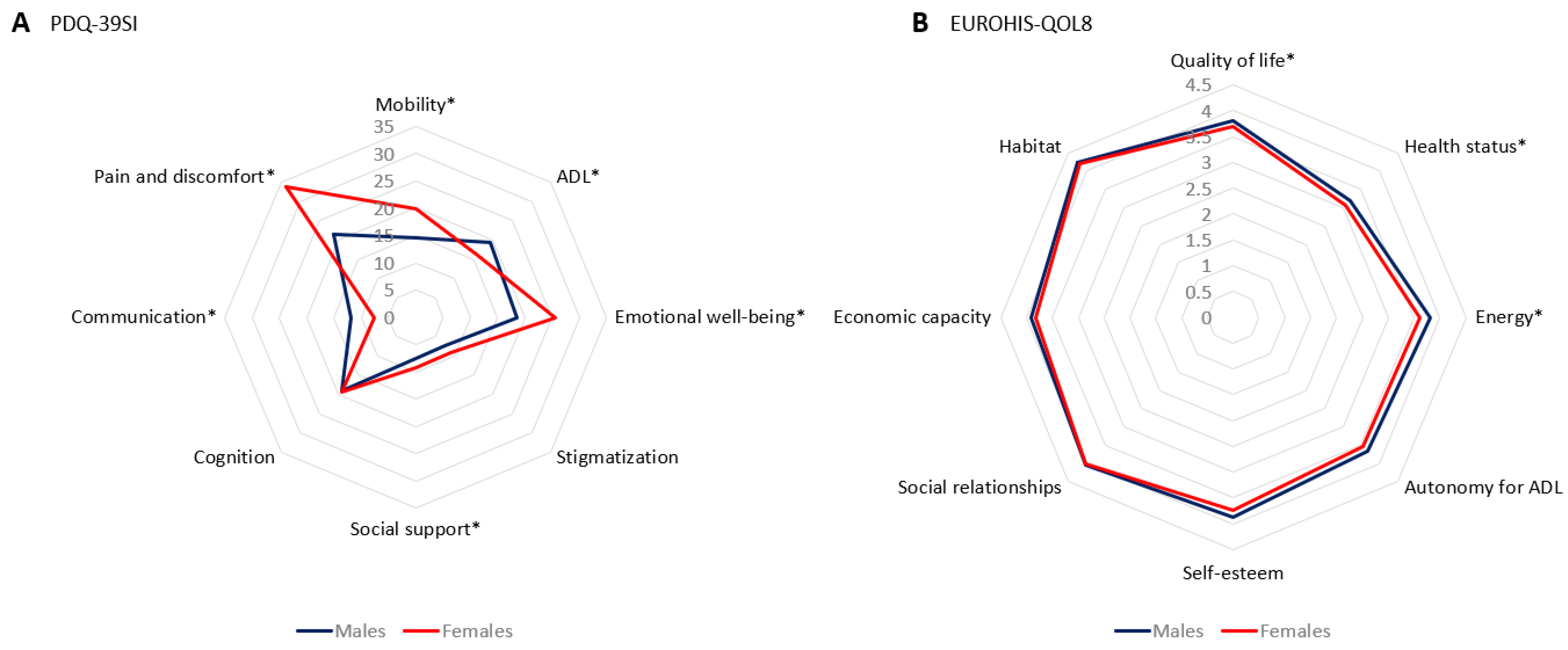
| Mobility | 16.69 ± 19.31 | 14.59 ± 17.88 | 19.87 ± 20.92 | 0.001 |
| Activities of daily living | 18.1 ± 18.71 | 19.41 ± 19.69 | 16.11 ± 16.98 | 0.034 |
| Emotional well-being | 21.4 ± 19.93 | 18.6 ± 18.72 | 25.64 ± 20.97 | <0.0001 |
| Stigmatization | 13.62 ± 19.57 | 13.1 ± 18.95 | 14.4 ± 20.49 | 0.665 |
| Social support | 8.21 ± 16.55 | 7.57 ± 16.88 | 9.18 ± 16.02 | 0.046 |
| Cognition | 19.22 ± 17.81 | 19.14 ± 17.51 | 19.33 ± 18.3 | 0.939 |
| Communication | 10.3 ± 15.34 | 11.99 ± 16.24 | 7.74 ± 13.52 | <0.0001 |
| Pain and discomfort | 26.36 ± 22.72 | 21.46 ± 20.2 | 33.76 ± 24.31 | <0.0001 |
| EUROHIS-QOL8 | 3.78 ± 0.55 | 3.82 ± 0.53 | 3.71 ± 0.56 | 0.009 |
| Quality of life | 3.8 ± 0.71 | 3.86 ± 0.7 | 3.73 ± 0.72 | 0.014 |
| Health status | 3.16 ± 0.88 | 3.23 ± 0.87 | 3.07 ± 0.87 | 0.020 |
| Energy | 3.76 ± 0.82 | 3.84 ± 0.77 | 3.65 ± 0.88 | 0.004 |
| Autonomy for ADL | 3.62 ± 0.86 | 3.66 ± 0.84 | 3.55 ± 0.89 | 0.062 |
| Self-esteem | 3.81 ± 0.81 | 3.87 ± 0.79 | 3.73 ± 0.84 | 0.054 |
| Social relationships | 4.04 ± 0.71 | 4.04 ± 0.72 | 4.03 ± 0.7 | 0.798 |
| Economic capacity | 3.86 ± 0.77 | 3.9 ± 0.78 | 3.81 ± 0.76 | 0.095 |
| Habitat | 4.23 ± 0.68 | 4.25 ± 0.68 | 4.21 ± 0.69 | 0.383 |
| Males V0 | Males V24M | Cohen’s | p a | Females V0 | Females V24M | Cohen’s | pb | pc | pd | |
|---|---|---|---|---|---|---|---|---|---|---|
| n = 294 | n = 294 | Test | n = 202 | n = 202 | Test | |||||
| Dose therapy | ||||||||||
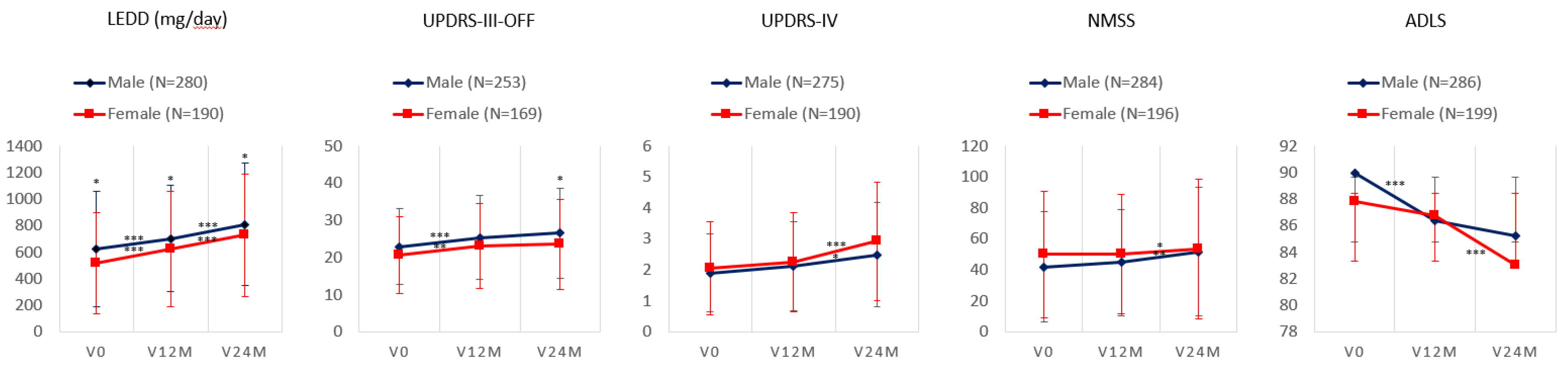
| LEDD (mg/day) | 625.25 ± 428.6 | 803.88 ± 455 | 0.73 | <0.0001 | 509.48 ± 381.37 | 719.22 ± 462.01 | 0.96 | <0.0001 | 0.249 | 0.007 |
| LEDD/weight | 7.61 ± 5.54 | 10.82 ± 6.07 | 0.87 | 0.131 | 7.69 ± 6.17 | 10.53 ± 7.51 | 0.71 | 0.005 | 0.859 | 0.706 |
| Motor Symptoms | ||||||||||
| UPDRS-III (OFF) | 22.84 ± 10.56 | 26.3 ± 12.01 | 0.56 | <0.0001 | 20.74 ± 10.38 | 23.76 ± 12.42 | 0.41 | <0.0001 | 0.686 | 0.554 |
| Hypomimia | 1.24 ± 0.72 | 1.35 ± 0.71 | 0.22 | 0.014 | 0.93 ± 0.66 | 0.99 ± 0.73 | 0.15 | 0.254 | 0.539 | <0.0001 |
| Speech | 0.72 ± 0.72 | 0.81 ± 0.75 | 0.13 | 0.032 | 0.4 ± 0.58 | 0.46 ± 0.64 | 0.04 | 0.084 | 0.808 | <0.0001 |
| Tremor | 3.3 ± 3.18 | 2.36 ± 2.62 | −0.47 | <0.0001 | 3.26 ± 0.21 | 2.41 ± 0.19 | −0.34 | <0.0001 | 0.889 | 0.763 |
| Rigidity | 5.83 ± 3.21 | 6.1 ± 3.62 | 0.17 | 0.131 | 4.76 ± 2.99 | 5.22 ± 3.19 | 0.18 | 0.030 | 0.514 | 0.018 |
| Bradykinesia | 5.86 ± 3.6 | 7.3 ± 4.19 | 0.55 | <0.0001 | 6.16 ± 3.76 | 7.02 ± 4.37 | 0.29 | 0.001 | 0.253 | 0.226 |
| Axial symptoms | 1.67 ± 1.76 | 3.03 ± 2.19 | 0.72 | <0.0001 | 2 ± 2.01 | 3.16 ± 2.31 | 0.41 | <0.0001 | 0.462 | 0.237 |
| Global bradykinesia | 1.37 ± 0.89 | 1.6 ± 0.93 | 0.39 | <0.0001 | 1.32 ± 0.92 | 1.46 ± 1.05 | 0.19 | 0.034 | 0.424 | 0.898 |
| UPDRS-IV | 1.91 ± 2.25 | 2.46 ± 2.64 | 0.31 | <0.0001 | 2.08 ± 2.6 | 2.94 ± 2.89 | 0.47 | <0.0001 | 0.164 | 0.105 |
| FOGQ | 3.65 ± 4.61 | 4.83 ± 5.17 | 0.43 | <0.0001 | 3.95 ± 4.85 | 4.97 ± 5.16 | 0.34 | 0.001 | 0.376 | 0.014 |
| Non-Motor Symptoms | ||||||||||
| PD-CRS | 91.61 ± 15.55 | 89.89 ± 17.22 | −0.21 | 0.011 | 92.4 ± 15.9 | 90.92 ± 19.35 | −0.15 | 0.068 | 0.886 | 0.615 |
| PD-CRS FS sub-score | 63.84 ± 14.29 | 61.99 ± 15.88 | −0.22 | 0.003 | 64.75 ± 14.44 | 63.2 ± 17.24 | −0.12 | 0.029 | 0.864 | 0.237 |
| PD-CRS PC sub-score | 27.98 ± 3.14 | 27.97 ± 2.9 | −0.03 | 0.950 | 27.55 ± 3.35 | 27.25 ± 3.5 | −0.11 | 0.200 | 0.449 | 0.021 |
| NMSS | 42.44 ± 35.81 | 52.25 ± 41.45 | 0.43 | <0.0001 | 48.99 ± 40.08 | 55.59 ± 43.88 | 0.25 | 0.013 | 0.469 | 0.012 |
| -Cardiovascular | 4.65 ± 8.82 | 11.73 ± 14.86 | 0.71 | <0.0001 | 6.58 ± 11.1 | 12.06 ± 13.26 | 0.57 | <0.0001 | 0.300 | 0.207 |
| -Sleep/fatigue | 14.71 ± 14.98 | 18.8 ± 17.84 | 0.33 | <0.0001 | 18.29 ± 16.65 | 19.83 ± 17.23 | 0.11 | 0.212 | 0.086 | 0.028 |
| -Mood/apathy | 9.2 ± 14.3 | 11.2 ± 16.77 | 0.33 | 0.015 | 14.2 ± 17.97 | 16 ± 19.49 | 0.1 | 0.159 | 0.934 | <0.0001 |
| -Perceptual symptoms | 2.98 ± 8.96 | 5.55 ± 13.29 | 0.37 | <0.0001 | 3.94 ± 10.39 | 5.43 ± 11.72 | 0.17 | 0.082 | 0.275 | 0.466 |
| -Attention/memory | 10.1 ± 14.84 | 12.59 ± 16.81 | 0.27 | 0.004 | 10.15 ± 14.65 | 12.68 ± 17.72 | 0.22 | 0.039 | 0.971 | 0.723 |
| -Gastrointestinal | 10.11 ± 13.76 | 11.82 ± 13.99 | 0.24 | 0.018 | 9.02 ± 12.51 | 12.67 ± 14.88 | 0.38 | <0.0001 | 0.123 | 0.984 |
| -Urinary symptoms | 22.35 ± 21.79 | 22.63 ± 22.44 | 0.02 | 0.109 | 21.02 ± 23.71 | 21.94 ± 23.36 | 0.11 | 0.517 | 0.237 | 0.493 |
| -Sexual dysfunction | 18.64 ± 24.96 | 24.77 ± 28.5 | 0.31 | <0.0001 | 19.04 ± 26.98 | 19.25 ± 26.27 | 0.02 | 0.821 | 0.101 | 0.219 |
| -Miscellaneous | 13.01 ± 14.06 | 14.39 ± 14.11 | 0.19 | 0.083 | 17.45 ± 17.12 | 18.77 ± 16.78 | 0.11 | 0.305 | 0.921 | <0.0001 |
| BDI-II | 7.34 ± 6.47 | 8.23 ± 7.23 | 0.16 | 0.043 | 9.52 ± 8.48 | 9.02 ± 7.92 | −0.08 | 0.417 | 0.062 | 0.003 |
| PDSS | 117.78 ± 24.3 | 117.71 ± 25.86 | −0.04 | 0.962 | 115.89 ± 25.13 | 117.97 ± 24.09 | 0.11 | 0.260 | 0.553 | 0.160 |
| QUIP-RS | 4.98 ± 9.21 | 5.12 ± 9.59 | 0.03 | 0.815 | 3.57 ± 6.98 | 3.63 ± 8.29 | 0.02 | 0.912 | 0.954 | 0.187 |
| NPI | 5.39 ± 7.52 | 5.51± 9.01 | 0.02 | 0.839 | 6.67 ± 8.64 | 7.27 ± 10.12 | 0.07 | 0.406 | 0.492 | 0.014 |
| VAS-PAIN | 2.11 ± 2.68 | 2.32 ± 2.59 | 0.12 | 0.240 | 3.31 ± 3.15 | 3.78 ± 2.99 | 0.15 | 0.079 | 0.398 | <0.0001 |
| VAFS–physical | 2.51 ± 2.54 | 2.77 ± 2.65 | 0.15 | 0.137 | 3.29 ± 2.82 | 3.68 ± 2.94 | 0.13 | 0.088 | 0.551 | <0.0001 |
| VAFS–mental | 1.86 ± 2.29 | 2.01 ± 2.45 | 0.11 | 0.353 | 2.39 ± 2.76 | 2.37 ± 2.79 | 0 | 0.937 | 0.005 | N. A. |
| Autonomy and QOL | ||||||||||
| PDQ-39SI | 15.37 ± 12.75 | 17.96 ± 15.45 | 0.32 | <0.0001 | 18.49 ± 13.45 | 23.27 ± 17.24 | 0.53 | <0.0001 | 0.027 | N. A. |
| EUROHIS-QOL8 | 3.82 ± 0.49 | 3.76 ± 0.56 | −0.13 | 0.063 | 3.69 ± 0.57 | 3.72 ± 0.61 | 0.07 | 0.046 | 0.040 | N. A. |
| ADLS | 89.12 ± 9.08 | 85.23 ± 12.58 | 0.49 | <0.0001 | 87.91 ± 11.42 | 82.76 ± 14.69 | 0.57 | <0.0001 | 0.176 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos-García, D.; Laguna, A.; Hernández-Vara, J.; de Deus Fonticoba, T.; Cores Bartolomé, C.; Feal Painceiras, M.J.; Íñiguez-Alvarado, M.C.; García Díaz, I.; Jesús, S.; Boungiorno, M.T.; et al. Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease. J. Clin. Med. 2023, 12, 1329. https://doi.org/10.3390/jcm12041329
Santos-García D, Laguna A, Hernández-Vara J, de Deus Fonticoba T, Cores Bartolomé C, Feal Painceiras MJ, Íñiguez-Alvarado MC, García Díaz I, Jesús S, Boungiorno MT, et al. Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease. Journal of Clinical Medicine. 2023; 12(4):1329. https://doi.org/10.3390/jcm12041329
Chicago/Turabian StyleSantos-García, Diego, Ariadna Laguna, Jorge Hernández-Vara, Teresa de Deus Fonticoba, Carlos Cores Bartolomé, Maria J. Feal Painceiras, Maria Cristina Íñiguez-Alvarado, Iago García Díaz, Silvia Jesús, Maria Teresa Boungiorno, and et al. 2023. "Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease" Journal of Clinical Medicine 12, no. 4: 1329. https://doi.org/10.3390/jcm12041329
APA StyleSantos-García, D., Laguna, A., Hernández-Vara, J., de Deus Fonticoba, T., Cores Bartolomé, C., Feal Painceiras, M. J., Íñiguez-Alvarado, M. C., García Díaz, I., Jesús, S., Boungiorno, M. T., Planellas, L., Cosgaya, M., García Caldentey, J., Caballol, N., Legarda, I., Cabo, I., López Manzanares, L., González Aramburu, I., Ávila Rivera, M. A., ... on behalf of the COPPADIS Study Group. (2023). Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease. Journal of Clinical Medicine, 12(4), 1329. https://doi.org/10.3390/jcm12041329