

Associations of Tinnitus Incidence with Use of Tumor Necrosis Factor-Alpha Inhibitors among Patients with Autoimmune Conditions
 and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Data Source
2.2. Study Populations and Study Periods
2.2.1. Overall Tinnitus Prevalence among All Adults
2.2.2. Incidence of Tinnitus among Adults with Autoimmune Disorders, Who Did or Did Not Receive Anti-TNFα
2.3. Outcomes
Handling of Missing Data
2.4. Covariates and PS Matching
2.5. Statistical Analyses
3. Results
3.1. Sample Selection
3.1.1. Tinnitus Prevalence Cohorts
3.1.2. Tinnitus Incidence Cohorts
3.2. Demographic and Clinical Characteristics
3.2.1. Tinnitus Prevalence Cohort
3.2.2. Tinnitus Incidence Cohorts
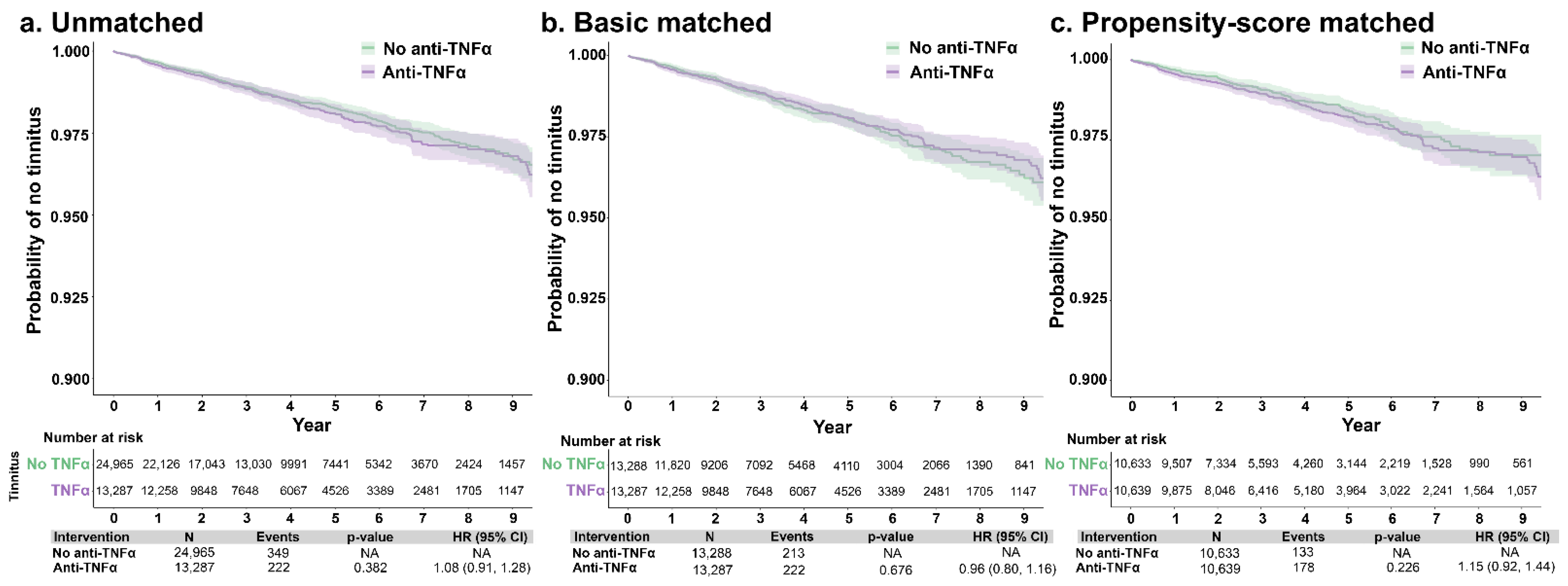
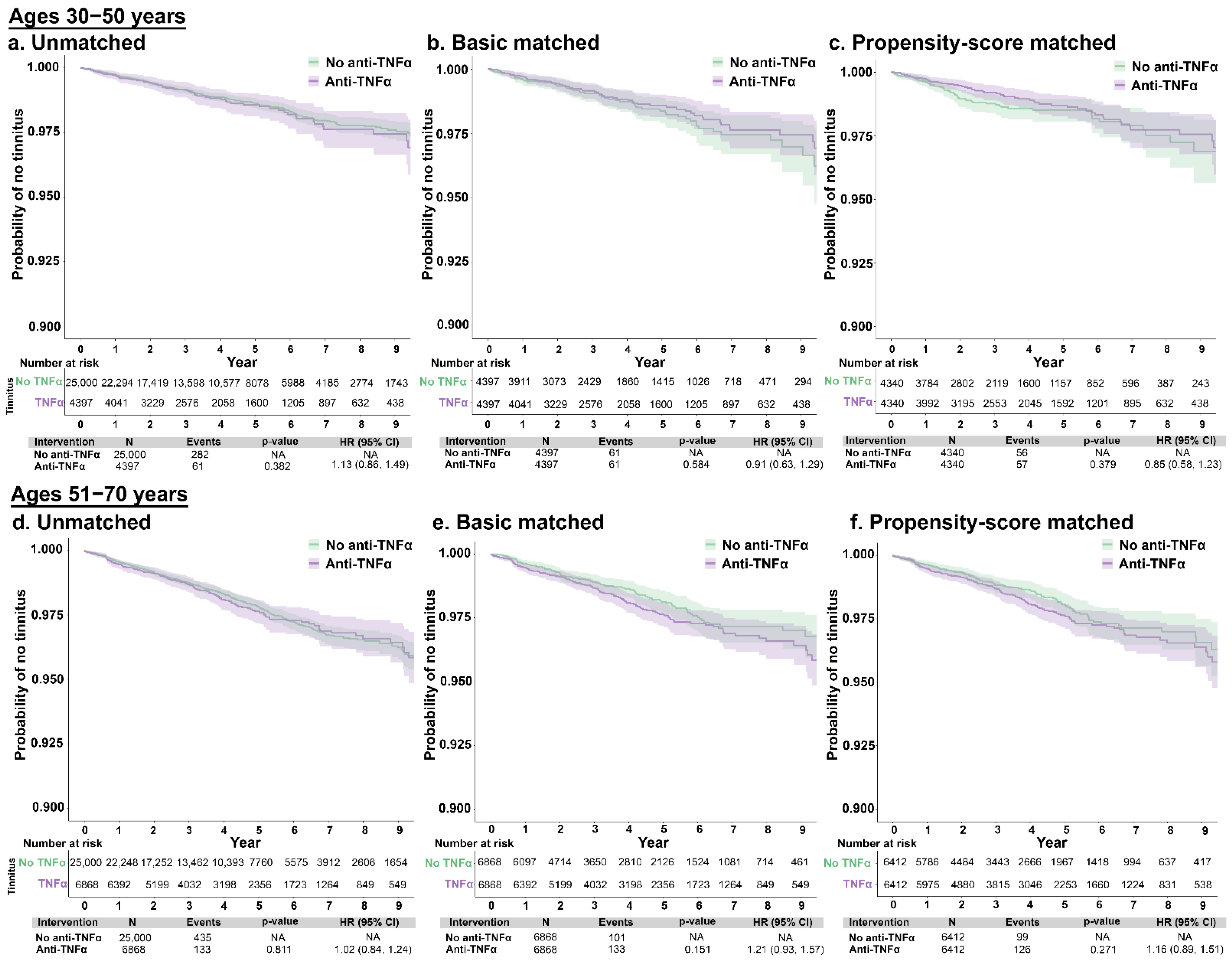
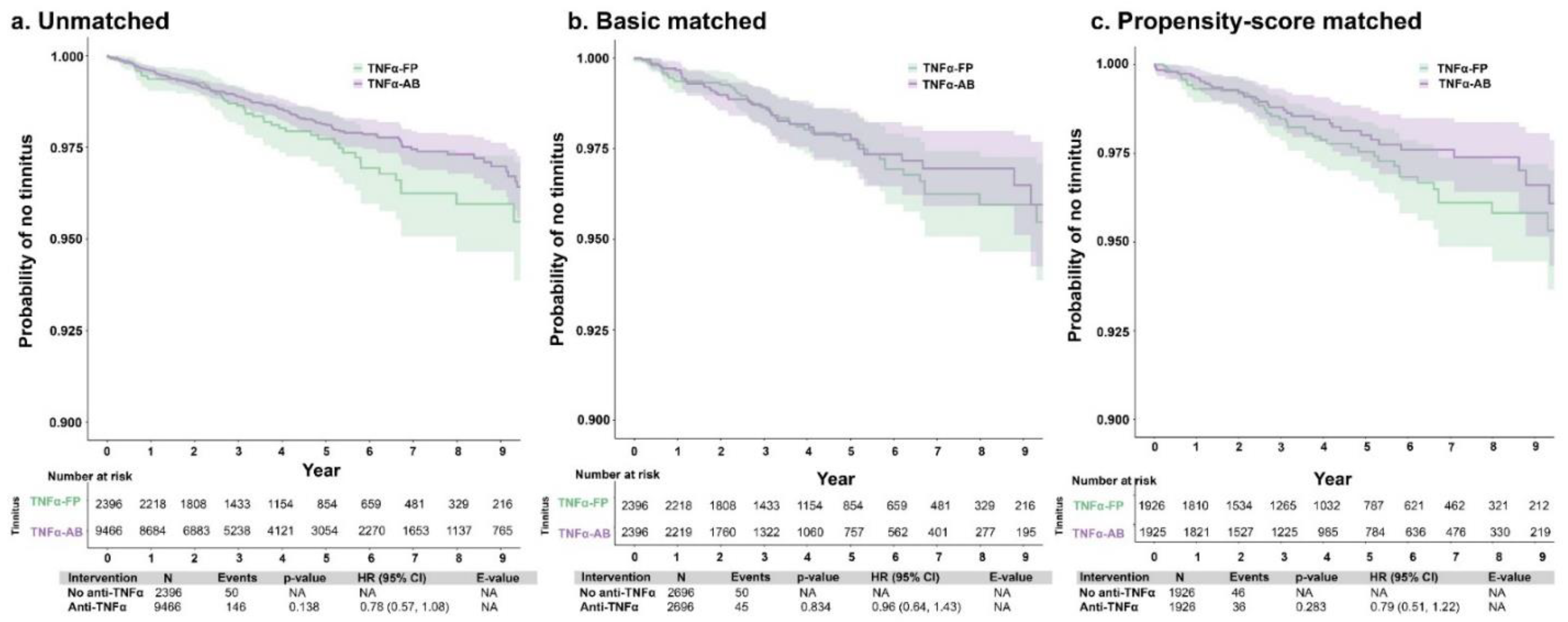
3.3. Tinnitus Incidence According to Anti-TNFα Therapy
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global prevalence and incidence of tinnitus: A systematic review and meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef]
- Esmaili, A.A.; Renton, J. A review of tinnitus. Aust. J. Gen. Pract. 2018, 47, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Chari, D.A.; Limb, C.J. Tinnitus. Med. Clin. N. Am. 2018, 102, 1081–1093. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Lin, H.W.; Bhattacharyya, N. Prevalence, severity, exposures, and treatment patterns of tinnitus in the United States. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 959–965. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, N.; Seidman, M. Tinnitus in the older adult: Epidemiology, pathophysiology and treatment options. Drugs Aging 2004, 21, 297–305. [Google Scholar] [CrossRef]
- Boecking, B.; Biehl, R.; Brueggemann, P.; Mazurek, B. Health-related quality of life, depressive symptoms, anxiety, and somatization symptoms in male and female patients with chronic tinnitus. J. Clin. Med. 2021, 10, 2798. [Google Scholar] [CrossRef]
- Tunkel, D.E.; Bauer, C.A.; Sun, G.H.; Rosenfeld, R.M.; Chandrasekhar, S.S.; Cunningham, E.R., Jr.; Archer, S.M.; Blakley, B.W.; Carter, J.M.; Granieri, E.C.; et al. Clinical practice guideline: Tinnitus. Otolaryngol. Head Neck Surg. 2014, 151, S1–S40. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus. Trends Neurosci. 2004, 27, 676–682. [Google Scholar] [CrossRef]
- Shore, S.E.; Roberts, L.E.; Langguth, B. Maladaptive plasticity in tinnitus—Triggers, mechanisms and treatment. Nat. Rev. Neurol. 2016, 12, 150–160. [Google Scholar] [CrossRef] [Green Version]
- Shulman, A.; Wang, W.; Luo, H.; Bao, S.; Searchfield, G.; Zhang, J. Neuroinflammation and tinnitus. Curr. Top. Behav. Neurosci. 2021, 51, 161–174. [Google Scholar]
- Ren, Y.; Stankovic, K.M. The role of tumor necrosis factor alpha (TNFα) in hearing loss and vestibular schwannomas. Curr. Otorhinolaryngol. Rep. 2018, 6, 15–23. [Google Scholar] [CrossRef]
- Mennink, L.M.; Aalbers, M.W.; van Dijk, P.; van Dijk, J.M.C. The role of inflammation in tinnitus: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 1000. [Google Scholar] [CrossRef]
- Adcock, K.; Vanneste, S. Neuroinflammation in tinnitus. Curr. Otorhinolaryngol. Rep. 2022, 10, 322–328. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, L.S.; Zinsmaier, A.K.; Patterson, G.; Leptich, E.J.; Shoemaker, S.L.; Yatskievych, T.A.; Gibboni, R.; Pace, E.; Luo, H.; et al. Neuroinflammation mediates noise-induced synaptic imbalance and tinnitus in rodent models. PLoS Biol. 2019, 17, e3000307. [Google Scholar] [CrossRef]
- Chen, X.H.; Zheng, L.L. Expression of pro-inflammatory cytokines in the auditory cortex of rats with salicylate-induced tinnitus. Mol. Med. Rep. 2017, 16, 5643–5648. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.-H.; Chen, J.-C.; Yang, S.-Y.; Wang, M.-F.; Chan, Y.-C. Expression of tumor necrosis factor-α and interleukin-1β genes in the cochlea and inferior colliculus in salicylate-induced tinnitus. J. Neuroinflammation 2011, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Deng, D.; Wang, W.; Bao, S. Diffusible tumor necrosis factor-alpha (TNF-α) promotes noise-induced parvalbumin-positive (PV+) neuron loss and auditory processing impairments. Front. Neurosci. 2020, 14, 573047. [Google Scholar] [CrossRef]
- Gonzalez-Gonzalez, S.; Cazevieille, C. 3,6′-dithiothalidomide reduces tinnitus phenotype in two different mouse preclinical models of tinnitus. J. Community Prev. Med. 2020, 3, 1–8. [Google Scholar] [CrossRef]
- Hwang, J.H.; Huang, D.C.; Lu, Y.C.; Yang, W.S.; Liu, T.C. Effects of tumor necrosis factor blocker on salicylate-induced tinnitus in mice. Int. Tinnitus J. 2017, 21, 24–29. [Google Scholar] [CrossRef]
- Katsumi, S.; Sahin, M.I.; Lewis, R.M.; Iyer, J.S.; Landegger, L.D.; Stankovic, K.M. Intracochlear perfusion of tumor necrosis factor-alpha induces sensorineural hearing loss and synaptic degeneration in guinea pigs. Front. Neurol. 2019, 10, 1353. [Google Scholar] [CrossRef] [Green Version]
- Marchiori, L.L.M.; Dias, A.C.M.; Gonçalvez, A.S.; Poly-Frederico, R.C.; Doi, M.Y. Association between polymorphism of tumor necrosis factor alpha (TNFα) in the region -308 g/a with tinnitus in the elderly with a history of occupational noise exposure. Noise Health 2018, 20, 37–41. [Google Scholar]
- Weber, C.; Arck, P.; Mazurek, B.; Klapp, B.F. Impact of a relaxation training on psychometric and immunologic parameters in tinnitus sufferers. J. Psychosom. Res. 2002, 52, 29–33. [Google Scholar] [CrossRef]
- Szczepek, A.J.; Haupt, H.; Klapp, B.F.; Olze, H.; Mazurek, B. Biological correlates of tinnitus-related distress: An exploratory study. Hear. Res. 2014, 318, 23–30. [Google Scholar] [CrossRef]
- Haider, H.F.; Ribeiro, S.F.; Martins, C.; Ribeiro, D.; Trigueiros, N.; Szczepek, A.J.; Caria, H.; Hoare, D.J.; Paço, J.; Borrego, L.-M. Tinnitus, hearing loss and inflammatory processes in an older Portuguese population. Int. J. Audiol. 2020, 59, 323–332. [Google Scholar] [CrossRef]
- Bradley, J.R. TNF-mediated inflammatory disease. J. Pathol. 2008, 214, 149–160. [Google Scholar] [CrossRef]
- Jang, D.-i.; Lee, A.-H.; Shin, H.-Y.; Song, H.-R.; Park, J.-H.; Kang, T.-B.; Lee, S.-R.; Yang, S.-H. The role of tumor necrosis factor alpha (TNF-α) in autoimmune disease and current TNF-α inhibitors in therapeutics. Int. J. Mol. Sci. 2021, 22, 2719. [Google Scholar] [CrossRef]
- Charlson, M.; Pompei, P.; Ales, K.; MacKenzie, R. Charlson comorbidity index. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Nondahl, D.M.; Cruickshanks, K.J.; Wiley, T.L.; Klein, R.; Klein, B.E.; Tweed, T.S. Prevalence and 5-year incidence of tinnitus among older adults: The epidemiology of hearing loss study. J. Am. Acad. Audiol. 2002, 13, 323–331. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Schneeweiss, S.; Rassen, J.A.; Glynn, R.J.; Avorn, J.; Mogun, H.; Brookhart, M.A. High-dimensional propensity score adjustment in studies of treatment effects using health care claims data. Epidemiology 2009, 20, 512–522. [Google Scholar] [CrossRef] [Green Version]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.M.; Eddings, W.; Glynn, R.J.; Schneeweiss, S. Regularized regression versus the high-dimensional propensity score for confounding adjustment in secondary database analyses. Am. J. Epidemiol. 2015, 182, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Low, Y.S.; Gallego, B.; Shah, N.H. Comparing high-dimensional confounder control methods for rapid cohort studies from electronic health records. J. Comp. Eff. Res. 2016, 5, 179–192. [Google Scholar] [CrossRef] [Green Version]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction, 2nd ed.; Springer: Berlin/Heidelberg, Germany; International Statistical Institute: Voorburg, The Netherlands, 2009. [Google Scholar]
- Jacobson, D.L.; Gange, S.J.; Rose, N.R.; Graham, N.M. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin. Immunol. Immunopathol. 1997, 84, 223–243. [Google Scholar] [CrossRef] [Green Version]
- Johns Hopkins University. Prevalence of Autoimmune Disorders. Available online: https://pathology.jhu.edu/autoimmune/prevalence (accessed on 25 October 2022).
- Morovic Vergles, J.; Radic, M.; Kovacic, J.; Salamon, L. Successful use of adalimumab for treating rheumatoid arthritis with autoimmune sensorineural hearing loss: Two birds with one stone. J. Rheumatol. 2010, 37, 1080–1081. [Google Scholar] [CrossRef] [Green Version]
- Emamifar, A.; Bjoerndal, K.; Hansen, I.M. Is hearing impairment associated with rheumatoid arthritis? A review. Open Rheumatol. J. 2016, 10, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Ralli, M.; D’Aguanno, V.; Di Stadio, A.; De Virgilio, A.; Croce, A.; Longo, L.; Greco, A.; de Vincentiis, M. Audiovestibular symptoms in systemic autoimmune diseases. J. Immunol. Res. 2018, 2018, 5798103. [Google Scholar] [CrossRef] [Green Version]
- Ciorba, A.; Corazzi, V.; Bianchini, C.; Aimoni, C.; Pelucchi, S.; Skarżyński, P.H.; Hatzopoulos, S. Autoimmune inner ear disease (AIED): A diagnostic challenge. Int. J. Immunopathol. Pharmacol. 2018, 32, 2058738418808680. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Shoup, A.; Weisman, M.H.; Harris, J. Etanercept treatment for autoimmune inner ear disease: Results of a pilot placebo-controlled study. Otol. Neurotol. 2005, 26, 903–907. [Google Scholar] [CrossRef]
- Van Wijk, F.; Staecker, H.; Keithley, E.; Lefebvre, P.P. Local perfusion of the tumor necrosis factor alpha blocker infliximab to the inner ear improves autoimmune neurosensory hearing loss. Audiol. Neurootol. 2006, 11, 357–365. [Google Scholar] [CrossRef]
- Derebery, M.J.; Fisher, L.M.; Voelker, C.C.; Calzada, A. An open label study to evaluate the safety and efficacy of intratympanic golimumab therapy in patients with autoimmune inner ear disease. Otol. Neurotol. 2014, 35, 1515–1521. [Google Scholar] [CrossRef]
- Jachiet, M.; Lependu, C.; Fragny, D.; Mariette, X.; Lepajolec, C.; Seror, R. Severe deafness associated with Crohn’s disease and spondylarthropathy: Successful treatment with anti-TNF. Rheumatology 2013, 52, 1145–1147. [Google Scholar] [CrossRef] [Green Version]
- Conway, R.; Khan, S.; Foley-Nolan, D. Use of adalimumab in treatment of autoimmune sensorineural hearing loss: A word of caution. J. Rheumatol. 2011, 38, 176. [Google Scholar] [CrossRef]
- Møller, A.R. Epidemiology of tinnitus in adults. In Textbook of Tinnitus; Møller, A.R., Langguth, B., De Ridder, D., Kleinjung, T., Eds.; Springer: New York, NY, USA, 2011; pp. 29–37. [Google Scholar]
- KochKin, S.; Tyler, R.; Born, J. MarkeTrak VIII: The prevalence of tinnitus in the United States and the self-reported efficacy of various treatments. Hear. Rev. 2011, 18, 10–27. [Google Scholar]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef]
- Gopinath, B.; McMahon, C.M.; Rochtchina, E.; Karpa, M.J.; Mitchell, P. Incidence, persistence, and progression of tinnitus symptoms in older adults: The Blue Mountains Hearing Study. Ear Hear. 2010, 31, 407–412. [Google Scholar] [CrossRef]
- Lee, H.M.; Han, K.d.; Kong, S.K.; Nam, E.C.; Park, S.N.; Shim, H.J.; Byun, J.Y.; Park, H.J.; Im, G.J.; Lee, I.-W. Epidemiology of clinically significant tinnitus: A 10-year trend from nationwide health claims data in South Korea. Otol. Neurotol. 2018, 39, 680–687. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients in the EHR with Tinnitus N = 155,091 | |
|---|---|
| N with minimum history a Mean pre-index days [SD] | 90,681 1953.6 [1797.2] |
| Duration of follow-up, mean [SD] days | 1280.2 [903.0] |
| Sex, n (%) female | 48,661 (53.7%) |
| Age, years | |
| Mean [SD] | 59.8 [14.3] |
| Distribution, n (%) | |
| 18–29 | 3613 (4.0%) |
| 30–39 | 5664 (6.2%) |
| 40–49 | 11,000 (12.1%) |
| 50–59 | 21,495 (23.7%) |
| 60–69 | 26,114 (28.8%) |
| 70–79 | 17,102 (18.9%) |
| 80–89 | 5693 (6.3%) |
| Race/ethnicity, n (%) | |
| White | 60,543 (66.8%) |
| Black | 5969 (6.6%) |
| Asian | 1002 (1.1%) |
| Other b | 23,167 (25.5%) |
| CCI | |
| Mean [SD] score | 2.6 [2.2] |
| Component disorders, n (%) | |
| Malignancy | 5211 (5.7%) |
| Metastatic solid tumor | 272 (0.3%) |
| Diabetes | 15,030 (16.6%) |
| Diabetes with complications | 4495 (5.0%) |
| Congestive heart failure | 2991 (3.3%) |
| Myocardial infarction | 1011 (1.1%) |
| Peripheral vascular disease | 4983 (5.5%) |
| Chronic pulmonary disease | 16,613 (18.3%) |
| Cerebrovascular disease | 5737 (6.3%) |
| Dementia | 622 (0.7%) |
| Hemiparaplegia | 379 (0.4%) |
| Mild liver disease | 3435 (3.8%) |
| Severe liver disease | 127 (0.1%) |
| Renal disease | 5382 (6.0%) |
| Peptic ulcer disease | 948 (1.1%) |
| Rheumatic disease | 2633 (2.9%) |
| HIV | 171 (0.2%) |
| Autoimmune Disorders Cohorts a | ||||
|---|---|---|---|---|
| Before Matching | After Matching | |||
| No-TNFα N = 25,000 b | Yes-TNFα N = 13,293 | No-TNFα N = 10,645 | Yes-TNFα N = 10,645 | |
| Duration of follow-up, mean [SD] days | 1418.8 [985.1] | 1577.3 [1044.2] | 1416.3 [968.3] | 1653.5 [1072.3] |
| Sex, n (%) female | 16,211 (64.8%) | 8816 (66.3%) | 6984 (65.6%) | 6952 (65.3%) |
| Age, years | ||||
| Mean [SD] | 56.2 [17.5] | 53.2 [14.7] | 53.4 [17.4] | 53.4 [14.7] |
| Distribution, n (%) | ||||
| 18–29 | 2566 (10.3%) | 1046 (7.9%) | 1332 (12.5%) | 843 (7.9%) |
| 30–39 | 2524 (10.1%) | 1567 (11.8%) | 1316 (12.4%) | 1234 (11.6%) |
| 40–49 | 3269 (13.1%) | 2528 (19.0%) | 1591 (14.9%) | 1950 (18.3%) |
| 50–59 | 4998 (20.0%) | 3500 (26.3%) | 2197 (20.6%) | 2821 (26.5%) |
| 60–69 | 5471 (21.9%) | 2989 (22.5%) | 2189 (20.6%) | 2439 (22.9%) |
| 70–79 | 4339 (17.4%) | 1392 (10.5%) | 1457 (13.7%) | 1136 (10.7%) |
| 80–89 | 1833 (7.3%) | 271 (2.0%) | 563 (5.3%) | 222 (2.1%) |
| Race/ethnicity, n (%) | ||||
| White | 15,421 (61.7%) | 8752 (66.8%) | 6855 (64.4%) | 6799 (63.9%) |
| Black | 1953 (7.8%) | 826 (6.2%) | 697 (6.5%) | 692 (6.5%) |
| Asian | 204 (0.8%) | 105 (0.8%) | 87 (0.8%) | 88 (0.8%) |
| Other c | 7422 (29.7%) | 3610 (27.2%) | 3006 (28.2%) | 3066 (28.8%) |
| CCI | ||||
| Mean score [SD] | 2.6 [2.4] | 2.1 [1.8] | 2.2 [2.2] | 2.1 [1.8] |
| Component disorders, n (%) | ||||
| Malignancy | 1129 (4.5%) | 249 (1.9%) | 367 (3.5%) | 216 (2.0%) |
| Metastatic solid tumor | 58 (0.2%) | 11 (0.1%) | 12 (0.1%) | 10 (0.1%) |
| Diabetes | 4086 (16.3%) | 1507 (11.3%) | 1478 (13.9%) | 1201 (11.3%) |
| Diabetes w/complications | 1093 (4.4%) | 321 (2.4%) | 350 (3.3%) | 255 (2.4%) |
| Congestive heart failure | 987 (4.0%) | 183 (1.4%) | 316 (3.0%) | 151 (1.4%) |
| Myocardial infarction | 271 (1.1%) | 78 (0.6%) | 82 (0.8%) | 66 (0.6%) |
| Peripheral vascular disease | 1465 (5.9%) | 268 (2.0%) | 457 (4.3%) | 236 (2.2%) |
| Chronic pulmonary disease | 4893 (19.7%) | 1520 (11.4%) | 1851 (17.4%) | 1214 (11.4%) |
| Cerebrovascular disease | 1294 (5.2%) | 273 (2.1%) | 388 (3.6%) | 227 (2.1%) |
| Dementia | 192 (0.8%) | 16 (0.1%) | 49 (0.5%) | 11 (0.1%) |
| Hemiparaplegia | 99 (0.4%) | 18 (0.1%) | 37 (0.4%) | 11 (0.1%) |
| Mild liver disease | 833 (3.3%) | 290 (2.2%) | 313 (2.9%) | 234 (2.2%) |
| Severe liver disease | 55 (0.2%) | 10 (0.1%) | 24 (0.2%) | 9 (0.1%) |
| Renal disease | 1406 (5.6%) | 305 (2.3%) | 435 (4.1%) | 249 (2.2%) |
| Peptic ulcer disease | 344 (1.4%) | 121 (1.0%) | 118 (1.1%) | 112 (1.1%) |
| Rheumatic disease | 7152 (28.6%) | 6538 (49.2%) | 3155 (29.6%) | 5012 (47.1%) |
| HIV | 49 (0.2%) | 7 (0.1%) | 17 (0.2%) | 5 (0.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natarajan, N.; Batts, S.; Gombar, S.; Manickam, R.; Sagi, V.; Curhan, S.G.; Stankovic, K.M. Associations of Tinnitus Incidence with Use of Tumor Necrosis Factor-Alpha Inhibitors among Patients with Autoimmune Conditions. J. Clin. Med. 2023, 12, 1935. https://doi.org/10.3390/jcm12051935
Natarajan N, Batts S, Gombar S, Manickam R, Sagi V, Curhan SG, Stankovic KM. Associations of Tinnitus Incidence with Use of Tumor Necrosis Factor-Alpha Inhibitors among Patients with Autoimmune Conditions. Journal of Clinical Medicine. 2023; 12(5):1935. https://doi.org/10.3390/jcm12051935
Chicago/Turabian StyleNatarajan, Nirvikalpa, Shelley Batts, Saurabh Gombar, Raj Manickam, Varun Sagi, Sharon G. Curhan, and Konstantina M. Stankovic. 2023. "Associations of Tinnitus Incidence with Use of Tumor Necrosis Factor-Alpha Inhibitors among Patients with Autoimmune Conditions" Journal of Clinical Medicine 12, no. 5: 1935. https://doi.org/10.3390/jcm12051935
APA StyleNatarajan, N., Batts, S., Gombar, S., Manickam, R., Sagi, V., Curhan, S. G., & Stankovic, K. M. (2023). Associations of Tinnitus Incidence with Use of Tumor Necrosis Factor-Alpha Inhibitors among Patients with Autoimmune Conditions. Journal of Clinical Medicine, 12(5), 1935. https://doi.org/10.3390/jcm12051935