

A Multi-Centre Non-Interventional Study to Assess the Tolerability and Effectiveness of Extended-Release Tacrolimus (LCPT) in De Novo Liver Transplant Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Objectives
2.3. Statistical Considerations
3. Guidelines
Ethical Considerations
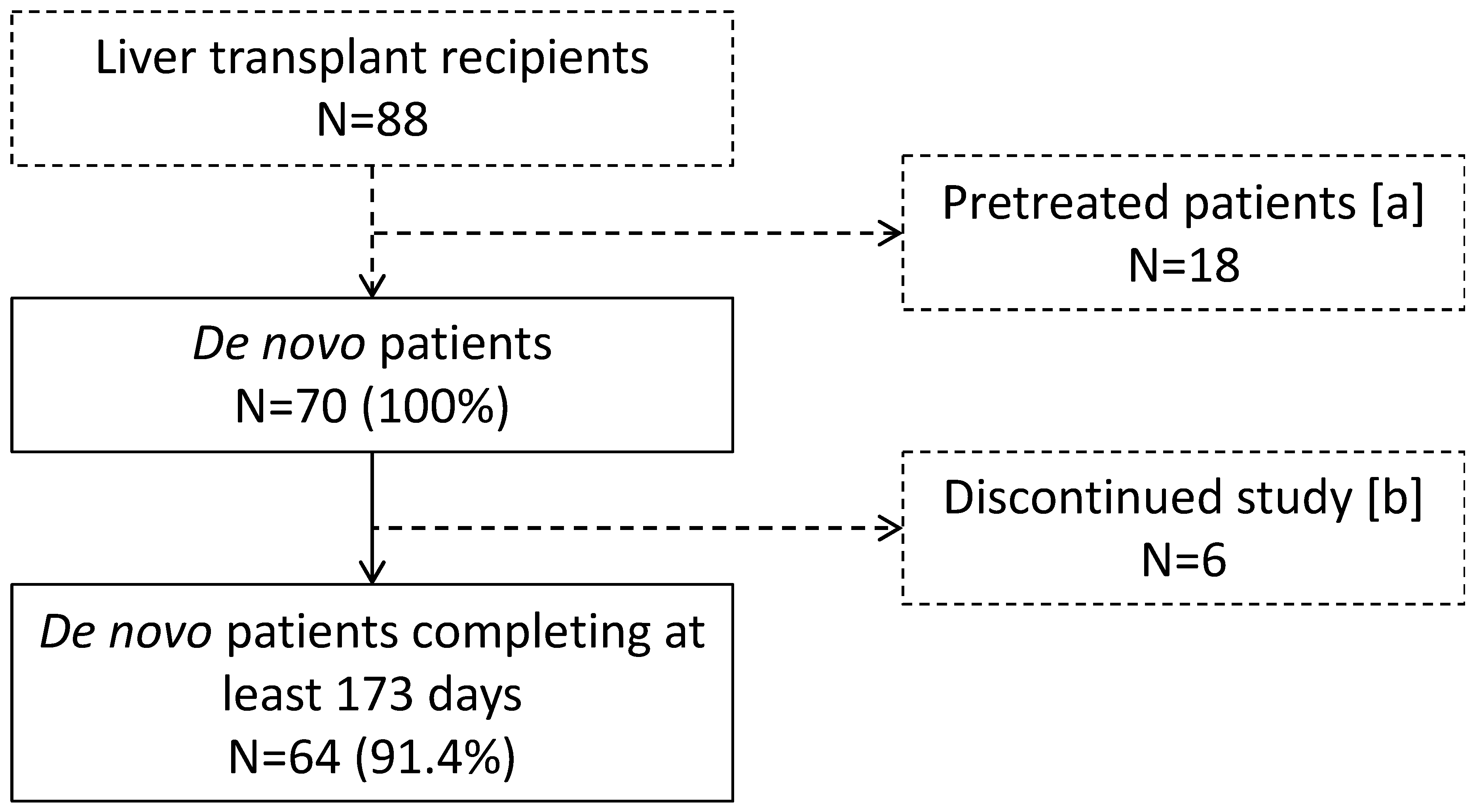
4. Results
4.1. Baseline Characteristics
4.2. LCPT Tolerability (Primary Objective)
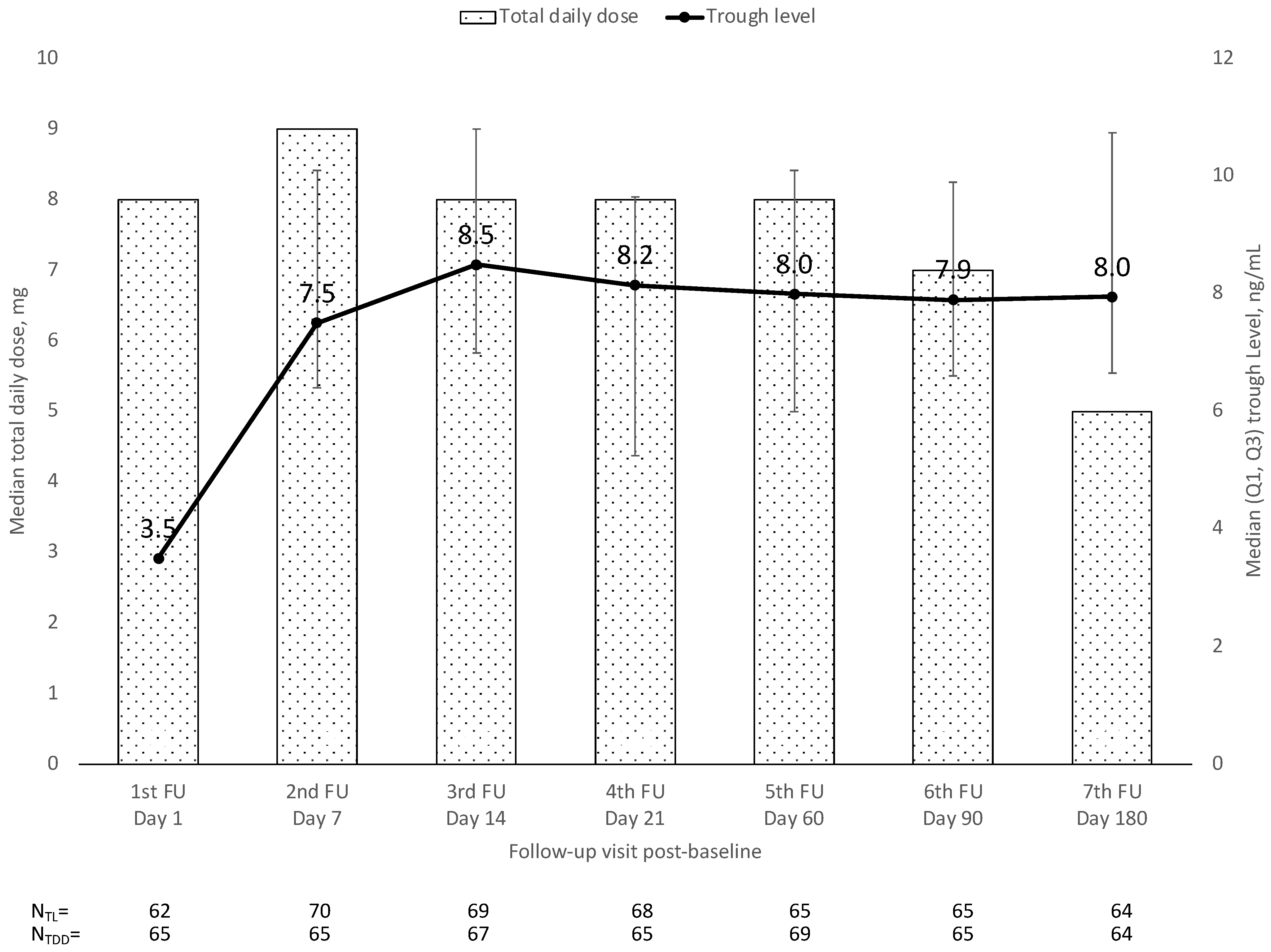
4.3. Tacrolimus Dosing and trough Levels over Time
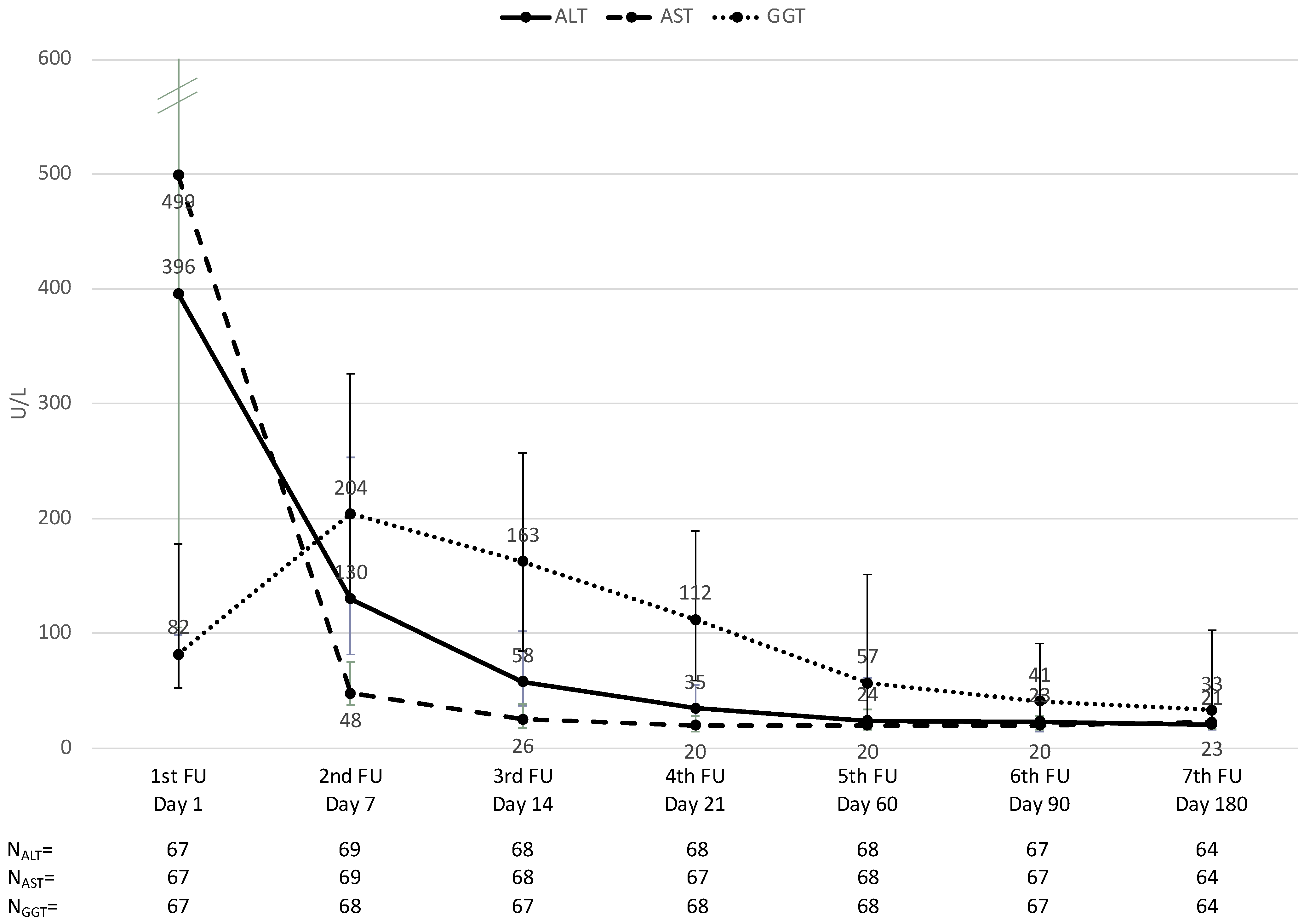
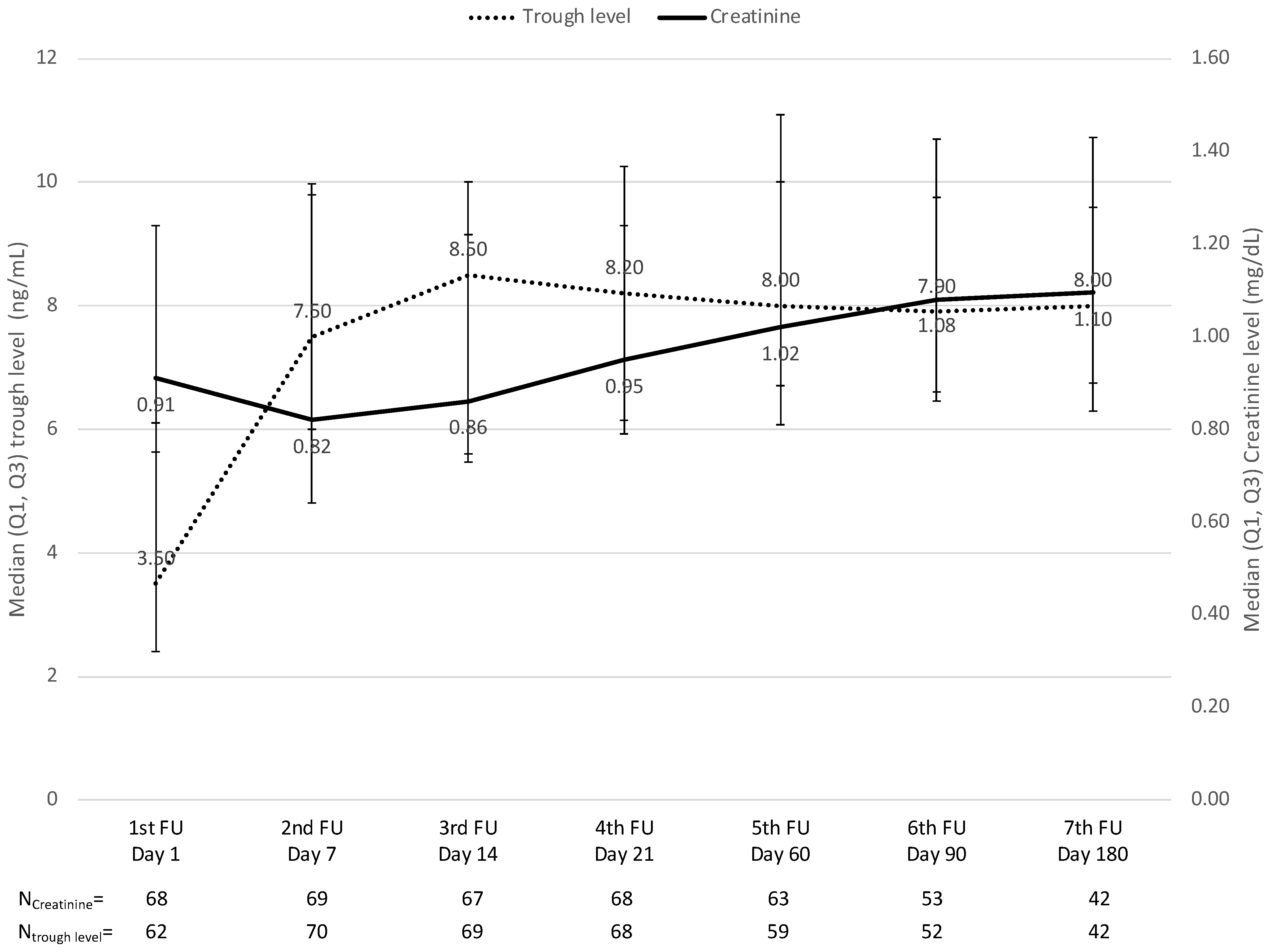
4.4. Liver and Kidney Function over Time
5. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADR | adverse drug reaction |
| AE | adverse event |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CNI | calcineurin inhibitor |
| ECD | extended criteria donor |
| eCRF | electronic case report form |
| FK506 | tacrolimus |
| GGT | gamma-glutamyl transferase |
| IR | immediate-release |
| LCP | Life Cycle Pharma |
| LCPT | LCP-tacrolimus |
| mAb | monoclonal antibody |
| MMF | mycophenolate mofetil |
| NIS | non-interventional study |
| NOS | not otherwise specified |
| POD | post-operative day |
| Q1 | 25% quartile |
| Q3 | 75% quartile |
| SD | standard deviation |
| SADR | serious adverse drug reaction |
| SAE | serious adverse event |
| SmPC | summary of product characteristics |
| STROBE | Reporting of Observational Studies in Epidemiology |
| SÚKL | Czech State Institute for Drug Control |
References
- Wagner, M.; Earley, A.K.; Webster, A.C.; Schmid, C.H.; Balk, E.M.; Uhlig, K. Mycophenolic acid versus azathioprine as primary immunosuppression for kidney transplant recipients. Cochrane Database Syst. Rev. 2015, CD007746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Maira, T.; Little, E.C.; Berenguer, M. Immunosuppression in liver transplant. Best Pract. Res. Clin. Gastroenterol. 2020, 46–47, 101681. [Google Scholar] [CrossRef] [PubMed]
- Jasiak, N.M.; Park, J.M. Immunosuppression in Solid-Organ Transplantation: Essentials and Practical Tips. Crit. Care Nurs. Q. 2016, 39, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.W.; Bonham, C.A.; Zeevi, A. Mode of action of tacrolimus (FK506): Molecular and cellular mechanisms. Ther. Drug Monit. 1995, 17, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Vicari-Christensen, M.; Repper, S.; Basile, S.; Young, D. Tacrolimus: Review of pharmacokinetics, pharmacodynamics, and pharmacogenetics to facilitate practitioners’ understanding and offer strategies for educating patients and promoting adherence. Prog. Transplant. 2009, 19, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Venkataramanan, R.; Swaminathan, A.; Prasad, T.; Jain, A.; Zuckerman, S.; Warty, V.; McMichael, J.; Lever, J.; Burckart, G.; Starzl, T. Clinical pharmacokinetics of tacrolimus. Clin. Pharmacokinet. 1995, 29, 404–430. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Envarsus: EPAR—Product Information. Available online: https://www.ema.europa.eu/en/documents/product-information/envarsus-epar-product-information_en.pdf (accessed on 29 May 2020).
- Wallemacq, P.; Armstrong, V.W.; Brunet, M.; Haufroid, V.; Holt, D.W.; Johnston, A.; Kuypers, D.; Meur, Y.L.; Marquet, P.; Oellerich, M.; et al. Opportunities to optimize tacrolimus therapy in solid organ transplantation: Report of the European consensus conference. Ther. Drug Monit. 2009, 31, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grinyo, J.M.; Petruzzelli, S. Once-daily LCP-Tacro MeltDose tacrolimus for the prophylaxis of organ rejection in kidney and liver transplantations. Expert Rev. Clin. Immunol. 2014, 10, 1567–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, S.; Nigro, V.; Weinberg, J.; Woodle, E.S.; Alloway, R.R. A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): An Open-Label, Prospective, Randomized, Two-Arm, Three-Period Crossover Study. Am. J. Transplant. 2017, 17, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Garnock-Jones, K.P. Tacrolimus prolonged release (Envarsus(R)): A review of its use in kidney and liver transplant recipients. Drugs 2015, 75, 309–320. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Guideline on Clinical Investigation of Immunosuppressants for Solid Organ Transplantation. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-immunosuppressants-solid-organ-transplantation_en.pdf (accessed on 2 July 2020).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaber, A.O.; Alloway, R.R.; Bodziak, K.; Kaplan, B.; Bunnapradist, S. Conversion from twice-daily tacrolimus capsules to once-daily extended-release tacrolimus (LCPT): A phase 2 trial of stable renal transplant recipients. Transplantation 2013, 96, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DuBay, D.A.; Teperman, L.; Ueda, K.; Silverman, A.; Chapman, W.; Alsina, A.E.; Tyler, C.; Stevens, D.R. Pharmacokinetics of Once-Daily Extended-Release Tacrolimus Tablets versus Twice-Daily Capsules in De Novo Liver Transplant. Clin. Pharmacol. Drug Dev. 2019, 8, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Baccarani, U.; Velkoski, J.; Pravisani, R.; Adani, G.L.; Lorenzin, D.; Cherchi, V.; Falzone, B.; Baraldo, M.; Risaliti, A. MeltDose Technology vs. Once-Daily Prolonged Release Tacrolimus in De Novo Liver Transplant Recipients. Transplant. Proc. 2019, 51, 2971–2973. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, A.; Wu, S.; Stranzinger, S.; Mohr, S.; Salar-Behzadi, S.; Bresciani, M.; Fröhlich, E. In vitro and in silico characterisation of Tacrolimus released under biorelevant conditions. Int. J. Pharm. 2016, 515, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Alloway, R.R.; Eckhoff, D.E.; Washburn, W.K.; Teperman, L.W. Conversion from twice daily tacrolimus capsules to once daily extended-release tacrolimus (LCP-Tacro): Phase 2 trial of stable liver transplant recipients. Liver Transplant. 2014, 20, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Hazell, L.; Shakir, S.A.W. Under-Reporting of Adverse Drug Reactions. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Liver Transplant Patients De Novo, n = 70 | |
|---|---|
| Male sex, n (%) | 51 (72.9) |
| Mean (SD) age, years | 54 (11.2) |
| Age group, n (%) | |
| <65 years | 60 (85.7) |
| ≥65 years | 10 (14.3) |
| Mean (SD) weight, kg | 78 (12.9) |
| Mean (SD) height, cm | 171 (11.9) |
| Mean (SD) BMI, kg/m2 | 27 (5.8) |
| Lab MELD (SD) | 17 (7.2) |
| Underlying disease, n [a] | |
| Alcoholic cirrhosis | 38 |
| Hepatocellular carcinoma | 25 |
| Post-hepatitic c cirrhosis | 10 |
| Sclerosing cholangitis | 9 |
| Cryptogenic liver cirrhosis | 5 |
| Acute hepatic failure | 4 |
| Cirrhosis of unknown causes | 4 |
| Wilson disease | 3 |
| Non-alcoholic steatohepatitis | 3 |
| Primary biliary cirrhosis | 3 |
| Secondary liver tumors | 3 |
| Autoimmune cirrhosis | 2 |
| Others | 5 |
| Immunosuppressive regimen [b, c], n (%) | |
| Induction therapy | 64/70 (91) |
| ATG | 58/64 (90.6) |
| Basiliximab | 6/64 (9.4) |
| Steroids | 70 (100) |
| MMF | 12 (17.1) |
| Number of Events | Adverse Events (n = 70) |
|---|---|
| Any AE | 24 |
| Mild AE | 21 |
| Moderate AE | 2 |
| Severe AE | 1 |
| ADRs (related to immunosuppression) | 17 |
| Leukopenia NOS | 3 |
| Arterial hypertension | 2 |
| Renal failure | 5 |
| Abdominal infection | 1 |
| Urinary tract infection | 2 |
| CMV infection | 2 |
| Epilepsy NOS | 1 |
| Hyperglycemia NOS | 1 |
| AEs (unrelated to immunosuppression) | 7 |
| Hemorrhagic anemia | 2 |
| Atrial flutter * | 1 |
| Hepatic enzyme increased | 1 |
| Hepatic function abnormal * | 1 |
| Collapse circulatory | 1 |
| Insomnia | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soliman, T.; Gyoeri, G.; Salat, A.; Mejzlík, V.; Berlakovich, G. A Multi-Centre Non-Interventional Study to Assess the Tolerability and Effectiveness of Extended-Release Tacrolimus (LCPT) in De Novo Liver Transplant Patients. J. Clin. Med. 2023, 12, 2537. https://doi.org/10.3390/jcm12072537
Soliman T, Gyoeri G, Salat A, Mejzlík V, Berlakovich G. A Multi-Centre Non-Interventional Study to Assess the Tolerability and Effectiveness of Extended-Release Tacrolimus (LCPT) in De Novo Liver Transplant Patients. Journal of Clinical Medicine. 2023; 12(7):2537. https://doi.org/10.3390/jcm12072537
Chicago/Turabian StyleSoliman, Thomas, Georg Gyoeri, Andreas Salat, Vladimír Mejzlík, and Gabriela Berlakovich. 2023. "A Multi-Centre Non-Interventional Study to Assess the Tolerability and Effectiveness of Extended-Release Tacrolimus (LCPT) in De Novo Liver Transplant Patients" Journal of Clinical Medicine 12, no. 7: 2537. https://doi.org/10.3390/jcm12072537
APA StyleSoliman, T., Gyoeri, G., Salat, A., Mejzlík, V., & Berlakovich, G. (2023). A Multi-Centre Non-Interventional Study to Assess the Tolerability and Effectiveness of Extended-Release Tacrolimus (LCPT) in De Novo Liver Transplant Patients. Journal of Clinical Medicine, 12(7), 2537. https://doi.org/10.3390/jcm12072537