
Optimal Timing of Targeted Temperature Management for Post-Cardiac Arrest Syndrome: Is Sooner Better?
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
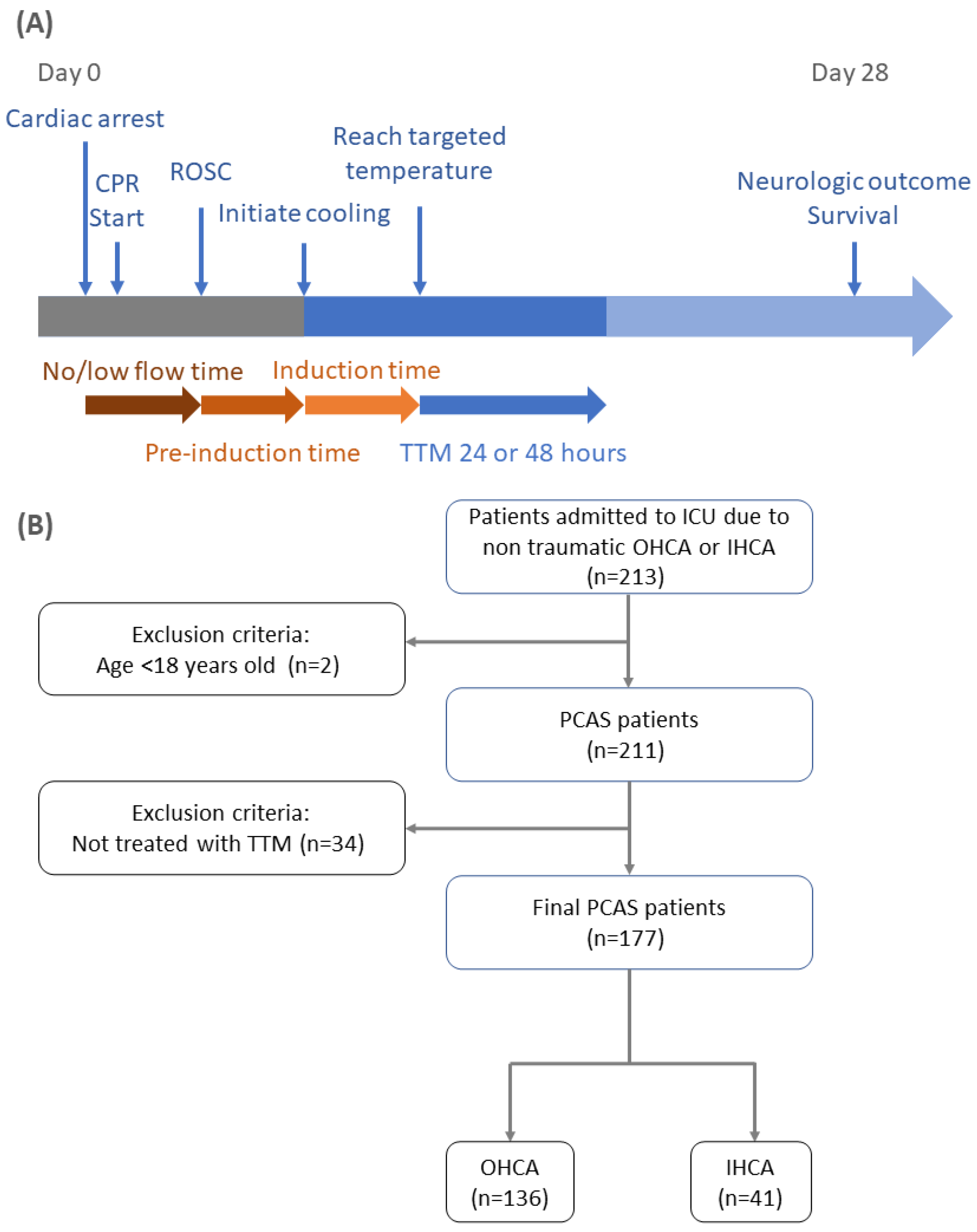
2.2. Protocol Description
2.3. Data Collection and Outcome Assessment
2.4. Statistical Analysis
3. Results
Population, Demographics, Arrest Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef] [PubMed]
- The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Scolletta, S.; Taccone, F.S.; Nordberg, P.; Donadello, K.; Vincent, J.L.; Castren, M. Intra-arrest hypothermia during cardiac arrest: A systematic review. Crit. Care 2012, 16, R41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, S.A.; Smith, K.; Finn, J.; Hein, C.; Grantham, H.; Bray, J.E.; Deasy, C.; Stephenson, M.; Williams, T.A.; Straney, L.D.; et al. Induction of therapeutic hypothermia during out-of-hospital cardiac arrest using a rapid infusion of cold saline: The RINSE trial (Rapid Infusion of Cold Normal Saline). Circulation 2016, 134, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, P.; Taccone, F.S.; Truhlar, A.; Forsberg, S.; Hollenberg, J.; Jonsson, M.; Cuny, J.; Goldstein, P.; Vermeersch, N.; Higuet, A.; et al. Effect of trans-nasal evaporative intra-arrest cooling on functional neurologic outcome in out-of-hospital cardiac arrest: The PRINCESS randomized clinical trial. JAMA 2019, 321, 1677–1685. [Google Scholar] [CrossRef]
- Bernard, S.A.; Smith, K.; Cameron, P.; Masci, K.; Taylor, D.M.; Cooper, D.J.; Kelly, A.M.; Silvester, W. Induction of prehospital therapeutic hypothermia after resuscitation from nonventricular fibrillation cardiac arrest*. Crit. Care Med. 2012, 40, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Schock, R.B.; Janata, A.; Peacock, W.F.; Deal, N.S.; Kalra, S.; Sterz, F. Time to cooling is associated with resuscitation outcomes. Ther. Hypothermia Temp. Manag. 2016, 6, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Wolff, B.; Machill, K.; Schumacher, D.; Schulzki, I.; Werner, D. Early achievement of mild therapeutic hypothermia and the neurologic outcome after cardiac arrest. Int. J. Cardiol. 2009, 133, 223–228. [Google Scholar] [CrossRef]
- Sendelbach, S.; Hearst, M.O.; Johnson, P.J.; Unger, B.T.; Mooney, M.R. Effects of variation in temperature management on cerebral performance category scores in patients who received therapeutic hypothermia post cardiac arrest. Resuscitation 2012, 83, 829–834. [Google Scholar] [CrossRef]
- Uribarri, A.; Bueno, H.; Pérez-Castellanos, A.; Loughlin, G.; Sousa, I.; Viana-Tejedor, A.; Fernández-Avilés, F. Impact of time to cooling initiation and time to target temperature in patients treated with hypothermia after cardiac arrest. Eur. Heart J. Acute Cardiovasc. Care 2015, 4, 365–372. [Google Scholar] [CrossRef]
- Polderman, K.H. Mechanisms of action, physiological effects, and complications of hypothermia. Crit. Care Med. 2009, 37, S186–S202. [Google Scholar] [CrossRef] [PubMed]
- Sonder, P.; Janssens, G.N.; Beishuizen, A.; Henry, C.L.; Rittenberger, J.C.; Callaway, C.W.; Dezfulian, C.; Polderman, K.H. Efficacy of different cooling technologies for therapeutic temperature management: A prospective intervention study. Resuscitation 2018, 124, 14–20. [Google Scholar] [CrossRef]
- Haugk, M.; Testori, C.; Sterz, F.; Uranitsch, M.; Holzer, M.; Behringer, W.; Herkner, H. Relationship between time to target temperature and outcome in patients treated with therapeutic hypothermia after cardiac arrest. Crit. Care 2011, 15, R101. [Google Scholar] [CrossRef] [Green Version]
- Perman, S.M.; Ellenberg, J.H.; Grossestreuer, A.V.; Gaieski, D.F.; Leary, M.; Abella, B.S.; Carr, B.G. Shorter time to target temperature is associated with poor neurologic outcome in post-arrest patients treated with targeted temperature management. Resuscitation 2015, 88, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.; Scales, D.C.; Dorian, P.; Kiss, A.; Common, M.R.; Brooks, S.C.; Goodman, S.G.; Salciccioli, J.D.; Morrison, L.J. Targeted temperature management processes and outcomes after out-of-hospital cardiac arrest: An observational cohort study*. Crit. Care Med. 2014, 42, 2565–2574. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 °C versus 36 °C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Dankiewicz, J.; Cronberg, T.; Lilja, G.; Jakobsen, J.C.; Levin, H.; Ullén, S.; Rylander, C.; Wise, M.P.; Oddo, M.; Cariou, A.; et al. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N. Engl. J. Med. 2021, 384, 2283–2294. [Google Scholar] [CrossRef]
- Wang, C.J.; Yang, S.H.; Lee, C.H.; Lin, R.L.; Peng, M.J.; Wu, C.L. Therapeutic hypothermia application vs standard support care in post resuscitated out-of-hospital cardiac arrest patients. Am. J. Emerg. Med. 2013, 31, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Yang, S.H.; Chen, C.H.; Chung, H.P. Targeted temperature management for in-hospital cardiac arrest: 6 years of experience. Ther. Hypothermia Temp. Manag. 2020, 10, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Randomized clinical study of thiopental loading in comatose survivors of cardiac arrest. N. Engl. J. Med. 1986, 314, 397–403. [CrossRef]
- Cummins, R.O.; Chamberlain, D.A.; Abramson, N.S.; Allen, M.; Baskett, P.J.; Becker, L.; Bossaert, L.; Delooz, H.H.; Dick, W.F.; Eisenberg, M.S.; et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style: A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991, 84, 960–975. [Google Scholar] [CrossRef] [Green Version]
- Swets, J.A. The relative operating characteristic in psychology: A technique for isolating effects of response bias finds wide use in the study of perception and cognition. Science 1973, 182, 990–1000. [Google Scholar] [CrossRef]
- Metz, C.E. Basic principles of ROC analysis. Semin. Nucl. Med. 1978, 8, 283–298. [Google Scholar] [CrossRef]
- Van der Schouw, Y.T.; Verbeek, A.L.; Ruijs, J.H. ROC curves for the initial assessment of new diagnostic tests. Fam. Pract. 1992, 9, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.H.; Lee, C.H.; Huang, W.C.; Wang, Y.C.; Su, C.H.; Sung, P.H.; Chien, S.C.; Hwang, J.J. 2020 focused update of the 2012 guidelines of the Taiwan society of cardiology for the management of ST-segment elevation myocardial infarction. Acta Cardiol. Sin. 2020, 36, 285–307. [Google Scholar] [CrossRef]
- Park, J.; Choi, K.H.; Lee, J.M.; Kim, H.K.; Hwang, D.; Rhee, T.M.; Kim, J.; Park, T.K.; Yang, J.H.; Song, Y.B.; et al. Prognostic implications of door-to-balloon time and onset-to-door time on mortality in patients with ST-segment-elevation myocardial infarction treated with primary percutaneous coronary intervention. J. Am. Heart Assoc. 2019, 8, e012188. [Google Scholar] [CrossRef] [Green Version]
- Erecinska, M.; Thoresen, M.; Silver, I.A. Effects of hypothermia on energy metabolism in Mammalian central nervous system. J. Cereb. Blood Flow Metab. 2003, 23, 513–530. [Google Scholar] [CrossRef]
- Xu, L.; Yenari, M.A.; Steinberg, G.K.; Giffard, R.G. Mild hypothermia reduces apoptosis of mouse neurons in vitro early in the cascade. J. Cereb. Blood Flow Metab. 2002, 22, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghupathi, R.; Graham, D.I.; McIntosh, T.K. Apoptosis after traumatic brain injury. J. Neurotrauma 2000, 17, 927–938. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; Marcheselli, V.L.; Janata, A.; Schratter, A.; Weihs, W.; Bayegan, K.; Milani, R.V.; Bazan, N.G. Lipid mediators as novel biomarkers and surrogate indicators of neurologic recovery after cardiac arrest in a hypothermic swine model. Circulation 2006, 114, II_1203. [Google Scholar]
- Arrich, J.; Herkner, H.; Müllner, D.; Behringer, W. Targeted temperature management after cardiac arrest. A systematic review and meta-analysis of animal studies. Resuscitation 2021, 162, 47–55. [Google Scholar] [CrossRef]
- Stanger, D.; Kawano, T.; Malhi, N.; Grunau, B.; Tallon, J.; Wong, G.C.; Christenson, J.; Fordyce, C.B. Door-to-targeted temperature management initiation time and outcomes in out-of-hospital cardiac arrest: Insights from the continuous chest compressions trial. J. Am. Heart Assoc. 2019, 8, e012001. [Google Scholar] [CrossRef]
- Awad, A.; Taccone, F.S.; Jonsson, M.; Forsberg, S.; Hollenberg, J.; Truhlar, A.; Ringh, M.; Abella, B.S.; Becker, L.B.; Vincent, J.L.; et al. Time to intra-arrest therapeutic hypothermia in out-of-hospital cardiac arrest patients and its association with neurologic outcome: A propensity matched sub-analysis of the PRINCESS trial. Intensive Care Med. 2020, 46, 1361–1370. [Google Scholar] [CrossRef]
- Carroll, M.; Beek, O. Protection against hippocampal CA1 cell loss by post-ischemic hypothermia is dependent on delay of initiation and duration. Metab. Brain Dis. 1992, 7, 45–50. [Google Scholar] [CrossRef]
- Hicks, S.D.; DeFranco, D.B.; Callaway, C.W. Hypothermia during reperfusion after asphyxial cardiac arrest improves functional recovery and selectively alters stress-induced protein expression. J. Cereb. Blood Flow Metab. 2000, 20, 520–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liou, A.K.; Clark, R.S.; Henshall, D.C.; Yin, X.M.; Chen, J. To die or not to die for neurons in ischemia, traumatic brain injury and epilepsy: A review on the stress-activated signaling pathways and apoptotic pathways. Prog. Neurobiol. 2003, 69, 103–142. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, E.J.; Dentcheva, E.; Curtis, K.M.; Roberts, V.L.; Siman, R.; Neumar, R.W. Neuroprotection with delayed initiation of prolonged hypothermia after in vitro transient global brain ischemia. Resuscitation 2005, 64, 383–388. [Google Scholar] [CrossRef]
- Che, D.; Li, L.; Kopil, C.M.; Liu, Z.; Guo, W.; Neumar, R.W. Impact of therapeutic hypothermia onset and duration on survival, neurologic function, and neurodegeneration after cardiac arrest. Crit. Care Med. 2011, 39, 1423–1430. [Google Scholar] [CrossRef] [Green Version]
- Singh, J.; Barrett, J.; Sangaletti, R.; Dietrich, W.D.; Rajguru, S.M. Additive protective effects of delayed mild therapeutic hypothermia and antioxidants on PC12 cells exposed to oxidative stress. Ther. Hypothermia Temp. Manag. 2021, 11, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Early- versus late-initiation of therapeutic hypothermia after cardiac arrest: Preliminary observations from the experience of 17 Italian intensive care units. Resuscitation 2012, 83, 823–828. [CrossRef]
- Chiu, W.T.; Lin, K.C.; Tsai, M.S.; Hsu, C.H.; Wang, C.H.; Kuo, L.K.; Chien, Y.S.; Wu, C.H.; Lai, C.H.; Huang, W.C.; et al. Post-cardiac arrest care and targeted temperature management: A consensus of scientific statement from the Taiwan Society of Emergency & Critical Care Medicine, Taiwan Society of Critical Care Medicine and Taiwan Society of Emergency Medicine. J. Formos. Med. Assoc. 2021, 120, 569–587. [Google Scholar] [CrossRef]
- Sessler, D.I. Thermoregulatory defense mechanisms. Crit. Care Med. 2009, 37, S203–S210. [Google Scholar] [CrossRef]
- Wandaller, C.; Holzer, M.; Sterz, F.; Wandaller, A.; Arrich, J.; Uray, T.; Laggner, A.N.; Herkner, H. Head and neck cooling after cardiac arrest results in lower jugular bulb than esophageal temperature. Am. J. Emerg. Med. 2009, 27, 460–465. [Google Scholar] [CrossRef]
- Benz-Woerner, J.; Delodder, F.; Benz, R.; Cueni-Villoz, N.; Feihl, F.; Rossetti, A.O.; Liaudet, L.; Oddo, M. Body temperature regulation and outcome after cardiac arrest and therapeutic hypothermia. Resuscitation 2012, 83, 338–342. [Google Scholar] [CrossRef]
- Nair, S.U.; Lundbye, J.B. The occurrence of shivering in cardiac arrest survivors undergoing therapeutic hypothermia is associated with a good neurologic outcome. Resuscitation 2013, 84, 626–629. [Google Scholar] [CrossRef]
- Thomsen, J.H.; Nielsen, N.; Hassager, C.; Wanscher, M.; Pehrson, S.; Køber, L.; Bro-Jeppesen, J.; Søholm, H.; Winther-Jensen, M.; Pellis, T.; et al. Bradycardia during targeted temperature management: An early marker of lower mortality and favorable neurologic outcome in comatose out-of-hospital cardiac arrest patients. Crit. Care Med. 2016, 44, 308–318. [Google Scholar] [CrossRef]
- Simpson, R.F.G.; Dankiewicz, J.; Karamasis, G.V.; Pelosi, P.; Haenggi, M.; Young, P.J.; Jakobsen, J.C.; Bannard-Smith, J.; Wendel-Garcia, P.D.; Taccone, F.S.; et al. Speed of cooling after cardiac arrest in relation to the intervention effect: A sub-study from the TTM2-trial. Crit. Care 2022, 26, 356. [Google Scholar] [CrossRef] [PubMed]
- Howes, D.; Gray, S.H.; Brooks, S.C.; Boyd, J.G.; Djogovic, D.; Golan, E.; Green, R.S.; Jacka, M.J.; Sinuff, T.; Chaplin, T.; et al. Canadian Guidelines for the use of targeted temperature management (therapeutic hypothermia) after cardiac arrest: A joint statement from The Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society (CNCCS), and the Canadian Critical Care Trials Group (CCCTG). Resuscitation 2016, 98, 48–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madden, L.K.; Hill, M.; May, T.L.; Human, T.; Guanci, M.M.; Jacobi, J.; Moreda, M.V.; Badjatia, N. The implementation of targeted temperature management: An evidence-based guideline from the Neurocritical Care Society. Neurocrit. Care 2017, 27, 468–487. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Nolan, J.P.; Andersen, L.W.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Lilja, G.; Morley, P.T.; et al. ERC-ESICM guidelines on temperature control after cardiac arrest in adults. Intensive Care Med. 2022, 48, 261–269. [Google Scholar] [CrossRef]
- Johnson, N.J.; Danielson, K.R.; Counts, C.R.; Ruark, K.; Scruggs, S.; Hough, C.L.; Maynard, C.; Sayre, M.R.; Carlbom, D.J. Targeted temperature management at 33 versus 36 degrees: A retrospective cohort study. Crit. Care Med. 2020, 48, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Nishikimi, M.; Ogura, T.; Nishida, K.; Hayashida, K.; Emoto, R.; Matsui, S.; Matsuda, N.; Iwami, T. Outcome related to level of targeted temperature management in postcardiac arrest syndrome of low, moderate, and high severities: A nationwide multicenter prospective registry. Crit. Care Med. 2021, 49, e741–e750. [Google Scholar] [CrossRef]
- Hifumi, T.; Kuroda, Y.; Kawakita, K.; Sawano, H.; Tahara, Y.; Hase, M.; Nishioka, K.; Shirai, S.; Hazui, H.; Arimoto, H.; et al. Effect of Admission Glasgow Coma Scale Motor Score on Neurological Outcome in Out-of-Hospital Cardiac Arrest Patients Receiving Therapeutic Hypothermia. Circ. J. 2015, 79, 2201–2208. [Google Scholar] [CrossRef] [Green Version]
- Suh, G.J.; Kwon, W.Y.; Kim, K.S.; Lee, H.J.; Jeong, K.Y.; Jung, Y.S.; Lee, J.H. Prolonged therapeutic hypothermia is more effective in attenuating brain apoptosis in a Swine cardiac arrest model. Crit. Care Med. 2014, 42, e132–e142. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Nagao, K.; Hase, M.; Tahara, Y.; Hazui, H.; Arimoto, H.; Kashiwase, K.; Sawano, H.; Yasuga, Y.; Kuroda, Y.; et al. Impact of therapeutic hypothermia in the treatment of patients with out-of-hospital cardiac arrest from the J-PULSE-HYPO study registry. Circ. J. 2011, 75, 1063–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkegaard, H.; Søreide, E.; de Haas, I.; Pettilä, V.; Taccone, F.S.; Arus, U.; Storm, C.; Hassager, C.; Nielsen, J.F.; Sørensen, C.A.; et al. Targeted Temperature Management for 48 vs 24 Hours and Neurologic Outcome After Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2017, 318, 341–350. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total n (%) | Non-Survivors (n = 109) | Survivors (n = 68) | p | |||
|---|---|---|---|---|---|---|
| OHCA (n = 76) | IHCA (n = 33) | OHCA (n = 60) | IHCA (n = 8) | |||
| Age (mean, std), years | 65.55 (15.10) | 67.25 (15.03) | 62.83 (14.09) | 0.0581 | ||
| Sex, Male (number, percentage) | 109 (61.58) | 68 (62.39) | 41 (60.29) | 0.7807 | ||
| APACHE II (mean, std) | 31.67 (6.70) | 32.62 (7.07) | 30.13 (6.29) | 0.0189 | ||
| Rate of cooling, °C/h (mean, std) | 0.39 (0.25) | 0.42 (0.28) | 0.33 (0.18) | 0.0097 | ||
| BT at cardiac arrest, min (mean, std) | 36.23 (1.20) | 36.25 (1.20) | 36.19 (1.21) | 0.7495 | ||
| BT at ROSC, min (mean, std) | 35.87 (1.31) | 35.72 (1.39) | 36.1 (1.13) | 0.0674 | ||
| BT at start of cooling, min (mean, std) | 35.79 (1.55) | 35.61 (1.62) | 36.07 (1.40) | 0.0539 | ||
| From CPR to ROSC, min (no/low flow time) (mean, std) | 33.46 (44.77) | 39.97 (54.04) | 23.32 (20.71) | 0.0048 | ||
| From ROSC to initial cooling, min (pre-induction time) (mean, std) | 350.27 (216.72) | 322.64 (174.08) | 394.5 (267.0) | 0.0510 | ||
| From cooling to target, min (induction time) (mean, std) | 270.90 (229.53) | 246.13 (229.27) | 310.6 (225.9) | 0.0690 | ||
| Arrest to TTM target, min (mean, std) | 659.22 (328.29) | 614.79 (296.65) | 728.5 (363.85) | 0.0254 | ||
| Good Neurological Function (n = 25) | Poor Neurological Function (n = 136) | p | |||
|---|---|---|---|---|---|
| OHCA (n = 21) | IHCA (n = 4) | OHCA (n = 102) | IHCA (n = 34) | ||
| Age, years, (mean, std) | 57.96 (13.59) | 66.02 (14.3) | 0.0068 | ||
| Sex, Male (number, percentage) | 18 (72) | 85 (62.5) | 0.4948 | ||
| APACHE II (mean, std) | 27.4 (5.85) | 32.2 (6.66) | 0.0007 | ||
| Rate of cooling, °C/h (mean, std) | 0.015 (0.012) | 0.0266 (0.036) | 0.096 | ||
| BT at cardiac arrest, min (mean, std) | 36.47 (1.01) | 36.26 (1.21) | 0.6008 | ||
| BT at ROSC, min (mean, std) | 36.34 (0.98) | 35.79 (1.34) | 0.0499 | ||
| BT at start of cooling, min (mean, std) | 36.68 (1.15) | 35.65 (1.56) | 0.0023 | ||
| From CPR to ROSC, min (no-low flow time) (mean, std) | 20.52 (21.39) | 37.18 (49.47) | 0.0107 | ||
| From ROSC to initial cooling (min) (pre-induction time) | 401.84 (324.76) | 346.85 (201.20) | 0.239 | ||
| From cooling to target, min (induction time) (mean, std) | 350 (224.25) | 259.79 (223.95) | 0.0225 | ||
| Arrest to TTM target, min (mean, std) | 772.36 (403.70) | 648.40 (319.11) | 0.107 | ||
| (A) | ||||
|---|---|---|---|---|
| Pre-Induction Time | p | |||
| 0–276 Min (n = 75) | 276–390 Min (n = 52) | >390 Min (n = 50) | ||
| Age, years (mean, std) | 67.5 (15.5) | 63.2 (16.7) | 65.2 (12.4) | 0.2761 |
| Gender, male (number, percentage) | 48 (64.0) | 31 (59.6) | 30 (60.0) | 0.8508 |
| APACHE II score (mean, std) | 32.13 (6.54) | 32.83 (7.03) | 30.77 (6.59) | 0.2998 |
| Rate of cooling (mean, std) | 0.50 (0.31) | 0.36 (0.16) | 0.25 (0.13) | <0.001 |
| CPC score 28 days after cardiac arrest (mean, std) | 4.40 (1.10) | 4.15 (1.41) | 3.72 (1.44) | 0.0182 |
| 28-day survival (mean, std) | 24 (32.00) | 17 (32.69) | 27 (54.00) | 0.0279 |
| (B) | ||||
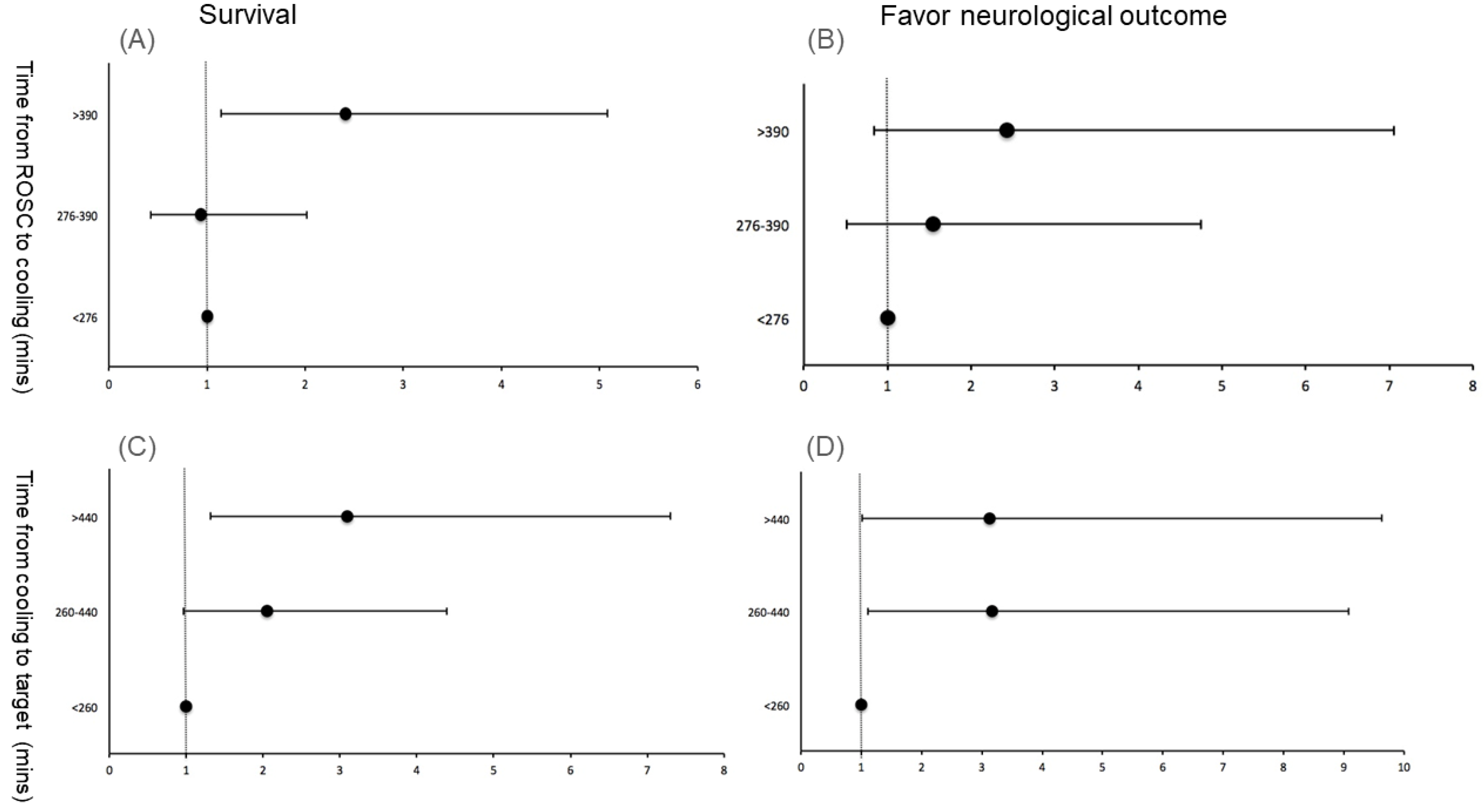
| Time from ROSC to Cooling * (min) | Odds Ratio | 95% CI | p Value | |
| Odds ratios for survival | ||||
| <276 | 1 | (Reference group) | ||
| 276–390 | 0.94 | 0.43–2.02 | 0.87 | |
| >390 | 2.41 | 1.14–5.08 | 0.02 | |
| Odds ratios for good neurological outcomes | ||||
| <276 | 1 | (Reference group) | ||
| 276–390 | 1.55 | 0.51–4.75 | 0.44 | |
| >390 | 2.43 | 0.84–7.96 | 0.1 | |
| (A) | ||||
|---|---|---|---|---|
| Induction Time | p | |||
| 0–260 Min (n = 106) | 260–440 Min (n = 40) | >440 Min (n = 31) | ||
| Age, years (mean, std) | 68.1 (14.7) | 62.9 (13.4) | 58.9 (16.2) | 0.0030 |
| Gender, male (number, percentage) | 62 (58.5) | 24 (60.0) | 23 (74.2) | 0.2788 |
| APACHE II score(mean, std) | 33.19 (6.46) | 28.62 (6.04) | 30.35 (6.82) | 0.0003 |
| Rate of cooling (mean, std) | 0.48 (0.28) | 0.30 (0.12) | 0.19 (0.10) | <0.001 |
| CPC score 28 days after cardiac arrest (mean, std) | 4.43 (1.05) | 3.85 (1.52) | 3.48 (1.58) | <0.001 |
| 28-day survival (mean, std) | 31 (29.25) | 19 (47.50) | 18 (58.06) | 0.0060 |
| (B) | ||||
| Time from Cooling to Target #(min) | Odds Ratio | 95% CI | p Value | |
| Odds ratio for survival | ||||
| <260 | 1 | (Reference group) | ||
| 260–440 | 2.05 | 0.96–4.39 | 0.06 | |
| >440 | 3.10 | 1.32–7.30 | 0.01 | |
| Odds ratio for good neurological outcomes | ||||
| <260 | 1 | (Reference group) | ||
| 260–440 | 3.17 | 1.11–9.08 | 0.03 | |
| >440 | 3.10 | 1.02–9.63 | <0.05 | |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Hazard ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
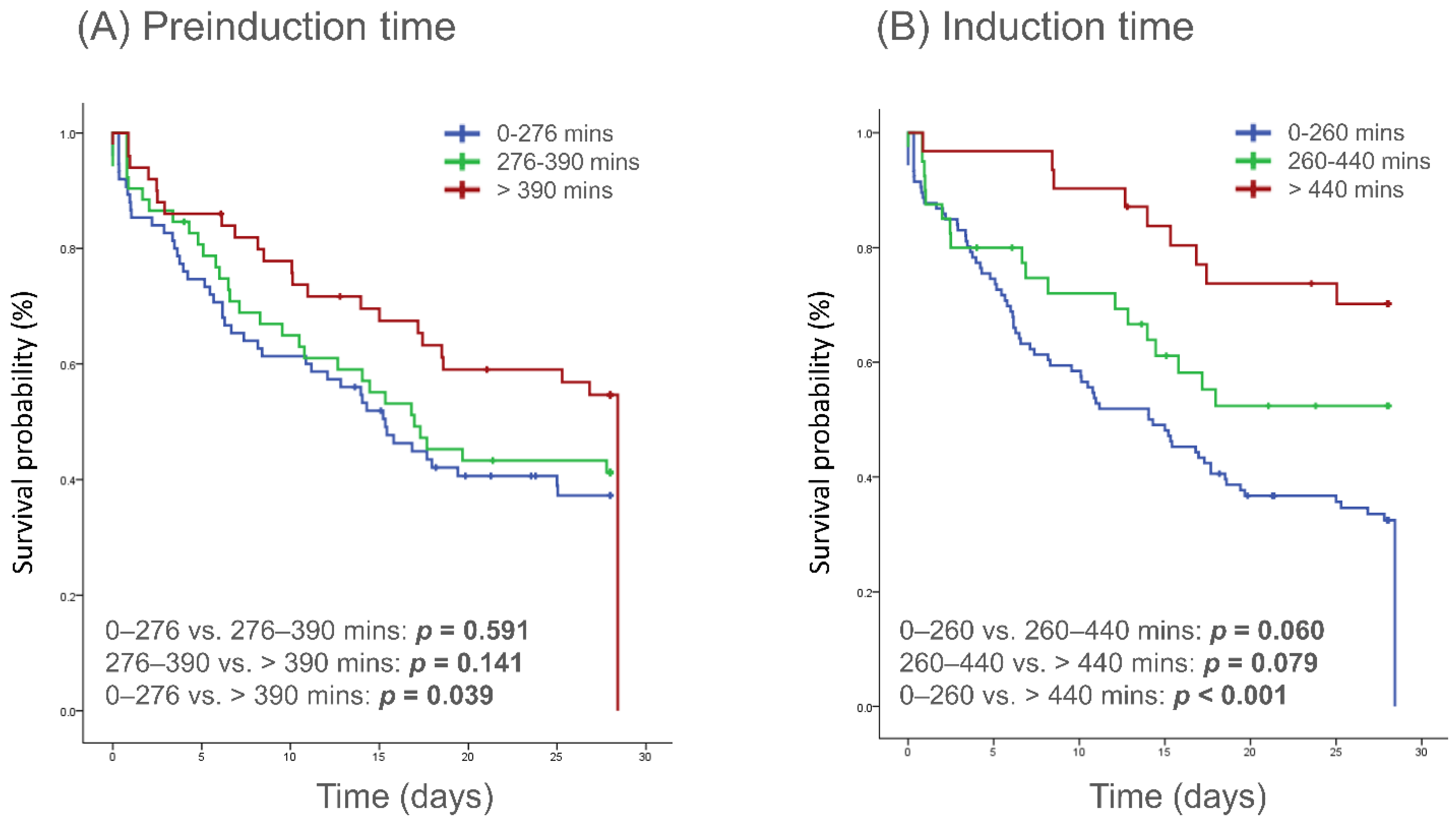
| Pre-induction time | ||||
| 0–276 min | 1 (Reference group) | 1 (Reference group) | ||
| 276–390 min | 0.902 (0.572–1.423) | 0.657 | 0.907 (0.570–1.444) | 0.681 |
| >390 min | 0.594 (0.358–0.984) | 0.043 | 0.636 (0.382–1.057) | 0.081 |
| Induction time | ||||
| 0–260 min | 1 (Reference group) | 1 (Reference group) | ||
| 260–440 min | 0.646 (0.389–1.072) | 0.091 | 0.781 (0.458–1.332) | 0.364 |
| >440 min | 0.304 (0.152–0.609) | 0.001 | 0.382 (0.187–0.776) | 0.008 |
| Age | 1.016 (1.002–1.030) | 0.026 | 1.005 (0.990–1.021) | 0.513 |
| Sex, male | 1.108 (0.741–1.655) | 0.618 | ||
| Witnessed | 0.738 (0.493–1.104) | 0.618 | ||
| Initial rhythm, shockable | 0.463 (0.267–0.802) | 0.006 | 0.600 (0.336–1.071) | 0.084 |
| Basic life support | 0.921 (0.539–1.574) | 0.763 | ||
| Duration of resuscitation effort | 1.002 (0.998–1.006) | 0.248 | ||
| APACHE II | 1.037 (1.007–1.067) | 0.014 | 1.019 (0.986–1.053) | 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, I.-T.; Wang, C.-J.; Chen, C.-H.; Yang, S.-H.; Chen, C.-Y.; Huang, Y.-C.; Lin, C.-Y.; Wu, C.-L. Optimal Timing of Targeted Temperature Management for Post-Cardiac Arrest Syndrome: Is Sooner Better? J. Clin. Med. 2023, 12, 2628. https://doi.org/10.3390/jcm12072628
Wang I-T, Wang C-J, Chen C-H, Yang S-H, Chen C-Y, Huang Y-C, Lin C-Y, Wu C-L. Optimal Timing of Targeted Temperature Management for Post-Cardiac Arrest Syndrome: Is Sooner Better? Journal of Clinical Medicine. 2023; 12(7):2628. https://doi.org/10.3390/jcm12072628
Chicago/Turabian StyleWang, I-Ting, Chieh-Jen Wang, Chao-Hsien Chen, Sheng-Hsiung Yang, Chun-Yen Chen, Yen-Chun Huang, Chang-Yi Lin, and Chien-Liang Wu. 2023. "Optimal Timing of Targeted Temperature Management for Post-Cardiac Arrest Syndrome: Is Sooner Better?" Journal of Clinical Medicine 12, no. 7: 2628. https://doi.org/10.3390/jcm12072628
APA StyleWang, I. -T., Wang, C. -J., Chen, C. -H., Yang, S. -H., Chen, C. -Y., Huang, Y. -C., Lin, C. -Y., & Wu, C. -L. (2023). Optimal Timing of Targeted Temperature Management for Post-Cardiac Arrest Syndrome: Is Sooner Better? Journal of Clinical Medicine, 12(7), 2628. https://doi.org/10.3390/jcm12072628